COUNTRY ACCOUNTABILITY FRAMEWORK: Scorecard* Lesotho · COUNTRY ACCOUNTABILITY FRAMEWORK:...
14
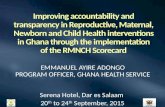
KEY: 1 2 3 5 Situation analysis (strengths, weaknesses/gaps) Priority Actions Assessment & Plan 1 Advocacy/mobilization key stakeholders Conduct full CRVS assessment and develop improvement plan Coordinating Mechanism 1 Establish interagency coordinating committee involving all key stakeholders. Hospital reporting 2.5 Establish a system which will link Ministry of Health and NICR for ease of reporting births using hospital birth certificate. Community reporting 2 Strengthen community reporting of births and deaths, implement innovative approaches. Mobilise Councillors and Village Health Workers to work together with the Chiefs so that every birth or death occurring in their communities is registered once they occur. Training workshops to be conducted to equip them with the requirements and better appreciation of all the NICR activities Strengthen community reporting through use of VA by community workers Strengthen the linkages between Health Facilities and the community in terms of reporting deaths and births Adaptation of Verbal Autopsy tools and capacity building at different levels Vital statistics 3 Increase the resources mobilization by all programs for dissemination of vital statistics Local studies for mortality 1 Develop the HDSS system Not present, needs to be developed Needs a lot of strengthening Needs some strengthening A rapid assessment which led to the formation of the Department of National Identity and Civil Registry in 2010 within the Ministry of Home Affairs was conducted. Key staff was recruited and recruiting of junior staff is in the process. Awareness campaigns on the Department's activities are performed. No assessment of the status and practices of CRVS has been conducted and no improvement plan has been developed. There is no interagency coordinating committee in place. Hospital reporting of deaths is not done. The only death reports from the hospitals are the ones made by the relatives if they feel like it. Hospital reporting of deaths includes a cause of death, using the ICD-10, with regular quality control are done by the Ministry of Health. Community births and deaths are reported covering the whole country but not using ICT, the Chiefs are responsible for that. Verbal Autopsy (VA) for deaths is not being done but is in the pipeline. Vital statistics (fertility and mortality) are not published every year but only after survey and census. It is available but delayed in dissemination to stakeholders. Local health and demographic surveillance sites (HDSS) are not available. COUNTRY ACCOUNTABILITY FRAMEWORK: Scorecard* Civil registration & vital statistics systems Already present/no action needed Lesotho * This final version has been reviewed and validated through a national accountability workshop involving a broader stakeholder group. Page 1/14
Transcript of COUNTRY ACCOUNTABILITY FRAMEWORK: Scorecard* Lesotho · COUNTRY ACCOUNTABILITY FRAMEWORK:...

KEY:
1
2
3
5
Situation analysis
(strengths, weaknesses/gaps)Priority Actions
Assessment & Plan 1 Advocacy/mobilization key stakeholders
Conduct full CRVS assessment and develop improvement plan
Coordinating Mechanism 1 Establish interagency coordinating committee involving all key
stakeholders.
Hospital reporting 2.5 Establish a system which will link Ministry of Health and NICR for
ease of reporting births using hospital birth certificate.
Community reporting 2 Strengthen community reporting of births and deaths, implement
innovative approaches. Mobilise Councillors and Village Health
Workers to work together with the Chiefs so that every birth or
death occurring in their communities is registered once they occur.
Training workshops to be conducted to equip them with the
requirements and better appreciation of all the NICR activities
Strengthen community reporting through use of VA by community
workers
Strengthen the linkages between Health Facilities and the
community in terms of reporting deaths and births
Adaptation of Verbal Autopsy tools and capacity building at
different levels
Vital statistics 3 Increase the resources mobilization by all programs for
dissemination of vital statistics
Local studies for mortality 1 Develop the HDSS system
Not present, needs to be developed
Needs a lot of strengthening
Needs some strengthening
A rapid assessment which led to the formation of the Department
of National Identity and Civil Registry in 2010 within the Ministry
of Home Affairs was conducted. Key staff was recruited and
recruiting of junior staff is in the process. Awareness campaigns on
the Department's activities are performed. No assessment of the
status and practices of CRVS has been conducted and no
improvement plan has been developed.
There is no interagency coordinating committee in place.
Hospital reporting of deaths is not done. The only death reports
from the hospitals are the ones made by the relatives if they feel
like it. Hospital reporting of deaths includes a cause of death,
using the ICD-10, with regular quality control are done by the
Ministry of Health.
Community births and deaths are reported covering the whole
country but not using ICT, the Chiefs are responsible for that.
Verbal Autopsy (VA) for deaths is not being done but is in the
pipeline.
Vital statistics (fertility and mortality) are not published every year
but only after survey and census. It is available but delayed in
dissemination to stakeholders.
Local health and demographic surveillance sites (HDSS) are not
available.
COUNTRY ACCOUNTABILITY FRAMEWORK: Scorecard*
Civil registration & vital statistics
systems
Already present/no action needed
Lesotho
* This final version has been reviewed and validated through a national accountability workshop involving a broader stakeholder group. Page 1/14

COUNTRY ACCOUNTABILITY FRAMEWORK: Scorecard* Lesotho
Situation analysis
(strengths, weaknesses/gaps)Priority Actions
M&E Plan 3 Finalise the National Health Strategy and update the M&E
framework
Finalise and align the Child Survival M&E plan with the National
Health Strategic Plan
M&E Coordination 2 Strengthen the Strategic Information coordination team, by
reviewing the ToRs, and incorporate relevant stakeholders
(statistics, academia and civil society) in to the SI coordination
committee
Health Surveys 2.5 To have a comprehensive survey plan within the M&E plan
Resource mobilisation
Facility data (HMIS) 2 Strengthen district information officers in data collection, collection
and analysis and integrate different data sets. Carryout data quality
baseline which will inform routine data quality assessment.
Enhance data analysis and advocate for data usage at district level
for informed decision making
Analytical capacity 3 Strengthen analytical capacity at district level
Equity 4
Data sharing 3 Strengthen national data repository with all relevant data and
reports and share information with the public
There is an M&E plan for the health sector running from 2008/09
to 2010/11, therefore there is a need to review M&E plan to be in
line with updated National Health Strategy. The Maternal and
Newborn M&E plan is aligned with the National Health sector
M&E plan. The Child survival strategy is in place but not as part of
the RMN. The national Strategic Information (M&E, Research and
HMIS) committee is in place but it is not inclusive of some
members such as statistics, academia and civil society and it
doesn’t meet on regular basis. There is no stand alone Health
survey plan, but the plan is inclusive in the overall National M&E
plan. There is insufficient funds for conducting health surveys. The
plan to conduct EMoNC is in place for 2012-2013. A system is
available with defined times of reporting from the facility, to the
next level. But we still have fragmented data sets collected by
different programmes which can compromise quality. Annual Joint
Review is informed by facility data verification and routine data
quality assessment is planned to be implemented in 2013. There is
a regular production of reports on progress made towards
achieving what was planned for, in the beginning of the year ( AJR,
Quarterly Review reports). The process has been decentralised to
the districts, but there is a need to capacitate districts in
producing good analytical progress reports. Among other forms of
data collection, health data are collected through surveys and
routine method. The health surveys clearly disaggregate data on
sex, income, minority and location, while the routine data covers
some aspects like age, sex, and location. Data sharing is partially
done to the public, through dissemination of data during Annual
Joint Review meetings. The Ministry is also in the process of
developing data warehouse.
Monitoring of results
* This final version has been reviewed and validated through a national accountability workshop involving a broader stakeholder group. Page 2/14

COUNTRY ACCOUNTABILITY FRAMEWORK: Scorecard* Lesotho
Situation analysis
(strengths, weaknesses/gaps)Priority Actions
Notification 4 Need to be reviewed this year 2013
Policy Review and Stakeholders meeting for validation
Capacity to review and act 2.5 Strengthen National capacity through training in MDSR and data
analysis. Review of the reporting and assessor's tools and customize
the MAMMAS software. Strengthen District capacity through training of assessors and other
health workers (midwives) in MDSR
Hospitals/facilities 3 Improve reporting in hospitals by capacitating the District
committees and private institutions and health workers; Training in
ICD certification and coding.Strengthen capacity of private sector in reviewing and reporting of
maternal deaths.
Quality of care 2 Support accreditation exercise and data analysis to improve quality
Community reporting & feedback 1 Capacitate the community structures in reporting of maternal
deaths occurring at the community
Strengthen communication at community level( Village Health
Workers (VHW)) for reporting maternal deaths that occur at
community level
Review of the system 1 Link the MDSR secretariat to the IDSR.
Review The MDSR annually in order to implement the
recommendations arising from the maternal death reports in order
to improve quality of care through AJR meeting
Maternal death surveillance &
response
There Policy is in place (National Reproductive Health Policy -
2009). Maternal deaths are a notifiable event in this policy
document. There is a National LCCEMD (Lesotho Committee on
Confidential Enquiry into Maternal Deaths) which sits quarterly or
as necessary. There is a secretariat for capturing all deaths
occurring at facility level. Capacity for data analysis is still a
challenge. There is a District Maternal Death Review Committee
which sits immediately when a death has occurred to review and
notify the LCCEMD within 7 days. At Hospital level there are
trained Maternal Death Assessors who participate in the Maternal
Death Reviews. There is a high turn over of the trained assessors
and other health workers. Reporting is taking place telephonically
within 24 hours, a written report is submitted within sven days
using ICD 10, however there is high attrition rate among trained
health workers and assessors. Only maternal deaths occurring in
the public hospitals are reviewed.
Quality of care assessments are conducted through accreditation
of facilities by Quality Assurance of the Ministry of Health
however there are limited resources to carryout this activity.
There is no tool developed for reporting community maternal
deaths, however the plan is in place to establish a system by end
of 2012. No electronic devices are used at community level for
reporting. A Verbal Autopsy tool has been developed for piloting
in 2013. Communities do not receive feed back yet. The gaps in
completeness and quality of care have been identified and are
being addressed, but there is need to link IDSR and MDSR
reporting.
* This final version has been reviewed and validated through a national accountability workshop involving a broader stakeholder group. Page 3/14

COUNTRY ACCOUNTABILITY FRAMEWORK: Scorecard* Lesotho
Situation analysis
(strengths, weaknesses/gaps)Priority Actions
Policy 3 Advocate the Government buy in into making e-health a reality
Capacity building for health workers in IT application
Infrastructure 2 Deploy IT personnel at district level to support and supervise
Services 2 Discussions are on-going for inclusion of MNCH data capturing into
the pilot phase of EMR
Establish the linkages between health workload data and facility
data
Establish the linkages between health workload data and facility
data
Standards 2 Determine the eHealth standards and interoperability components
required to support eHealth services, applications and
infrastructure, as well as to support broader changes to health
information flows.
Governance 1 Develop and support a strong effective coordination mechanism
(coordination committee)
Mobilise financial and human resources for implementation of e-
Health
Protection 2.5 Strengthen enforcement of the data protection law
Enforce compliance to data protection policies
Innovation and eHealth
The national ehealth strategy is integrated in the National Health
Policy and strategy. At district level (DHMT and Hospitals) there is
mobile and internet connectivity, while in in the Health Centres
there is an on-going programme for installation of ICT
infrastructure. There is need for training on IT application.
Maternal Deaths are captured at district level using computerised
registers, while immunisation data is still paper based. The
Electronic Medical Record which will be capturing data
electronically is being piloted in one district. There are no links
between health workload and facility data. There are means of
storage of data in the central level, but there is need introduce
means of data storage at district level. There is no coordinating
committee for e-Health with the involvement of other
stakeholders. There is data protection, legislation and regulatory
frameworks for sharing of health information. Data protection
policies are not enforced.
* This final version has been reviewed and validated through a national accountability workshop involving a broader stakeholder group. Page 4/14

COUNTRY ACCOUNTABILITY FRAMEWORK: Scorecard* Lesotho
Situation analysis
(strengths, weaknesses/gaps)Priority Actions
National health accounts 1 Sensitize the stakeholders about the importance of developing NHA
framework
Assess the potential link of the current system and NHA
Compact 2 Organize a meeting to engage government and development
partners and work towards "compact"
Coordination 1 Set up a steering committee, officially approved, with institutional
support, and functioning using results-based management methods
Ensure inclusion of all key stakeholders in resource tracking/NHA
Production 1 Train staff on system of health accounts 2011; train district and
regional staff
Map government codes to NHA codes and develop IT conversion
tool for NHA
Develop/strengthen database for production of NHA
Analysis 1 Develop SHA
Introduce the SHA 2011 system
Data Use 1 Advocate for/promote use of NHA data in policy making process
There is no system and Government commitment to introducing
the NHA framework. There is IFMIS for Government budget
allocation and tracking of resources, but it is not able to clearly
capture the health sector expenditure. There is individual
agreement between the partner and the Government for
reporting commitments and disbursements. There is no NHA
steering committee in place, and there is no human capacity to
produce NHA tables and core indicators. No analytical summaries
are produced on SHA 2011 health accounts.
Monitoring of resources
* This final version has been reviewed and validated through a national accountability workshop involving a broader stakeholder group. Page 5/14

COUNTRY ACCOUNTABILITY FRAMEWORK: Scorecard* Lesotho
Situation analysis
(strengths, weaknesses/gaps)Priority Actions
Reviews 3.5 Operationalize implementation of the recommendations
Consolidate and harmonise the PHC review meetings and the district
quarterly review meeting to form one district review meeting
Synthesis of information & policy context 2.5 Strengthen the capacity of Health centre nurses and district health
information office to prepare analytical reports prior to the reviews
Strengthen mechanism to compile all policy/qualitative information
to inform annual reviews
From review to planning 2.5 Strengthen the use of review results for planning purposes
Ensure greater involvement of all stakeholders
Compacts or equivalent mechanisms 2.5 Ensure the existence of a single national M&E framework that
national health plan will fit into
Establish Partner's coordination focal person and Develop Swap
ToRs
Review processes
The Annual Joint Review meeting is conducted annually to review
health sector performance against set targets and goals however
the recommendations from the meeting are not being closely
followed
Key stakeholders are actively involved in the preparation and
execution of the reviews. RMNCH programme reviews are
included in the Annual Joint Review report. The Primary Health
Care quarterly review meetings are held at the district level but
there is a need for strengthening. Health Sector reviews are
informed by a good synthesis of health data including RMNCH.
The health sector reviews are informed by a systematic analysis of
qualitative data, where the mini survey is administered over and
above the performance of the key indicators to captured public
opinions about service delivery. There is a mechanism, whereby
after the reviews the recommendations are translated into the
priorities of the Ministry but there is no follow up on the
recommendations implementation. Key stakeholders are involved
from the process of priority setting, target setting and during
development of operational plans. A country compact or similar
mechanism (a government-led process of planning, coordination
and facilitation of all development partners, including funding
flows) exists and the Minister of Finance chairs the meeting. The
partners coordination is not as expected but the Ministry has
engaged a SWaP consultant for developing partner coordination
mechanism.
* This final version has been reviewed and validated through a national accountability workshop involving a broader stakeholder group. Page 6/14

COUNTRY ACCOUNTABILITY FRAMEWORK: Scorecard* Lesotho
Situation analysis
(strengths, weaknesses/gaps)Priority Actions
Parliament active on RMNCH issues 3 The new members of the Parliament need to be sensitized.
Integration of RMNCH issues in Parliaments' speeches.
Civil Society Coalition 2 Capacity building for civil society coalition on RMNCH to produce
evidence based advocacy messages and materials.
Media role 3 Capacity building for media personnel on RMNCH related issues to
produce evidence based advocacy messages and materials.
Sensitise the community on RMNCH through the radio sessions.
Work with the media to strengthen monitoring and reporting on
RMNCH.
Countdown event for RMNCH 2 Establish Countdown Coordinating Committee
Prepare Countdown report/profile using all evidence
There is a portfolio on Health issues inclusive of RMNCH. Public
forums for information sharing and discussions on RMNCH issues
are starting on a small scale. A civil society coalitions exist but are
not focusing on RMNCH. Evidence-based advocacy messages and
materials with exist but are not focusing on RMNCH. There are
some TV and radio programmes focusing on RMNCH, but it is not
systematic. There is a representation of media in the LCCEMD and
PMML(Prevention of Maternal Mortality in Lesotho). The media is
interested in the issues of RMNCH but the areas of accountability,
reporting towards implementation of national commitments still
has some challenges. Media covers the annual reviews. A national
countdown event for RMNC is planned to be undertaken before
the end of 2012/2013 and there is no countdown committee in
place. A country Countdown report or profile is not available yet.
Advocacy & outreach
* This final version has been reviewed and validated through a national accountability workshop involving a broader stakeholder group. Page 7/14

Actions Priority
(1-2=high,
3=medium,
4=low)
Approach/actions Lead govt/ national
institute
Partners 2012 2013 2014 2015 Total
Estimated
Cost per
action
2012/13
Catalytic
funding
Unfunded
balance
Potential
sources for
funding unmet
balance
Advocacy /mobilization key
stakeholders
1 Meeting Ministry of Home Affairs UNICEF X X $1,200 $1,200 MOHA
Conduct full CRVS assessment and
develop improvement plan
1 Survey Ministry of Home Affairs
(MOHA)
UNFPA x $50,000 $44,500 $5,500 MOHA/CoIA
Establish interagency coordinating
committee involving all key
stakeholders
1 Meeting MOHA WHO $1,200 $1,200 MOHA
Establish a system which will link
Ministry of Health and NICR for
ease of reporting births using
hospital birth certificate
1 Inter Ministerial/Agencies
coordinating committee
MOHA/MOH UNFPA X X $11,000 $11,000 UNICEF/UNFPA
Strengthen community reporting of
births and deaths, implement
innovative approaches. Mobilise
Councillors and Village Health
Workers to work together with the
Chiefs so that every birth or death
occurring in their communities is
registered once they occur .Training
workshops to be conducted to
equip them with the requirements
and better appreciation of all the
NICR activities
1 Workshop MOHA/MOH UNICEF/WHO X X $60,000 $60,000 UNICEF/UNFPA
Strengthen community reporting
through use of VA by community
workers
1 Workshop MOH WHO/UNFPA X X X $25,000 $15,000 $10,000 UNFPA/CoIA
Strengthen the linkages between
Health Facilities and the community
in terms of reporting deaths and
births
1 Workshop MOH UNFPA/WHO/
UNICEF
X X $25,000 $15,000 $10,000 UNFPA
Adaptation of Verbal Autopsy tools
and capacity building at different
levels
2 Workshop MOHA WHO/UNFPA X X $1,200 $1,200 MOHA
Increase the resources mobilization
by all programs for dissemination
of vital statistics
2 Proposal for funding MOHA/BOS x x
Develop the HDSS system 3 BOS/MOH UNFPA X $37,000 $37,000 BOS/MOH/
UNFPA
COUNTRY ACCOUNTABILITY FRAMEWORK: Roadmap* Lesotho
CIVIL REGISTRATION AND VITAL STATISTICS SYSTEMS (CRVS)
* This final version has been reviewed and validated through a national accountability workshop involving a broader stakeholder group. Page 8/14

Actions Priority
(1-2=high,
3=medium,
4=low)
Approach/actions Lead govt/ national
institute
Partners 2012 2013 2014 2015 Total
Estimated
Cost per
action
2012/13
Catalytic
funding
Unfunded
balance
Potential
sources for
funding unmet
balance
COUNTRY ACCOUNTABILITY FRAMEWORK: Roadmap* Lesotho
CIVIL REGISTRATION AND VITAL STATISTICS SYSTEMS (CRVS)
Finalise the National Health
Strategy and update the M&E
framework
2 Workshop MOH WHO X X $15,000 $7,500 $7,500 MOH/CoIA
Finalise and align the Child Survival
M&E plan with the National Health
Strategic Plan
2 Workshop MOH HMIS X X $1,200 $1,200 $0 CoIA
Strengthen the Strategic
Information coordination team, by
reviewing the ToRs, and
incorporate relevant stakeholders
(statistics, academia and civil
society) in to the SI coordination
committee
2 Meeting MOH HMIS/CDC X X $1,000 $1,000 $0 CoIA
To have a comprehensive survey
plan within the M&E plan
2 Workshop X X $1,500 $1,500 $0 CoIA
Resource mobilisation 2 Strategic Information (SI) TWG MOH X X X
Strengthen district information
officers in data collection, collection
and analysis and integrate different
data sets. Carryout data quality
baseline which will inform routine
data quality assessment
Enhance data analysis and advocate
for data usage at district level for
informed decision making
2 Workshop MOH IHM/CDC $56,000 $12,000 $44,000 MOH/IHM/CoIA
Strengthen analytical capacity at
district level
1
Strengthen national data repository
with all relevant data and reports
and share information with the
public
2
MONITORING OF RESULTS
* This final version has been reviewed and validated through a national accountability workshop involving a broader stakeholder group. Page 9/14

Actions Priority
(1-2=high,
3=medium,
4=low)
Approach/actions Lead govt/ national
institute
Partners 2012 2013 2014 2015 Total
Estimated
Cost per
action
2012/13
Catalytic
funding
Unfunded
balance
Potential
sources for
funding unmet
balance
COUNTRY ACCOUNTABILITY FRAMEWORK: Roadmap* Lesotho
CIVIL REGISTRATION AND VITAL STATISTICS SYSTEMS (CRVS)
Policy Review and Stakeholders
meeting for validation
3 Workshop MOH WHO/UNFPA/UNI
CEF
X $12,000 $12,000 UNFPA
Strengthen National capacity
through training in MDSR and data
analysis. Review of the reporting
and assessor's tools and customize
the MAMMAS software
1 Workshop MOH UNFPA/WHO/ X X $12,000 $12,000 UNFPA
Strengthen District capacity
through training of assessors and
other health workers (midwives) in
MDSR
1 Workshop MOH UNFPA/WHO X X $24,000 $24,000 $0 CoIA
Improve reporting in hospitals by
capacitating the District committees
and private institutions and health
workers; Training in ICD
certification and coding
1 Workshop MOH UFPA/WHO X X $24,000 $24,000 CoIA
Strengthen capacity of private
sector in reviewing and reporting
of maternal deaths
1 Workshop MOH UFPA/WHO X X $12,000 $12,000 UNFPA
Support accreditation exercise and
data analysis to improve quality
2 Survey MOH X X $476,000 $24,000 $452,000 CoIA/MOH
Capacitate the community
structures in reporting of maternal
deaths occurring at the community
1 Workshop MOH WHO X X $12,000 $12,000 MOH
Strengthen communication at
community level( Village Health
Workers (VHW)) for reporting
maternal deaths that occur at
community level
1 Procurement MOH/WHO WHO X $36,000 $36,000 $0 CoIA
Link the MDSR secretariat to the
IDSR
1 Meeting MOH WHO X $1,200 $1,200 WHO/UNFPA
Review The MDSR annually in order
to implement the
recommendations arising from the
maternal death reports in order to
improve quality of care through AJR
meeting
1 Meeting MOH UNFPA x $12,000 $12,000 UNFPA
MATERNAL DEATH SURVEILLANCE AND RESPONSE
* This final version has been reviewed and validated through a national accountability workshop involving a broader stakeholder group. Page 10/14

Actions Priority
(1-2=high,
3=medium,
4=low)
Approach/actions Lead govt/ national
institute
Partners 2012 2013 2014 2015 Total
Estimated
Cost per
action
2012/13
Catalytic
funding
Unfunded
balance
Potential
sources for
funding unmet
balance
COUNTRY ACCOUNTABILITY FRAMEWORK: Roadmap* Lesotho
CIVIL REGISTRATION AND VITAL STATISTICS SYSTEMS (CRVS)
Advocate the Government buy in
into making e-health a reality
1 Meeting MOH x x x $12,000 $12,000 $0 CoIA
Capacity building for health workers
in IT application
2 Workshop MOH X $138,889 $6,000 $132,889 CoIA/MOH
Deploy IT personnel at district level
to support and supervise
1 Office/Procurement MOH X $22,000 $22,000 MOH
Discussions are on-going for
inclusion of MNCH data capturing
into the pilot phase of EMR
1 Meeting MOH x x x $1,200 $1,200 $0 CoIA
Establish the linkages between
health workload data and facility
data
2 Workshop MOH x x $166,666 $1,200 $165,466 MOH
Determine the eHealth standards
and interoperability components
required to support eHealth
services, applications and
infrastructure, as well as to support
broader changes to health
information flows.
1 Meeting MOH x x $12,000 $1,200 $10,800 MOH/CoIA
Develop and support a strong
effective coordination mechanism
(coordination committee)
1 Inter Ministerial/Agencies
coordinating committee
MOH x x $1,200 $1,200 $0 CoIA
Mobilise financial and human
resources for implementation of e-
Health
2 Proposal for funding MOH x x $500 $500 MOH
Strengthen enforcement of the
data protection law
2 Meeting MOH x x $10,000 $7,700 $2,300 MOH/CoIA
Enforce compliance to data
protection policies
2 Meeting MOH x x
INNOVATION AND E-HEALTH
* This final version has been reviewed and validated through a national accountability workshop involving a broader stakeholder group. Page 11/14

Actions Priority
(1-2=high,
3=medium,
4=low)
Approach/actions Lead govt/ national
institute
Partners 2012 2013 2014 2015 Total
Estimated
Cost per
action
2012/13
Catalytic
funding
Unfunded
balance
Potential
sources for
funding unmet
balance
COUNTRY ACCOUNTABILITY FRAMEWORK: Roadmap* Lesotho
CIVIL REGISTRATION AND VITAL STATISTICS SYSTEMS (CRVS)
Sensitize the stakeholders about
the importance of developing NHA
framework
1 Workshop MOH x x
Assess the potential links of the
current system and NHA
1 Meeting MOH x
Organize a meeting to engage
government and development
partners and work towards
"compact"
1 Meeting MOH x x x $1,200 $1,200 $0 CoIA
Set up a steering committee,
officially approved, with
institutional support, and
functioning using results-based
management methods
1 Inter Ministerial/Agencies
coordinating committee
MOH X $1,200 $1,200 $0 CoIA
Ensure inclusion of all key
stakeholders in resource tracking
/NHA
MOH
Train staff on system of health
accounts 2011; train district and
regional staff
2 Training Workshop MOH X X $72,000 $12,000 $60,000 CoIA/MOH
Map government codes to NHA
codes and develop IT conversion
tool for NHA
2 MOH
Develop /strengthen database for
production of NHA
3 MOH X
Develop SHA 2 MOH
Introduce the SHA 2011 system 2 MOH
Advocate for /promote use of NHA
data in policy making process
2 MOH
MONITORING OF RESOURCES
* This final version has been reviewed and validated through a national accountability workshop involving a broader stakeholder group. Page 12/14

Actions Priority
(1-2=high,
3=medium,
4=low)
Approach/actions Lead govt/ national
institute
Partners 2012 2013 2014 2015 Total
Estimated
Cost per
action
2012/13
Catalytic
funding
Unfunded
balance
Potential
sources for
funding unmet
balance
COUNTRY ACCOUNTABILITY FRAMEWORK: Roadmap* Lesotho
CIVIL REGISTRATION AND VITAL STATISTICS SYSTEMS (CRVS)
Operationalize implementation of
the recommendations
1 MOH x x x
Consolidate and harmonise the PHC
review meetings and the district
quarterly review meeting to form
one district review meeting
2 Meeting MOH x $30,000 $10,000 $20,000 CDC/CoIA/MOH
Strengthen the capacity of Health
center nurses and district health
information office to prepare
analytical reports prior to the
reviews
1 Workshop MOH x x x $44,000 MOH/IHM/CDC
Strengthen mechanism to compile
all policy / qualitative information
to inform annual reviews
1 Workshop MOH x x
Strengthen the use of review
results for planning purposes
1 MOH x x
Ensure greater involvement of all
stakeholders
1 MOH x x x
Ensure the existence of a single
national M&E framework that
national health plan will fit into
1 MOH x x x
Establish Partner's coordination
focal person and Develop Swap
ToRs
1 Inter Ministerial/Agencies
coordinating committee
MOH x x x $1,200 $1,200 $0 CoIA/MOH
REVIEW PROCESSES
* This final version has been reviewed and validated through a national accountability workshop involving a broader stakeholder group. Page 13/14

Actions Priority
(1-2=high,
3=medium,
4=low)
Approach/actions Lead govt/ national
institute
Partners 2012 2013 2014 2015 Total
Estimated
Cost per
action
2012/13
Catalytic
funding
Unfunded
balance
Potential
sources for
funding unmet
balance
COUNTRY ACCOUNTABILITY FRAMEWORK: Roadmap* Lesotho
CIVIL REGISTRATION AND VITAL STATISTICS SYSTEMS (CRVS)
The new members of the
Parliament need to be sensitized
1 Meeting MOH WHO X $1,200 $1,200 $0 CoIA
Integration of RMNCH issues in
Parliaments' speeches
1 Public gatherings MOH WHO/UNPA X X X $10,000 $10,000 UNFPA
Capacity building for civil society
coalition on RMNCH to produce
evidence based advocacy messages
and materials
1 Workshop MOH WHO/UNFPA/UNI
CEF
X X $20,000 $6,000 $14,000 UNICEF/CoIA
Capacity building for media
personnel on RMNCH related issues
to produce evidence based
advocacy messages and materials
1 Workshop MOH UNICEF X X $10,000 $10,000 UNICEF
Sensitise the community on RMNCH
through the radio sessions
X X $47,000 $5,000 $42,000 UNICEF/CoIA
Establish Countdown Coordinating
Committee
3 Meeting MOH WHO X $1,200 $1,200 WHO/UNFPA
Prepare Countdown report/profile
using all evidence
3 Workshop MOH WHO X $12,000 $12,000 UNFPA
TOTALS 1,522,955 250,000 1,272,955 -
Needs Catalytic request Unfunded balance
CRVS $211,600 $74,500 $137,100
Monitoring of results $74,700 $23,200 $51,500
MDSR $621,200 $84,000 $537,200
eHealth & Innovation $364,455 $30,500 $333,955
Monitoring of resources $74,400 $14,400 $60,000
Reviews $75,200 $11,200 $64,000 Advocacy $101,400 $12,200 $89,200
TOTAL $1,522,955 $250,000 $1,272,955
ADVOCACY & OUTREACH
* This final version has been reviewed and validated through a national accountability workshop involving a broader stakeholder group. Page 14/14