Countdown to 2015 Maternal Newborn and Child Survival

of 228
-
Upload
newborn2013 -
Category
Documents
-
view
214 -
download
0
Transcript of Countdown to 2015 Maternal Newborn and Child Survival
-
7/28/2019 Countdown to 2015 Maternal Newborn and Child Survival
1/228
Building a Futurefor Women and Children
The 2012 Report
-
7/28/2019 Countdown to 2015 Maternal Newborn and Child Survival
2/228
ISBN: 978-92-806-4644-3
World Health Organization and UNICEF 2012
All rights reserved. Publications o the World Health Organization are available on the WHO web site (www.who.int) or can be purchased rom WHO Press, World Health
Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel.: +41 22 791 3264; ax: +41 22 791 4857; e-mail: [email protected]).
Requests or permission to reproduce or translate WHO publications whether or sale or or noncommercial distribution should be addressed to WHO Press through
the WHO web site (http://www.who.int/about/licensing/copyright_orm/en/index.html).
The designations employed and the presentation o the material in this publication do not imply the expression o any opinion whatsoever on the part o the World
Health Organization concerning the legal status o any country, territory, city or area or o its authorities, or concerning the delimitation o its rontiers or boundaries. Dot-
ted lines on maps represent approximate border lines or which there may not yet be ull agreement.
The mention o specifc companies or o certain manuacturers products does not imply that they are endorsed or recommended by the World Health Organization inpreerence to others o a similar nature that are not mentioned. Errors and omissions excepted, the names o proprietary products are distinguished by initial capital
letters.
All reasonable precautions have been taken by the World Health Organization to veriy the inormation contained in this publication. However, the published material is
being distributed without warranty o any kind, either expressed or implied. The responsibility or the interpretation and use o the material lies with the reader. In no
event shall the World Health Organization be liable or damages arising rom its use.
This publication has been prepared to acilitate the exchange o knowledge and to stimulate discussion. The logos that appear on the back cover represent the institution-
al afliations o individual participants in report preparation and do not imply institutional endorsement o the contents or recommendations or approval o any specifc
intervention or which data are included. Implementation o specifc intervention is dependent on the legal context in each country. While all reasonable precautions have
been taken to veriy the inormation contained in this publication, Countdown partners accept no responsibility or errors.
Printed in Washington, DC.
Photo credits: cover, 2002, Leela Khanal, Courtesy o Photoshare; page 3, 2012 Cassandra Mickish/CCP, Courtesy o Photoshare; page 4, Joshua Roberts/Save
the Children; page 12, 2009 Joydeep Mukherjee, Courtesy o Photoshare; page 21, 2007 WHO/Christopher Black; page 22, 2006 Salma Siddique, Courtesy o
Photoshare; page 30, UNICEF/NYHQ2002-0516/Vitale; page 41, UNICEF/NYHQ2009-0600/Noorani; page 50, Colin Crowley/Save the Children; page 200, 2007
Bonnie Gillespie, Courtesy o Photoshare.
Editing and layout by Communications Development Incorporated, Washington, DC.
Contributors
Lead writers: Jennier Requejo (PMNCH/Johns
Hopkins University), Jennier Bryce (Johns Hopkins
University), Cesar Victora (University o Pelotas)
Subeditors/writers: Aluisio Barros (University o
Pelotas), Peter Berman (Harvard School o Public
Health), Zulfqar Bhutta (Aga Khan University),
Ties Boerma (WHO), Bernadette Daelmans (WHO),
Adam Deixel (Family Care International), Joy Lawn
(Saving Newborn Lives), Elizabeth Mason (WHO),
Holly Newby (UNICEF), Ann Starrs (Family Care
International)
Profle team: Tessa Wardlaw (UNICEF), Archana
Dwivedi (UNICEF), Holly Newby (UNICEF)
Additional writing team: Andres de Francisco
(PMNCH), Carole Presern (PMNCH), Mickey Chopra(UNICEF), Blerta Maliqi (WHO), Giorgio Cometto
(Global Health Workorce Alliance), Justine Hsu
(LSHTM), Matthews Matthai (WHO), Priyanka
Saksena (WHO), Sennen Hounton (UNFPA)
Production team: Christopher Trott and
Elaine Wilson (Communications Development
Incorporated), Jennier Requejo (PMNCH/Johns
Hopkins University), Adam Deixel (Family Care
International), Dina El Husseiny (PMNCH)
Countdown Coordinating Committee: Mickey
Chopra (co-chair), Zulfqar Bhutta (co-chair),Jennier Bryce, Joy Lawn, Carole Presern, Elizabeth
Mason, Ann Starrs, Peter Berman, Bernadette
Daelmans, Tessa Wardlaw, Ties Boerma, Cesar
Victora, Flavia Bustreo, Andres de Francisco,
Jennier Requejo, Laura Laski, Nancy Terreri,
Holly Newby, Archana Dwivedi, Zoe Matthews,
Jacqueline Mahon, Lori McDougall
Technical Working Groups
Coverage:Jennier Bryce (co-chair), Tessa
Wardlaw (co-chair), Holly Newby, Archana
Dwivedi, Jennier Requejo, Alison Moran, Shams
El Arieen, Sennen Hounton, Steve Hodgins,
Angella Mtimumi, Blerta Maliqi, Lale Say, James
Tibenderana, Nancy Terreri
Equity:Cesar Victora (co-chair), Ties Boerma
(co-chair), Henrik Axelson, Aluisio Barros, CarineRonsmans, Wendy Graham, Betty Kirkwood,
Edilberto Loaiza, Zulfqar Bhutta, Kate Kerber,
Financing:Peter Berman (chair), Henrik Axelson,
Jacqueline Mahon, Lara Brearley, Justine Hsu,
Daniel Kraushaar, Ravi Rannan-Eliya, Anne Mills,
Karin Stenberg
Health systems and policies:Bernadette
Daelmans (co-chair), Zoe Matthews (co-chair),
Blerta Maliqi, Nancy Terreri, Giorgio Cometto,
Priyanka Saksena, Sennen Hounton, Amani Siyam,
Daniel Kraushaar, Eleonora Cavagnero, MarkYoung, Lara Brearley, Amani Siyam
-
7/28/2019 Countdown to 2015 Maternal Newborn and Child Survival
3/228
Building a Futurefor Women and Children
The 2012 Report
-
7/28/2019 Countdown to 2015 Maternal Newborn and Child Survival
4/228
Building a Future for Women and Children The 2012 Reportii
Acknowledgements
Countdownwould like to thank the ollowing:
UNICEF/Statistics and Monitoring Section or use
o global databases, preparation o country proles
and inputs to, and review o, report text. Particular
recognition goes to David Brown, Danielle Burke,
Xiaodong Cai, Liliana Carvajal, Elizabeth Horn-
Phathanothai, Priscilla Idele, Rouslan Karimov,
Mengjia Liang, Rol Luyendijk, Colleen Murray,
Khin Wityee Oo, Chiho Suzuki and Danzhen You.
University o Pelotas colleagues Andrea Damaso
and Giovanny Frana or their inputs to the equity
analyses.
The PMNCH secretariat or convening meetingsand teleconerences or the Countdown and
PMNCH colleagues Dina El Husseiny or providing
administrative support and Henrik Axelson,
Lori McDougall and Shyama Kuruvilla or their
contributions to the report.
Amani Siyam rom WHO (HQ), Thomas H. H.
Walter rom the University o Technology Berlin,
Fekri Dureab rom the WHO Yemen country oce
and Carmen Dolea or their inputs to the health
systems and health policies analyses.
Steve Hodgins, Cindy Berg, Andre Lalonde, Cherrie
Evans, Wendy Graham and Claudia Hanson or
their inputs on the quality o care panel. The
PMNCH or convening a meeting on quality o care.
Robert E. Black at Johns Hopkins University or his
inputs into the nutrition and cause o child death
analyses.
Lale Saye and Iqbal Shah rom WHO or their
inputs to the maternal mortality and causes o
maternal death analyses.
Nancy Terreri or her contributions to the report.
Nuriye Ortayli rom UNFPA or inputs to the amily
planning analyses.
The Bill and Melinda Gates Foundation, the World
Bank and the Governments o Australia, Canada,
Norway, Sweden and the United Kingdom or their
support or Countdown to 2015.
-
7/28/2019 Countdown to 2015 Maternal Newborn and Child Survival
5/228
Building a Future for Women and Children The 2012 Report
Building a uture or women and children
In the ve minutes it takes to read this page,
3 women will lose their lives to complications
o pregnancy or childbirth, 60 others will suer
debilitating injuries and inection due to the
same causes, and 70 children will die, nearly 30
o them newborn babies. Countless other babies
will be stillborn or suer potentially long-term
consequences o being born prematurely. The
vast majority o these deaths and disabilities are
preventable.
During these same ve minutes, however,
countless lives will be saved. A baby, ed only
breastmilk or her rst six months o lie, will
avoid diarrhoeal disease. Another will survive
pneumonia because he received appropriateantibiotics. A child will avoid malaria because
she sleeps under an insecticide-treated net.
Another, exposed to measles, will not succumb
to disease because he has been vaccinated. An
adolescent, not yet physically, emotionally or
nancially ready to have a child, will receive
amily planning services, including counselling to
prevent unintended pregnancy; a new mother will
choose to delay her next pregnancy until a saer
time. A pregnant, HIV-positive woman will receive
treatment that protects her health and that o her
baby. An expectant mother, at a routine antenatal
care visit, will receive treatment or the high bloodpressure that can threaten her lie; another will
give birth at a health acility where skilled birth
attendants save her lie when she experiences
postpartum bleeding; yet another will receive
antenatal corticosteroids to develop her babys
lungs to ensure a better chance o survival. And
a newborn and her mother will receive liesaving
treatment or inection within the rst week ater
birth.
The countdown to the 2015 Millennium
Development Goal deadline is a race against
time, a race to add to the list o lives saved andsubtract rom the tally o maternal, newborn
and child deaths. Each lie saved creates innite
possibilitiesor a healthy, productive individual;
or a stable, thriving amily; or a stronger
community and nation; or a better world. And
interventions that improve maternal, newborn
and child health and nutrition contribute to a
uture generation o healthier, smarter and more
productive adults.
This report highlights country progressand
obstacles to progresstowards achieving
Millennium Development Goals 4 and 5 to reduce
child mortality and improve maternal health
(box 1). Countdown to 2015ocuses on evidence-
based solutionshealth interventions proven to
save livesand on the health systems, policies,
nancing and broader contextual actors that
aect the equitable delivery o these interventions
to women and children. Countdownocuses
on data, because building a better uture andprotecting the basic human right to lie require
understanding where things stand right now
and how they got to where they are today.
And Countdownocuses on what happens in
countrieswhere investments are made or
not made, policies are implemented or not
implemented, health services are received or not
received and women and children live or die.
Box 1
News in the 2012 report
Status reprt n mrtaity and nutritin.
Evidence n the scae preterm birth and
stibirths.
Changes in cverage interventins.
Detaied equity anaysis.
A cus n the determinants cverage.
Picy, nancia and systems inputs needed
r prgress.
Ppuatin grwth and pitica cnfict as key
chaenges.
Miestneswhat des success k ike?
Hw t read and use the cuntry pres.
Countdown mving rward t 2015.
Quaity care.
Cuntry-eve engagement.
-
7/28/2019 Countdown to 2015 Maternal Newborn and Child Survival
6/228
Contents
Countdownheadlines or 2012: saving the lives o
the worlds women, newborns and children 1
Countdown to 2015: tracking progress, ostering
accountability 5
The Countdowncountry prole: a tool or
action 10
Progress towards Millennium Development Goals
4 and 5 13
Coverage along the continuum o care 23
Determinants o coverage 32
Milestones o progress on the path to success 42
Accountability now or Millennium Development
Goals 4 and 5 48
Country proles 51
Annex A Country prole indicators and data
sources 203
Annex B Denitions oCountdown
indicators 206
Annex C Denitions o policy and health systems
indicators 208
Annex D Essential interventions or reproductive,
maternal, newborn and child health 210
Annex E Countdown priority countries
considered to be malaria endemic 211
Annex F Details on estimates rom the Inter-agency Group or Child Mortality Estimation used
in the Countdownreport 212
Notes 213
Reerences 214
-
7/28/2019 Countdown to 2015 Maternal Newborn and Child Survival
7/228
Building a Future for Women and Children The 2012 Report
Countdownheadlinesfor 2012: saving the livesof the worlds women,
newborns and children
Maternal and child survival: progress, but not
enough . . .
Maternalmortalityhasdeclineddramatically,
butfasterprogressisneeded.
Maternaldeathshavedroppedfrom543,000
ayearin1990to287,000in2010.
Only9Countdowncountriesareontrackto
achieveMillenniumDevelopmentGoal5;25
havemadeinsufcientornoprogress.
MaternalmortalityisconcentratedinSub-
SaharanAfricanandSouthAsiancountries:
anAfricanwomanslifetimeriskofdying
frompregnancy-relatedcausesis100times
higherthanthatofawomaninadeveloped
country.
Childmortalityisdownsharply,butmoreneeds
tobedone.
Deathsamongchildrenunderage5
worldwidehavedeclinedfrom12milliona
yearin1990to7.6millionin2010.
Only23Countdowncountriesareontrackto
achieveMillenniumDevelopmentGoal4;13
havemadelittleornoprogress.
Despiterecentimprovements,pneumonia
anddiarrhoeastillcausemorethantwo
milliondeathsayearthatcouldbeavoided
byavailablepreventivemeasuresandprompt
treatment.
Newbornsurvivalisimprovingtooslowly,and
stillbirths,especiallyintrapartumstillbirths,and
pretermbirthsneedurgentattention.
40%ofchilddeathsoccurduringtherst
monthoflife.
Morethan10%ofbabiesarebornpreterm,
agurethatisrising,andcomplications
duetopretermbirtharetheleadingcause
ofnewborndeathsandthesecondleading
causeofchilddeaths.
Countdowncountriesthathavesuccessfully
reducedneonatalmortalitysuchas
Bangladesh,NepalandRwandaoffermodelsforimprovingnewbornsurvival.
MostCountdowncountriesfaceasevere
nutritioncrisis.
Undernutri tioncontributestomorethana
thirdofchilddeathsandtoatleastafthof
maternaldeaths.
Inthemajori tyofCountdowncountries,more
thanathirdofchildrenarestunted;stunting
ismostcommonamongpoorchildren.
Coverage: gains, gaps, inequities, challenges
Bangladesh,Cambodia,EthiopiaandRwanda,
countriesthathaverapidlyincreasedcoverage
formultipleinterventionsacrossthecontinuum
ofcare,offerlessonsforcountrieswithslower
ormoreunevenprogress.
Highcoveragelevelsforvaccines(over80%on
averageacrossallCountdowncountries)andrapid
progressindistributionofinsecticide-treatednets
showwhatispossiblewithhighlevelsofpolitical
commitmentandnancialresources.
Progressismuchslower,andinequitiesin
coveragemuchwider,forskilledattendant
atbirthandotherinterventionsthatrequire
astronghealthsystem.Newapproachesare
neededthatimprovethequalityofservices,
bringservicesclosertohomeandexpand
accesstoessentialcare.
-
7/28/2019 Countdown to 2015 Maternal Newborn and Child Survival
8/228
Building a Future for Women and Children The 2012 Report2
There are wide ranges in coverage across the
Countdowncountries or many interventions.
Coverage o demand or amily planning
satised, or example, ranges rom 17% in
ragile states such as Sierra Leone to 93% in
Vietnam and Brazil and 97% in China. Countries
with high coverage o specic interventions
show what can be achieved with the right
policies, adequate investments, appropriate
implementation strategies and strong demand.
To increase coverage, the volume o services
provided must grow at a aster pace than the
population. Nigeria, or example, has seen the
number o births grow rom 4.3 million in 1990
to 6.1 million in 2008, with 7 million projected
in 2015. Although the country has doubled
the number o births attended by a skilled
health care provider since 1990, coverage has
increased only 8%.
The Millennium Development Goal 7 target or
access to an improved drinking water source has
been achieved globally and in 23 Countdown
countries; progress in access to an improved
sanitation acility is lagging. For both interventions
the need is most pronounced in rural areas.
Poor people have less access to health services
than richer people, and geographic and urban-
rural inequities also exist in many countries,
highlighting the importance o digging deeper into
subnational data to support eective planning and
resource allocation according to need.
Context matters: supportive policies, adequate
fnancing, sufcient human resources and peace
Countries such as Ghana, Malawi, Lao Peoples
Democratic Republic and Tanzania have
achieved results through innovative human
resources policies such as task shiting. Other
countries need to ollow this lead.
Ocial development assistance or maternal,
newborn and child health in Countdowncountries has increased steadily over the
past decade, accounting or around 40% o
ocial development assistance or health that
Countdowncountries received in 2009, but the
rate o increase appears to be slowing.
Though domestic health unding is essential, 40
Countdowncountries devote less than 10% o
government spending to health.
In most countries a severe disease episode or
a major pregnancy or childbirth complication
can push amilies into nancial catastrophe: in
all but 5 Countdowncountries out-o-pocket
payments or health services account or 15% or
more o health expenditure.
53 Countdowncountries continue to experience
a severe shortage o health workers.
Countries with high-intensity conficts have lower
coverage and higher inequity and mortality.
Providing broader access to education,
expanding opportunities or girls and women,
reducing poverty and improving living
conditions, and respecting human rights,
including eliminating violence against women,
can improve health and reduce mortality.
Making good on commitments
Countries and their partners have pledged to work
together to meet Millennium Development Goals
4 and 5. There is still time. Countdowndata show
that by transorming commitment into action,
rapid progress is possible. To build a better uture
or women and children, we all must keep our
promises. Millions o womens and childrens lives
depend on it.
Countries must continue to:
Implement costed national health plans that
emphasize service integration and include
programmes or reproductive, maternal,
newborn and child health.
Strengthen health inormation systems,
including vital registration systems and national
health accounts, so that timely, accurate data
can inorm policies and programmes.
Increase domestic unding allocations or and
expenditures on health.
Build the numbers, motivation and skill mix o
the health workorce.
Analyse subnational data to identiy gaps
and inequities and to monitor and evaluate
programmes and policies.
Develop strategies to rapidly address nutrition
shortalls and increase coverage o essential
-
7/28/2019 Countdown to 2015 Maternal Newborn and Child Survival
9/228
Building a Future for Women and Children The 2012 Report
health interventions across the ull continuum o
care, especially or the poor.
All stakeholders must continue to:
Advocate or sucient unding or reproductive,
maternal, newborn and child health.
Undertake research to develop the evidence on
eective interventions and innovative strategies
or service delivery.
Support country eorts to implement innovative
strategies that increase access to timely,
equitable and high-quality care.
Together we can:
Demand accountability and act accountably.
Build a better uture or millions o women and
children.
-
7/28/2019 Countdown to 2015 Maternal Newborn and Child Survival
10/228
-
7/28/2019 Countdown to 2015 Maternal Newborn and Child Survival
11/228
Building a Future for Women and Children The 2012 Report
Countdown to 2015:tracking progress,ostering accountability
Countdown to 2015is a global movement to
track, stimulate and support country progress
towards achieving the health-related Millennium
Development Goals, particularly goals 4 (reduce
child mortality) and 5 (improve maternal health;
box 2). Since 2005 Countdownhas produced
periodic reports and country proles on key
aspects o reproductive, maternal, newborn and
child health, achieving global impact with its ocuson accountability and use o available data to hold
stakeholders to account or global and national
action.
Countdown to 2015:
Focuses on coverage levels and trends o
interventions proven to improve reproductive,
maternal, newborn and child health as well
as critical determinants o coverage: health
systems unctionality, health policies and
nancing.
Examines equity in coverage across dierent
population groups within and across Countdown
countries.
Uses these data to hold countries and their
international partners accountable or progress
in reproductive, maternal, newborn and child
health (box 3).
Supports country-level countdowns to promote
evidence-based accountability (see concluding
section or a description o country-level
Countdownactivities).
Countdownincludes academics, governments,
international agencies, proessional associations,
donors and nongovernmental organizations, with
The Lancetas a key partner.
Countdown ocuses on countries
Countdowntracks progress in the 75 countries
where more than 95% o all maternal and
child deaths occur (map 1) and produces
country proles and reports to be used by all
stakeholdersinternationally and at the country
levelto advocate or action on reproductive,
maternal, newborn, and child health.
The number oCountdowncountries has
increased, refecting an evolution rom a child
survival initiative to a movement supportive o thecontinuum o care and responsive to the global
accountability agenda. Countdowncountries
are selected primarily based on burden o
maternal, newborn and child mortality, taking into
consideration both numbers and rates o death.
Details on the country selection process or this
and previous Countdowncycles are available at
www.countdown2015mnch.org.
Countdown is more than tracking coverage ointerventions!
Countdowngathers and synthesizes data oncoverage o liesaving interventions across
the continuum o care rom pre-pregnancy
and childbirth through childhood up to age 5,
highlighting progress and missed opportunities.
Coverage is dened as the proportion o
individuals needing a health service or intervention
who actually receive it. Countdownalso tracks
key determinants o coverage in countriesequity
patterns across population groups, health system
unctionality and capacity, supportive health
policies and nancial resources or maternal,
newborn and child health.
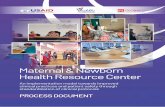
Figure 1 shows the overarching conceptual
ramework oCountdown, illustrating the links
between coverage and its determinants as well
as the broader contextual actors that aect
maternal, newborn and child survival. Countdown
is engaging in cross-cutting research to answer
questions rom countries and their partners in
response to previous Countdownreports and
proles about the ingredients needed or success
in achieving high, sustained and equitable
-
7/28/2019 Countdown to 2015 Maternal Newborn and Child Survival
12/228
Building a Future for Women and Children The 2012 Report6
Equity in coverage, a central component o the
Countdownconceptual ramework, is highlighted
throughout this report. The Commission on
Accountability or Womens and Childrens
Healths Keeping Promises, Measuring Results,1
emphasizes disaggregating all coverage data by
key equity considerations to assess progress.
National-level aggregate statistics oten hide
important within-country inequities that
countries must address to achieve the health
intervention coverage. This research aims to
expand the evidence base on eective delivery
strategies or increasing coverage that take into
consideration critical health policy and systems,
political, economic, nancial, environmental
and social actors. Recognizing that eective
coverage depends on service quality, Countdown
is expanding eorts to examine barriers and
acilitating actors to improving the quality o
care.
Box 2
Countdown and the accountability agenda
At a September 2010 UN Genera Assemby summit
t assess prgress n the Miennium Devepment
Gas, Secretary-Genera Ban Ki-mn aunched the
Gba Strategy r Wmens and Chidrens Heath,
an unprecedented pan t save the ives 16 miin
wmen and chidren by 2015.1 This was wed by
the estabishment the Cmmissin n Inrmatin
and Accuntabiity r Wmens and Chidrens Heath,
which was charged with deveping an accuntabiity
ramewrk t mnitr and track cmmitments made
t the Gba Strategy. In May 2011 the Cmmissin
reeased Keeping Promises, Measuring Results,2 which
drew n advice rm Countdown members and ther
technica eperts t identiy a set cre indicatrs3
that enabe stakehders t track prgress in imprving
cverage interventins acrss the cntinuum care
and resurces r wmens and chidrens heath. Thereprt urged that a cverage data be disaggregated
by key equity cnsideratins. In September 2011 the
UN Secretary-Genera appinted the independent
Epert Review Grup t reprt annuay n prgress
in impementing the Cmmissins recmmendatins
n reprting, versight and accuntabiity in the 75
pririty cuntries.
Countdown to 2015has cntributed signicanty t
this accuntabiity ramewrk. In Nvember 2011
Countdown cabrated with the Heath Metrics
Netwrk in deveping Monitoring Maternal, Newborn
and Child Health: Understanding Key ProgressIndicators,4 which summarizes the key pprtunities
r and chaenges t eective mnitring the
cre indicatrs identied by the Cmmissin. In
March 2012 Countdown pubished Accountability or
Maternal, Newborn and Child Survival: An Update o
Progress in Priority Countries,5 which eatured cuntry
pres custmized t shwcase the cmmissin
indicatrs. That pubicatin was aunched at the
126th Assemby the Inter-Pariamentary Unin,
in Kampaa, Uganda, where a histric resutin n
the re pariaments in addressing key chaenges
t securing the heath wmen and chidren was
unanimusy adpted.6Countdown partners have
as cabrated with a wide range ther gba
heath initiativesincuding the Internatina Heath
Partnership,7 the GAVI Aiance8 and the Gba Fund t
Fight AIDS, Tubercusis and Maaria, amng thers
n deveping a cmmn, harmnized cnceptua
ramewrk9 r mnitring and evauating resuts.
Countdown is cmmitted t deepening its
engagement in the accuntabiity agenda thrugh:
Countdown pres cused n the Cmmissin
indicatrs, updated annuay with new data and
resuts.
Specia anayses t address accuntabiityquestins and inrm the independent Epert
Review Grup.
Cuntry-eve Countdown prcesses that incude
natina cnsutatins, wrkshps r pubicatins
and use Countdown data and methdgica
appraches (see cncuding sectin).
Notes
1. See www.everywmaneverychid.rg r up-t-date inrmatin
n cmmitments t the Gba Strategy.
2. Cmmissin n Inrmatin and Accuntabiity r Wmens and
Chidrens Heath 2011.
3. The cre Cmmissin indicatrs r resuts are a subset the
Countdown indicatrs and are incuded in the cuntry pres; see
annees A and B r denitins.
4. Cuntdwn t 2015, Heath Metrics Netwrk, UNICEF and WHo
2011.
5. Cuntdwn t 2015 2012.
6. IPU 2012.
7. Berma and thers 2010.
8. GAVI Aiance 2010.
9. Bryce and thers 2011.
-
7/28/2019 Countdown to 2015 Maternal Newborn and Child Survival
13/228
Building a Future for Women and Children The 2012 Report
Millennium Development Goals and universal
coverage.
Countdownreviews, analyses and compiles
statistics on reproductive, maternal, newborn and
child health by child gender, household wealth
quintile, maternal education, urban-rural residence
and region o the country and produces scientic
publications with these results.2 Detailed equityproles or each country are available at www.
countdown2015mnch.org.
Countdown data sources and methods
Building on others work, Countdownaims
to make data on coverage levels and trends,
equity, health policies and systems, and nancial
resources or maternal, newborn and child health
readily accessible. The data or the coverage
indicators, publicly available at www.childino.
org, come mostly rom household surveys (box 4).
The two main surveys used to collect nationally
representative data or reproductive, maternal,
newborn and child health in the Countdown
countries are U.S. Agency or International
Developmentsupported Demographic and Health
Surveys and United Nations Childrens Fund
(UNICEF)supported Multiple Indicator Cluster
Surveys. These surveys also provide estimates
o coverage by household wealth, urban-rural
residence, gender, educational attainment and
geographic location.
The Countdownproles refect the estimates
available or each country. Missing values
and data that are more than ve years old
indicate an urgent need or concerted action to
increase data collection eorts so that timely
evidence is available or policy and programme
development.
The most important criterion or including
an intervention or approach in Countdownis
internationally accepted (peer-reviewed) evidence
demonstrating that it can reduce mortality
among mothers, newborns or children underage 5. Countdowncoverage indicators must also
produce results that are nationally representative,
Box 3
Countdownaddresses multiple MillenniumDevelopment Goals
Miennium Devepment Ga 4 t reduce chid
mrtaity.
Miennium Devepment Ga 5 t imprve
materna heath.
Miennium Devepment Ga 1 t eradicate
etreme pverty and hunger, specicay by
addressing nutritin with a cus n inant and
yung chid eeding.
Miennium Devepment Ga 6 t cmbat
HIV/AIDS, maaria and ther diseases.
Miennium Devepment Ga 7 t ensure
envirnmenta sustainabiity, thrugh tracking
access t an imprved water surce and an
imprved sanitatin aciity.
See www.un.rg/mienniumgas/ r mre
inrmatin n the Miennium Devepment
Gas.
MAP 1
The 75 CountdownPriority countries
-
7/28/2019 Countdown to 2015 Maternal Newborn and Child Survival
14/228
Building a Future for Women and Children The 2012 Report8
reliable and comparable across countries and time,
clear and easily interpreted by policymakers and
programme managers, and available regularly
in most Countdowncountries. The ull list o
Countdownindicators, data sources and methods
used to select the indicators, collect the health
policy and health systems data, and calculate the
equity and nancing measures are available at
www.countdown2015mnch.org.
Data quality control is a critical component o
Countdowntechnical output. Countdownworks
closely with UNICEF and many other groups
responsible or maintaining global databases
and conducts additional quality checks to
ensure consistency and reliability. Countdowns
technical tasks are carried out by working
groups in our areascoverage, equity, health
systems and policies, and nancingand by an
overarching scientic review group. They work
together to ensure data quality and analytic
rigour. A detailed description oCountdowns
organizational structure is available at www.
countdown2015mnch.org.
Supportive policies
For example, maternal protection,community health workers andmidwives authorized to provideessential services, vital registration,adoption of new interventions
Health systems and financing
For example, human resources, functioningemergency obstetric care, referral andsupply chain systems, quality of healthservices, financial resources forreproductive, maternal, newborn andchild health, user fees
Increased survival and improved health and nutrition for women and children
Political, economic, social, technological and environmental factors
Increased and equitable intervention coverage
Pre-pregnancy Pregnancy Birth Postnatal Childhood
Family planningWomens nutrition
Antenatal careIntermittent preventive
treatment for malariaPrevention of mother-to-child
transmission of HIVTetanus vaccines
Skilled attendantat birth
Caesarean sectionand emergency
obstetric care
Postnatal care formother and baby
Infant and youngchild feeding
Case managementof childhood illness
VaccinesMalaria prevention
(insecticide-treatednets and indoorresidual spraying)
FIGURE 1
Summary impact model guiding Countdown work
-
7/28/2019 Countdown to 2015 Maternal Newborn and Child Survival
15/228
Building a Future for Women and Children The 2012 Report
Box 4
Sources of country-level Countdowndata
Natinal health inrmatin systems encmpass a
brad range data surces essential r planning
and r rutine mnitring and evaluatin, including
censuses, husehld surveys, health acility reprting
systems, health acility assessments, vital registratin
systems, ther administrative data systems and
surveillance. Cncerted erts are needed t
strengthen health inrmatin systems acrss the 75
Countdown cuntries t increase the availability
reliable and timely data (see table).1
The preerred surce r mrtality data is high-quality
vital registratin with cmplete reprting deaths
and accurate attributin cause death. Hwever,
nly arund a third Countdown cuntries have birth
registratin cverage ver 75%, and arund 14% have
death registratin cverage ver 50%. Since 2000nly 16% cuntries have been able t generate
cause death inrmatin rm a civil registratin
system r mre than 50% deaths, well belw the
level required r prducing reliable cause death
inrmatin. Mrtality data in Countdown cuntries are
als cllected thrugh surveys r censuses. Mre than
hal Countdown cuntries cnducted such surveys
r child mrtality during 2000 06 and 200711, but
less than a fth did s r maternal mrtality (see
table), hampering cuntry ability t assess mrtality
levels and trends.
Given weak vital registratin systems and the lack ther natinally representative surces mrtality
data, mrtality levels in mst Countdown cuntries
are derived rm mdel-based estimates that use
data rm several surces, including vital registratin,
husehld surveys, censuses, and ther studies.
Cuntry-specifc estimates nenatal and under-fve
mrtality are prduced by the United Natins Inter-
agency Grup r Child Mrtality Estimatin.2 Cuntry-
specifc causes nenatal and child death prfles are
rm natinal estimates calculated by the Child Health
Epidemilgy Reerence Grup with the Wrld Health
organizatin (WHo). Maternal mrtality ratis are rm
the Maternal Mrtality Estimatin Inter-agency Grup.3
Glbal and reginal cause maternal death prfles are
prduced thrugh a WHo systematic review prcess.
Interventin cverage respnds mre quickly t
prgrammatic changes than des mrtality and shuld
be measured mre requently t prmte evidence-
based decisinmaking. only 29 Countdown cuntries
(39%) cnducted a husehld survey during 200911,
and 21 them (28%) had als cnducted a previus
survey during 200608. Facility reprts can prvide
estimates r sme cverage indicatrs, but data
quality is ten a prblem in Countdown cuntries, and
these estimates are nt natinally representative.
Data availability in Countdown countries
Topic PeriodNumber ofcountries
Share ofCountdown
countries (%)
Coverage of civil registration
Births (more than 75%) 200510 23 31
Deaths (more than 50%) 200510 10 14
Cause-of-death (morethan 50%) 200010 12 16
Data collection (at least one in period)
Child mortality200711 43 58
And during 200006 41 55
Maternal mortality200711 12 16
And during 200006 8 11
Reproductive, maternal,newborn and child healthintervention coverage
200911 29 39
And during 200608 21 28
Accurate, timely and cnsistent data are crucial r
cuntries t eectively manage their health systems,
allcate resurces accrding t need and ensure
accuntability r delivering n cmmitments t wmen,
newbrns and children. Enhancing cuntry capacity
t mnitr and evaluate results is a cre Countdownprinciple and central t the accuntability agenda.
Achieving this gal requires a lng-term apprach with
shrt-term milestnes. Recmmended actins include4:
Develping a harmnized prgramme husehld
health surveys.
Investing in vital registratin systems and rutine
inrmatin systems.
Evaluating inrmatin and cmmunicatin
technlgies t imprve data cllectin.
Building cuntry capacity t mnitr, review and act
n available data.
Cuntry-level cuntdwn prcesses can cntribute t
building this capacity (see cncluding sectin).
Notes
1. Health Metrics Netwrk and WHo 2011.
2. UNICEF, WHo, Wrld Bank, UNDESA 2011.
3. UNICEF, WHo, Wrld Bank, UNDESA 2012.
4. Cuntdwn t 2015, Health Metrics Netwrk, UNICEF, WHo 2011.
-
7/28/2019 Countdown to 2015 Maternal Newborn and Child Survival
16/228
Building a Future for Women and Children The 2012 Report10
The Countdowncountryprole: a tool or action
Countdowncountry proles present in one place
the best and latest evidence to assess country
progress in improving reproductive, maternal,
newborn and child health (gure 2). The two-page
proles in this report are updated every two years
with new data and analyses. Countdownhas also
committed to annually updating the core indicators
selected by the Commission on Inormation and
Accountability or Womens and Childrens Health.
Reviewing the inormation
The rst step in using the country proles is to explore
the range o data presented: demographics, mortality,
coverage o evidence-based interventions, nutritional
status and socioeconomic equity in coverage. Key
questions in reviewing the data include:
Are trends in mortality and nutritional status
moving in the right direction? Is the country
on track to achieve the health Millennium
Development Goals?
How high is coverage or each intervention? Are
trends moving in the right direction towards
universal coverage? Are there gaps in coverage
or specic interventions?
How equitable is coverage? Are certain
interventions particularly inaccessible or the
poorest segment o the population?
Identiying areas to accelerate progress
The second step in using the country proles is toidentiy opportunities to address coverage gaps
and accelerate progress in improving coverage
and health outcomes across the continuum o care.
Questions to ask include:
Are the coverage data consistent with the
epidemiological situation? For example:
I pneumonia deaths are high, are policies
in place to support community case
management o pneumonia? Are coverage
levels low or careseeking and antibiotic
treatment or pneumonia, and what can be
done to reach universal coverage? Are the
rates o deaths due to diarrhoea consistent
with the coverage levels and trends o
improved water sources and sanitationacilities?
In priority countries or eliminating mother-
to-child transmission o HIV, are sucient
resources being targeted to preventing
mother-to-child transmission?
Does lagging progress on reducing maternal
mortality or high newborn mortality refect
low coverage o amily planning, antenatal
care, skilled attendance at birth and postnatal
care?
Do any patterns in the coverage data suggest
clear action steps? For example, coverage or
interventions involving treatment o an acute
need (such as treatment o childhood diseases
and childbirth services) is oten lower than
coverage or interventions delivered routinely
through outreach or scheduled in advance (such
as vaccinations). This gap suggests that health
systems need to be strengthened, or example
by training and deploying skilled health workers
to increase access to care.
Do the gaps and inequities in coverage alongthe continuum o care suggest prioritizing
specic interventions and increasing unding
or reproductive, maternal, newborn and child
health? For example, is universal access to
labour, delivery and immediate postnatal care
being prioritized in countries with gaps in
interventions delivered around the time o birth?
-
7/28/2019 Countdown to 2015 Maternal Newborn and Child Survival
17/228
-
7/28/2019 Countdown to 2015 Maternal Newborn and Child Survival
18/228
Building a Future for Women and Children The 2012 Report12
-
7/28/2019 Countdown to 2015 Maternal Newborn and Child Survival
19/228
Building a Future for Women and Children The 2012 Report
Progress towardsMillennium DevelopmentGoals 4 and 5
Improving maternal, newborn and child survival
across Countdowncountries depends on each
countrys ability to reach women, newborns
and children with eective interventions along
the continuum o care. Reproductive, maternal,
newborn and child health is inextricably
interconnected: improving maternal health and
nutrition will reduce newborn and young child
deaths. In turn, reducing stunting, improving childhealth and lowering adolescent and total ertility
rates will reduce the risk o a maternal death
among the next generation o women.
Under-ve mortality is declining! A huge
reduction in global deaths among children
under age 5 has been achieved, rom more
than 12 million in 1990 to 7.6 million in 2010, the
latest year or which estimates are available.3
Countdowncountries account or over 95% o
these deaths. The decline has accelerated in the
past decaderom 1.9% a year in the 1990s to
2.5% a year over 200010showing that ocusedgoals and attention make a dierence. Despite
the remarkable progress, much work remains.
The majority o the 7.6 million unacceptable child
deaths that occur each year could be prevented
using eective and aordable interventions.
Mortality is not being reduced uniormly, and
reductions in neonatal mortality lag behind
survival gains among older children. As a result,
the share o neonatal deaths in all deaths among
children under age 5 has increased rom 36%
to 40% over the past decade.4 Faster reductions
in neonatal mortality are critical or achieving
Millennium Development Goal 4. Lessons canbe taken rom Bangladesh, Nepal and Rwanda,
Countdowncountries that have reduced their
neonatal mortality rate by more than 30% in the
last decade.
Modelled estimates o maternal mortality or 2010
based on socioeconomic determinants5 show a
substantial decline in maternal deaths over the
last two decades. The number o women who
die during pregnancy or childbirth has decreased
nearly 50% globally since 1990rom 543,000
deaths to around 287,000 in 2010.6 The majority o
maternal deaths are concentrated in Countdown
countries in Sub-Saharan Arica and South Asia, an
indication o global disparities in womens access
to needed obstetrical care and other services,
including amily planning and quality antenatal and
postnatal care. Data on a womans lietime risk o
a maternal death accentuate these disparitiesorexample, a woman in Chad has a 1 in 15 chance
o dying rom a maternal cause during her lie
time and a woman rom Aghanistan has a 1 in 32
chance, compared with 1 in 3,800 or a woman in a
developed country.
The maternal mortality ratio and lietime risk
o a maternal death are important measures o
health system unctionality. For every woman
who dies due to a pregnancy or childbirth
complication, approximately 20 others suer
injuries, inection and disabilities. The millions o
women experiencing adverse pregnancy outcomesare a critical marker o the worlds commitment
to improving maternal health and achieving
Millennium Development Goal 5.
Table 1 shows country specic progress towards
Millennium Development Goals 4 and 5, including
estimated under-ve mortality rates and maternal
mortality ratios or 1990, 2000 and 2010; the
average annual rate o reduction or 19902010 or
the two measures; and a summary assessment
o progress. Criteria or judging which countries
are on track to achieve Millennium Development
Goal 4 were developed by the Inter-agencyReerence Group on Child Mortality Estimation
and include three categories (on track, insucient
progress and no progress); criteria or judging
which countries are on track to achieve Millennium
Development Goal 5 were developed by the
Maternal Mortality Estimation Inter-agency Group
and include our categories (on track, making
progress, insucient progress and no progress).
See the ootnote to table 1 or more details on
these criteria.
-
7/28/2019 Countdown to 2015 Maternal Newborn and Child Survival
20/228
Building a Future for Women and Children The 2012 Report14
(continued)
Countries and territories
Under-fve mortality rate Maternal mortality ratio, modelled
Deaths per 1,000live births
Averageannual rate oreduction (%) Assessment
o progressa
Deaths per 100,000live births
Averageannual rate oreduction (%) Assessment
o progressb1990 2000 2010 19902010 1990 2000 2010 19902010
Aghanistan 209 151 149 1.7 Insufcient progress 1,300 1,000 460 5.1 Making progressAngola 243 200 161 2.1 Insufcient progress 1,200 890 450 4.7 Making progress
Azerbaijan 93 67 46 3.5 Insufcient progress 56 65 43 1.3 Insufcient progress
Bangladesh 143 86 48 5.5 On track 800 400 240 5.9 On track
Benin 178 143 115 2.2 Insufcient progress 770 530 350 3.9 Making progress
Bolivia (Plurinational State o) 121 82 54 4.0 On track 450 280 190 4.1 Making progress
Botswana 59 96 48 1.0 Insufcient progress 140 350 160 0.7 No progress
Brazil 59 36 19 5.7 On track 120 81 56 3.5 Making progress
Burkina Faso 205 191 176 0.8 No progress 700 450 300 4.1 Making progress
Burundi 183 164 142 1.3 Insufcient progress 1,100 1,000 800 1.5 Insufcient progress
Cambodia 121 103 51 4.3 On track 830 510 250 5.8 On track
Cameroon 137 148 136 0.0 No progress 670 730 690 0.2 No progress
Central Arican Republic 165 176 159 0.2 No progress 930 1,000 890 0.2 Insufcient progress
Chad 207 190 173 0.9 No progress 920 1,100 1,100 0.7 No progress
China 48 33 18 4.9 On track 120 61 37 5.9 On track
Comoros 125 104 86 1.9 Insufcient progress 440 340 280 2.2 Making progress
Congo 116 104 93 1.1 Insufcient progress 420 540 560 1.5 No progress
Congo, Democratic Republic 181 181 170 0.3 No progress 930 770 540 2.7 Making progress
Cte dIvoire 151 148 123 1.0 Insufcient progress 710 590 400 2.8 Making progress
Djibouti 123 106 91 1.5 Insufcient progress 290 290 200 1.9 Insufcient progress
Egypt 94 47 22 7.3 On track 230 100 66 6.0 On track
Equatorial Guinea 190 152 121 2.3 Insufcient progress 1,200 450 240 7.9 On track
Eritrea 141 93 61 4.2 On track 880 390 240 6.3 On track
Ethiopia 184 141 106 2.8 Insufcient progress 950 700 350 4.9 Making progress
Gabon 93 88 74 1.1 Insufcient progress 270 270 230 0.8 Insufcient progress
Gambia 165 128 98 2.6 Insufcient progress 700 520 360 3.4 Making progress
Ghana 122 99 74 2.5 Insufcient progress 580 550 350 2.6 Making progress
Guatemala 78 49 32 4.5 On track 160 130 120 1.5 Insufcient progressGuinea 229 175 130 2.8 Insufcient progress 1,200 970 610 3.4 Making progress
Guinea-Bissau 210 177 150 1.7 Insufcient progress 1,100 970 790 1.7 Insufcient progress
Haiti 151 109 165 0.4 No progress 620 460 350 2.7 Making progress
India 115 86 63 3.0 Insufcient progress 600 390 200 5.2 Making progress
Indonesia 85 54 35 4.4 On track 600 340 220 4.9 Making progress
Iraq 46 43 39 0.8 On track 89 78 63 1.7 Insufcient progress
Kenya 99 111 85 0.8 No progress 400 490 360 0.5 Insufcient progress
Korea, Democratic Peoples Republic 45 58 33 1.6 On track 97 120 81 0.9 Insufcient progress
Kyrgyzstan 72 52 38 3.2 On track 73 82 71 0.2 Insufcient progress
Lao Peoples Democratic Republic 145 88 54 4.9 On track 1,600 870 470 5.9 On track
Lesotho 89 127 85 0.2 No progress 520 690 620 0.9 No progress
Liberia 227 169 103 4.0 On track 1,200 1,300 770 2.4 Making progress
Madagascar 159 102 62 4.7 On track 640 400 240 4.7 Making progress
Malawi 222 167 92 4.4 On track 1,100 840 460 4.4 Making progress
Mali 255 213 178 1.8 Insufcient progress 1,100 740 540 3.5 Making progress
Mauritania 124 116 111 0.6 No progress 760 630 510 2.0 Making progress
Mexico 49 29 17 5.3 On track 92 82 50 3.0 Making progress
Morocco 86 55 36 4.4 On track 300 170 100 5.1 Making progress
Mozambique 219 177 135 2.4 Insufcient progress 910 710 490 3.1 Making progress
Myanmar 112 87 66 2.6 Insufcient progress 520 300 200 4.8 Making progress
Nepal 141 84 50 5.2 On track 770 360 170 7.3 On track
Table 1
Country progress towards Millennium Development Goals 4 and 5
-
7/28/2019 Countdown to 2015 Maternal Newborn and Child Survival
21/228
Building a Future for Women and Children The 2012 Report
Of74Countdowncountrieswithavailable
data,23areontracktoachieveMillennium
DevelopmentGoal4(gure3).Bangladesh,
Brazil,EgyptandPerureducedtheunder-ve
mortalityrate66%ormore,andChina,Lao
PeoplesDemocraticRepublic,Madagascar,
MexicoandNepalreducedit60%65%.But
muchremainstobedone:13countriesmade
noprogress,and38madeinsufcientprogress.
Countriesandtheirdevelopmentpartnersmust
continueprioritizingchildsurvivaleffortsto
maintainforwardmomentumbeyond2015andto
preventreversals.
Only9of74Countdowncountrieswithavailable
dataareontracktoachieveMillennium
DevelopmentGoal5(gure4).Eightofthem
(Bangladesh,Cambodia,China,Egypt,Eritrea,
LaoPeoplesDemocraticRepublic,Nepaland
Vietnam)arealsoontracktoachieveMillennium
Source:Unde-fve motaity, UNICEF, WHO, Wod Bank and UNDESA 2011; matena motaity, WHO, UNICEF, UNFPA and Wod Bank 2012.
Countries and territories
Under-fve mortality rate Maternal mortality ratio, modelled
Deaths per 1,000live births
Averageannual rate oreduction (%) Assessment
o progressa
Deaths per 100,000live births
Averageannual rate oreduction (%) Assessment
o progressb1990 2000 2010 19902010 1990 2000 2010 19902010
Niger 311 218 143 3.9 Insufcient progress 1,200 870 590 3.6 Making progressNigeria 213 186 143 2.0 Insufcient progress 1,100 970 630 2.6 Making progress
Pakistan 124 101 87 1.8 Insufcient progress 490 380 260 3.0 Making progress
Papua New Guinea 90 74 61 1.9 Insufcient progress 390 310 230 2.6 Making progress
Peru 78 41 19 7.1 On track 200 120 67 5.2 Making progress
Philippines 59 40 29 3.6 On track 170 120 99 2.8 Making progress
Rwanda 163 177 91 2.9 Insufcient progress 910 840 340 4.9 Making progress
So Tom and Prncipe 94 87 80 0.8 No progress 150 110 70 3.8 Making progress
Senegal 139 119 75 3.1 Insufcient progress 670 500 370 3.0 Making progress
Sierra Leone 276 233 174 2.3 Insufcient progress 1,300 1,300 890 1.8 Insufcient progress
Solomon Islands 45 35 27 2.6 On track 150 120 93 2.2 Making progress
Somalia 180 180 180 0.0 No progress 890 1,000 1,000 0.7 No progress
South Arica 60 78 57 0.3 No progress 250 330 300 0.9 No progress
Sudanc 125 114 103 1.0 Insufcient progress 1,000 870 730 1.6 Insufcient progress
Swaziland 96 114 78 1.0 Insufcient progress 300 360 320 0.3 No progress
Tajikistan 116 93 63 3.1 Insufcient progress 94 120 65 1.8 Insufcient progress
Tanzania, United Republic o 155 130 76 3.6 Insufcient progress 870 730 460 3.2 Making progress
Togo 147 124 103 1.8 Insufcient progress 620 440 300 3.5 Making progress
Turkmenistan 98 74 56 2.8 Insufcient progress 82 91 67 1.0 Insufcient progress
Uganda 175 144 99 2.8 Insufcient progress 600 530 310 3.2 Making progress
Uzbekistan 77 63 52 2.0 Insufcient progress 59 33 28 3.7 Making progress
Viet Nam 51 35 23 4.0 On track 240 100 59 6.9 On track
Yemen 128 100 77 2.5 Insufcient progress 610 380 200 5.3 Making progress
Zambia 183 157 111 2.5 Insufcient progress 470 540 440 0.4 Insufcient progress
Zimbabwe 78 115 80 0.1 No progress 450 640 570 1.2 No progress
a. On tack indicates that the unde-fve motaity ate o 2010 is ess than 40 deaths pe 1,000 ive biths o that it is 40 o moe with an aveage annua ate
o eduction o 4% o highe o 19902010; insufcient pogess indicates that the unde-fve motaity ate o 2010 is 40 deaths pe 1,000 ive biths o
moe with an aveage annua ate o eduction o 1%3.9% o 19902010; no pogess indicates that the unde-fve motaity ate o 2010 is 40 deaths pe
1,000 ive biths o moe with an aveage annua ate o eduction o ess than 1% o 19902010.
b. On tack indicates that the aveage annua ate o eduction o the matena motaity atio o 19902010 is 5.5% o moe; making pogess indicates
that the aveage annua ate o eduction o the matena motaity atio o 19902010 is between 2% and 5.5%; insufcient pogess indicates that the
aveage annua ate o eduction o the matena motaity atio o 19902010 is ess than 2%; no pogess indicates that the aveage annua ate o eduction
o the matena motaity atio o 1990 2010 is negativethat is, that the matena motaity atio has inceased. Counties with a matena motaity atio
beow 100 deaths pe 100,00 0 ive biths in 1990 ae not categoized by the Matena Motait y Estimation Inte-agency Goup. Countdown to 2015cacuated
the assessment o pogess o Countdown counties that a into this goup.
c. Data ee to Sudan as it was constituted in 2010, beoe South Sudan seceded. Data o South Sudan and Sudan as sepaate states ae not avaiabe.
TABlE 1 (CONTINUED)
Country progress towards Millennium Development Goals 4 and 5
-
7/28/2019 Countdown to 2015 Maternal Newborn and Child Survival
22/228
Building a Future for Women and Children The 2012 Report16
DevelopmentGoal4.Onlythreecountries
(EquatorialGuinea,NepalandVietnam)reduced
themodelledmaternalmortalityratio75%ormore
from1990to2010,thoughCambodia,Bangladesh,
Egypt,EritreaandLaoPeoplesDemocratic
Republiccameclose,reducingit70%74%.
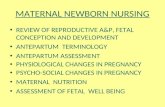
Causes of child deaths
Newanalysesfor2010showthat64%ofchild
deathsareattributabletoinfectiousdiseasesin
newbornsandchildren,and40%occurduring
theneonatalperiod(gure5).Undernutrition
contributestooverathirdofchilddeaths.7The
leadingcausesofneonataldeathsarecomplications
ofpretermbirth(box 5),intrapartum-relatedevents,
andsepsisandmeningitis;theleadingcausesof
deathamongolderchildrenremainpneumonia,
diarrhoea(box6)andmalaria(31%).
Causes of maternal deaths
Haemorrhageandhypertensiontogetheraccount
formorethanhalfofmaternaldeathsdeaths
ofwomenwhilepregnantorwithin42daysof
terminationofpregnancy,regardlessofthesiteor
durationofpregnancy,fromanycauserelatedtoor
aggravatedbythepregnancyoritsmanagement
andsepsisandunsafeabortion(box7)combined
accountfor17%(gure6).Indirectcauses,
includingdeathsduetoconditionssuchasmalaria,
HIV/AIDSandcardiacdiseases,accountfor
about20%.Indirectmaternaldeathsattributable
toAIDSin15CountdowncountrieswithHIV
prevalenceabove5%rangesfrom8%to67%,
withamedianof27%.8Thecategoriesofmaternal
deathsarebasedonaWHOclassicationsystem
thatconsidersobstructedlabourandanaemia
tobecontributingconditionsratherthandirect
causes.Deathsrelatedtothesetwoconditions
areclassiedunderhaemorrhageorsepsis.Clear
programmaticactionslinkedtoobstructedlabour
FIGUrE 3
Progress towards Millennium DevelopmentGoal 4 in Countdowncountries
Source:Countdown to 2015anaysis based on UNICEF, WHO, Wod
Bank and UNDESA 2011.
0
10
20
30
40
Overall progress as of 2010
Number of Countdown countries
On track Insufficientprogress
No progress
FIGUrE 4
Progress towards Millennium DevelopmentGoal 5 in Countdowncountries
Source:Countdown to 2015anaysis based on WHO, UNICEF, UNFPA
and Wod Bank 2012.
0
10
20
30
40
Overall progress as of 2010
Number of Countdown countries
On track Makingprogress
Insufficientprogress
No progress
9
40
16
9
FIGUrE 5
Roughly 40% of child deaths occur duringthe neonatal period
Source:liu and othes othcoming.
Global causes of death among children ages 059 months, 2010
Diarrhoea
10%
Measles 1%
Diarrhoea, neonatal 1%
Tetanus 1%
Pneumonia 14%Preterm birth
complications 14%
Intrapartum-
related events9%
Other
non-neonatal18%
Malaria 7%
Sepsis and
meningitis 5%
Congenitalabnormalities 4%
Injury 5%
AIDS 2%
Meningitis 2%
Other neonatal 2%
Pneumonia, neonatal 4%
Neonatal
40%
Neonatal
40%
-
7/28/2019 Countdown to 2015 Maternal Newborn and Child Survival
23/228
Building a Future for Women and Children The 2012 Report
(continued)
Preterm births and stibirths have been verked
n the gba heath agenda. Countdown is reprting
preterm birth estimates and stibirth rates r the
rst time t raise their visibiity and prmte their
priritizatin r actin. Many the interventins r
preventing preterm births and stibirths are eective
in imprving ther materna and newbrn heath
utcmes.
15 million preterm births a year
Preterm birth cmpicatins are the eading cause
newbrn deaths and the secnd-eading cause
deaths in chidren under age 5. Mre than 1.1 miin
chidren a year die due t cmpicatins being brn
t sn,1 and many thers eperience a ietime
disabiity.2
Apprimatey 80% preterm births ccurbetween 32 and 37 weeks gestatins, and mst
these babies survive when they receive essentia
newbrn care; 75% deaths preterm babies can
be prevented withut intensive care.
Accrding t the rst natina estimates preterm
birth (bere 37 cmpeted weeks pregnancy),
apprimatey 14.9 miin babies a yearmre than
1 in 10are brn t sn.o the 65 cuntries in
the wrd with reiabe trend data, ny 3 have shwn
substantia reductins ver 19902010. Abut 84%
a preterm births ccur in Countdown cuntries. The
preterm birth rate in Countdown cuntries ranges rm7% in Papua New Guinea and Iraq t 18% in Maawi,
with a median 12%.
There is a stark surviva and care gap r premature
babies between w- and high-incme cuntries.
Yet many preterm babies can be saved thrugh
easibe, w-cst interventins such as breasteeding
supprt, therma care and basic care r inectins
and breathing dicuties. An anaysis using the lives
Saved T und that universa cverage kangar
mther care cud prevent 450,000 deaths a year
ane.3 Nurses, midwives and cmmunity-based
wrkers prviding pstnata care need training in
kangar mther care, breasteeding supprt and
ther preterm baby care skis as we as access t
reiabe suppies key cmmdities and equipment.
Eective care bere, during and between pregnancies
and chidbirth is as imprtant r preventing preterm
births and imprving the surviva chances preterm
babies. Antenata crticsterid injectins, a pririty
medicine the United Natins Cmmissin n
lie-Saving Cmmdities r Wmen and Chidren,
deivered t wmen in preterm abur, reduce the risk
death and respiratry distress in preterm babies.
Cverage antenata crticsterids is w in the ew
Countdown cuntries with estimates. Scaing up t
universa cverage acrss Countdown cuntries cud
save an estimated 400,000 preterm babies a year.
Investment in research is essentia r better
understanding the causes preterm birth in rder
t devep preventive interventins r universa
appicatin. Research t imprve impementatin
prven interventins in w-resurce settings
and n w-cst techngica sutins t address
cmpicatins prematurity is needed.
The May 2012 Born Too Soon: The Global Action
Report on Preterm Births3supprted by Countdown
and arund 50 rganizatinssets a new ga
having deaths due t preterm birth by 2025.
Almost 3 million stillbirths a year
An estimated 2.7 miin third-trimester stibirths ccur
every year, a drp 1.1% a year ver 1995-2009.
Countdown cuntries accunted r 93% stibirths
in the 193 cuntries with data r 2009, with rates
ranging rm 5 per 1,000 tta births in Meic t 47 in
Pakistan and a median 23.
Wrdwide, apprimatey 1.2 miin stibirths
ccur during abur; these are knwn as intrapartum
stibirths. The risk intrapartum stibirth is 24 times
higher r an Arican wman than r a wman in a
high-incme cuntry. Yet these deaths are argey
preventabe. The mst imprtant strategy t reduce
stibirths is imprved care at birth, which as saves
materna and newbrn ives, giving a tripe return
n investments in training skied birth attendants
and increasing the number unctina basic and
cmprehensive emergency bstetric care aciities.4
other interventins prven t reduce stibirths are
amiy panning, supprtive picies prtecting wmen
rm harmu wrking cnditins and epsure t
envirnmenta tins (such as indr air putin rm
ckstves and tbacc smke) and quaity antenata
care services (such as eary recgnitin and treatment
intrauterine grwth restrictin; prtectin rm maaria
Box 5
Preterm births and stillbirths: making them count
-
7/28/2019 Countdown to 2015 Maternal Newborn and Child Survival
24/228
Building a Future for Women and Children The 2012 Report18
thrugh insecticide-treated net use and deivery
intermittent preventive treatment r pregnant wmen;
and identicatin and treatment hypertensin,
diabetes and seuay transmitted diseases, particuary
syphiis). Stibirths can as be reduced by inducing
pst-term pregnancies (at 41 weeks and ater) and
by cnducting newbrn resuscitatin. Scaing up
eective care, especiay quaity chidbirth services,
cud have stibirth rates by 2020.5
Notes
1. liu and thers rthcming.
2. Bencwe and thers rthcming.
3. March Dimes, PMNCH, Save the Chidren and WHo 2012.
4. lawn and thers 2011; Bhutta and thers 2011.
5. Pattinsn and thers 2011.
Box 5 (CoNTINUED)
Preterm births and stillbirths: making them count
Source:UNICEF rthcming.
Accrding t UNICEFs (rthcming) Pneumonia and
Diarrhoea: Tackling the Deadliest Diseases or the
Worlds Poorest Children, ewer chidren under age
5 are dying due t pneumnia and diarrhea than a
decade ag. Hwever, these tw diseases cmbined
sti accunt r cse t 2 miin deaths a year. o
the 7.6 miin deaths amng chidren under age 5 in
2010 (incuding nenata deaths), 18% were due t
pneumnia and 11% t diarrhea (see gure 5 in the
main tet). Apprimatey 90% these deaths were
in Sub-Saharan Arica and Suth Asia, and the ve
cuntries with the mst deaths are a Countdowncuntries: India, Pakistan, Nigeria, Demcratic Repubic
the Cng and Ethipia.
Preventive interventins, sme which reduce
the incidence bth diseases, incude ptima
breasteeding practices and adequate nutritin,
immunizatins, hand washing with sap and access
t imprved water and sanitatin aciities. liesaving
treatment ptins ater a chid gets sick incude
antibitics r bacteria pneumnia and ra rehydratin
sats and zinc r diarrhea. Hwever, cverage
these interventins remains w, particuary amng
the mst vunerabe.
In Countdown cuntries the median cverage
ecusive breasteeding (r the rst si mnths
ie), antibitic use r pneumnia and ra
rehydratin therapy with cntinued eeding are a
ess than 50% (see gure 9 in the main tet). ony
39 Countdown cuntries have picies r cmmunity
case management pneumnia that cud epand
treatment access t the underserved (see gure 15
in the main reprt). Athugh the number cuntries
adpting picies n w-smarity ra rehydratin
sats and zinc r managing diarrhea is increasing,
zinc treatment remains unavaiabe in neary a third
Countdown cuntries. Median cverage access
t an imprved water surce is 76% in Countdown
cuntries, but access t an imprved sanitatin aciityhvers at an unacceptabe 40%. Mst Countdown
cuntries reprt high cverage meases and
Haemophilus infuenzaetype b vaccines, but ny 9 are
impementing picies r rtavirus vaccine and 16 r
pneumccca cnjugate vaccines. Epanding vaccine
uptake is essentia t reaize the u ptentia these
interventins in reducing deaths due t pneumnia and
diarrhea, particuary as vaccines against rtavirus and
pneumcccus are being intrduced in mre cuntries.
A gba actin pan r pneumnia has been in pace
since 2009. A cnsrtium partners incuding
academic universities, UN agencies and the Cintn
Heath Access Initiative is deveping an integrated
gba actin pan r diarrhea and pneumnia t scae
up prven interventins and increase cmmitment t
addressing these tw eading kiers chidren.
Box 6
Pneumonia and diarrhoea: neglected killers
-
7/28/2019 Countdown to 2015 Maternal Newborn and Child Survival
25/228
Building a Future for Women and Children The 2012 Report
(continued)
Wrdwide apprimatey 22 miin unsae abrtins,
ha a induced abrtins, ccur each year, resuting
in the deaths 47,000 wmen and temprary r
permanent disabiity amng an additina 5 miin
wmen. Amst a these deaths and disabiities
ccur in deveping cuntries.1 An abrtin is dened
as unsae when perrmed by an individua wh
acks the necessary skis r in an envirnment that
des nt meet minima medica standards. Deaths
due t unsae abrtin resut mainy rm severe
inectins, beeding and rgan damage caused by
the prcedure. Preventing unsae abrtins wud
cntribute substantiay twards achieving Miennium
Devepment Ga 5.
Countdown cuntries represent a wide spectrum
pubic heath cnsequences unsae abrtin,ranging rm itte r nne in sme cuntries (Centra
and Sutheast Asian cuntries and thse in Far East
Asia) t abut 1 in 5 materna deaths due t unsae
abrtin in Countdown cuntries in East Arica (see
map). In genera, materna deaths due t unsae
abrtins are high in Countdown cuntries with high
vera materna mrtaity.
Gbay the abrtin rate e between 1995 and 2003
rm 35 per 1,000 wmen reprductive age (ages
1544) t 29 but has since stagnated at 28 in 2008.
over 2003-2008 the tta number abrtins rse,
refecting increased gba ppuatin. The prprtin
abrtins that were unsae increased rm 44% in
1995 t 49% in 2008.2
Mre than 80% unintended pregnancies in
deveping cuntries ccur t wmen wh have an
unmet need r mdern cntraceptin. Given the
etent unintended pregnancy and the high eves
unsae abrtin arund the wrd, cntinuing
erts t prvide amiy panning services (see b
9), educatin and inrmatin t prevent unsae
abrtins are essentia pubic heath interventins.3
Eective, high-quaity amiy panning services arecharacterized by a variety ardabe cmmdities,
cmpete inrmatin r wmen abut ptentia
benets and side eects and attentin t scia
and cutura actrs t epand wmens access t
cntraceptin.4 WHo estimates that 75% unsae
abrtins cud be avided i the need r amiy
panning were uy met.5
Unsae abortions are concentrated in Latin America and the Caribbean and Central Arica
Unsafe abortions
per 1,000 women
ages 154430 or more
2029
1019
19
None or negligible
Source:WHo 2008.
Box 7
Unsae abortion: a preventable cause o maternal deaths
-
7/28/2019 Countdown to 2015 Maternal Newborn and Child Survival
26/228
Building a Future for Women and Children The 2012 Report20
and anaemia include increasing womens accessto comprehensive emergency obstetric care and
nutrition interventions, respectively.
Undernutrition: grave crisisa call or action
Undernutrition contributes to over a third o
child deaths globally.9 The result o inadequate
energy or micronutrient intake and oten rooted in
poverty, undernutrition increases the risk o death
and ill-health or both mother and baby during
pregnancy, childbirth and the postnatal period
through early childhood. Stunting prevalence is
a critical indicator o progress in child survival,
refecting long-term exposure to poor health and
nutrition, especially in the rst two years o lie.10
Children under age 5 around the world have the
same growth potential, and stunting prevalence
above 3% indicates the need or remedial actions.
a. Incudes deaths due t bstructed abur r anaemia.
b. Neary a (99%) abrtin deaths are due t unsae abrtin.
Source:Preiminary data rm the Wrd Heath organizatin.
Global estimates of the causes of maternal deaths, 19972007
Haemorrhagea
35%
Hypertension18%
Sepsisa
8%Unsafe
abortionb
9%
Embolism 1%
Other direct11%
Indirect18%
FIGURE 6
Haemorrhage and hypertension accountor more than hal o maternal deaths
As stated by the Inter-Agency Grup r Sae
Mtherhd, Unsae abrtin is the mst
negectedand mst preventabecause materna
death. These deaths can be signicanty reduced by
ensuring that [materna heath] prgrammes incude
cient-centered amiy panning services t prevent
unwanted pregnancy, cntraceptive cunseing r
wmen wh have had an induced abrtin, the use
apprpriate techngies r wmen wh eperience
abrtin cmpicatins, and, where nt against the
aw, sae services r pregnancy terminatin.6
Where unsae abrtins ccur, cmprehensive pst-
abrtin care r wmen is imprtant t address
cmpicatins and ensure access t cntraceptin.
Skied heath wrkers, apprpriate pain cntr
management, w-up care incuding identicatin
and treatment beeding r inectin, remving
heath wrker stigma r caring r wmen ater an
abrtin, and increasing and imprving amiy panning
cunseing and services are a necessary cmpnents.7
Notes
1. Wrd Heath organizatin 2011.
2. Sedgh and thers 2012.
3. WHo 2005.
4. WHo 2009.
5. WHo 2011.
6. Inter-Agency Grup r Sae Mtherhd 1998.
7. Singh and thers 2009.
Box 7 (CoNTINUED)
Unsae abortion: a preventable cause o maternal deaths
FIGURE 7
Two-thirds o Countdowncountries havestunting prevalence o 30% or more
Source:UNICEF gba databases, Apri 2012, based n Demgraphic
and Heath Surveys, Mutipe Indicatr Custer Surveys and ther
husehd surveys
0
5
10
15
20
25
50%
or more
40%
49%
30%
39%
20%
29%
5%
19%
Less
than 5%
Number of Countdown countries (n = 63)
Prevalence of stunting, 20062010
-
7/28/2019 Countdown to 2015 Maternal Newborn and Child Survival
27/228
Building a Future for Women and Children The 2012 Report
All 63 Countdowncountries with available data
since 2006 have stunting prevalence above this
threshold (gure 7). In the majority o these
countries more than a third o children are
stunted, a situation requiring urgent attention, and
prevalence is particularly high among the poorest
populations (gure 8). In a th o these countries
more than hal o children in the poorest 20% o
households are stunted. Multisectoral programmes
that emphasize reaching the poor must continue to
be a major priority in Countdowncountries.
Wasting, or low weight or height, in children
under age 5, is the most reliable indicator o
acute ood insecurity and signals an urgent need
or action. The short-term mortality risk is much
higher or a wasted child than or a stunted child.
In 62 Countdowncountries with available data
since 2006 the prevalence o wasting ranges rom
0.8% in Swaziland to 21% in the last survey in
pre-secession Sudan, with a median o 7%. Niger
(16%), Chad (16%), Bangladesh (18%) and India
(20%) also have high prevalence o wasting. The
median prevalence is 10% in the nine Countdown
countries in the Sahel region prone to severe
drought and amine.
Maternal undernutrition is a risk actor or poor
maternal, newborn and child health outcomes,
and interventions to improve womens nutritionalstatus beore, during, ater and between
pregnancies are essential (box 8). The Scale
Up Nutrition road map, the Global Alliance or
Improved Nutrition, the Renewed Eorts Against
Child Hunger, the U.S. and Irishled 1,000 days:
Change a Lie, Change the Future campaign
and similar initiatives are under way to address
maternal and child undernutrition;11 the challenge
is to ensure that these are ully integrated with
country-level reproductive, maternal, newborn and
child health programmes.12
FIGURE 8
Poorer children are more likely to be stunted
Source:Demgraphic and Heath Surveys and Mutipe Indicatr
Custer Surveys
0
10
20
30
40
50
Median prevlance of stunting by wealth quintile,Countdown countries with data (%)
Poorest Second Middle Fourth Richest
42 42
36
32
25
-
7/28/2019 Countdown to 2015 Maternal Newborn and Child Survival
28/228
Building a Future for Women and Children The 2012 Report22
Key indicatrs materna nutritin are materna
stature, bdy mass inde and micrnutrient deciency.
Pr materna nutritin cntributes t at east 20%
materna deaths, and increases the prbabiity
ther pr pregnancy utcmes, incuding newbrn
deaths.1 Materna undernutritin is particuary severe
in Suth Asian Countdown cuntries. In Pakistan, r
eampe, mre than 25% wmen ages 1519 have
a w bdy mass inde (bew 18.5 kigrams per
square metre) and 10% had shrt stature (ess than
145 centimetres).2
In this reprt Countdown tracks r the rst time the
prevaence w bdy mass inde amng wmen
reprductive age, an imprtant risk actr r intrauterine
grwth restrictin, w birthweight and nenata
mrtaity. less data are avaiabe n the nutritina status wmen than n the nutritina status chidren. In
24 Countdown cuntries with a recent Demgraphic and
Heath Survey the median prevaence w bdy mass
inde amng wmen reprductive age is 11%, with
a w 0.7% in Egypt. Fur cuntries reprt etremey
high prevaence: Nepa (26%), Madagascar (28%),
Bangadesh (33%) and India (40%).
Shrt materna stature, ten a resut chidhd
stunting, is as a risk actr r bstructed abur and
caesarean deivery due t a disprprtin between
the babys head and the materna pevis. Prnged
bstructed abur cmbined with n r deayedaccess t caesarean deivery can resut in materna
mrtaity, debiitating ng-term heath cnsequences
such as bstetric stua and nenata mrtaity due
t birth asphyia. Many Countdown cuntries with
high materna undernutritin as ack readiy avaiabe
emergency caesarean sectins.
limited inrmatin is avaiabe n materna
micrnutrient deciencies. A WHo review natinay
representative surveys rm 1993 t 2005 und that
42% pregnant wmen wrdwide are anaemic,
mre than ha them due t irn deciency.2
Prenata ic acid deciency, as widespread, is
assciated with increased risk neura tube deects.
Further research is needed t understand the
reatinships between materna undernutritin
and shrt- and ng-term materna and chid heathutcmes. Mre and better data are as needed
n measures materna nutritina status and n
cverage evidence-based interventins, incuding
ic acid suppementatin in the pericnceptina
perid, irn and ic acid uptake amng wmen at risk
irn deciency anaemia and nutritin prgrammes
t address d insecurity and w materna bdy
mass inde.
Notes
1. Back and thers 2008; Sttzus, Muany and Back 2004.
2. Zugar A. Bhutta and thers, Aga Khan University, Natina
Nutritin Survey, Pakistan, 2011.
3. WHo and CDC 2008.
Box 8
A new ocus on maternal undernutrition
-
7/28/2019 Countdown to 2015 Maternal Newborn and Child Survival
29/228
Building a Future for Women and Children The 2012 Report
Coverage along thecontinuum of care
This section presents levels and trends in the
Countdowncoverage indicators, including
measures o equity in coverage. It reviews the
number o countries with coverage data available
or Countdownindicators, discusses new
indicators included or the rst time in 2012 and
summarizes coverage trends since 2000.
Figure 9 shows median coverage values basedon the latest available estimates since 2006 or
21 Countdown indicators. Table 2 shows the
number o countries with available data or
each Countdown indicator, the median coverage
values and the range in coverage across reporting
countries. Figure 9 and table 2 do not include the
caesarean section rate, prevention o mother-to-
child transmission o HIV and eligible HIV-positive
pregnant women receiving antiretroviral treatment
or their own health, which are reported on
separately.
New coverage indicators or 2012 refect
advancements in amily planning and inant
eeding: demand or amily planning satised (anindicator o met need or amily planning; box 9)
and introduction o solid or semisolid oods.
Coverage is reported both or the compound
measure o oral rehydration therapy with
continued eeding and or oral rehydration salts
alone. Inormation on oral rehydration salts use
Figure 9
Coverage of interventions varies across the continuum of care
a. Data a fo 2010.
b. Analyss s basd on conts wth 75% o mo of th poplaton at sk of p. falciparum tansmsson.
Source:immnzaton ats, WHO and uNiCeF; postnatal vst fo moth, Savn Nwbon Lvs analyss of Dmoaphc and Halth Svys;
mpovd wat and santaton, WHO and uNiCeF Jont Monton Poamm 2012; all oth ndcatos, uNiCeF lobal databass, Apl 2012, basd on
Dmoaphc and Halth Svys, Mltpl indcato Clst Svys and oth natonal svys.
0
25
50
75
100
Median national coverage of selected Countdown interventions, most recent year since 2006 (%)
Pregnancy Birth Postnatal Infancy Childhood Water and
sanitation
Pre-
pregnancy
Improvedsanitation
facilities
Improved
drinking
watersources
Oralrehydrationsalts
Malariatreatment
(first-lineantimalarial)b
Antibioticsforpn
eumonia
Careseekingforpn
eumonia
Childrensleepingunder
insecticide-treatednetsb
VitaminAsupplem
entation
(tw
odoses)
Haemophilusinfluenzaetypeb
immunization(threedoses)a
Measlesimmu
nizationa
DTP3immu
nizationa
Introduction
ofsolid,
semisolidors
oftfoods
Exclusivebrea
steeding
(forfirstsix
months)
Postnatalvisitfo
rmother
Early
initiation
ofbreastfeeding
Skilledattendan
tatbirth
Neonataltetanusp
rotection
Intermittentpreventive
treatmento
fmalaria
forpregnantwomen
Antenatalcare
(atleastfo
urvisits)
Antenatalcare
(atleastonevisit)
Demandforfamily
planning
satisfied
-
7/28/2019 Countdown to 2015 Maternal Newborn and Child Survival
30/228
Building a Future for Women and Children The 2012 Report24
alone has considerable programme relevance but
is not captured in the oral rehydration therapy with
continued eeding measure.
These results demonstrate what is possible. All
our vaccines (neonatal tetanus protection, DTP3,
measles and Haemophilius infuenzaetype b
[three doses]) and vitamin A supplementation (two
doses) have median coverage o 80% or more in
Countdowncountries with available data. In most
Countdowncountries vaccines and vitamin A
are provided in health acilities as well as during
campaigns such as child health days, when outreach
teams can reach a high proportion o the population.
Median coverage o at least one antenatal visit is
also very high, at 88%, but coverage o our or more
antenatal visits is only 55%.
At least one country has achieved coverage
above 80% or each o 17 interventions, and
at least one country has reached coverage o
70%80% or each o our other interventions
(postnatal visit or baby, exclusive breasteeding,
children sleeping under insecticide-treated nets
and diarrhoea treatment with oral rehydration
salts). For intermittent preventive treatment o
malaria or pregnant women and oral rehydration
therapy with continued eeding coverage is
below 70% in the highest perorming country.
Substantial progress is still needed. The median
coverage o interventions related to case
management o childhood illnesses, demand
or amily planning satisfed, early initiation o
breasteeding and exclusive breasteeding hover
at or below 50%.
a. Numer o countries is ased on the 50 countries with 75% or more o the popuation at risk o p. aciparum transmission.
. Not isted in fgure 9.
Source:UNICEF goa dataases, Apri 2012, ased on Demographic and Heath Surveys, Mutipe Indicator Custer Surveys and other nationa surveys.
IndicatorNumber of countries
with dataMedian coverage
(%)Range
(%)
Pre-pregnancy
Demand or amily planning satisfed 46 56 1797
Pregnancy
Antenatal care (at least one visit) 69 88 26100Antenatal care (at least our visits) 49 55 697
Intermittent preventive treatment o malaria or pregnant womena 39 13 069
Neonatal tetanus protection 66 85 6094
Birth
Skilled attendant at birth 67 57 10100
Postnatal
Early initiation o breasteeding 55 46 1881
Postnatal visit or mother 22 41 2287
Postnatal visit or babyb 4 50 877
Inancy
Exclusive breasteeding 57 37 174
Introduction o solid, semisolid or sot oods 39 73 1694
Diphtheria-tetanus-pertussis (three doses) 74 85 3399
Measles immunization 73 84 4699
Haemophilius infuenzaetype b immunization (three doses) 58 83 4599
Vitamin A supplementation (two doses) 56 92 0100
Childhood
Children sleeping under insecticide-treated nets a 36 34 370
Careseeking or pneumonia 57 55 1383
Antibiotic treatment or pneumonia 45 39 388
Malaria treatment (frst-line antimalarial)a 31 25 091
Oral rehydration therapy with continued eedingb 53 45 768
Oral rehydration salts 57 33 1077
Water and sanitation
Improved drinking water sources (total) 70 76 2999
Improved sanitation acilities (total) 71 40 9100
TAblE 2
National coverage of Countdowninterventio