Costa Et Al. 2010 - IJTR - Commentary on Behaviour of the Muscle-tendon Unit During Static...
12
132 International JournaloTherapyandRehabilitation,March2010,Vol17,No3 Research S tretching exercises are commonly under- taken in sports and rehabilitation set- tings. Among the benets o stretching o human musculoskeletal structures are injury prevention, and improved perormance by regaining joint range o motion (Hortobagyi et al, 1985; Taylor et al, 1990; Wilson et al, 1991; Witvrouw et al, 2004). Similarly, in physical therapy, stretching is one o the most eective techniques used or lengthening shortened mus- cles, and improvement o joint range o motion (Ylinen, 2008). To determine the most eective stretching method and optimal stretching time, an under- standing o the response to stretching o the muscle-tendon unit in various states is required. The reaction o a healthy muscle-tendon unit to stretching has been previously examined in healthy adults (Herbert et al, 2002; Kubo et al, 2005; Morse et al, 2008). Herbert et al (2002) measured changes in length o muscle ascicles in relaxed human gastrocnemius muscle during passively imposed changes in joint angle. They Behaviourothemuscle- tendonunitduringstatic stretchingollowingunloading reported that in gastrocnemius, which has rela- tively long tendons, only 27% o the total change in muscle-tendon length was transmitted to the muscle ascicles. Kubo et al (2005) showed that while the muscle ascicles, tendon and apone- urosis stretched during passive dorsifexion o the ankle joint, the elongation o the tendon was signicantly greater than that o the aponeuro- sis. Morse et al (2008) reported that the muscle- tendon unit length increased by 21.9 mm during stretching. However, the reaction to stretching o an unhealthy muscle-tendon unit, such as in muscle injuries including muscle strain, muscle tendon atrophy , or unloading, is largely unknown. The aims o the present study were to inves- tigate the reaction o the muscle-tendon unit to stretching ater a period o non-weight-bearing, compared with that o a healthy muscle-tendon unit, and to quantiy, using ultrasonograms, the displacement o the ascicle-deep aponeurosis junction (DA) and the myotendinous junction (MTJ) during stretching o the medial head o the gastrocnemius muscle. Aims: To determine the amount o displacement in the muscle-tendon unit o the medial head o the human gastrocnemius muscle during static stretching, ater a period o non-weight-bearing ollowing injury. Methods: Twenty emale patients with a unilateral lower leg injury participated in this study ( N = 13 ollowing ankle racture-dislocation; N = 7 ollowing racture o the tibiofbula). The dierence in displacement o the junction o the ascicle and the deep aponeurosis junction (DA) at ¼ proximal height o the lower leg and that o the myotendinous junction (MTJ) between the injured and uninjured leg was measured using ultrasonograms and analyzed by two way analysis o variance or repeated measures and paired t-tests. Findings: Initially , DA displacement was larger, and MTJ displacement was smaller, in the injured compared with the uninjured leg. Ater treatment, DA and MTJ displacements in the injured leg approached levels o the uninjured leg. At all time points, DA and MTJ displaced distally during the frst three minutes o stretching in both legs ( P < 0.01). Conclusions: Following a non-weight-bearing period, ascicles and tendon may be excessively extended. Recovery o the muscle tendon complex might be accelerated by applying exercises aimed at attaining increased extensibility o the aponeurotic tissue. Keywords: nmuscle-tendonunit nrehabilitation nstretching nunloading Submitted 7 August 2009, sent back or revisions 1 October 2009; accepted or publication ollowing double-blind peer review 3 December 2009 Hiroshi Kanazawa, Yukio Urabe, Taizan Shirakawa Hiroshi Kanazawa is Senior Physiotherapist, Director o Department o Rehabilitation, Department o Rehabilitation, Matterhorn Rehabilit ation Hospital, and Doctorate Student, Graduate School o Health Sciences, Hiroshima University, Hiroshima; Yukio Urabe is Proessor, Graduate School o Health Sciences, Hiroshima University, Hiroshima ; and Taizan Shirakawa is Senior Orthopedic Surgeon, President o Matterhorn Rehabilitation Hospital, Matterhorn Rehabilitation Hospital, Hiroshima, Japan Correspondence to: H Kanazawa E-mail: kanah@mbe. ocn.ne.jp
Transcript of Costa Et Al. 2010 - IJTR - Commentary on Behaviour of the Muscle-tendon Unit During Static...

8/8/2019 Costa Et Al. 2010 - IJTR - Commentary on Behaviour of the Muscle-tendon Unit During Static Stretching Following U…
http://slidepdf.com/reader/full/costa-et-al-2010-ijtr-commentary-on-behaviour-of-the-muscle-tendon-unit 1/11
132 InternationalJournaloTherapyandRehabilitation,March2010,Vol17,No3
Research
Stretching exercises are commonly under-
taken in sports and rehabilitation set-
tings. Among the benets o stretching
o human musculoskeletal structures are
injury prevention, and improved perormance by
regaining joint range o motion (Hortobagyi et
al, 1985; Taylor et al, 1990; Wilson et al, 1991;
Witvrouw et al, 2004). Similarly, in physical
therapy, stretching is one o the most eective
techniques used or lengthening shortened mus-cles, and improvement o joint range o motion
(Ylinen, 2008).
To determine the most eective stretching
method and optimal stretching time, an under-
standing o the response to stretching o the
muscle-tendon unit in various states is required.
The reaction o a healthy muscle-tendon unit
to stretching has been previously examined in
healthy adults (Herbert et al, 2002; Kubo et al,
2005; Morse et al, 2008). Herbert et al (2002)
measured changes in length o muscle ascicles
in relaxed human gastrocnemius muscle during
passively imposed changes in joint angle. They
Behaviourothemuscle-tendonunitduringstatic
stretchingollowingunloading
reported that in gastrocnemius, which has rela-
tively long tendons, only 27% o the total change
in muscle-tendon length was transmitted to the
muscle ascicles. Kubo et al (2005) showed that
while the muscle ascicles, tendon and apone-
urosis stretched during passive dorsifexion o
the ankle joint, the elongation o the tendon was
signicantly greater than that o the aponeuro-
sis. Morse et al (2008) reported that the muscle-
tendon unit length increased by 21.9 mm duringstretching. However, the reaction to stretching
o an unhealthy muscle-tendon unit, such as in
muscle injuries including muscle strain, muscle
tendon atrophy, or unloading, is largely unknown.
The aims o the present study were to inves-
tigate the reaction o the muscle-tendon unit to
stretching ater a period o non-weight-bearing,
compared with that o a healthy muscle-tendon
unit, and to quantiy, using ultrasonograms, the
displacement o the ascicle-deep aponeurosis
junction (DA) and the myotendinous junction
(MTJ) during stretching o the medial head o the
gastrocnemius muscle.
Aims: To determine the amount o displacement in the muscle-tendon unit o the medial head o the
human gastrocnemius muscle during static stretching, ater a period o non-weight-bearing ollowing injury.
Methods: Twenty emale patients with a unilateral lower leg injury participated in this study ( N= 13
ollowing ankle racture-dislocation; N= 7 ollowing racture o the tibiofbula). The dierence in
displacement o the junction o the ascicle and the deep aponeurosis junction (DA) at ¼ proximal
height o the lower leg and that o the myotendinous junction (MTJ) between the injured and
uninjured leg was measured using ultrasonograms and analyzed by two way analysis o variance or
repeated measures and paired t-tests.
Findings: Initially, DA displacement was larger, and MTJ displacement was smaller, in the injured
compared with the uninjured leg. Ater treatment, DA and MTJ displacements in the injured leg
approached levels o the uninjured leg. At all time points, DA and MTJ displaced distally during the
frst three minutes o stretching in both legs ( P < 0.01).
Conclusions: Following a non-weight-bearing period, ascicles and tendon may be excessively
extended. Recovery o the muscle tendon complex might be accelerated by applying exercises aimed
at attaining increased extensibility o the aponeurotic tissue.
Keywords:nmuscle-tendonunitnrehabilitationnstretchingnunloading
Submitted 7 August 2009, sent back or revisions 1 October 2009; accepted or publication ollowing double-blind peer review
3 December 2009
Hiroshi Kanazawa, Yukio Urabe, Taizan Shirakawa
Hiroshi Kanazawa
is Senior Physiotherapist,
Director o Department
o Rehabilitation,
Department o
Rehabilitation,
Matterhorn
Rehabilitation Hospital,
and Doctorate Student,
Graduate School
o Health Sciences,
Hiroshima University,
Hiroshima; Yukio
Urabeis Proessor,Graduate School
o Health Sciences,
Hiroshima University,
Hiroshima; and Taizan
Shirakawa is Senior
Orthopedic Surgeon,
President o Matterhorn
Rehabilitation
Hospital, Matterhorn
Rehabilitation Hospital,
Hiroshima, Japan
Correspondence to:
H Kanazawa
E-mail: kanah@mbe.
ocn.ne.jp

8/8/2019 Costa Et Al. 2010 - IJTR - Commentary on Behaviour of the Muscle-tendon Unit During Static Stretching Following U…
http://slidepdf.com/reader/full/costa-et-al-2010-ijtr-commentary-on-behaviour-of-the-muscle-tendon-unit 2/11
InternationalJournaloTherapyandRehabilitation,March2010,Vol17,No3 133
maximal ankle dorsifexion angle o the injured
leg. Equal distribution o load between both legs
was ensured at the beginning o stretching by
asking the patient to apply hal their body weight
to each o two independent scales. Pelvis and
trunk orientation during stretching was moni-
tored by visual observation.
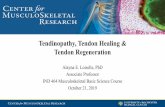
During stretching, ultrasonograms were
recorded every minute using an ultrasonic appa-
ratus (Power Vision 6000 SSA-370A; ToshibaMedical Systems Co., Japan) with an 8MHz linear
scanning probe (PLM-805AT; Toshiba Medical
Systems Co.). The amount o distal displacement
o each o the markers in the recorded images was
measured using ImageJ image analysis sotware
(NIH, USA). A probe xation rame made rom
an ethylene-vinyl acetate sponge was used during
ultrasonographic measurements to help maintain
the position o the probe. A given coordinate point
was precisely reproduced by using records o our
squares o the probe xation rame. A photograph
o an representative ultrasonographic measure-
ment is shown in Figure 3.
Methods
dgThe study was an observational clinical study
design. Using an ultrasonogram, the amount o
displacement o two markers in the DA and MTJduring stretching on a stretching board was meas-
ured in both the injured and uninjured legs o
each patient. The amount o distal displacement
o each o the markers refects the reaction o the
muscle-tendon unit to stretching.
ParpaTwenty emale patients (age 52.6 ± 12.2 years;
height, 154.6 ± 6.4 cm; weight 57.3 ± 4.6 kg;
(mean±SD)) were examined. All patients were
non-weight-bearing on one leg ollowing a unilat-
eral lower leg injury. Thirteen patients were diag-
nosed with a racture-dislocation o the ankle, and
seven with tibiobular ractures. All patients had
undergone surgical repair, but none had received
direct injury to the gastrocnemius muscle or
soleus muscles, or to the Achilles tendon.
All participants provided written inormed con-
sent ollowing study approval by the Institutional
Review Board o the authors’ hospital, in accord-
ance with the principles o the Declaration o
Helsinki. Anonymity and condentiality o the
patients were assured.
PrrDetermining markers in the medial head of
the gastrocnemius muscle
Two markers were identied in the gastrocnemius
muscle by ultrasonogram perormed in a stand-
ing position. The markers were the junction o
the ascicle and the DA at ¼ proximal height o
the lower leg and at the MTJ ( Figure 1). These
markers were careully chosen and conrmed to
show clear echoes.
Ultrasonographic measurements
Ultrasonographic measurements were perormed
ater medical approval was given or the patientto begin weight-bearing o more than hal o their
body weight on the injured limb. In a standing
position, the maximal ankle dorsifexion angle o
the patients’ injured leg was quickly measured on
a stretching board, using a reely adjustable angle
and an attached incline level meter (Niigata Seiki
Co., Japan; Figure 2).
In each experimental session, the maximal
ankle dorsifexion angle was determined as the
angle o tolerable submaximal stretching pain, or
the angle just beore the patients bent their knee.
Patients then stood or 10 minutes on the stretch-
ing board, which was set to the predetermined
proximal distal proximal distal
Figure 1. Determination o the markers. Markers were determined on ultrasonogram
(arrows). The let image shows the ascicle-deep aponeurosis junction (DA). The
right image shows the myotendinous junction (MTJ). DA was determined with high
brightness and a clearly depicted point in the junction o ascicle and deep aponeurosis
at 1/4 proximal height o the lower leg.
Figure 2. The stretching board with a reely adjustable
angle, and the level metre.
8/8/2019 Costa Et Al. 2010 - IJTR - Commentary on Behaviour of the Muscle-tendon Unit During Static Stretching Following U…
http://slidepdf.com/reader/full/costa-et-al-2010-ijtr-commentary-on-behaviour-of-the-muscle-tendon-unit 3/11
134 InternationalJournaloTherapyandRehabilitation,March2010,Vol17,No3
Research
Ultrasonographic measurements were repeated
every week, and were concluded when there was
no statistical laterality in the amount o displace-
ment o both markers ater stretching. One physi-
cal therapist blinded to the purpose and methods
o the study measured the displacement o the
markers in the ultrasonograms.
Calf circumference
Cal circumerence was measured using a bre-
glass tape measure at the point o maximum cal girth. One physical therapist blinded to the pur-
pose and methods o the study measured the cal
circumerence.
saa aayAll statistical tests were perormed in GraphPad
Prism 5.00 (GraphPad Sotware, La Jolla, CA).
Two-way analysis o variance or repeated meas-
ures (actors: injured leg, uninjured leg and time)
was used to compare the dierence in the amount
o displacement o DA and MTJ between the
uninjured and injured legs or every 1 minute
(a= 0.05). Upon detection o a signicant main
eect, paired t -tests were perormed to compare
the dierence between the uninjured and injured
legs. Bonerroni correction or multiple com-
parisons was applied, and the level o signii-
cance was set at 0.005. Paired t -tests were used
to assess the dierence in the amount o dis-
placement o DA and MTJ or every 1 minute
a=0.0011). Paired t -tests were used to detect sig-
nicant dierences in maximal ankle dorsifexion
angle and circumerences o the cal between the
rst and nal measurements (a=0.05). Data are
presented as means ± 1SD.
Figure 3. Ultrasonographic measurement. A probe xation
rame was used to acilitate the depiction o the markers.
proximal distal proximal distal
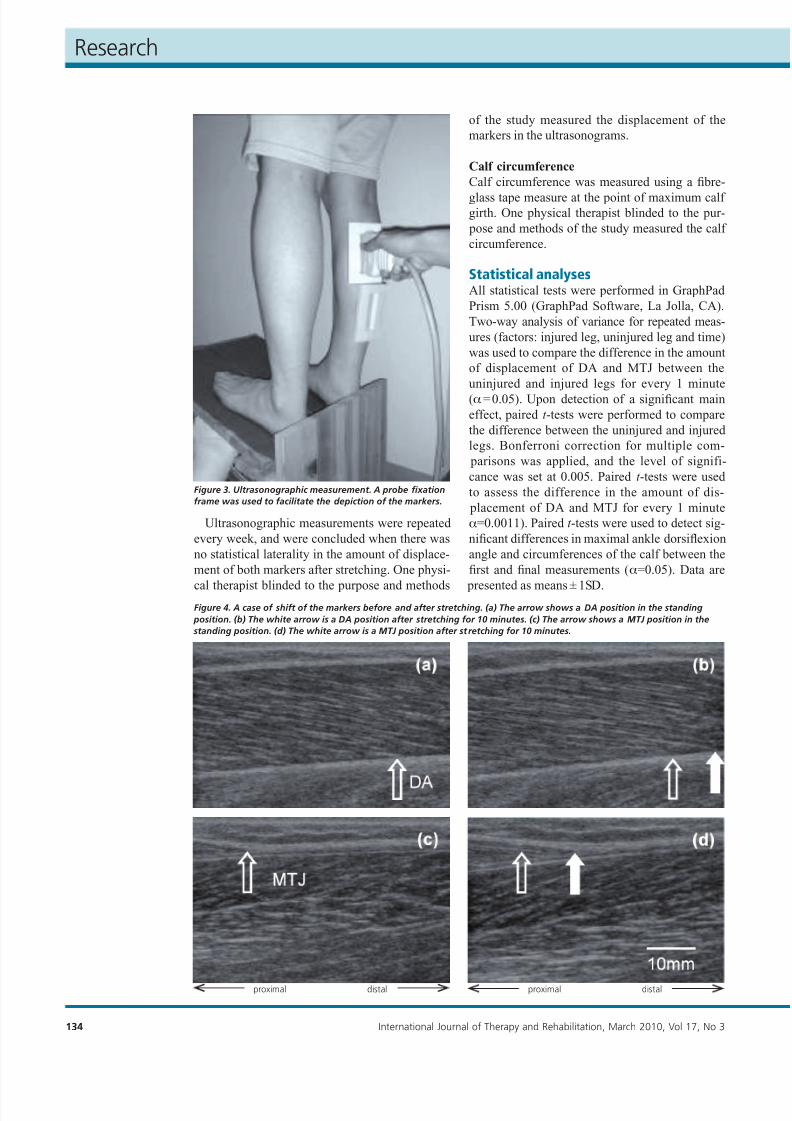
Figure 4. A case o shit o the markers beore and ater stretching. (a) The arrow shows a DA position in the standing
position. (b) The white arrow is a DA position ater stretching or 10 minutes. (c) The arrow shows a MTJ position in the
standing position. (d) The white arrow is a MTJ position ater stretching or 10 minutes.

8/8/2019 Costa Et Al. 2010 - IJTR - Commentary on Behaviour of the Muscle-tendon Unit During Static Stretching Following U…
http://slidepdf.com/reader/full/costa-et-al-2010-ijtr-commentary-on-behaviour-of-the-muscle-tendon-unit 4/11
InternationalJournaloTherapyandRehabilitation,March2010,Vol17,No3 135
Results
The average postoperative period beore approval
or partial weight-bearing (50% body weight) was
6.9 ± 2.4 weeks, at which time the maximal angle
o ankle dorsifexion in the injured leg improved rom 4.8 ± 3.8° at the beginning o measurements
to 18.8 ± 4.6° at the nal measurement ( P < 0.05).
There was no signiicant change in the maxi-
mal ankle dorsifexion angle in the uninjured leg
(23.5 ± 4.1° vs 24.3 ± 3.9°; P = 0.73).
At the beginning o measurements, maximal
cal circumerence was 1.8 ± 0.6cm smaller in the
injured leg than in the uninjured leg ( P = 0.023).
At the nal measurement, cal circumerence was
1.3 ± 0.7 cm lower in the injured leg than in the
uninjured leg ( P = 0.035) indicating muscle atro-
phy (Table 1). There was a signicant main eect
between uninjured and injured legs at the DA
( P< 0.05).
Signicant dierences in the amount o dis-
placement o DA or every 1 minute between
the uninjured and injured legs were ound dur-
ing the three minutes beore the nal measure-
ment ( P < 0.01). At the MTJ, a signicant main
eect between uninjured legs and injured legs
was ound ( P < 0.05), and there was a signicant
dierence in the amount o displacement o MTJ
between uninjured legs and injured legs or every
one minute, during the three minutes prior to
the nal measurement ( P < 0.01). No signicantinteractions between actors were ound or unin-
jured and injured legs. The amount o displace-
ment o the DA and MTJ at the rst and nal
measurements is shown in Table 2.
A typical case o DA and MTJ displace-
ments measured by ultrasonogram are shown in
Figure 4a, b and Figure 4c, d , respectively. The
overall average o DA displacement is shown in
Figure 5. The distal displacement o DA on the
injured side was larger than that on the unin-
jured side in irst measurement ( Figure 5a).
Subsequently, the distal displacement o DA on
the injured side gradually decreased towards thenal measurements ( Figure 5b, c). In the nal
measurement, the distal displacement o DA
became more similar to that o the uninjured
side ( Figure 5d ). During the entire measurement
period, DA displaced signicantly until three min-
utes beore the nal measurement, on both the
injured and uninjured sides ( P< 0.01). The aver-
age MTJ displacement is shown in Figure 6 . The
distal displacement o MTJ on the injured side
was smaller than that on the uninjured side in
the rst measurement ( Figure 6a). Subsequently,
the distal displacement o MTJ on the injured
side gradually increased towards the nal meas-
urements ( Figure 6b, c). In the nal measure-
ment, the distal displacement o MTJ became
increasingly similar to that o the uninjured side
( Figure 6d ). During the entire measurement
period, MTJ displaced signicantly until three
minutes beore the nal measurement on both
the injured and uninjured sides (P < 0.01). The
amount o the displacement o DA and MTJ did
not dier signicantly ater our minutes.
discussion
Ultrasonograms o the gastrocnemius muscle inhumans with a unilateral lower leg injury were
used to examine the reaction to static stretching
in the present study. The DA and the MTJ were
identied by the deep aponeurosis-ascicle junc-
tion and the myotendinous junction, respectively.
Previous histological studies have demonstrated
a high incidence o damage to the myotendi-
nous junction in muscle strain injuries (Garrett
et al, 1987; Nikolaou et al, 1987; Taylor et al,
1993; Noonan et al, 1994). Furthermore, detailed
observations revealed a deep aponeurosis-asci-
cle junction and/or supercial aponeurosis-as-
cicle junction in injured regions (Hughes et al,1995). These regions are easily injured and are
aected by changes in the state o the muscle-
tendinous tissue. As such, the authors considered
that these regions may be particularly responsive
to muscle stretching.
Tabl 1. Chag f th circumfrc f th calf
Circumfrc f th calf (cm)
Firt maurmt Fial maurmt
Uijurd lg (a) 32.2±3.2 32.5±3.1
Ijurd lg (b) 30.4±3.2 31.2±2.8
Latralit (a)-(b) -1.8±0.6 -1.3±0.7
Note:*P<0.05:signicantdierencebetweenguresjoinedbylines
Tabl 2. Amut f diplacmt f th DA ad MTJ durig 10 miut trtchig
DA (mm) MTJ (mm)
Firt maurmt Fial maurmt Firt maurmt Fial maurmt
Uijurd 5.4±0.9 5.7±0.9 16.1±1.4 15.8±1.2
Ijurd 9.7±2.6 5.6±1.1 4.8±2.0 15.1±1.2
Note:*P<0.05:signicantdierencebetweenguresjoinedbylines
**
* *

8/8/2019 Costa Et Al. 2010 - IJTR - Commentary on Behaviour of the Muscle-tendon Unit During Static Stretching Following U…
http://slidepdf.com/reader/full/costa-et-al-2010-ijtr-commentary-on-behaviour-of-the-muscle-tendon-unit 5/11
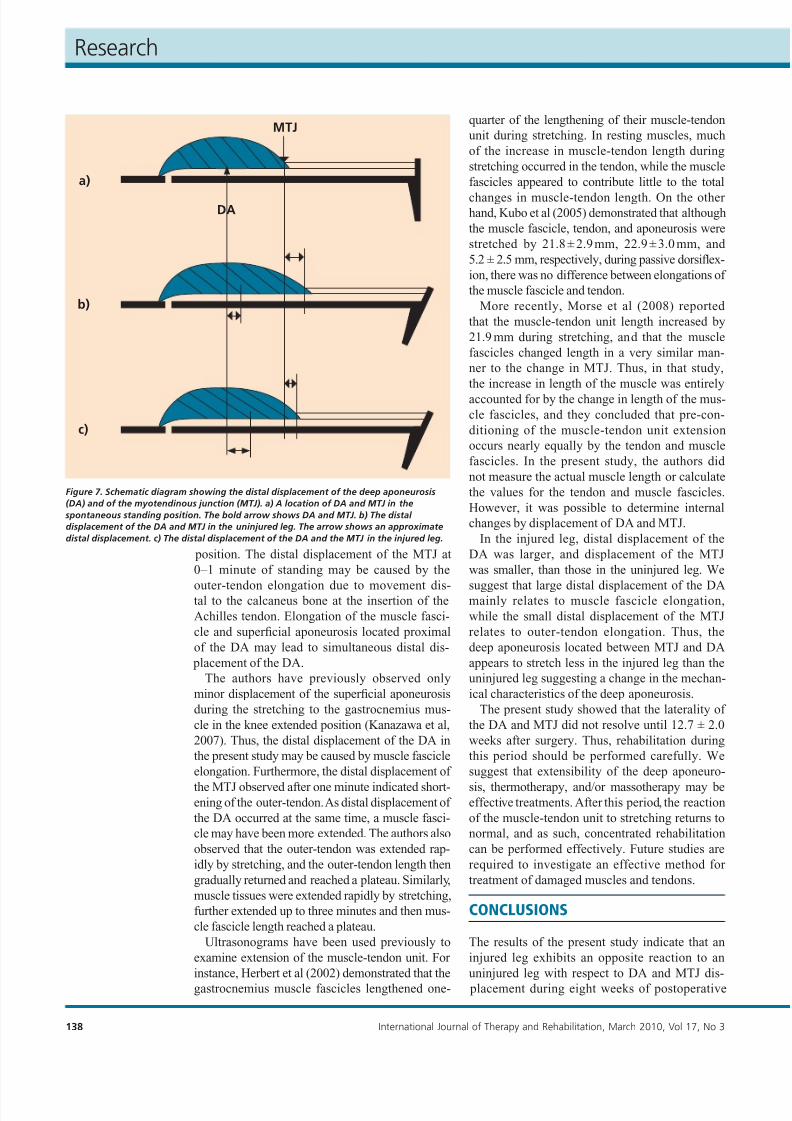
In this study, injured DA displacement was
greater than that in uninjured legs, ollowing 10
minutes o stretching, at the time o rst measure-
ment. In contrast, injured MTJ displacement was
smaller than that in uninjured legs at this time,
showing a reversed reaction to that seen in the
uninjured leg ( Figure 7 ). Following longer periodso recovery, the reaction o the injured leg became
closer to that o the uninjured leg. These ndings
may relate to changes in the mechanical character-
istics o the muscle–tendon complex.
Mechanical properties o human muscle and
tendon reported in the literature include tendon
stiness, tendon hysteresis and Young’s modulus
(Shorten, 1987; Fukashiro et al, 2001; Bennet et
al, 1986; Hubbard and Soutas-Little, 1984; Ker,
1981; Pollock and Shadwick, 1994; Maganaris and
Paul, 2002). Unloading can aect these properties,
as shown in animal models. Suspended rat tendons
had lower values or maximal stress and tangent
136 InternationalJournaloTherapyandRehabilitation,March2010,Vol17,No3
Research
modulus than tendons o control rats (Almeida-
Silveira et al, 2000). In addition, decreased sti-
ness o the suspended rat soleus muscle (Canon
and Goubel, 1995) has been reported. Eliasson
et al (2007) ound that the mechanical properties
most aected by unloading in the rat were hys-
teresis and creep, and both decreased with disusecompared with the control rat. Achilles tendon
suspension resulted in smaller surace area o col-
lagen bres (Nakagawa et al, 1989) and lower con-
centration o collagen (Vailas et al, 1988).
These actors could explain the mechanical
changes in the passive part o series elasticity
(Almeida-Silveira et al, 2000) and increased ten-
don compliance, which has been observed in dis-
use and ageing (Reeves et al, 2005; Narici, 2005).
These mechanical characteristic changes would
infuence the results o this study. However, the
authors were not able to identiy a specic actor
to explain the change observed in the patients.
D i s t a l d i s p l a c e m e n t (
m m )
D i s t a l d i s p l a c e m e n t (
m m )
Stretchingtime(min) Stretchingtime(min)
**
**
** **
****
**P <0.01
**
**
** **
****
a) Post-operation 6.9 ± 2.4 weeks (rst measurement)
Ankle dorsifexion angle: 4.8 ± 3.8°
b) Post-operation 8.1 ± 2.4 weeks
Ankle dorsifexion angle: 7.8 ± 3.0°
Figure 5. Total average o the distal displacement o the deep aponeurosis junction (DA). a) In the rst measurement, on the
injured side, the distal displacement o the DA was larger than the uninjured side. b) In the postoperation 8.1 weeks and c)
postoperation 10.7 weeks measurements, the distal displacement o DA on the injured side were gradually decreased, to the
nal measurements, d), where the distal displacement o DA became similar to that o the uninjured side. Over the whole o
the measurement period, DA displaced signicantly ( P< 00.1) until three minutes on both the injured and uninjured sides.
D i s t a l d i s p l a c e m e n t ( m m )
D i s t a l d i s p l a c e m e n t ( m m )
Stretchingtime(min) Stretchingtime(min)
**
** **
**
**
**
**** **
****
c) Post-operation 10.7 ± 1.2 weeks Ankle dorsifexion angle: 13.6 ± 4.3°
d) Post-operation 12.7 ± 2.0 weeks (nal measurement) Ankle dorsifexion angle: 18.8 ± 4.6°
**

8/8/2019 Costa Et Al. 2010 - IJTR - Commentary on Behaviour of the Muscle-tendon Unit During Static Stretching Following U…
http://slidepdf.com/reader/full/costa-et-al-2010-ijtr-commentary-on-behaviour-of-the-muscle-tendon-unit 6/11
Laterality o injured cal circumerence was
observed. Skeletal muscle atrophy due to inac-
tivity has been investigated using experimental
animal models o hind limb suspension (Morey,
1979; Winiarski et al, 1987) and plaster cast xa-
tion (Cooper, 1972; Herbison et al, 1978). Those
studies suggested that shortening o the cross-sectional area and minimization o the muscular
bre (Desplanches et al, 1987; Hauschka et al,
1987), irregularity o the muscular bre sequence
(Winiarski et al, 1987; Desplanches et al, 1990),
and decreased tensile strength during muscle
contraction (McDonald et al, 1994) occurred in
the atrophic muscle. Hind limb suspension and
plaster cast ixation resulted in 40% and 42%
weight reduction in the rat gastrocnemius and
soleus muscles, respectively (Herbison et al,
1978; Morey, 1979). In addition, Herbison et al
(1979) observed injury to muscle cells ollowing
six weeks o a plaster cast xed to the hind leg o
InternationalJournaloTherapyandRehabilitation,March2010,Vol17,No3 137
D i s t a l d i s p l a c e m e n t (
m m )
D i s t a l d i s p l a c e m e n t (
m m )
Stretchingtime(min) Stretchingtime(min)
a rat. Thus, the laterality o cal muscle circum-
erence in this study may refect muscle atrophy,
and greater lengthening o the muscle belly in the
injured leg may have been caused by decreased
tensile strength o the muscle.
Many authors consider that a muscle electro-
myogram (EMG) level must be lower than 1% o that during maximal voluntary contraction beore
considering that muscular contraction is negli-
gible (McNair et al, 2002; Gajdosik, 2006). The
authors did not measure the EMG o the gastroc-
nemius muscle at the period o unloading in the
present study. However, the 5.6% decrease in the
circumerence o the cal in the injured leg com-
pared with that in the uninjured leg, at the time
o the rst measurements, suggests the presence
o muscle atrophy.
Ultrasonographic measurements in the present
study showed that both markers were distally dis-
placed in both legs in the spontaneous standing
**P <0.01
**
a) Post-operation 6.9 ± 2.4 weeks (rst measurement)
Ankle dorsifexion angle: 4.8 ± 3.8°
b) Post-operation 8.1 ± 2.4 weeks
Ankle dorsifexion angle: 7.8 ± 3.0°
Figure 6. Total average o the distal displacement o the myotendinous junction (MTJ). (a) In the rst measurement, on the
injured side, the distal displacement o MTJ was smaller than uninjured side. (b) In the postoperation 8.1 weeks, and (c) in the
postoperation 10.7 weeks measurements, the distal displacement o MTJ on the injured side were gradually increased, to the
nal measurements d), the distal displacement o MTJ became increasingly similar to that o the uninjured side. Over the whole
o the measurement period, MTJ displaced signicantly until three minutes ( P< 0.01) on both the injured and uninjured sides.
**
******
**
**
**
** **
****
D i s t a l d i s p l a c e m e n t ( m m )
D i s t a l d i s p l a c e m e n t ( m m )
Stretchingtime(min) Stretchingtime(min)
c) Post-operation 10.7 ± 1.2 weeks Ankle dorsifexion angle: 13.6 ± 4.3°
d) Post-operation 12.7 ± 2.0 weeks (nal measurement) Ankle dorsifexion angle: 18.8 ± 4.6°
****
****
**
**
**
**
** **
****
8/8/2019 Costa Et Al. 2010 - IJTR - Commentary on Behaviour of the Muscle-tendon Unit During Static Stretching Following U…
http://slidepdf.com/reader/full/costa-et-al-2010-ijtr-commentary-on-behaviour-of-the-muscle-tendon-unit 7/11
138 InternationalJournaloTherapyandRehabilitation,March2010,Vol17,No3
Research
position. The distal displacement o the MTJ at
0–1 minute o standing may be caused by the
outer-tendon elongation due to movement dis-tal to the calcaneus bone at the insertion o the
Achilles tendon. Elongation o the muscle asci-
cle and supercial aponeurosis located proximal
o the DA may lead to simultaneous distal dis-
placement o the DA.
The authors have previously observed only
minor displacement o the supercial aponeurosis
during the stretching to the gastrocnemius mus-
cle in the knee extended position (Kanazawa et al,
2007). Thus, the distal displacement o the DA in
the present study may be caused by muscle ascicle
elongation. Furthermore, the distal displacement o
the MTJ observed ater one minute indicated short-ening o the outer-tendon. As distal displacement o
the DA occurred at the same time, a muscle asci-
cle may have been more extended. The authors also
observed that the outer-tendon was extended rap-
idly by stretching, and the outer-tendon length then
gradually returned and reached a plateau. Similarly,
muscle tissues were extended rapidly by stretching,
urther extended up to three minutes and then mus-
cle ascicle length reached a plateau.
Ultrasonograms have been used previously to
examine extension o the muscle-tendon unit. For
instance, Herbert et al (2002) demonstrated that the
gastrocnemius muscle ascicles lengthened one-
quarter o the lengthening o their muscle-tendon
unit during stretching. In resting muscles, much
o the increase in muscle-tendon length during
stretching occurred in the tendon, while the muscle
ascicles appeared to contribute little to the total
changes in muscle-tendon length. On the other hand, Kubo et al (2005) demonstrated that although
the muscle ascicle, tendon, and aponeurosis were
stretched by 21.8 ± 2.9 mm, 22.9 ± 3.0 mm, and
5.2 ± 2.5 mm, respectively, during passive dorsifex-
ion, there was no dierence between elongations o
the muscle ascicle and tendon.
More recently, Morse et al (2008) reported
that the muscle-tendon unit length increased by
21.9 mm during stretching, and that the muscle
ascicles changed length in a very similar man-
ner to the change in MTJ. Thus, in that study,
the increase in length o the muscle was entirely
accounted or by the change in length o the mus-
cle ascicles, and they concluded that pre-con-
ditioning o the muscle-tendon unit extension
occurs nearly equally by the tendon and muscle
ascicles. In the present study, the authors did
not measure the actual muscle length or calculate
the values or the tendon and muscle ascicles.
However, it was possible to determine internal
changes by displacement o DA and MTJ.
In the injured leg, distal displacement o the
DA was larger, and displacement o the MTJ
was smaller, than those in the uninjured leg. We
suggest that large distal displacement o the DAmainly relates to muscle ascicle elongation,
while the small distal displacement o the MTJ
relates to outer-tendon elongation. Thus, the
deep aponeurosis located between MTJ and DA
appears to stretch less in the injured leg than the
uninjured leg suggesting a change in the mechan-
ical characteristics o the deep aponeurosis.
The present study showed that the laterality o
the DA and MTJ did not resolve until 12.7 ± 2.0
weeks ater surgery. Thus, rehabilitation during
this period should be perormed careully. We
suggest that extensibility o the deep aponeuro-
sis, thermotherapy, and/or massotherapy may beeective treatments. Ater this period, the reaction
o the muscle-tendon unit to stretching returns to
normal, and as such, concentrated rehabilitation
can be perormed eectively. Future studies are
required to investigate an eective method or
treatment o damaged muscles and tendons.
conclusions
The results o the present study indicate that an
injured leg exhibits an opposite reaction to an
uninjured leg with respect to DA and MTJ dis-
placement during eight weeks o postoperative
MTJ
DA
a)
b)
c)
Figure 7. Schematic diagram showing the distal displacement o the deep aponeurosis
(DA) and o the myotendinous junction (MTJ). a) A location o DA and MTJ in the
spontaneous standing position. The bold arrow shows DA and MTJ. b) The distal
displacement o the DA and MTJ in the uninjured leg. The arrow shows an approximate
distal displacement. c) The distal displacement o the DA and the MTJ in the injured leg.

8/8/2019 Costa Et Al. 2010 - IJTR - Commentary on Behaviour of the Muscle-tendon Unit During Static Stretching Following U…
http://slidepdf.com/reader/full/costa-et-al-2010-ijtr-commentary-on-behaviour-of-the-muscle-tendon-unit 8/11
InternationalJournaloTherapyandRehabilitation,March2010,Vol17,No3 139
n Thereactiontostretchingoanunhealthymuscle-tendonunitislargelyunknown.
n Theaimothestudywastoinvestigatethereactionothemuscle-tendon
unittostretchingateraperiodonon-weight-bearingbyultrasonograms.
n Atalltimepoints,thejunctionotheascicleandthedeepaponeurosis
(DA)andthemyotendinousjunction(MTJ)displaceddistallyduringthefrst
threeminutesostretchinginbothlegs( P <0.01).
n InjuredDAdisplacementwasinitiallygreaterthanthatintheuninjuredleg
andinjuredMTJdisplacementwassmallerthanthatintheuninjuredleg.
n Atertreatment,DAandMTJdisplacementsintheinjuredlegapproached
levelssimilartothatotheuninjuredleg.
n Followinganinjury,asciclesandtendonmayhavebeenexcessivelyextended.
n Recoveryothemuscletendoncomplexmightbeacceleratedbyapplying
exercisesaimedatattainingincreasedextensibilityotheaponeurotictissue.
Key PoInTsrecovery rom a unilateral lower leg injury. The
large distal displacement o the DA suggests
muscle ascicle elongation, while the small dis-
tal displacement o the MTJ suggests outer-ten-
don elongation. There was less elongation o the
deep aponeurosis located between the DA and MTJ. Thereore, normalization o the muscle ten-
don complex might be accelerated by attaining
increased extensibility o the aponeurotic tissue
during the treatment period. IJTR
Conlict o interest: none Acknowledgements: The authors acknowledge the sta at the Department o Rehabilitation, Matterhorn Rehabilitation
Hospital or their help with the data collection. The authorsalso acknowledge the students at the Graduate School o
Health Sciences, Hiroshima University or their continuous support with this project.
Almeida-Silveira MI, Lambertz D, Perot C, Goubel F (2000)Changes in stiness induced by hindlimb suspension in ratAchilles tendon. Eur J Appl Physiol 81(3): 252–7
Bennet MB, Ker RF, Dimery NJ, Alexander RM (1986)Mechanical properties o various mammalian tendons. J Zool 209(3): 537–48
Canon F, Goubel F (1995) Changes in stiness induced byhind limb suspension in rat soleus muscle. Pfugers Arch429(3):332–7
Cooper RR (1972) Alterations during immobilization and regeneration o skeletal muscle in cats. J Bone Joint Surg
Am 54(5): 919–53Desplanches D, Mayet MH, Sempore B, Flandrois R (1987)
Structural and unctional responses to prolonged hindlimbsuspension in rat muscle. J Appl Physiol 63(2): 558–63
Desplanches D, Kayar SR, Sempore B, Flandrois R, Hoppeler H (1990) Rat soleus muscle ultrastructure ater hindlimbsuspension. J Appl Physiol 69(2): 504–08
Eliasson P, Fahlgren A, Pasternak B, Aspenberg P (2007)
Unloaded rat Achilles tendons continue to grow, but loseviscoelasticity. J Appl Physiol 103(2): 459–63Fukashiro S, Noda M, Shibayama A (2001) In vivo deter-
mination o muscle viscoelasticity in the human leg. Acta Physiol Scand 172(4): 241–8
Gajdosik RL (2006) Inluence o a low-level contrac-tile response rom the soleus, gastrocnemius and tibia-lis anterior muscles on viscoelastic stress-relaxation o aged human cal muscle-tendon units. Eur J Appl Physiol 96(4): 379–88
Garrett WE Jr, Saran MR, Seaber AV, Glisson RR, Ribbeck BM (1987) Biomechanical comparison o stimulated and nonstimulated skeletal muscle pulled to ailure. Am J Sports Med 15(5):448–54
Hauschka EO, Roy RR, Edgerton VR (1987) Size and meta- bolic properties o single muscle bers in rat soleus ater hindlimb suspension. J Appl Physiol 62(6): 2338–47
Herbert RD, Moseley AM, Butler JE, Gandevia SC (2002)Change in length o relaxed muscle ascicles and ten-
dons with knee and ankle movement in humans. J Physiol 539(Pt 2): 637–45Herbison GJ, Jaweed MM, Ditunno JF (1978) Muscle ber
atrophy ater cast immobilization in the rat. Arch Phys Med Rehabil 59(7): 301–5
Hortobagyi T, Faludi J, Tihanyi J, Merkely B (1985) Eectso intense stretching-fexibility training on the mechanical
prole o the knee extensors and on the ROM o the hip joint. Int J Sports Med 6(6): 317–21
Hubbard RP, Soutas-Little RW (1984) Mechanical propertieso human tendon and their age dependence. J Biomech Eng 106(2): 144–50
Hughes C 4th, Hasselman CT, Best TM, Martinez S, GarrettWE Jr (1995) Incomplete, intrasubstance strain injuries o the rectus emoris muscle. Am J Sports Med 23(4): 500–6
Kanazawa H, Urabe Y, Iwamoto H, Shirakawa T (2007) Invivo dynamics o human gastrocnemius muscle-tendon unitduring static stretching. J Clin Sport Med 15(3): 401–6
Ker RF (1981) Dynamic tensile properties o the plantaris
tendon o sheep. J Exp Biol 93: 283–302Kubo K, Kanehisa H, Fukunaga T (2005) Eect o clod and
hot water immersion on the mechanical properties o humanmuscle and tendon in vivo. Clin Biomech 20(3): 291–300Maganaris CN, Paul JP (2002) Tensile properties o the in vivo
human gastrocnemius tendon. J Biomech 35(12): 1639–46McDonald KS, Blaser CA, Fitts RH (1994) Force-Velocity
and power characteristics o rat soleus muscle bers ater hindlimb suspension. J Appl Physiol 77(4): 1609–16
McNair PJ, Hewson DJ, Dombroski E, Stanley SN (2002)Stiness and passive peak orce changes at the ankle joint:the eect o dierent joint angular velocities. Clin Biomech 17(7): 536–40
Morey ER (1979) Spacefight and bone turnover : correla-tion with a new rat model o weightlessness. Bioscience 29(3): 168–172
Morse CI, Degens H, Seynnes OR, Maganaris CN, Jones DA(2008) The acute eect o stretching on the passive sti-ness o the human gastrocnemius muscle tendon unit. J
Physiol 586(1): 97–106 Nakagawa Y, Totsuka M, Sato T, Hirota K (1989) Eects o
disuse on the ultrastructure o the Achilles tendon in rats. Eur J Appl Physiol 59(3): 239–42 Narici MV (2005) Myotendinous alterations and eects o resis-
tive loading in old age. Scand J Med Sci Sport 15(6): 392–401 Nikolaou PK, Macdonald BL, Glisson RR, Seaber AV, Garrett
WE Jr (1987) Biomechanical and histological evaluationo muscle ater controlled strain injury. Am J Sports Med 15(1): 9–14
Noonan TJ, Best TM, Seaber AV, Gar rett WE Jr (1994)Identication o a threshold or skeletal muscle injury. Am
J Sports Med 22(2): 257–61Pollock CM, Shadwick RE (1994) Relationship between body
mass and biomechanical properties o limb tendons in adultmammals. Am J Physiol 266(3 Pt 2): 1016–21
Reeves ND, Maganaris CN, Narici MV (2005) Plasticity o dynamic muscle perormance with strength training in eld-erly humans. Muscle Nerve 31(3): 355–64
Shorten MR (1987) Muscle elasticity and human perorm-ance. Med Sport Sci 25: 1–18
Taylor DC, Dalton JD, Seaber AV, Gar rett WE (1990)Viscoelastic properties o muscle-tendon units. The biome-chanical eects o stretching. Am J Sports Med 18(3): 300–9
Taylor DC, Dalton JD Jr, Seaber AV, Garrett WE Jr (1993)Experimental muscle strain injury. Early unctional and structural decits and the increased risk or reinjury. Am J Sports Med 21(2): 190–4
Vailas AC, Duluna DM, Lewis LL, Curwin SL, Roy RR, Alord EK (1988) Adaptation o bone and tendon to prolonged hindlimb suspension in rats. J Appl Physiol 65(1): 373–6
Wilson GJ, Wood GA, Elliott BC (1991) The relationship between stiness o the musculature and static fexibility:an alternative explanation or the occurrence o muscular injury. Int J Sports Med 12(4): 403–7
Winiarski AM, Roy RR, Alord EK, Chiang PC, Edgerton VR (1987) Mechanical properties o rat skeletal muscle ater hind limb suspension. Exp Neurol 96(3): 650–60
Witvrouw E, Mahieu N, Danneels L, McNair P (2004)Stretching and injury prevention: an obscure relationship.
Sports Med 34(7): 443–9Ylinen J (2008) Stretching Therapy. Elsevier, Philadelphia

8/8/2019 Costa Et Al. 2010 - IJTR - Commentary on Behaviour of the Muscle-tendon Unit During Static Stretching Following U…
http://slidepdf.com/reader/full/costa-et-al-2010-ijtr-commentary-on-behaviour-of-the-muscle-tendon-unit 9/11
140 InternationalJournaloTherapyandRehabilitation,March2010,Vol17,No3
Research
Stretching exercises are com-
monly undertaken or sports
and rehabilitation proceduresater injury. The displacement
in the muscle-tendon unit o
the hum an gas trocne mius
muscleduringstaticstretching,
ater a period o non-weight-
bearing ollowing injury, is o
importanceinbothsportsand
and stroke injuries.In physical
therapy,stretchingisoneothe
mosteectivetechniquesused
orlengtheningshortenedmus-
cles,andimprovementojoint
rangeomotion.Inthistypeo
clinicalsetting,anunderstand-ing o optimal stretching time
isessential.
Herbertetal(2002)measured
changesinthelengthomuscle
ascicles in a relaxed human
gastrocnemius muscle during
passively imposed changes in
joint angle. Kubo et al (2005)
showed that while the muscle
ascicles,tendonandaponeuro-
sisstretchedduringpassivedor-
sifexion othe anklejoint, the
elongation o the tendon was
signicantly greater than thatotheaponeurosis.Meanwhile,
the stretching reaction o an
unhealthy muscle-tendon unit,
such as in muscle injuries,
including musclestrain, muscle
tendonatrophy,orunloading,is
o high clinical signicance but
largelyunknown.
Inthisstudy,ultrasonograph-
ic measurementso equal dis-
tributionoloadbetweenboth
legs were made, with equal
distributionatthebeginningo
stretchingensuredbyaskingthe
patienttoapplyhaltheirbody
weight to each o two inde-
pendentscales.Ultrasonograms
were recorded every minute,
usinganultrasonicimagingsys-
tem. Corresponding distal dis-
placementmeasurementswere
carried out using the image
analysissotware.
Thendings rom theultra-
sonic imaging quantitative
study included a signicant
maineectbetweenuninjured
and injured legs at the deep
aponeurosisjunction(DA),and
signicant dierences in theamountodisplacementoDA.
At the myotendinous junction
(MTJ),asignicantmaineect
between uninjured legs and
injuredlegswasalsoound.No
signicantinteractionsbetween
actors were ound or unin-
juredandinjuredlegs.
Further, the distal displace-
mentoDAontheinjuredside
gradually decreased towards
the nal measurements and
nally, the distal displacement
o DA became more similarto that o the uninjured side.
ThedistaldisplacementoMTJ
on the injured side gradually
increased towards the nal
measurements and lastly, the
distal displacement o MTJ
became increasingly similar
to that o the uninjured side.
Thus, the nal outcome ater
treatment was DA and MTJ
displacements in the injured
leg approached levels o the
uninjured leg. These ndings
may relate to changes in themechanical characteristics o
themuscle–tendoncomplex.
Earlierstudiessuggestedthat
shorteningothecross-section-
alareaandminimizationothe
muscularbre(Desplancheset
al,1987;Hauschkaetal,1987),
irregularity o the muscular
bresequence(Winiarskietal,
1987;Desplanchesetal,1990),
anddecreased tensilestrength
during m us cle contraction
(McDonaldet al,1994) occurs
in the atrophic muscle. More
recently, Morse et al (2008)
reported that the muscle-ten-
don unit length increased by
21.9mm during stretching,
and that the muscle ascicles
changedlengthinaverysimi-
lar manner to the change in
MTJ.Inthisstudy,theauthors
wereabletodetermineinternal
changesbydisplacementoDA
andMTJ.
In the injured leg, dis tal
displacement o the DA was
larger,anddisplacementothe
MTJ was smaller, than those
in the uninjured leg. It wassuggestedthatlargedistaldis-
placement o the DA mainly
relatestomuscleascicleelon-
gation, while the small distal
displacementotheMTJrelates
to outer-tendon elongation.
Thus, the deep aponeurosis
located between MTJ and DA
appears to stretch less in the
injured leg thanthe uninjured
leg, suggesting a change in
the mechanical characteristics
othedeepaponeurosis.
Hence, rehabilitation dur-ing this peri od should be
perormed very careully. The
authorssuggestextensibilityo
thedeepaponeurosis,thermo-
therapy, and/or massotherapy
as eective treatments. Ater
thisperiod,thereactionothe
muscle-tendonunit to stretch-
ing returns to normal. The
authors o this study suggest
uture studies are required to
investigateaneectivemethod
ortreatmentodamagedmus-
clesandtendons.Earlierliteraturerevealsthata
muscle electromyogram(EMG)
levelmustbelowerthan1%o
that during maximal voluntary
contractionbeore considering
that muscular contraction as
negligible(McNairetal,2002;
Gajdosik,2006).Theauthorsin
thisstudydidnotmeasurethe
EMGothemuscleattheperi-
odounloading.Itisproposed
thaturther studyshould look
attheEMGinthesemuscles,as
there may be muscle atrophy.
There is 5.6%decrease in the
circumerences o the cal in
theinjuredleg comparedwith
thatintheuninjuredlegatthe
timeotherstmeasurements
– suggesting the presence o
muscleatrophy.
The results o the present
study indicate that an injured
leg, ater postoperative recov-
ery rom a leg injury, exhib-
its an oppositereaction to an
uninjured leg with respect to
DA and MTJ displacement.
Normalization o the muscle
tendoncomplexmightacceler-atebyattainingincreasedexten-
sibilityotheaponeurotictissue
during the treatment period.
Theproceduralndingsothe
present study would help in
postoperativecareduringreha-
bilitation, something o great
importancetothepatient.
Desplanches D, Mayet MH, Sempore B,Flandrois R (1987) Structural and func-tional responses to prolonged hindlimbsuspension in rat muscle. J Appl Physiol
63(2): 558–63
Desplanches D, Kayar SR, Sempore B,Flandrois R, Hoppeler H (1990) Rat soleusmuscle ultrastructure after hindlimb sus-pension. J Appl Physiol 69(2): 504–08
Gajdosik RL (2006) Influence of a low-levelcontractile response from the soleus, gas-trocnemius and tibialis anterior muscleson viscoelastic stress-relaxation of agedhuman calf muscle-tendon units. Eur J
Appl Physiol 96(4): 379–88
Hauschka EO, Roy RR, Edgerton VR (1987)Size and metabolic properties of singlemuscle fibers in rat soleus after hind-limb suspension. J Appl Physiol 62(6):2338–47
Herbert RD, Moseley AM, Butler JE, GandeviaSC (2002) Change in length of relaxedmuscle fascicles and tendons with knee
and ankle movement in humans. J Physiol 539(Pt 2): 637–45
Kubo K, Kanehisa H, Fukunaga T (2005)Effect of clod and hot water immersionon the mechanical properties of humanmuscle and tendon in vivo. Clin Biomech 20(3): 291–300
McDonald KS, Blaser CA, Fitts RH (1994)Force-Velocity and power character-istics of rat soleus muscle fibers afterhindlimb suspension. J Appl Physiol
77(4): 1609–16
McNair PJ, Hewson DJ, Dombroski E, StanleySN (2002) Stiffness and passive peakforce changes at the ankle joint: theeffect of different joint angular velocities.Clin Biomech 17(7): 536–40
Morse CI, Degens H, Seynnes OR, Maganaris
CN, Jones DA (2008) The acute effect ofstretching on the passive stiffness of thehuman gastrocnemius muscle tendonunit. J Physiol 586(1): 97–106
Winiarski AM, Roy RR, Alford EK, Chiang PC,Edgerton VR (1987) Mechanical proper-ties of rat skeletal muscle after hind limbsuspension. Exp Neurol 96(3): 650–60
Manjunatha Mahadevappa, PhD Assistant Proessor,School o Medical Science and Technology,Indian Institute o Technology Kharagpur, [email protected]
COMMENTARIES

8/8/2019 Costa Et Al. 2010 - IJTR - Commentary on Behaviour of the Muscle-tendon Unit During Static Stretching Following U…
http://slidepdf.com/reader/full/costa-et-al-2010-ijtr-commentary-on-behaviour-of-the-muscle-tendon-unit 10/11
InternationalJournaloTherapyandRehabilitation,March2010,Vol17,No3 141
This article represents a unique
andinterestingstudythatexam-
ined the muscle-tendon unit’s
responses to static stretching
using an ultrasound imaging
device in the injured and unin- jured legs o 20 women. The
authors should be commended
ortheireortstoinvestigatethe
pragmaticuseostaticstretching
orthepurposesorehabilitation.
The majority o research
related to stretching is most
oten ocused on perormance
and mechanistic approaches.
Much less isknown about the
applicationostretchinginreha-
bilitation settings. Thereore,
the present study supports
the hypothesis that stretchingan injured limb can improve
the range o motion to that
demonstratedby the uninjured
limb,whichurtherimpliesthat
stretchingis an important part
o the postoperative rehabilita-
tion programme. Furthermore,
the authors suggested that
the improved range o motion
mayberelatedtoanincreased
extensibilityotheaponeuroses.
Thus, stretching may infuence
the noncontractile, rather than
the contractile elements o themusculotendinousunit.
Thesendingsare consistent
with those o previous studies
(Morseetal,2008;Ryanetal,
2009)thathavesuggestedthat
theelongationothemusculo-
tendinousunitmaybeexplained
by viscoelastic changes in the
perimysium,whichisstructurally
andphysiologicallysimilartothe
aponeuroses described in the
presentstudy.
The undamental question
stillremains,however,regarding
theacuteviscoelasticchangesvs
stretch tolerance increases. For
instance, stretching has been
shown to decrease musculo-
tendinous stiness (Ryan et al,
2008; 2009) which is usually
causedbychangesinviscoelastic
propertiesothemusculotendi-
nous unit. Conversely, stretch-
ing may just cause a transient
increaseinstretchtolerance,not
necessarily muscle extensibility
(BenandHarvey,2009).
Thedierencebetweenthese
two responses may be due to
the duration o the stretch-
ing protocol. Presumably, it is
the viscoelastic alterations and
decreases in musculotendinousstinessthataredesirableeects
ostretchingsoastoelicitpro-
gressive increases in range o
motion and perhaps (although
this is debatable) decrease the
risk o injury. Nevertheless, an
increaseinstretchtolerancecan
alsobeapositiveoutcomerom
stretchingconsideringthatthere
is a plausible analgesic eect
which refects less pain dur-
ing stretching (Malliaropoulos
etal,2004).Thus,urtherstud-
iesareneededinclinicalpopu-lations to help answer these
undamentalquestions.
Acute stretching-induced
orce decits (Shrier, 2004;
Rubini et al, 2007) must also
beacknowledgedashavingthe
potential to transiently weaken
the stretched muscles – even
duringrehabilitation.Thepresent
study examined the range o
motionotheinjuredvsnonin-
jured limbs as outcome meas-
ures to assess the eectiveness
otherehabilitationstretching.However, strength assess-
m ents are also requently
conducted in order to assess
muscle imbalances and the
progress o the rehabilitation
programme. For example, a
common assessment used to
assess the risk o thigh muscle
strain injuries, track rehabilita-
tionprogress,anddecidewhen
athletescanreturntoplayisthe
hamstrings-to-quadriceps (H:Q)
ratio.Previousstudiesromour
laboratory have indicated that
anacuteboutostretchingmay
aecttheH:Qratio(Costaetal,
2009a; 2009b). We previously
suggestedthatcliniciansshould
use caution when interpreting
the H:Q ratio i this test was
perormed immediately ater
stretching (Costa et al,2009a).
Thus, attention must be given
astowhenthestretchingproto-
colisperormedduringareha-
bilitation session. Conversely,
although acute stretching has
been consistently shown to
decreasestrength(Shrier,2004;
Rubinietal,2007),thesendings
needtobeplacedinthecontext
o a comprehensive rehabilita-
tion programme. For example,Marek et al (2005) suggested
thatintheearlystagesoreha-
bilitation,when thereis a clear
benetoregainingaunctional
rangeo motion, smallstretch-
ing-induced strength decits
maynotbeclinicallyrelevant.
However, as the rehabilita-
tion programme progresses,
care must be taken and clini-
cians should beawareo these
stretching-inducedstrengthde-
cits when conducting strength
assessments immediately aterstretchingontheirpatients,par-
ticularly i the results o these
testsaretobeusedormaking
decisionsregardingrehabilitation
progressorthereturntoplayor
athletes(Mareketal,2005).
Asshowninthisstudy,dier-
encesbetweenthe injured and
non-injured side only resolved
aternearly 13weeks otreat-
ment.Thereore,weagreewith
the authors that extreme care
mustbetakenduringtheperiod
whereinjury-relatedbilateraldi-erencesarestillsignicant.
Future well-controlled stud-
iesshouldocusonthechronic
eectsostaticstretchingduring
a rehabilitation programme on
injuredlimbsinordertoprovide
urther support or the recom-
mendation o stretching during
post-injuryrehabilitation.Finally,
specic rehabilitation guidelines
concerning the type o stretch-
ing regimen, stretch volume,
duration,andrequencyhaveyet
tobeestablished,andthesemay
infuenceordeterminetheeec-
tivenessostretchingasareha-
bilitationtool(Malliaropouloset
al,2004).
Collectively,evidenceisbuild-
ing to suggest that stretching
mayindeedbeanecessaryreha-
bilitation component or recov-
eryollowingamusculoskeletal
injury, as long as precautions
are taken regarding when the
stretching protocol takes place
within a rehabilitation session,
particularlywhen strength test-
ing may also occur during the
samesession.
Furthermore , a ddit iona l
researchisneededtodelineate
thetype,duration,andintensityo stretching necessary to elicit
changes in musculotendinous
stinessandviscoelasticchang-
esasopposedtomereincreases
instretchtolerance.
Ben M, Harvey LA (2010) Regular stretchdoes not increase muscle extensibility: arandomized controlled trial. Scand J Med
Sci Sports 20(1): 136–44
Costa PB, Ryan ED, Herda TJ, Defreitas JM,Beck TW, Cramer JT (2009a) Effects ofstatic stretching on the hamstrings-to-quadriceps ratio and electromyographicamplitude in men. J Sports Med Phys
Fitness 49(4): 401–09Costa PB, Ryan ED, Herda TJ, DeFreitas JM,
Beck TW, Cramer JT (2009b) Effects ofstretching on peak torque and the H:Qratio. Int J Sports Med 30(1): 60–5
Malliaropoulos N, Papalexandris S, PapaladaA, Papacostas E (2004) The role ofstretching in rehabilitation of hamstringinjuries: 80 athletes follow-up. Med Sci
Sports Exerc 36(5): 756–59
Marek SM, Cramer JT, Fincher AL et al (2005)Acute effects of static and proprioceptiveneuromuscular facilitation stretching onmuscle strength and power output. J Athl
Train 40(2): 94–103
Morse CI, Degens H, Seynnes OR, MaganarisCN, Jones DA (2008) The acute effect of
stretching on the passive stiffness of thehuman gastrocnemius muscle tendonunit. J Physiol 586(1): 97–106
Rubini EC, Costa AL, Gomes PS (2007) Theeffects of stretching on strength perform-ance. Sports Med 37(3): 213–24
Ryan ED, Beck TW, Herda TJ et al (2008) Thetime course of musculotendinous stiffnessresponses following different durations ofpassive stretching. J Orthop Sports Phys
Ther 38: 632–9
Ryan ED, Herda TJ, Costa PB, Defreitas JM,Beck TW, Stout J, Cramer JT (2009)Determining the minimum number ofpassive stretches necessary to alter musc-ulotendinous stiffness. J Sports Sci 27(9):957–61
Shrier I (2004) Does stretching improveperformance? A systematic and criticalreview of the literature. Clin J Sport Med 14(5): 267–73
Pablo B. CostaDoctoral Research Assistant;
Joel T. Cramer Assistant Proessor,Biophysics Laboratory,Department o Health and Exercise Science,University o Oklahoma,Oklahoma, USA

8/8/2019 Costa Et Al. 2010 - IJTR - Commentary on Behaviour of the Muscle-tendon Unit During Static Stretching Following U…
http://slidepdf.com/reader/full/costa-et-al-2010-ijtr-commentary-on-behaviour-of-the-muscle-tendon-unit 11/11
The challenge o sot tissue
stretching to alleviate pain,
to increase range o motion,
and to decrease the stiness
and the thixotropicproperties
o the whole unit ollowing
injury,isundamentalandcen-
tralorphysiotherapypractice,
andmustbesolvedinorderto
choose the best intervention
programmeorpatients.Since
theirstroleingoodpracticeis
‘donot harm’, twoquestions
that requently come up and
we struggle with are: ‘should
we stretch by any means?’,
and‘howmuchistoomuch?’.
Eventhoughtheconclusiono
thisarticlewasconvincinglyin
support o stretching, it lacks‘scientiic humility’ and some
degreeoprudence.
Applyingstretchingisalways
controversial among praction-
ers.Onemayask:‘whybother
with stretching?’. Previous
studies have indicated that
during passive stretching o
the gastrocnemius muscle,
only a small percentage (less
th an 2 5% ) o th e ov eral l
length(i.e.,theasciclelength-
ens,andconsequentlytheten-
don) change,and these small
changes are not maintained
minutesater the intervention
ceases. On the other hand,
some believethat recovery o
the muscle tendon complex
mightbeacceleratedbyapply-
ingstretching.
Themuscletendonregionisa
complexunit,bothanatomically
and biomechanically, and one
mustalwaysabolishthepoten-
tial or urther muscle-tendon
injuriesduringastretch.
Themyotendinousunitplays
animportantroleinorcetrans-missionrom myobrilsacross
themusclecellmembrane,to
the extracellular matrix, and
thantothetendon.Themag-
nitude o the orce transmit-
ted rom muscle to tendon
is directly infuenced by the
unique, complex and ragile,
structureothisunit.
As well-described by many
investigators, during stretch-
ing, a) the quiescent/inactive
brocytes in the myo-tendon
region are replaced by acti-
vated broblasts; b) there is
anincreaseinbasementmem-
branes in the myo side; and
c)thereisenlargementothe
rough sarcoplasmic reticulum.
The basement membrane is
modied by the presence o
caveolae and vacuoles, and
at the tendon side, the col-
lagen bundles are disrupted,
resulting in the ormation o
disorientedbres.
These apparently adaptive
changes to stretching are a
non-infammatory reaction othemyo-tendonregion,charac-
terizedby intensivemembrane
renewal and recycling. Yet,
rom the mechanical point o
viewthis local response might
permanentlyweakenthemyo-
tendon resistance to stretch,
and result in intererence or
obstruction o the electrome-
chanicaldelay, in terms o the
extent o myotendon complex
loose.So,inalongrunwemay
losemorethanwegain.
As long as a denite and
explicitanswerdoesnotexist,
w he n p re sc ri bi ng s tr et ch
exercises to our patients, it
is important to use cautious
steps. These should consider
severalactors: intensity: how
intense should the stretch be
–isitpain-ree;duration:how
longshouldthestretchbeheld
(slowandprolongedupto20
seconds); and requency: how
otenshouldoneperormthe
stretch(5–6timesperweek).
Dr Eli Carmeli Proessor,Physical Therapy Department,Sackler Faculty o Medicine,Stanley Steyer School o HealthProessions,Tel Aviv University,Israel [email protected]
Karina McGann
Text takes a holistic approach to
the assessment and management of
pain and its multi-dimensional nature
Includes pharmacological and
non-pharmacological approaches
Patient-centred and evidence based
essential text on the management
of painISBN-13: 978-1-85642-292-5;
234 x 156 mm; paperback; 176 pages;
publication January 2007; £19.99
To claim your discount call
01722 716 935and quote code: QBJA Offer expires 30 April 2010
To find out more about Quay books titles visit www.quaybooks.co.uk
Fundamental Aspects of
Pain Assessmentand ManagementKarina McGann
Fundamental Aspects of Nursing series
O n l y
£1 4. 9 9
S P E C I A L O F
F E R
2 5 % O F F
142 InternationalJournaloTherapyandRehabilitation,March2010,Vol17,No3
Research