Spinal Cord, Spinal Nerves A&P lab Dr. Kandula. Anatomy of Spinal Cord.
Upload
truongtrucCategory
view
213download
0
Cost study on spinal cord injury
rehabilitation care in Sweden
Version: Final
Date: 2014-05-12
Quantify Research Authors
Name: Anders Gustavsson Name: Linda Karlsson Title: Partner Title: Senior Researcher Phone +46 70 715 7863 Phone +46 70 982 3725 E-mail: [email protected] E-mail: [email protected] Name: Stefanie Luthman Title: Researcher Phone +46 76 834 2262 E-mail: [email protected]

1
Table of contents
1. Introduction ............................................................................................................... 4
1.1 Background .............................................................................................................................. 4
1.2 Rationale .................................................................................................................................. 4
1.3 Objectives ................................................................................................................................ 5
2. Methods .................................................................................................................... 5
2.1 Questionnaire to clinics ........................................................................................................... 5
2.1.1 Development and distribution of questionnaire ............................................................. 5
2.1.2 Responding clinics ........................................................................................................... 5
2.1.3 Primary rehabilitation...................................................................................................... 6
2.1.4 Re-admissions .................................................................................................................. 7
2.1.5 Outpatient and day care visits ......................................................................................... 8
2.1.6 Staff ................................................................................................................................. 9
2.1.7 Facilities at the clinic ..................................................................................................... 11
2.2 Questionnaire to SCI-specialists ............................................................................................ 13
2.3 Unit costs ............................................................................................................................... 15
2.4 Model .................................................................................................................................... 16
3. Results ..................................................................................................................... 16
3.1 Base case analysis .................................................................................................................. 16
3.1.1 Care provision ................................................................................................................ 16
3.1.2 Staff resources and facilities .......................................................................................... 18
3.1.3 Costs .............................................................................................................................. 20
3.2 One-way sensitivity analysis .................................................................................................. 21
3.2.1 Sensitivity analysis 1: Including total number of visits when determining number of
full-time employees in decentralised care .................................................................................... 22
3.2.2 Sensitivity analysis 2: Assuming equal occupancy rates in decentralised and centralised
care 22
3.2.3 Sensitivity analysis 3: Assuming the SCI-experts underestimated the true staff-need
with 10%, hence increasing the full-time employees needed by 10% in centralised care ........... 22
3.3 Multi-way sensitivity analysis ................................................................................................ 23
3.3.1 Sensitivity analysis 4 ...................................................................................................... 23
3.3.2 Sensitivity analysis 5 ...................................................................................................... 24
4. Discussion ................................................................................................................ 25
4.1 Staffing costs ......................................................................................................................... 25

2
4.2 Acute care costs .................................................................................................................... 25
4.3 Facility costs .......................................................................................................................... 26
4.4 Re-admissions and outpatient visits ...................................................................................... 26
4.5 Care at home ......................................................................................................................... 26
4.6 Other benefits ....................................................................................................................... 27
4.7 Model limitations .................................................................................................................. 27
4.8 Conclusions ............................................................................................................................ 28
5. References ............................................................................................................... 29
6. Appendix A: Questionnaire to clinics ........................................................................ 30
7. Appendix B: Questionnaire to SCI-specialists ............................................................ 38

3
Study Glossary
Term Definition
Average Arithmetic mean
DRG diagnosis-related-groups
ESCIF European Spinal Cord Injury Federation
KPP Cost per patient
SCI Spinal Cord Injury
SCIC Spinal Cord Injury Centre
Weighted average Average based on number of patients in primary
rehabilitation 2012 or number of incident patients in 2012

4
1. Introduction
1.1 Background
Spinal cord injuries are damage or trauma to the spinal cord that results in a loss or impaired
function causing reduced mobility or sensibility. Common causes of a spinal cord injury are falls,
diving accidents, car accidents or disease [1]. While the incidence of spinal cord injury (SCI) is
relatively low, the physical, medical, psychological, social and financial consequences of such injuries
are highly complex and, potentially, devastating for the injured person and his/her family [2]. It is
therefore important for these patients to receive the best care possible to make their re-integration
back into society after injury as successful as possible.
The rehabilitation care of SCI-patients today is decentralised to 20-30 different hospitals around the
country. These clinics do not only care for SCI-patients but also care for other patients in primary
rehabilitation (e.g. patients with stroke and traumatic brain injuries). The Swedish Association for
Survivors of Accident and Injury (RTP) [3] has for a long time worked for the establishment of
centralised rehabilitation care for SCI-patients in Sweden. By centralizing the care for SCI-patients to
2-4 spinal cord injury centres (SCIC), these centres would specialize on SCI-care and possibly be able
to provide better care for this specific patient group. Centralization also enable specialisation of staff,
more focus on research and innovation, knowledge and information pooling, availability of role
models during rehabilitation (so called peer-support) and economies of scale. A thorough description
of centralised care, what it should include and potential benefits are presented in a report from the
European Spinal Cord Injury Federation (ESCIF) [2]. ESCIF and its members also work to promote
centralised care of SCI-patients [4] which today is available in other countries such as Denmark,
Norway, Switzerland, the United States and Australia.
1.2 Rationale
Although many experts seem to agree that centralization would lead to better care for SCI-patients,
little or no evidence of the potential benefits are available. This may be explained by the low
incidence of SCI and high variation in the injury, opportunities for rehabilitation and outcomes of the
patients. These factors make any comparative study on alternative interventions within Sweden (e.g.
decentralized or centralized care) very difficult. Comparisons across countries are also difficult to
interpret because there are a range of differences in care structure and other circumstances which
may all be potential causes of any differences in outcomes.
In absence of feasible ways of showing that centralisation causes improved care for SCI patients, this
study will focus on the potential changes in costs by centralization of SCI-care. By learning more
about the costs of centralization, decision makers will have more information at hand when
considering centralization. Estimations of costs will necessarily need to be estimated aided by
assumptions because we don’t know how an actual centralised organisation would turn out, what
resources would be needed exactly and what potential effects the centralisation process would have
on today’s care providers. For this reason, an economic model was developed, combining available
data and various assumptions to estimate care and resource needs as well as their costs.
5
1.3 Objectives
The aim of this study was to compare the available resources and costs for today’s decentralised care
of SCI-patients with the resources and costs that are expected to be needed in a hypothetical
scenario where the care of the same patients would be centralised to fewer sites. The study aims to
answer the below listed questions:
What are the available resources and costs for rehabilitation of SCI-patients in Sweden today?
How would a hypothetical centralised care of SCI-patients in Sweden be organised regarding
resources and costs?
What differences in total costs are expected with centralised care?
Is there a difference between costs for today’s decentralised care and for a hypothetical
centralised care?
2. Methods
Two questionnaires were prepared to collect data on the current and potential care and resource use
in today’s decentralised scenario and a hypothetical centralised scenario, respectively (see
appendices A and B). These data were analysed and the results are summarised below. Data on costs
of units of resources were derived from price lists and other publicly available sources, and also
summarised below. The responses from the questionnaire and the unit costs where then used as
inputs in a model comparing rehabilitation care today (decentralised care) and a hypothetical SCIC
scenario (centralised care). The model used is presented in section 2.4.
2.1 Questionnaire to clinics
2.1.1 Development and distribution of questionnaire
The questionnaire was developed by Quantify Research together with SCI-specialists [5-8] and an
expert from Personskadeförbundet RTP [9] to capture all relevant resource use both related to all
care at the clinic and to SCI-patients only. The questionnaire included questions regarding primary
rehabilitation, re-admissions, outpatient visits, day care visits, staff and facilities at the clinic (see
appendix A). Twenty-six clinics were identified and considered for inclusion. Three clinics were
excluded (Mälarsjukhuset Eskilstuna, Skaraborgs sjukhus in Skövde and Södra Älvsborg Sjukhus in
Borås) for the following reasons; one did not report any patients in primary rehabilitation, one sent
in the questionnaire after all the analyses had been conducted and one referred all SCI-patients to
other hospitals and did therefore not have any SCI-patients. Before distributing the questionnaire,
the clinics were contacted by phone and asked to participate. The questionnaire was thereafter e-
mailed to the clinics, and they were reminded both by e-mail and phone if not responding in time.
2.1.2 Responding clinics
Of the remaining 23 clinics, 20 responded (response rate = 87%) and the responding clinics are listed
below:
Akademiska sjukhuset in Uppsala
Blekingesjukhuset in Karlshamn
Centralsjukhuset in Karlstad

6
Karolinska Universitetssjukhuset in Stockholm
Länssjukhuset Centrallasarettet in Växjö
Länssjukhuset in Halmstad
Länssjukhuset Sunderby in Luleå
Länssjuhuset Sundsvall/Härnösand
Länssjukhuset Ryhov
Norrlands Universitetssjukhus (NUS), Umeå
RehabStation Stockholm
Rehabiliteringsenheten, Sahlgrenska Universitetssjukhuset in Gothenburg
Ryggmärgsskadeenheten, Sahlgrenska Universitetssjukhuset in Gothenburg
Sandvikens sjukhus
Skånes Universitetssjukhus in Höör
Stockholms sjukhem
Universitetssjukhuset in Linköping
Universitetssjukhuset in Örebro
Västmanlands sjukhus in Västerås
Östersunds sjukhus
Time constraints were the main reason for three clinics not participating (Falu lasarett, Uddevalla
sjukhus and Västerviks sjukhus). In the following sub-sections preliminary variables received from the
questionnaire are described and the majority of these were later used as input in the model
described in section 2.4.
2.1.3 Primary rehabilitation
The number of patients and length of stay in primary rehabilitation are presented in Table 1. In total
2,310 patients (18 responding clinics) were in primary rehabilitation during 2012 (including all
patients at the clinic irrespective of whether a spinal cord injury was the cause of rehabilitation). We
did not ask how many of these were hospitalised in 2012 (i.e. incident patients) but they can be
estimated to 1,960 patients assuming that the average length of stay did not change over time.
Table 1 Primary rehabilitation in today’s decentralised care of SCI-patients
Number of
responding clinics
Mean Sd Min Median Max Adjusted mean
1
Average number of patients in primary rehabilitation during 2012 per clinic
All patients 182 128.3 108.1 35 86 471
SCI-patients 20 21.1 21.5 1 10 65
Average number of incident patients in 2012 per clinic3
All patients 182 108.9 93.6 30 72 391
SCI-patients 20 17.5 17.8 1 8 50
Average number of days per hospitalisation in primary rehabilitation per patient
All patients 18 39.1 14.9 14.2 37 64
SCI-patients 15 58.5 26.4 27.8 51 120.4 61.7
1. Adjusted mean across all responding clinics based on total number of SCI-patients and their average care time at each clinic. 2. Two clinics only reported results for their SCI-patients. 3. Estimated assuming that the average length of stay did not change over time.

7
Considering SCI-patients only; 20 clinics reported a total of 422 patients in primary rehabilitation
during 2012 and the estimated number of incident patients in 2012 was 350. Transferring from one
clinic to another during a patient’s primary rehabilitation was not captured in the questionnaire.
Based on the SCI-specialists knowledge regarding transfers it was assumed that the total adjusted
number of incident SCI-patients in 2012 was about 270 (13.5 incident patients per clinic).
To estimate the length of stay for patients in primary rehabilitation the questionnaire included a
question regarding the average number of days per hospitalisation at the clinic. The weighted
average across all clinics (based on number of SCI-patients in primary rehabilitation in 2012 and their
average hospitalisation time in each clinic) was 61.7 days. The average total number of days in
primary rehabilitation (including potential transfers) was estimated to 80 days. This was calculated by
multiplying the weighted average number of days per hospitalisation per clinic (61.7) with the total
number SCI-patients in all responding clinics (350) and dividing by the estimated number of unique
incident patients (270).
2.1.4 Re-admissions
Table 2 Re-admissions in today’s decentralised care of SCI-patients
Number of
responding clinics
Mean Sd Min Median Max Adjusted
mean
Number of re-admissions per clinic
All patients 12 19.6 28.2 0 5 76
SCI-patients 13 10.2 17.7 0 2 58 21.31
Average number of days per hospitalisation for re-admitted SCI-patients
SCI-patients 82 23.5 22.7 5 18 77 13.5
3
1. Adjusted mean across all responding clinics based on the number of incident SCI-patients 2012 in primary rehabilitation. 2. Eight clinics reporting at least one re-admission. 3. Adjusted mean across all responding clinics based on number of re-admissions and total hospitalisation time for these re-admissions at each clinic.
Re-admissions during 2012 were also asked for in the questionnaire and the results are summarised
in Table 2. A total of 235 re-admissions (12 responding clinics) were reported for all patients at the
clinics with an average of 19.6 re-admissions per clinic. Considering SCI-patients, there were 133 re-
admissions (13 responding clinics) with an average of 10.2 re-admissions per clinic. Weighting the
average number of re-admissions based on the clinic’s size (number of incident SCI-patients in
primary rehabilitation) resulted in a weighted average of 21.3 re-admissions for SCI-patients per
clinic. The weighted average number of days per hospitalisation at the clinics for re-admitted
patients was estimated to 13.5 days (based on the eight clinics reporting re-admitted SCI-patients). In
addition, for the eight clinics, a ratio of re-admissions / primary rehabilitations in 2012 was
calculated. No clear pattern between re-admissions and primary rehabilitation for SCI-patients was
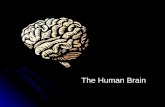
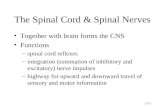
seen between larger/smaller clinics (see Figure 1).

8
Figure 1 Correlation between number of admissions and patients in primary rehabilitation.
2.1.5 Outpatient and day care visits
Clinics were asked to report the total number of outpatient and day care visits (including for example
physician visits for prescription of medical drugs, physiotherapist/occupational therapist training
visits and nurse visits for care of pressure sores). Table 3 presents outpatient and day care visits
separately and in total. The total row in Table 3 includes 6 clinics which were not able to separate
outpatient/day care visits and/or to separate SCI-patients’ visits from the total number of visits.
A problem with the above results was that several clinics with outpatient/day care visits had only
reported physician visits excluding any other outpatient/day care visits. Therefore calculations were
also performed by only including 7 clinics reporting the complete range of possible visits, raising the
mean number of outpatient/day care visits from 566 to 1316. In addition, a weighted (based on
number of incident SCI-patients in 2012) average ratio (0.7) was calculated as number of visits
divided by number of primary rehabilitation days in 2012 for the reporting clinics which had at least
one outpatient or day care visit.
Table 3 Outpatient and day care visits for SCI-patients
Number of
responding clinics
Mean Sd Min Median Max Ratio1
Number of visits per clinic
Outpatient visits 9 313.9 322.4 0 271 1004
Day care visits 5 140.4 209.1 5 65 510
All visits2 20 566.1 1532.4 0 81 6960
All visits only including
clinics reporting all possible
visits
7 1316.2 2520.0 0 361 6960 0.7
1. Weighted average ratio of outpatient and day care visits divided by total number of hospitalisation days in primary rehabilitation for SCI-patients in 2012 at responding clinics. 2. Outpatient and/or day care visits.
0
0.5
1
1.5
2
2.5
0 10 20 30 40 50
Nu
mb
er
of
re-a
dm
itte
d S
CI-
pat
ien
ts /
n
um
be
r o
f SC
I-p
atie
nts
in p
rim
ary
reh
abili
tati
on
20
12
Number of patients in primary rehabilitation 2012

9
2.1.6 Staff
The clinics were asked for number of full-time employees for the below listed groups:
Administrative assistant
Counsellor
Dietician
Head of administration
Nurse
Nursing assistant
Occupational therapist
Psychologist
Physician
Physiotherapist
Rehabilitation assistant
Speech therapist
Urotherapist
Other, please state
They were also asked to state, if possible, percentage of the employees’ time that was intended for
SCI-patients. Seven clinics were able to report how much of their employees’ working time that was
spent on SCI-patients (see Table 4 for number of full time employees working with SCI-patients).
Table 4 Number of full-time employees working with SCI-patients
Number of
responding clinics
Mean Sd Min Median Max
Administrative assistant 6 0.7 0.7 0 0.5 2
Counsellor 7 1.2 0.9 0.5 1 3.1
Dietician 3 0.1 0.1 0 0.1 0.1
Head of administration 6 1.0 1.0 0 0.8 3
Nurse 7 6.3 3.4 1.5 7 10
Nursing assistant 7 8.5 3.4 1.5 9 12.8
Occupational therapist 6 2.9 1.3 2 2.5 5.6
Psychologist 5 0.3 0.2 0 0.5 0.5
Physician 7 1.9 0.8 0.5 2 3
Physiotherapist 7 2.9 1.8 0.5 2.5 6.4
Rehabilitation assistant 4 1.0 0.7 0.5 0.8 2
Speech therapist 1 0 - 0 0 0
Urotherapist 3 0.2 0.2 0 0.3 0.4
To estimate how staff intensive the decentralised clinics were on average, two ratios (number of
employees per 10,000 hospitalisation days) and (number of employees per 10,000 hospitalisation
days and visits) were calculated for each clinic. Two out of the seven clinics (29%) did not have

10
complete information regarding number of outpatient and/or day care visits which resulted in that
the estimated ratio including visits was based on fewer clinics compared with only considering
hospitalisations. In addition, a weighted average of full-time employees per 10,000 hospitalisation
days or per 10,000 hospitalisation days + visits were calculated for each occupation based on the
ratios calculated for each clinic. The weighting was based on number of SCI-patients in primary
rehabilitation 2012. The results are presented in Table 5 and Table 6. As can be seen, nurses and
nursing assistants were the most resource intensive occupations.
Table 5. Number of full time employees working with SCI-patients, per 10 000 hospitalisation days
(both including patients in primary rehabilitation and re-admitted patients)
Number of
responding clinics
Mean Sd Min Median Max Weighted
mean1
Administrative assistant 5 2.7 2.6 0 2.0 6.6 3.2
Counsellor 7 8.8 11.0 1.0 4.8 32.8 5.2
Dietician 2 0.3 0.1 0.2 0.3 0.3 0.2
Head of administration 5 4.3 3.3 1.6 3.8 9.8 4.3
Nurse 7 38.1 30.0 10.8 38.9 98.3 27.1
Nursing assistant 7 46.0 26.3 20.5 38.9 98.3 36.8
Occupational therapist 6 11.2 5.5 4.1 9.5 18.2 10.5
Psychologist 5 1.5 1.2 0 1.6 3.1 1.7
Physician 7 11.8 9.6 4.1 9.7 32.8 8.3
Physiotherapist 7 15.1 8.3 4.1 12.7 29.5 12.4
Rehabilitation assistant 4 11.4 14.3 4.0 4.4 32.8 5.3
Speech therapist 1 0 - - - - -
Urotherapist 3 1.1 1.3 0 0.8 2.5 1.3
1. Weighted mean across all responding clinics based on number of SCI-patients in primary rehabilitation 2012.

11
Table 6. Number of full time employees working with SCI-patients, per 10 000 hospitalisation days
and visits (both including patients in primary rehabilitation/re-admitted patients and
outpatient/day care visits to the clinic)
Number of
responding clinics
Mean Sd Min Median Max Weighted
mean1
Administrative assistant 3 1.9 1.2 0.8 2.0 3.1 1.6
Counsellor 5 3.4 1.1 2.2 3.0 5.1 3.3
Dietician 1 0.3 - 0.3 0.3 0.3 0.3
Head of administration 4 2.6 0.9 1.3 3.0 3.1 2.5
Nurse 5 23.4 16.0 3.3 29.3 38.9 20.6
Nursing assistant 5 30.1 13.9 9.1 38.8 41.0 28.0
Occupational therapist 5 8.5 3.3 5.5 7.3 14.1 7.6
Psychologist 4 1.4 1.0 0.2 1.4 2.6 1.2
Physician 5 6.5 2.6 3.0 6.5 10.3 5.9
Physiotherapist 5 9.7 3.1 6.3 10.1 14.1 9.0
Rehabilitation assistant 2 3.3 0.8 2.7 3.3 3.8 3.0
Speech therapist 0 - - - - - -
Urotherapist 2 1.2 1.3 0.2 1.2 2.1 0.8
1. Weighted mean across all responding clinics based on number of incident SCI-patients in primary rehabilitation 2012.
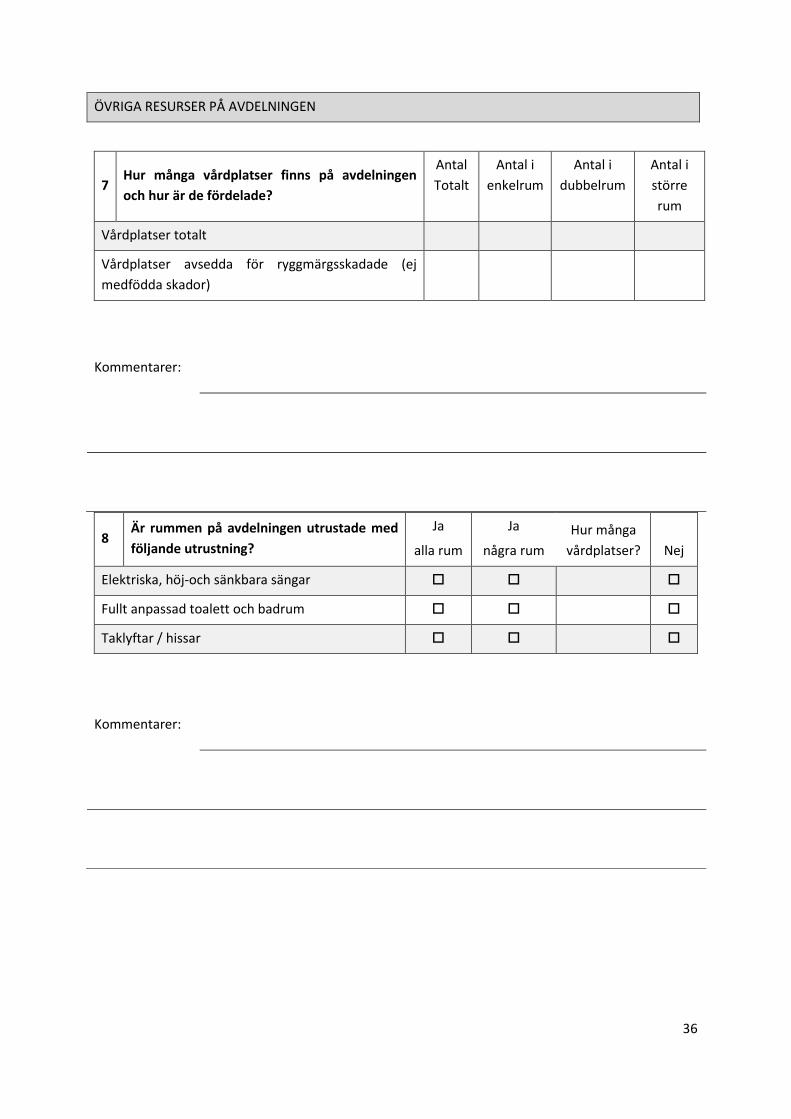
2.1.7 Facilities at the clinic
The clinics were asked how many inpatient beds they had in total and how many of these were
intended for SCI-patients. In today’s decentralised care no beds are “reserved” for SCI-patients,
however these patients are a prioritised group when injured. The occupancy rate for each clinic was
therefore calculated based on all patients and all available beds at the clinics.
According to ESCIF [2] all rooms at a SCIC should be equipped with:
Electric, height-adjustable beds
Fully-adapted toilet and bathroom facilities
Ceiling hoists/lifts and other appropriate aids.
In addition the following facilities should be present:
Access to patients’ mini bus
Access to specialised driving tuition
Day room
Dental facilities
Dining area
Family accommodation
Fitness room and sports hall
Helicopter pad
Internet café
Isolation rooms en-suite

12
Kitchen facilities
Library
Meeting room/consultation room
Offices and facilities for personnel and therapists employed
Outdoor recreational and training facilities
Restaurant (staff, patient, visitor)
Seating and posture clinic
Shop
Swimming pool
Training apartments
Twin bedded rooms en-suite (for patients and carer/personal assistant)
Vocational training facilities
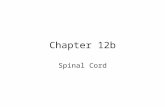
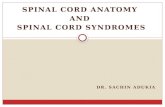
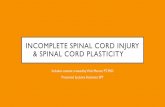
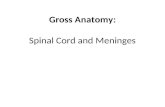
The share of clinics where all rooms were equipped with electric/height-adjustable beds, fully
adapted bathroom facilities and ceiling hoists/lifts are presented in Figure 2, whereas the share of
clinics which had access to the above described facilities are presented in Figure 3.
Figure 2. Share of clinics where all rooms are equipped with ceiling hoists/lifts and other
appropriate aids, fully-adapted toilet and bathroom facilities and electric height-adjustable beds
0% 20% 40% 60% 80% 100%
Electric, height-adjustable beds
Fully-adapted toilet and bathroom facilities
Ceiling hoists/lifts and other appropriate aids.
Share of the clinics where all rooms have the above described equipment

13
Figure 3. Share of the responding clinics which had access to facilities described by ESCIF
2.2 Questionnaire to SCI-specialists
Four SCI-specialists (Håkon Ro, Skåne Universitetssjukhus, Per Ertzgaard, Linköpings
Universitetssjukhus, Claes Hultling, Karolinska Universitetssjukhuset/ Spinalis Stockholm and Richard
Levi, Umeå Universitetssjukhus) [5-8] were given a questionnaire (see appendix B) in which they
were asked to visualise a SCIC in Sweden with the following characteristics:
Primary rehabilitation: SCI-patients are referred to the centre from acute/emergency care once
medically stable and all relevant decisions on surgical interventions have been made. One centre
was assumed to care for approximately 70 incident SCI-patients per year (4 centres in total).
Reintegration in the community resource: The centre is responsible for a patient’s reintegration
in society including contact with the patient’s employer, 24-hour-phone service with physicians,
physiotherapists in general practice and local caregivers, and for conducting home visits in the
patient’s community.
Re-admissions: The centre is responsible for re-admissions of patients that have ended their
rehabilitation at the centre. An estimated 30% of patients in primary rehabilitation are assumed
to be re-admitted during their life-time.
Life-long follow-up: The centre should follow-up on each patient that has ended his/her primary
rehabilitation at the centre on a regular basis including home visits, specialised outpatient care if
needed and contact with local care providers.
Assuming the above, the SCI-specialists were asked questions regarding capacity for re-admissions,
outpatient/day care visits, home-visits, how many inpatient beds and full-time employees that are
needed for each centre in order to maintain the above described scenario.
0%
20%
40%
60%
80%
100%Sh
are
of
clin
ics
that
had
acc
ess
to
th
e b
elo
w
de
scri
be
d f
acili
tie
s

14
Two SCI-specialists (Expert A) completed the questionnaire together and had pictured a SCIC
following the above description and imagined how a future SCIC would be organised in their area of
work (more rural area). Another SCI-specialist (Expert B), working at a SCI-specialist centre in a more
urban area today had looked at how the care of their SCI-patients was managed in 2012 and from
that imagined an increase in patients and resources needed by 35%. Hence, when estimating how
many re-admissions the centre would have capacity for the SCI-expert first considered how many re-
admissions the centre had in 2012 and assumed a 35% increase to arrive at the number of re-
admissions in a centralised scenario. The same calculation was done when estimating number of
hospital beds, number of visits (outpatient/day care/home visits) and staff resources needed. The
results are presented in Table 7 and Table 8.
Table 7. Estimated capacity (by SCI-specialists) for a SCIC assuming 70 incident SCI-patients/year,
centre responsible for patient’s re-integration in society, re-admissions and life-long follow-up of
patients who have completed primary rehabilitation at the centre
Expert A Expert B
Number of re-admissions/year 15 46
Number of outpatient/day care visits 10001 1082
Number of home-visits 5002 128
Number of hospital beds 15 17-18
1. Outpatient visits only (Day care visits could not be estimated). 2. Number based on assumption that half of the SCI-population can go to the SCIC for a visit and the other half needs a home-visit.
Table 8. SCI-specialists estimated number of full-time employees at the SCIC
Expert A Expert B
Administrative assistant 2.5 2
Counsellor 2 3
Dietician 1 1
Head of administration 3 2
Nurse * 8.5-9
Nursing assistant * 13.3-17.3
Occupational therapist 6 6
Psychologist 1 1
Physician 6 3.5
Physiotherapist 7 6
Rehabilitation assistant 2 2
Speech therapist 0.2 1
Urotherapist 1 2
* Could not be estimated

15
2.3 Unit costs
Average salaries for different types of staff were collected from Statistics Sweden [10] and were
adjusted (+48%) to include social security contributions paid by the employer [11]. Total yearly
salaries are presented in Table 9.
Table 9. Average yearly salaries for employees including social fees
Salary (SEK)
Administrative assistant 526,655
Counsellor 507,083
Dietician 512,421
Head of administration 652,091
Nurse 541,482
Nursing assistant 434,135
Occupational therapist 482,174
Psychologist 619,176
Physician 1,047,972
Physiotherapist 487,512
Rehabilitation assistant 462,602
Speech therapist 535,551
Urotherapist 541,482
The yearly cost for one inpatient bed excluding staff resources and inventories was estimated in
discussion with Maria Karlberg at Skåne University hospital [12]. The Spinal Cord Injury clinic at Skåne
University hospital rent their premises (including 12 hospital beds, meeting rooms, dining areas, and
offices for physicians/nurses/nursing assistants) for a total of 1.3 million SEK yearly. In addition the
unit has a training facility together with three other clinics for a total cost of 6 million SEK yearly
which is divided equally between the clinics (1.5 million per clinic). The training facilities include for
example training rooms for occupational therapists/physiotherapists, fitness room, pool, conference
and separate training rooms. The above information resulted in a total cost of 233,333 SEK (1.5+1.3
million SEK divided by 12) per inpatient bed excluding staff resources.
The cost for SCI-patients’ time spent in acute care was calculated using the “cost per patient” (KPP)-
database available from the Swedish Association of Local Authorities and Regions (SKL) [13]. The KPP-
database covers around 70% of the care episodes in the Swedish inpatient care and is built on
“diagnosis-related-groups” (DRG) which is an administrative method to group care-contacts. To track
costs for SCI-patients in the acute phase, DRG-codes of 004 (surgeries on spinal cord and surrounding
tissue) and 009 (sickness and injuries related to the spinal cord) was searched for in the KPP-
database. These DRG-codes correspond to the following main diagnoses in the ICD-10 system: S140,
S141, S142, S143, S240, S241, S243, S340, S341, S342 and S343. A total of 4,093 hospitalisation days
corresponding to 135 care episodes were located for these codes with a total cost of 40.3 million
SEK. This resulted in an average cost per care-episode of 299,000 SEK.

16
An average from regional pricelists from Uppsala läns landsting [14] and Södra regionsnämnden [15]
was used when pricing primary care visits to a physician (SEK 1,541). The cost of a visit to
physiotherapists, occupational therapists and nurses was not reported separately but assumed to be
the same (SEK 530).
2.4 Model
An economic model was developed combining the data discussed in this method section to estimate
the care provision, resource use and costs for the decentralised and centralised scenario,
respectively. The model was based on the questionnaires and accounted for primary rehabilitation,
re-admitted patients and patients visiting the clinics/future SCIC for outpatient and day care visits. A
lot of assumptions were needed to fill gaps in the collected questionnaires where the respondents
could not give any answer. These assumptions have been detailed below. The model did not consider
that patients may transfer from one clinic to another during their primary rehabilitation. The model
captured resources (including staff) needed to care for the estimated number of SCI-patients. Apart
from the information received from the questionnaires the model also accounted for acute care and
long-term care in the community setting. The different parts of the model and its results are
presented in detail in section 3.
3. Results
The model was based on the questionnaires and built in order to capture (as far as possible) all
relevant parts/costs of care for SCI-patients. The care provided in the twenty responding clinics in
today’s scenario was compared to a hypothetical centralised scenario with 4 SCICs. Four SCIC was
estimated to be needed based on 270 incident SCI-patients per year. The model can be divided into
three different parts:
Care provision
Resources
Costs
Much of the data inputs going into the model are uncertain. We therefore first present a base case
analysis which is a “best guess” based on input received from the questionnaires and key
assumptions. Thereafter, the model inputs are modified in a set of sensitivity analyses showing how
the results may change using different assumptions where there is uncertainty.
3.1 Base case analysis
The results from the base case analysis is presented in Table 10 and discussed below.
3.1.1 Care provision
Based on section 2.1.2 it was assumed that there were 270 incident SCI-patients in Sweden each year
resulting in 13.5 incident patients per centre today and 67.5 patients per SCIC. In discussion with SCI-
experts it was assumed that 7000 prevalent SCI-patients live in Sweden. Incident SCI-patients were
assumed to stay in primary rehabilitation for 80 days on average in both the decentralised and
centralised scenario. This resulted in a total of 21,592 hospitalisation days in primary rehabilitation in

17
both scenarios with 1,080 hospitalisation days per clinic (20 in total) today and 5,398 hospitalisation
days per SCIC (4 in total).
No clear correlation between re-admissions and primary rehabilitation for SCI-patients was seen
comparing larger and smaller clinics (see Figure 1). Therefore, we used the average number of re-
admitted patients (10.2) rather than the weighted average (21.3) when estimating number of re-
admitted patients per year and clinic for decentralised care in the model. For centralised care, the
SCI-experts estimations varied from 15 to 46 re-admissions per centre. Expert B’s estimation of 46 re-
admissions per year and centre was used in the base case analysis after agreement from Expert A.
The weighted average length of stay for re-admitted patients (13.5) retrieved from the questionnaire
was used for both decentralised and centralised care when calculating number of hospitalisation
days for each scenario. A total of 2,754 hospitalisation days for decentralised care (138 per clinic) and
2,484 hospitalisation days for centralised care (621 per SCIC) were estimated.
Common reasons to why SCI-patients may need to see a physician, nurse, physiotherapist etcetera in
an outpatient or day care setting are urinary tract infections (UTI), pressure sore assessment,
prescriptions, nociceptive- neurogenic pain, autonomic dysreflexia, orthostatic hypotension, legal
matters, fecal/urinary incontinence, life style associated disorders and neurological assessment.
There are no data available on how often these visits occur in practice today but there is
undoubtedly high variation across patients. When estimating the number of outpatient and day care
visits per clinic in today’s decentralised care the ratio (number of visits divided by number of
hospitalisation days in primary rehabilitation 2012) described in section 2.1.2 was multiplied with the
total estimated number of hospitalisation days in primary rehabilitation per clinic (1,080). This
resulted in a total of 15,468 visits (773 visits per clinic, 20 clinics). For the centralised scenario, the
SCI-experts’ estimations regarding visits (including outpatient, day care and home visits) varied from
~1,200 to ~1,500 per SCIC. In the base case model it was assumed that each SCIC had 1,500 visits,
resulting in a total of 6,000 visits. This resulted in a difference of ~9,500 visits between decentralised
and centralised care. In a centralised scenario, it is anticipated that many of these visits will take
place in primary care instead. Because many patients will have farther to travel to a SCIC, they are
assumed to go to a local care provider with some of their needs. It is unknown how many primary
care visits SCI-patients have on average during a year. In the model, we assume that SCI-patients on
average see a general practitioner 2 times a year and a physiotherapist, nurse or occupational
therapist 5 times a year in a primary care setting. It is furthermore assumed that 95% of the 9,500
fewer visits in centralised care would take place in primary care instead and that half of these
additional primary care visits are to a physician and the other half to a physiotherapist, nurse or
occupational therapist. A 5% decrease in total outpatient, day care, home and/or primary care visits
is expected in a centralised scenario.
Due to the longer transportation (in some cases) between acute care and primary rehabilitation, SCI-
patients in a centralised scenario are assumed to stay longer (5%) in acute care compared with a
decentralised setting.

18
Table 10. Estimated care of SCI-patients in decentralised and centralised care
Care for SCI-patients Decentralised Centralised
Number of incident patients 270 270
Number of centres 20 4
Average number of incident patients per centre 13.5 67.5
Number of prevalent patients 7,000 7,000
Primary rehabilitation
Number of unique admissions in primary rehabilitation per centre1 13.5 67.5
Average number of days per hospitalisation in primary rehabilitation2 80 80
Total number of hospitalisation days in primary rehabilitation per centre3 1,080 5,398
Long-term follow-up
Total number of re-admissions per centre4 10.2 46.0
Average number of re-admissions per primary rehabilitation5 0.8 0.7
Average number of days per hospitalisation for re-admitted patients6 13.5 13.5
Total number of hospitalisation days for re-admitted patients per centre7 138 621
Total number of hospitalisation days per centre8 1,217 6,019
Total number of outpatient and day care visits9 per centre 773 1,500
Number of visits per hospitalisation days10
0.64 0.25
1. 270/20 vs. 270/4 2. Based on assumption on the share of patients transferring from one clinic to another and the weighted average hospitalisation time for a clinic. 3. 13.5*80 vs. 67.5*80 4. Average number of visits from the questionnaire to clinics vs. SCI-experts estimation of number of re-admitted patients to a SCIC. 5. Total number of re-admissions per centre divided by average number of incident patients per centre. 6. Weighted average of days per hospitalisation for re-admitted patients. Retrieved from the questionnaire to clinics and based on centres reporting at least one re-admitted SCI-patient. 7. 10.2*13.5 vs. 46*13.5, 8. Including both patients in primary rehabilitation and re-admitted patients 9. Outpatient and day care visits. Home visits are included in centralised care, but were not captured in the questionnaire to the clinics. 10. Total number of visits divided by total number of hospitalisation days per centre.
3.1.2 Staff resources and facilities
In the base case scenario it was decided to use staff weighted ratios calculated using hospitalisation
days only compared with including outpatient and day care visits as well (see section 2.1.2). This was
decided due to the fact that estimations including more clinics could be utilised. However, including
visits as well for the staff calculation was accounted for in sensitivity analyses.
The weighted ratios for each occupation were multiplied with the estimated total number of
hospitalisation days (1,217) per centre in order to estimate average number of staff for one
decentralised centre. For the centralised scenario the SCI-experts estimated how staff-intensive a

19
SCIC would be, based on the description presented in section 2.2. In situations where the SCI-experts
gave different estimates, an average number of staff was calculated with the following exceptions:
Expert B’s estimations for nurses and nursing assistants were used since Expert A had not estimated
these. In addition, Expert A’s answer for total number of physicians was used since their estimates
had included time for research.
Table 11. Number of full-time employees per centre and per 10,000 hospitalisation days in the
base case model for decentralised and centralised care
Full time employees per centre Full-time employees per 10,000
hospitalisation days
Number of full-time employees Decentralised Centralised Decentralised Centralised
Administrative assistant 0.4 2.3 3.2 3.7
Counsellor 0.6 2.5 5.2 4.2
Dietician 0.03 1.0 0.2 1.7
Head of administration 0.5 2.5 4.3 4.3
Nurse 3.3 9.0 27.1 15.0
Nursing assistant 4.5 17.3 36.8 28.7
Occupational therapist 1.3 6.0 10.5 10.0
Psychologist 0.2 1.0 1.7 1.7
Physician 1.0 6.0 8.3 10.0
Physiotherapist 1.5 6.5 12.4 10.8
Rehabilitation assistant 0.6 2.0 5.3 3.3
Speech therapist 0.0 0.6 0 1.0
Urotherapist 0.2 1.5 1.3 2.5
Total number of full-time employees per centre 14.2 58.2 - -
Total number of full-time employees for all
centres
284.0 232.8 - -
Total number of full-time employees per 10,000
hospitalisation days
- - 116.3 96.9
The results from the staff calculations are presented in Table 11. In both the decentralised and
centralised scenario, nurses and nursing assistants were the most resource intensive occupations.
Including all occupations, a total of 14.2 full-time positions per centre (284 in total) were estimated
in decentralised care and 58.2 full-time positions per centre (233 in total) in centralised care. Hence,
a 20% lower staff need was seen in a hypothetical centralised care compared to today’s
decentralised care. Possible explanations to this difference are discussed in section 4.
The results of average occupancy rate and average number of hospital beds needed are shown in
Table 12. The SCI-experts estimations of needed number of hospital beds per SCIC varied between 15
and 18. In the base case model it was assumed that an average of 17 hospital beds was needed at
each SCIC. Together with the calculated total number of hospitalisation days for SCI-patients during
2012 (both in primary rehabilitation and for re-admitted patients) this resulted in a total occupancy

20
rate of 95%. For decentralised care, the total occupancy rate for all patients was calculated using the
number of hospital beds and the estimated total number of patients in primary rehabilitation 2012
and re-admitted patients. Two clinics had not reported total number of patients and were therefore
excluded from this calculation. For the clinics which were unable to report re-admissions these were
estimated by using the weighted average ratio of total number of re-admissions/all patients in
primary rehabilitation 2012 (0.4) for the clinics which reported both. This ratio was thereafter
multiplied with the number of patients in primary rehabilitation 2012 to receive the estimated
number of re-admitted patients per clinic. Thereafter the weighted average of hospitalisation days
for all re-admitted patients (13.8) was multiplied with the estimated number of re-admitted patients
to get total hospitalisation days. The estimates of number of hospital beds and total hospitalisation
days in primary rehabilitation/re-admissions resulted in a weighted average occupancy rate of 87%
with a total need of 4 hospital beds per clinic.
Table 12. Occupancy rates for decentralised and centralised care
Decentralised Centralised
Assumed bed occupancy rate 87% 95%
Number of hospital beds per centre 4 17
Total number of hospital beds for all centres 76 68
3.1.3 Costs
Table 13. Summary of the costs for decentralised and centralised care
Per incident patient
(SEK)
Per centre
(million SEK)
The whole country
(million SEK)
Decentralised Centralised Decentralised Centralised Decentralised Centralised
Acute/
emergency care
299,000 313,950 4.0 21.2 80.7 84.8
Centre
-Staff 558,228 474,175 7.5 32.0 150.7 128.0
-Facilities 66,485 58,765 0.9 4.0 18.0 15.9
Subtotal 624,713 532,941 8.4 36.0 168.7 143.9
Care at home 148,607 182,197 2.0 12.3 40.1 49.2
Total 1,072,320 1,029,088 14.5 69.5 289.5 277.9
Change with
centralised care
-43,233 54 -12

21
A summary of the costs for decentralised and centralised care is presented in Table 13. The cost for
acute care was estimated to be 5% higher per patient in a centralised setting compared to a
decentralised setting due to longer transportations to reach a SCIC. For the whole country this
resulted in a cost difference of 4 million SEK. Costs for staff resources were estimated to be higher in
decentralised care compared to centralised care. Per patient a cost difference of ~84,000 SEK was
seen and cost-savings in a centralised scenario were estimated to a total of 23 million SEK. Costs for
facilities were higher in a decentralised setting with a difference of 2 million SEK in the whole country
compared with a centralised setting. Due to the increase in primary care visits in a centralised setting
this cost was estimated to be higher in a centralised scenario compared to decentralised care (total
cost difference: 9 million SEK). In summary, the total costs of care for SCI-patients would according to
our base case model be lower (-12 million SEK) with centralised care compared with decentralised
care. The cost savings can mostly be derived to the lower staff costs in a centralised scenario.
3.2 One-way sensitivity analysis
We performed two types of sensitivity analyses; one-way and multi-way. In a one-way sensitivity
analysis certain parameters are varied to see how this specific parameter would impact the results,
whereas in a multi-way sensitivity analysis more than one parameter is changed at the same time.
The following sections present the results from three one-way and two multi-way sensitivity
analyses.
Table 14. One-way sensitivity analyses. The results are presented for the whole country in million
SEK.
Base case analysis Sensitivity analysis 1
1
Sensitivity analysis 2
2
Sensitivity
analysis 33
Decentralised Centralised Decentralised Decentralised Centralised
Acute/emergency
care
80.7 84.8 80.7 80.7 84.8
Centre
-Staff 150.7 128.0 176.6 150.7 140.8
-Facilities 18.0 15.9 18.0 16.4 15.9
Subtotal 168.7 143.9 194.6 167.1 156.7
Care at home 40.1 49.2 40.1 40.1 49.2
Total 289.5 277.9 315.4 288.0 290,7
Change with
centralised care
-12 -38 -10 1
1. Including total number of visits when determining number of full-time employees in decentralised care. 2. Assuming the same occupancy rate in decentralised and centralised setting. 3. Assuming that the SCI-experts underestimated the true staff need with 10%.

22
The results from the one-way sensitivity analyses are presented in Table 14 together with the results
from the base-case analysis in order to ease comparisons.
3.2.1 Sensitivity analysis 1: Including total number of visits when determining number of full-time employees in decentralised care
Estimation of number of full-time employees could either be done by using a ratio based on
hospitalisation days or by also including total number of visits (see section 2.1.2). In the base case
analysis, estimation of full-time employees in decentralised care was estimated based on number of
hospitalisation days but not visits (outpatient and day care) to the clinic. In this sensitivity analysis
visits are included in the staff calculation and the estimations of total staff need are therefore based
on 6 clinics since the remaining 2 did not report all possible visits in their answers. It is also assumed
that one visit has the same resource need as one hospitalisation day. To estimate the total number of
full-time employees based on both hospitalisations and visits, the weighted ratios for each
occupation were multiplied with the estimated total number of hospitalisation days and visits (1,990)
per decentralised centre.
When considering visits in the staff calculation a higher number of full-time employees per centre
were estimated in decentralised care compared with not including visits (a total of 16.7 vs. 14.2 full-
time employees per centre). This corresponds to a 17% increase in total decentralised care staff costs
(from 151 to 177 million SEK) and even higher cost-savings compared with the base case analysis (38
million SEK vs. 12 million SEK) for centralised care vs. decentralised care.
3.2.2 Sensitivity analysis 2: Assuming equal occupancy rates in decentralised and centralised care
The occupancy rate in the decentralised base case scenario was estimated based on the clinics
occupancy rates for all patients cared for at the clinic. It is possible that the occupancy rate would
have been higher if it would have been possible to only consider SCI-patients at the clinics.
Assuming that both decentralised and centralised care had an occupancy rate of 95% (estimated in
centralised care based on the SCI-experts input) resulted in similar hospital bed costs in a
decentralised and centralised scenario. The difference in total cost between centralised and
decentralised care decreased by 2 million SEK compared with the base case analysis (10 million in
cost-savings for centralised care vs. decentralised care compared with 12 million in the base case
analysis).
3.2.3 Sensitivity analysis 3: Assuming the SCI-experts underestimated the true staff-need with 10%, hence increasing the full-time employees needed by 10% in centralised care
In this scenario it was assumed that the SCI-experts underestimated the true staff-need for a SCIC by
10%. This is not unlikely since no SCIC exists today in Sweden and it is therefore difficult to foresee
exactly how much staff resources that are needed.
Assuming a 10% increase in staff resources resulted in a 5% increase in total cost for centralised care
to 291 million SEK compared with 278 million SEK in the base case scenario. This resulted in a total
difference in costs between decentralised and centralised care of 1 million SEK. Hence, with a 10%
increase in estimated staff resources in centralised care, no cost-savings in a centralised setting could
be seen compared with a decentralised setting.

23
3.3 Multi-way sensitivity analysis
The results from the multi-way analyses are presented in Table 15. The two analyses describe what
would happen with costs and how centralised and decentralised care would differ in two extreme
scenarios.
Table 15 Multi-way analyses for decentralised vs centralised SCI-patient care. The results are
presented for the whole country in million SEK.
Base case analysis Sensitivity analysis 44 Sensitivity analysis 5
5
Decentralised Centralised Decentralised Centralised Decentralised Centralised
Acute/emergency
care
80.7 84.8 80.7 84.8 80.7 88.8
Centre
-Staff 150.7 128.0 176.6 115.2 126.6 128.0
-Facilities 18.0 15.9 20.8 15.9 16.4 15.9
Subtotal 168.7 143.9 197.4 131.1 142.9 143.9
Care at home 40.1 49.2 40.1 49.2 40.1 60.8
Total 289.5 277.9 318.2 265.1 263.8 293.5
Change with
centralised care
-12 -53 30
4. Assumptions: Number of full-time employees per centre in a decentralised setting was based on number of hospitalisation days and visits per clinic. The SCI-experts had overestimated the true staff-need in a centralised scenario by 10%, hence a 10% decrease in staff resources compared with the base-case analysis was accounted for. The occupancy rate in decentralised care was assumed to be lower (75%) compared with the base case scenario (87%). 5. Assumptions: Number of full time employees per 10,000 hospitalisation days was the same in decentralised care as in centralised care. The occupancy rate in decentralised care was equal to the occupancy rate in centralised care. Centralised care is causing a higher increase in primary care at the patient’s home community then was first expected, resulting in an increase with 20,000 visits compared with previously assumed 9,000. Patients stay even longer at acute care in a centralised scenario than was previously assumed (10% longer compared with previously 5% longer).
3.3.1 Sensitivity analysis 4
In this analysis, compared with the base case analysis, it was assumed that:
Number of full-time employees per centre in a decentralised setting was based on number of
hospitalisation days and visits per clinic (described in Sensitivity analysis 1).
The SCI-experts had overestimated the true staff-need in a centralised scenario by 10%, hence a
10% decrease in staff resources compared with the base-case analysis was accounted for in this
sensitivity analysis.
The occupancy rate in decentralised care was assumed to be lower (75%) compared with the
base case scenario (87%).
Based on the above assumptions, staff resources in decentralised care increased compared with the
base case analysis; this is also described in Sensitivity analysis 1. Together with the 10% lower staff

24
need in centralised care, this resulted in an increase of the cost difference considering staff resources
between centralised and decentralised care from 23 to 61 million SEK compared with the base case
analysis. A lower occupancy rate in decentralised care resulted in higher costs and a total difference
of almost 5 million SEK compared with centralised care. In the base case analysis this difference was
less than 2 million SEK. In summary, this described scenario resulted in cost savings with centralised
care of 53 million SEK compared with decentralised care.
3.3.2 Sensitivity analysis 5
In this analysis, compared with the base case analysis, it was assumed that:
Number of full time employees per 10,000 hospitalisation days was the same in decentralised
care as in centralised care.
The occupancy rate in decentralised care was equal to the occupancy rate in centralised care.
Centralised care was causing a higher increase in primary care at the patient’s home community
then was first expected, resulting in an increase to 20,000 visits compared with previously
assumed 9,000.
Patients stay even longer at acute care in a centralised scenario than was previously assumed
(10% longer compared with previously 5% longer).
Based on the above assumptions, total resources costs (hospital beds and staff) were approximately
the same in decentralised and centralised care (143 vs. 144 million SEK). In the base case analysis the
difference was almost 25 million SEK. An increase in primary care visits in the centralised scenario
resulted in an increase in costs compared with the decentralised setting (a 20 million SEK difference
compared with 9 million SEK in the base case analysis). In addition, since patients in centralised care
were assumed to stay even longer in emergency care the cost difference for acute care, between
centralised and decentralised care, increased with 100% (from 4 million SEK difference to 8). In
summary, this scenario shows that unlike the base case analysis, decentralised care is less costly and
the cost increase in a centralised setting would be approximately 30 million SEK.

25
4. Discussion
The aim of this study was to compare available resources and costs for today’s decentralised care of
SCI-patients with the resource needs and costs for a hypothetical scenario with centralised care. This
was done with use of an economic model combining data from a questionnaire to clinics caring for
SCI-patients today (see appendix A), another questionnaire to SCI-specialists asked to envision a
hypothetical spinal cord injury centre (see appendix B), unit cost data from publicly available sources
and a range of assumptions to fill data gaps. Many such assumptions had to be made because the
responding centres had difficulties in answering our questions. Generally, we assumed that the
responses we actually received were representative to all centres (adjusting for centre size where
applicable). A range of sensitivity analyses were performed to test different assumptions where the
available data was uncertain.
4.1 Staffing costs
Our base case analysis showed that the hypothetical centralised scenario that our experts were
asked to envision would result in lower costs in total, albeit based on several uncertain assumptions.
The decrease in costs was mainly driven by lower staffing levels and the costs of staffing accounted
for approximately half of the total costs. The staffing costs rely on several uncertain assumptions.
Firstly, only one in four of the responding centres were able to provide estimates on their current
staffing which indicates how difficult it is to estimate already available resources. Furthermore, this
implied that we had to make assumptions on the staffing of the other centres without knowing
whether the responses we received were representative of all centres. In the base case analysis we
assumed that the staffing per number of hospitalisation days would be the same across all centres on
average. This implies that, in the base case analysis, the model did not take varying staff levels due
differences in number of visits into account. In the sensitivity analysis, this assumption was changed
to include both number of hospitalisation days and number of outpatient and day care visits at each
centre. This resulted in higher costs for decentralised care and larger cost savings from centralised
care. Secondly, the staffing of centralised care was based on expert assumptions of the staffing needs
of the described SCIC. These are also uncertain because no such centre is available in Sweden today.
In the sensitivity analysis, we showed that the cost savings from centralised care would
approximately be offset by a 10% increase in the staffing of centralised care. Although our estimates
related to staffing are uncertain, it is reasonable to assume that a higher degree of specialisation may
lead to economies of scale and efficiency gains that would result in lower staffing needs.
4.2 Acute care costs
The acute care costs were assumed to increase in the centralised scenario because many patients
may need to move from the initial emergency ward (the closest to the accident) to another acute
care facility where an SCIC is situated. This cost may very well change more or less than with our
assumptions, which was exemplified in the sensitivity analysis. It was pointed out by the SCI-experts
[5-8] that the average estimated unit costs for acute care (299,000 SEK) for SCI-patients was low.
When only considering a specific University Hospital using the same DRG-codes and main diagnoses
in the ICD-10 system the cost was estimated to be ~50% higher [16] than what was seen utilizing all
information captured in the KPP-database. If the true cost of acute care is higher than what has been

26
assumed in our calculations it would imply a larger cost increase in acute care associated with
centralised care and smaller total cost difference between the two scenarios.
4.3 Facility costs
The expert assumptions on the number of beds needed, caused relatively high occupancy rates. This
may not be achievable if there is a large variation in the admission of new patients. However, a large
centre with many beds should be able to handle such variation more easily than a small centre which
speaks in favour of our assumptions. There may also be need for careful planning of non-acute
hospitalisations so that they admitted during times of vacancy. This should also be easier in a
centralised setting where the competence is available within the same facilities. The facility costs
were based on interviews with one centre and their internal charges (or rent) were attributed to a
cost per inpatient bed and assumed to be representative to the whole country. The facilities which
the calculations were based on are partly old and newer facilities would naturally have a higher
rental cost. The estimated facility costs did not account for costs for specific equipment such as
electric, height adjustable beds and ceiling hoists. This may have resulted in underestimations of the
true facility costs but if so to a similar extent to both the decentralised and centralised care scenario.
4.4 Re-admissions and outpatient visits
According to the expert assumptions, the total number of re-admissions and outpatient care visits
would decrease in a centralised care scenario. This was reflected in the model assumptions and had
impact on the centre staffing and facility costs. This may be due to the farther distance to the SCIC
for many patients, implying that they would not be admitted to the SCIC to the same extent that they
are to a local rehabilitation centre. It is also possible that centralisation would increase the quality of
care resulting in a lower need for re-admissions and outpatient visits.
SCI-patients are sometimes sent on so called rehabilitation sun trips to for example Vintersol, a
Swedish neurological rehabilitation centre located in Los Cristianos, Spain [17]. How many SCI-
patients that are sent each year on these trips varies between counties in Sweden. Two of our SCI-
specialists [5, 8] stated that they rarely refer patients on these trips. A representative from
Stockholm county council [18] informed that they in 2012 sent 12 SCI-patients on these trips to a
total cost of 895,000 SEK. If this would be representative for the whole country it would imply costs
in the range of 4 million SEK per year for Sweden. In a centralised scenario more patients may travel
to a SCIC for rehabilitation instead of out of the country, which would imply reductions in these costs
for rehabilitation trips.
4.5 Care at home
The centralised scenario implies that the SCIC takes a larger responsibility for both the re-integration
in the community (after the completion of the primary rehabilitation) and the long-term care for the
patient. The resources needed for this at the SCIC have been included in the estimates provided by
the SCI-experts. However, resources on the local level will also be needed both during re-integration
and long-term follow-up. In the model, it was assumed that the number of visits to some of these
local resources (e.g. general practitioner and physiotherapist) would increase, because patients
would have farther to travel to the closest rehabilitation centre. This increase resulted in higher costs
in the centralised scenario which were also further elaborated in the sensitivity analysis. It has been

27
argued that centralised care may in fact not increase primary care visits if ambulating teams and e-
health from the SCIC would enable managing SCI-patients in their homes. If so, this would result in
even larger cost-savings in a centralised scenario compared with the base-case analysis. On top of
this, local care providers are expected to spend more time and resources on communication with the
SCIC and function as a link between each patient and the SCIC, both during re-integration and long-
term care. The costs of these resources are difficult to estimate but are not expected to be significant
compared to the care that is already provided by the local care provider. In some cases, the support
from the SCIC can even result in lower costs for the local care provider, assuming that more
competence results in more efficient care provision and a reduced care need in the long run.
4.6 Other benefits
As noted in the introduction, centralised care is expected by many to lead to better care for patients
with spinal cord injury. For example, Swedish qualitative studies have shown that today’s care of SCI-
patients has been unclear to some SCI-patients and that the lack of customised rehabilitation
programmes with clear, measurable goals could affect the SCI-patient negatively [19, 20].
Centralisation is expected to induce higher specialisation with more competent staff which may
result in better outcomes for patients. This may very well lead to fewer complications in the long run,
e.g. by optimizing the rehabilitation process increasing the chance of the each patient learning how
to avoid pressure sores. Similarly, better peer-support may increase the self-confidence and
motivation of patients increasing the chance of them getting back into work. Avoiding complications
and improving chances to work would both increase the quality of life of patients and their families,
and reduce costs to society. The indirect societal costs from work absence can be estimated at about
507,000 SEK1 per year, assuming equal value to what the employer would pay for one year salary
including social security contributions [10, 11]. Increasing the ability to work would therefore have
major impact on the total costs from a societal perspective.
4.7 Model limitations
In addition to the uncertainty discussed under the previous headings the model has the following
limitations that are worth mentioning.
The model assumed 270 incident patients while the actual number is unknown. This may of course
change from year to year but is expected to affect the costs of the decentralised and centralised
scenarios in similar ways.
In both scenarios patients were assumed not to transfer between clinics during their primary
rehabilitation although we know they do in today’s decentralised scenario. However, because we
accounted for the total time during primary rehabilitation this should not have any implications for
the results.
Some costs that may change with centralised care were not considered in the model due to lack of
data. These include costs for transportation (both for patients, their families and centre staff during
home visits), and certain one-time costs that may be associated with the change of organisational
1 SEK 29,800*1.48*12, where 29,800=Average monthly salary for all sectors from Statistics Sweden and 1.48=
adjustment to include social security contributions paid by the employer

28
systems. It is likely that the centralisation process would induce higher costs at the start during a
process where the SCICs are established, the right facilities and competence are put in place. There
may also be significant costs for setting up referral processes and contracts and routines between
county councils enabling centralised care.
The model did not consider what would happen with the available resources at the decentralised
centres if patients would move to a SCIC. In many cases, these resources are expected to be used in
the care of others whereas they in some cases would be redundant.
4.8 Conclusions
Our analysis indicates that a centralised organisation of the care for patients with spinal cord injuries
would be cost saving compared to the decentralised organisation of today. However, these results
are highly sensitive to assumptions on care and resource needs as outlined in this report, and altering
the assumptions may result in centralised care being more costly. According to our interpretation,
our results imply that the expected benefits of centralisation in terms of improved quality of care
would at worst come at a modest increase in costs with a higher potential for cost savings overall.

29
5. References
1. Apparelyzed, Spinal Cord Injury Peer Support. Available from: http://www.apparelyzed.com/. 2. Whooley, C., et al., ESCIF report on Centralisation of the treatment, rehabilitation and life-
long care of persons with spinal cord injury May 2010: www.escif.org. 3. The Swedish Association for Survivors of Accident and Injury (RTP). Available from:
http://www.rtp.se/. 4. ESCIF, policy statement. Available from: http://www.escif.org/ESCIF,,policy_statement.htm. 5. Ertzgaard, P., Linköpings Univeristetssjukhus. 6. Hultling, C., Rehab Station Stockholm 7. Levi, R., Umeå Universitetssjukhus. 8. Ro, H., Skåne Universitetssjukhus. 9. Åhrén, G., Personskadeförbundet, RTP. 10. Statistics Sweden. Available from: http://www.scb.se/sv_/Hitta-
statistik/Statistikdatabasen/Variabelvaljare/?px_tableid=ssd_extern%3aLonYrkeRegion4&rxid=bf4f2657-05ee-47e7-a8b7-47e76e4ceba4.
11. Arbetsgivarverket. Available from: http://www.bth.se/for/ekonomi.nsf/bilagor/avgifter-och-skatter-2014_pdf/$file/avgifter-och-skatter-2014.pdf.
12. Karlberg, M., Skåne Universitetssjukhus. 13. Swedish Association of Local Authorities and Regions (SKL). Available from:
http://www.skl.se/vi_arbetar_med/statistik/kostnad-per-patient/databas. 14. Prislista utomlänspatienter i Primärvården Uppsala län 2013. Available from:
http://svnuppsalaorebro.se/document/prislistor/2013/Uppsala2013.pdf. 15. Södra regionvårdsnämnden, primärvård/allmänmedicin. Available from:
http://www.skane.se/Upload/Webbplatser/Sodra%20regionvardsnamnden/prislista/2012/77_primarvard_ovr_spec2012.pdf.
16. Persson, H., Universitetssjukhuset i Linköping. 17. Vintersol. Available from: http://www.vintersol.com/?page_id=32. 18. Jonsson, K., Stockholm County Council. 19. Nordgren, C., et al., Societal services after traumatic spinal cord injury in Sweden. J Rehabil
Med, 2003. 35(3): p. 121-6. 20. Sand, A., I. Karlberg, and M. Kreuter, Spinal cord injured persons' conceptions of hospital care,
rehabilitation, and a new life situation. Scand J Occup Ther, 2006. 13(3): p. 183-92.

30
6. Appendix A: Questionnaire to clinics
GENERELL INFORMATION OM AVDELNINGEN
Tel: E-post:
PATIENTER PÅ AVDELNINGEN
1 Vilka patientgrupper vårdas på avdelningen? Ja Nej
Ryggmärgsskada (ej medfödda skador)
Icke-trauma
Trauma
Medfödd ryggmärgsskada
Hjärnskador (t.ex. stroke)
Multipel Skleros
Andra neurologiska skador och sjukdomar (t.ex.
patienter med ryggmärgsbråck)
Andra skador och sjukdomar
Avdelning:
Klinik:
Sjukhus:
Kontaktperson för enkäten:
Kommentarer:

31

32
2 Primärrehabilitering år 2012 Samtliga patienter
inlagda på avdelningen
Patienter med
traumatiska
ryggmärgsskador
Patienter med
icke-traumatiska
ryggmärgsskador
Hur många patienter fick
primärrehabilitering i slutenvård
år 2012?
I genomsnitt, hur många dagar
vårdades varje patient?
3 Återinskrivningar år 2012
Samtliga patienter
återinskrivna på
avdelningen
Patienter med
traumatiska
ryggmärgsskador
Patienter med
icke-traumatiska
ryggmärgsskador
Hur många patienter återinskrevs
i slutenvård år 2012?
I genomsnitt, hur många dagar
vårdades varje patient?
Kommentarer:
Kommentarer:

33
4 Öppen- och dagvård år 2012
Samtliga patienter som
nyttjade denna typ av
vård på avdelningen
Patienter med
traumatiska
ryggmärgsskador
Patienter med
icke-traumatiska
ryggmärgsskador
Hur många öppenvårdsbesök
gjordes vid avdelningen år 2012?
Hur många dagvårdsbesök
gjordes vid avdelningen år 2012?
PERSONAL PÅ AVDELNINGEN
Kommentarer:
5 Vilka yrkesgrupper bedriver
vård på avdelningen? Antal heltidstjänster totalt
vid avdelningen
(t.ex. 2 eller 0,5)
Andel av deras arbetstid som
avser vård av
ryggmärgsskadade patienter
(ej medfödda skador)
(t.ex. 50% eller 75%)
Arbetsterapeut
Dietist
Kurator
Läkare
Logoped
Psykolog
Rehabassistent
Sjukgymnast
Sjuksköterska
Undersköterska
Uroterapeut

34
Annan (vänligen ange)

35
6
Vilka yrkesgrupper arbetar på
administrativ nivå på
avdelningen?
Antal heltidstjänster totalt
vid avdelningen
(t.ex. 2 eller 0,5)
Andel av deras arbetstid som
avser ryggmärgsskadade
patienter (ej medfödda
skador)
(t.ex. 50% eller 75%)
Administrativ chef
Administrativ assistent
Annan (vänligen ange)
Kommentarer:
Kommentarer:
36
ÖVRIGA RESURSER PÅ AVDELNINGEN
7 Hur många vårdplatser finns på avdelningen
och hur är de fördelade?
Antal
Totalt
Antal i
enkelrum
Antal i
dubbelrum
Antal i
större
rum
Vårdplatser totalt
Vårdplatser avsedda för ryggmärgsskadade (ej
medfödda skador)
8 Är rummen på avdelningen utrustade med
följande utrustning?
Ja
alla rum
Ja
några rum
Hur många
vårdplatser? Nej
Elektriska, höj-och sänkbara sängar
Fullt anpassad toalett och badrum
Taklyftar / hissar
Kommentarer:
Kommentarer:

37
9 Finns det följande resurser och tjänster på eller i anslutning
till avdelningen? Ja Nej
Bibliotek
Butik
Dagrum
Ergonomiska träningsmöjligheter
Gym
Helikopterplatta
Internetmöjligheter
Isoleringsrum
Köksmöjligheter (t.ex. handikappanpassat kök)
Matplats
Möjligheter till arbetsrehabilitering
Mötesrum
Pool
Restaurang
Rum med övernattningsmöjligheter för anhöriga
Specialiserad förarutbildning (för handikappanpassade fordon)
Tandvårdsmöjligheter
Träningslägenheter
Tvåbäddsrum för patienter och vårdgivare / personlig assistent
Utomhusträningsmöjligheter
Stort tack för din medverkan!
Kommentarer:

38
7. Appendix B: Questionnaire to SCI-specialists
Vänligen föreställ dig ett specialiserat ryggmärgsskadecentre som har resurser att klara följande
Primärrehabilitering
Patienter remitteras till centret när de är resporatoriskt och cirkulatoriskt stabila samt alla kirurgiska
ställningstaganden är gjorda. Sammantaget fyra centre i Sverige ska ansvara för
primärrehabiliteringen av samtliga personer som drabbas av traumatiska (~120 per år) och akut icke-
traumatiska (~150 per år) ryggmärgsskador. Detta innebär ca. 30 traumatiska och knappt 40 akuta
icke-traumatiska ryggmärgsskador per centre och år. Genomsnittlig vårdtid i Skåne var 58 dagar år
2012.
Återintegrering i samhället
I slutet av primärrehabiliteringsfasen ansvarar varje centre också för sina patienters återintegrering i
samhället. Detta innefattar följande:
i. kontakt med samhällsfunktioner och arbetsplats på hemorten
ii. konstant tillgång till jourtelefon för vårdpersonal på hemorten
iii. videokonferenser mellan centre och vårdpersonal/patient på hemorten
iv. ambulerande team vid centret som kan göra hembesök (vanligen två personer, t.ex.
arbetsterapeut och sjukgymnast/kurator)
Återinläggningar
Varje centre ska ansvara för återinläggningar av personer som avslutat sin primärrehabilitering vid
centret (ca. 30%). Genomsnittlig vårdtid i Skåne 2012 var 22 dagar år 2012.
Långtidsuppföljning
Varje centre ska ansvara för den långsiktiga uppföljningen av sina patienter. Detta innefattar
följande:
i. konstant tillgång till jourtelefon för vårdpersonal på hemorten
ii. videokonferenser mellan centre och vårdpersonal/patient på hemorten (ca. 1 gång per år)
iii. ambulerande team vid centret som kan göra hembesök (ca. 1 gång vartannat år)
iv. uppföljning på ryggmärgsskadeenheten med inkluderad reha (ca. 1 gång vartredje år i ca 3-4
veckor med boende på patienthotell)
v. specialiserad öppen- och dagvård av personer med ryggmärgsskador efter behov

39
Vänligen, föreställ dig ett sådant centre och besvara följande frågor
1
Antag att centret skulle ta hand
om ca. 70 personer med nya
ryggmärgsskador per år, deras
primärrehabilitering,
återintegrering i samhället samt
långtidsuppföljning.
Antal Kommentarer
Hur många återinläggningar per år
skulle detta centre ha kapacitet för?
Hur många öppenvårdsbesök per år
skulle detta centre ha kapacitet för?
Hur många dagvårdsbesök per år
skulle detta centre ha kapacitet för?
Hur många hembesök per år skulle
detta centre ha kapacitet för?
Hur många slutenvårdplatser skulle
centret ha?
Kommentarer:______________________________________________________________________
__________________________________________________________________________________
__________________________________________________________________________________

40
2
Hur många heltidsanställda per
yrkeskategori behövs för varje
typ av vård vid centret?
Primär-
rehabilitering
Åter-
integrering i
samhället
Åter-
inläggningar
Långtids-
uppföljning Kommentarer
Arbetsterapeut
Dietist
Kurator
Läkare
Logoped
Psykolog
Rehabassistent
Sjukgymnast
Sjuksköterska
Undersköterska
Uroterapeut
Annan (vänligen ange)

Confidential
0
3 Hur många heltidsanställda per yrkeskategori behövs för
administration vid centret?
Administrativ chef
Administrativ assistant
Annan (vänligen ange)
Kommentarer:______________________________________________________________________
__________________________________________________________________________________
__________________________________________________________________________________