Cost saving strategies_updated
42
Cost Savings Strategies Steven Moskowitz MD, Senior Medical Director, Paradigm Outcomes Jeremy Corbe>, Chief Medical Officer, Kentucky Spirit Health Plan/Centene CorporaFon April 2 – 4, 2013 Omni Orlando Resort at ChampionsGate
-
Upload
opunite -
Category
Health & Medicine
-
view
823 -
download
1
description
Third-Party Payer Track, National Rx Drug Abuse Summit, April 2-4, 2013. Presentation by Dr. Steven Moskowitz and Dr. Jeremy Corbett.
Transcript of Cost saving strategies_updated

Cost Savings Strategies
Steven Moskowitz MD, Senior Medical Director, Paradigm Outcomes
Jeremy Corbe>, Chief Medical Officer, Kentucky Spirit Health Plan/Centene CorporaFon
April 2 – 4, 2013 Omni Orlando Resort
at ChampionsGate

Learning Objec3ves
• Learn the latest data about the cost of prescripFon drug abuse to insurance companies
• Outline alternaFves to treaFng paFents in workers’ compensaFon claims
• Prepare strategies that you can implement in your state

Disclosure Statement
• Steven Moskowitz has no financial relaFonships with proprietary enFFes that produce health care goods and services.
• Jeremy Corbe> has no financial relaFonships with proprietary enFFes that produce health care goods and services.

Introduc3on
• Opioid use for non cancer pain commonplace, without evidence of effecFveness
• Cost of opioids and medicaFons to treat complicaFons have sky-‐rocketed
• Overdose and death rates conFnue to rise • The range of soluFons includes state-‐wide intervenFon and direct case management

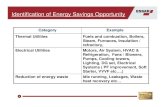
$100 billion esFmated annual cost in the US of health care, lost income and lost producFvity due to chronic pain according to the NIH1
76 million Americans suffer from chronic pain according to the NIH1
40% of physician office visits due to pain2
The Cost of Chronic Pain
5
1. NIH Guide: New direcFons in Pain Research (NaFonal InsFtutes of Health, September 4, 1998); 2. Koch, H. “The management of chronic pain in office-‐based ambulatory care: NaFonal Ambulatory Medical Care Survey (Advance Data from Vital and Health StaFsFcs, No. 123, DHHS PublicaFon No. PHS 86-‐1250)

■ Hydrocodone: “The most popular medicine in the U.S. …even as a panel of experts called together by the Food and Drug AdministraFon recommended that regulators ban it.”1
■ Total US societal costs of prescripFon opioid abuse were esFmated at $55.7 billion in 2007 (USD in 2009)2
The Cost of Opioids
1. FORBES.com America's Most Popular Drugs, Ma>hew Herper, 5/11/10
2. Economic costs of nonmedical use of prescripFon opioids, Clin J Pain. 2011 Mar-‐Apr;27(3):194-‐202

■ Admission rates for abuse of opiates other than heroin—including prescripFon painkillers—rose by 450% from 1998-‐20081
■ 120,000 Americans a year go to the ER aoer overdosing on opioid painkillers2
■ CDC 14,800 prescripFon opioid deaths in US in 20082
– 475,000 ER visits for abuse of prescripFon pain killer
– 12 million of non-‐medical users of prescripFon pain killers
The Cost of Chronic Opioids
1. Substance Abuse and Mental Health Services AdministraFon, Office of Applied Studies. Treatment Episode Data Set (TEDS): 1998-‐2008. NaFonal Admissions to Substance Abuse Treatment Services, DASIS Series: SÐ50, DHHS PublicaFon No. (SMA) 409-‐4471, Rockville, MD, April 2010. 2. Policy Impact: PrescripFon Painkiller Overdoses, Centers for Disease Control and PrevenFon, NaFonal Center for Injury PrevenFon and Control, Division of UnintenFonal Injury PrevenFon

Case Management Strategies in Workers’ Compensa3on
April 2 – 4, 2013 Omni Orlando Resort
at ChampionsGate

Worker’s CompensaFon Idiosyncrasies
• LifeFme medical cost coverage • Coverage limited to work-‐related condiFons
• Indemnity issues
• HIPPA exempFon
• State regulaFons differ • Different uFlizaFon review controls • LiFgious

Opioids in Worker’s CompensaFon
• Costly cases are a small percent of all claims – 6% of cases account for 50% of costs1
• According to NCCI, 20% of WC medical costs of fully developed claims are spent on prescripFon drugs; narcoFcs account for 34% of this spend
• Have contributed to medical cost inversion – Medical costs now 58% (indemnity 42%) 2
• Fee schedules affect uFlizaFon • LiFgious issues make UR more complex
1. Lipton, et.al. “Medical Services by Size of Claim”, NCCI, 2009 2. Workers’ CompensaFon Insurance RaFng Bureau of California, 2008 California Workers’
CompensaFon Losses and Expenses

Framing the Problem
• Pharmacy cost is a major claims issue • Prescribing is the management issue
• Physician-‐paFent behavior drive prescripFon • Why do physicians prescribe opioids?
– Observable behaviors of the paFent were the only significant and meaningful predictor of physicians' opioid prescribing pracFces1
1. What Factors Affect Physicians’ Decisions to Prescribe Opioids for Chronic Noncancer Pain PaFents? Clinical Journal of Pain, December 1997, Vol 13, 4 p 330-‐336

MaladapFve Cycle
Illness conviction Catastrophizing Fear avoidance
Quick fix seeking
Maladaptive Treatment
Lack of objective measures Quick fixes
Trial and error approach
Poly-pharmacy Escalating
interventions
Maladaptive Coping

Breaking the Cycle
• Physician-‐specific intervenFons – Monitor outcome – Avoid adverse effects – Prescribe less – Use alternaFve tools
• Injured worker-‐specific intervenFons – Become less passive – Make more effecFve medical decisions – Less medicaFon seeking

Case Management Tools
Federal • FDA Risk EvaluaFon and MiFgaFon Strategy
State
• State law and legal acFon • State work comp regulaFons/formulary
• State pharmacy PMP-‐40+ states
• State medical boards: CME/license renewal
• State work comp UR guidelines/EBM/Peer review
– Risk assessment, UDS, reassessment, outcomes
– Opioids not effecFve
Local • Local providers of excellence • Independent medical evaluaFons
• Onsite case management
Carrier • PBM reports, alerts, formulary
• Meds not approved for certain use • Alerts and follow up

Be Strategic
• Pain is a biopsychosocial problem • Manage opioid use in context of larger pain management plan
• Why is the opioid a problem in this IW? – Expensive – IneffecFve – Adverse effects – Use disorder: dependence, withdrawal, addicFon, misuse

Be Strategic
• Validate treaFng diagnosis –frequent inaccurate/incomplete diagnosis (CRPS)
• Coordinate care that is evidence based • Track the outcome or lack of outcome
• Define, acknowledge and manage behavior

Injured Worker IntervenFons
• Engage and moFvate: stages of change • MedicaFon list review
• Review side effects of medicaFons
• IdenFfy realisFc real life outcome measures
• Offer alternaFves

Case Example
• 36 year old obese male, two failed back surgeries, failed SCS trial, repeat injecFons, iniFal MEDD of 180, total “couch potato”
• Moved from NJ to NC for his wife’s job. Refilled medicaFons in NJ as well as in NC
• Referred him to new conservaFve MD in NC • Case manager worked with IW as did MD, stages of change, slow wean, worker agreeable
• 1 year later 20 MG MEDD, stay at home dad

MD: Specific IntervenFons
• Engage MD: what is biggest reason MD prescribes opioids?
• Define behavioral obstacles to recovery • Med list review for effecFveness, weeding • Define effecFveness measures and outcomes • IdenFfy adverse effects, safety issues and misuse • Implement contract and UDS screen • Follow-‐up of UDS results and consequences • Offer alternaFves

Case Example
• 45-‐year-‐old male with low back from 1992 injury • Status post mulFple failed back surgeries, spinal cord sFmulator
and intrathecal drug pumps and mulFple infecFons and revision. Oral opioids and pump opioids with total MEDD of 19,000. Current infecFon of old sFmulator site with resecFon of clavicle
• IntervenFon: Engaged IW: onsite case management, family engagement; Engaged MD to “stand down”; inpaFent rehab and detoxificaFon facility
• Outcome: Pump out, SCS off, off all opioids, fully funcFonal, new MD, no more procedures

Pain Outcomes
Decrease in Morphine Equivalents
Release to Return to Work
Decrease in Morphine Equivalents
61%
Release to Return to Work
Early Interven3on Pain (referral less than one year
from date of injury)
Chronic Pain (referral average six years
from date of injury)
Pain Management Costs
32%
78%
77% 41% LOWER

Can a Popula3on be Managed? Managed Care OrganizaFons and PrescripFon Drug
Abuse
April 2 – 4, 2013
Omni Orlando Resort at ChampionsGate

Centene
Managed Care 101




Start Smart for Your Baby
Health Steps IniFaFve







TOTALS OVERLAP Members idenFfied as pregnant 3,149 Members in B3 and B4 22
Pregnant members who filled teratogens in the last 30 days. 51 1.6% B3 and B7 39
Pregnant members who filled any amount of narcoFcs in the last 90 days. 292 9.3% B3 and B8 3
Pregnant members who filled more than 90 tablets of narcoFcs and/or filled narcoFcs more than three Fmes in the last 90 days (heavy users). 82 2.6% B4 and B7 206
Pregnant members who filled narcoFcs in the last 90 days but did not qualify as heavy users (see above). 210 6.7% B4 and B8 4
Pregnant members who have not filled any prenatales in the last 90 days. 2,441 77.5% B7 and B8 10
Pregnant members who filled more than 4 disFnct drugs in the last 14 days (Poly pharmacy) 17 0.5% B3, B4 and B7 14
Pregnant members who filled Methadone or Suboxone in the last 90 days. 61 1.9% B3, B4 and B8 1
Pregnant members who have ever filled HIV medicaFons. 0 0.0% B3, B7 and B8 2
B4, B7 and B8 2 B3, B4, B7 and B8 1 Members in at least one of B3, B4, B7, B8 or B10. 2,535



Kentucky Spirit Health Plan
Controlled Substance Pilot





“The best way to do something ‘lean’ is to gather a Gght group of people, give them very liIle money, and very liIle Gme.” -‐ Bob Klein