Cost Effectiveness of Guanfacine Extended-Release versus Atomoxetine for the Treatment of...
15
Cost Effectiveness of Guanfacine Extended-Release versus Atomoxetine for the Treatment of Attention-Deficit/Hyperactivity Disorder Application of a Matching-Adjusted Indirect Comparison M. Haim Erder, 1 Jipan Xie, 2 James E. Signorovitch, 2 Kristina S. Chen, 2 Paul Hodgkins, 1 Mei Lu, 2 Eric Q. Wu 2 and Vanja Sikirica 1 1 Shire Development LLC, Wayne, PA, USA 2 Analysis Group, Inc., Boston, MA, USA Abstract Background: About 7% of children and adolescents are diagnosed with at- tention-deficit/hyperactivity disorder (ADHD) in the US. Patients with ADHD who are intolerant of or do not have an optimal response to stimu- lants often use non-stimulants as alternative therapies. Guanfacine extended- release (GXR) and atomoxetine (ATX) are the only non-stimulants approved by the US Food and Drug Administration for once-daily use in the treatment of children and adolescents with ADHD in the US. ATX has been on the market since 2002 while GXR was recently approved in 2009. To date, there is no comparative effectiveness or cost-effectiveness study comparing the two drugs. Objectives: The aim of this study was to assess the cost effectiveness of GXR versus ATX for the treatment of ADHD in children and adolescents, using the comparative efficacy results from a matching-adjusted indirect compar- ison (MAIC). Methods: The MAIC method was used to compare the efficacy between GXR (target dose and lower doses) and ATX (target dose) in the absence of head- to-head clinical trials. Individual patients in the GXR trials were weighted such that the summary baseline characteristics and the efficacy of the placebo arm of the GXR trials matched exactly with those from published ATX trials. After weighting, the efficacy (i.e. change in the ADHD rating scale, fourth edition [ADHD-RS-IV] total score from baseline) was compared between each GXR dosing group and the ATX group. The results from the MAIC analyses were used to populate a 1-year Markov model that is used to com- pare the cost effectiveness of GXR versus ATX from a US third-party payer perspective. Effectiveness outcomes for each treatment group were estimated as the proportion of responders, defined as patients with ‡25% reduction in ADHD-RS-IV total score from baseline, and average quality-adjusted life ORIGINAL RESEARCH ARTICLE Appl Health Econ Health Policy 2012; 10 (6): 381-395 1175-5652/12/0006-0381/$49.95/0 Adis ª 2012 Springer International Publishing AG. All rights reserved.
Transcript of Cost Effectiveness of Guanfacine Extended-Release versus Atomoxetine for the Treatment of...

Cost Effectiveness of GuanfacineExtended-Release versusAtomoxetine for the Treatment ofAttention-Deficit/Hyperactivity DisorderApplication of a Matching-Adjusted Indirect Comparison
M. Haim Erder,1 Jipan Xie,2 James E. Signorovitch,2 Kristina S. Chen,2 Paul Hodgkins,1
Mei Lu,2 Eric Q. Wu2 and Vanja Sikirica1
1 Shire Development LLC, Wayne, PA, USA
2 Analysis Group, Inc., Boston, MA, USA
Abstract Background: About 7% of children and adolescents are diagnosed with at-
tention-deficit/hyperactivity disorder (ADHD) in the US. Patients with
ADHD who are intolerant of or do not have an optimal response to stimu-
lants often use non-stimulants as alternative therapies. Guanfacine extended-
release (GXR) and atomoxetine (ATX) are the only non-stimulants approved
by the US Food and Drug Administration for once-daily use in the treatment
of children and adolescents withADHD in theUS. ATXhas been on themarket
since 2002 while GXR was recently approved in 2009. To date, there is no
comparative effectiveness or cost-effectiveness study comparing the two drugs.
Objectives: The aim of this study was to assess the cost effectiveness of GXR
versus ATX for the treatment of ADHD in children and adolescents, using
the comparative efficacy results from a matching-adjusted indirect compar-
ison (MAIC).
Methods: TheMAICmethod was used to compare the efficacy between GXR
(target dose and lower doses) and ATX (target dose) in the absence of head-
to-head clinical trials. Individual patients in the GXR trials were weighted
such that the summary baseline characteristics and the efficacy of the placebo
arm of the GXR trials matched exactly with those from published ATX trials.
After weighting, the efficacy (i.e. change in the ADHD rating scale, fourth
edition [ADHD-RS-IV] total score from baseline) was compared between
each GXR dosing group and the ATX group. The results from the MAIC
analyses were used to populate a 1-year Markov model that is used to com-
pare the cost effectiveness of GXR versus ATX from a US third-party payer
perspective. Effectiveness outcomes for each treatment group were estimated
as the proportion of responders, defined as patients with ‡25% reduction in
ADHD-RS-IV total score from baseline, and average quality-adjusted life
ORIGINAL RESEARCH ARTICLEAppl Health Econ Health Policy 2012; 10 (6): 381-395
1175-5652/12/0006-0381/$49.95/0
Adis ª 2012 Springer International Publishing AG. All rights reserved.

years (QALYs). Utilities associated with response/non-response and dis-
utilities due to adverse events were applied in the model. Costs included drug
and medical service costs and were inflated to 2011 US dollars ($US). In-
cremental cost/QALY and incremental cost/responder were estimated. Uni-
variate sensitivity analyses were conducted by varying all model parameters,
including costs, utilities, and response rate.
Results: The target dose of GXR was 0.12mg/kg/day. In match-adjusted
populations with balanced baseline characteristics, patients receiving GXR at
the dose of 0.09–0.12 (p= 0.0009) and 0.075–0.09mg/kg/day (p = 0.0248) hadbetter efficacy, while those receiving GXR at the dose of 0.046–0.075mg/kg/dayhad comparable efficacy (p= 0.0699), compared with patients receiving ATX at
the target dose of 1.2mg/kg/day. In the base case of the cost-effectiveness analysis(CEA), GXR had incremental cost-effectiveness ratios of $US10637/QALY and
$US853/responder, compared with ATX (incremental costs: $US74; incremental
effectiveness: 0.007 QALYs and 86 responders per 1000 patients treated). Results
of all univariate sensitivity analyses showed that the model results were robust to
changes in model inputs.
Conclusions: To our knowledge, this is the first application of the novel com-
parative efficacy method of MAIC to a CEAmodel. TheMAIC results indicate
thatGXR (0.075–0.12mg/kg/day) wasmore effective thanATX (1.2mg/kg/day)in the trial population. The CEA results indicate that GXR is cost effective
compared with ATX for the treatment of ADHD in children and adolescents.
Key points for decision makers
� Using a novel comparative effectiveness method, matching-adjusted indirect comparison(MAIC), the study showed guanfacine extended-release (GXR) 0.09–0.12mg/kg/day and0.075–0.090mg/kg/day were associated with better efficacy compared with atomoxetine(ATX) 1.2mg/kg in the trial population
� Using the efficacy inputs obtained from the MAIC, the study estimated incremental cost-effectiveness ratios at $US10637 per QALY and $US853 per responder comparing GXR withATX for the treatment of children and adolescents with attention-deficit/hyperactivity disorderin the base case, indicating that GXR is cost effective compared with ATX
Introduction
Attention-deficit/hyperactivity disorder (ADHD)is a common psychiatric disorder in children, af-fecting up to 7.2% of the population aged 4–17years in the US in 2007.[1] It presents a substantialeconomic burden with estimated incrementalcosts of $US143–$US266 billion (year 2010 val-ues).[2] ADHD treatment options approved by theUS Food and Drug Administration (FDA) in-
clude stimulants and non-stimulants. Stimulantsare the recommended first-line treatments forADHD; however, one study showed that approxi-mately 30% of children age 6–12 years with ADHDdid not have adequate response to the stimulantmethylphenidate,[3] and may need alternative treat-ments to control their symptoms. Non-stimulantsare not controlled substances and pose less risk ofdrug abuse or dependence.[4] Atomoxetine (ATX)and guanfacine extended-release (GXR) are the
382 Erder et al.
Adis ª 2012 Springer International Publishing AG. All rights reserved. Appl Health Econ Health Policy 2012; 10 (6)

only two FDA-approved once-daily non-stimulantsfor the treatment of children and adolescents withADHD.[5,6] Clinical trials have shown that bothdrugs had superior efficacy compared with pla-cebo;[7-10] however, to date, there is no head-to-head clinical trial comparing their relativeefficacy, nor is there any study evaluating the costeffectiveness of GXR compared with ATX.[11]
Comparative effectiveness research (CER) canhelp clinicians and policy makers make inform-ed decisions about alternative treatments. TheAmericanRecovery andReinvestmentAct (ARRA)passed in 2009 allocated $US1.1 billion to fundCER. Because direct comparisons between treat-ments in head-to-head trials are often unavail-able, indirect comparisons are the only remainingoption to obtain CER data in a timely fashion forpayers, physicians and patients to evaluate thevalue of a new treatment compared with alterna-tives. This study applies the comparative efficacydata of GXR and ATX from a newly developedmethod called matching-adjusted indirect com-parison (MAIC)[12] to evaluate the cost effective-ness of GXR versus ATX for the treatment ofADHD in children and adolescents from a USthird-party payer’s perspective.
Methods
Comparative Efficacy of GuanfacineExtended-Release (GXR) versus Atomoxetine(ATX) Using Matching-Adjusted IndirectComparison
The MAIC method has been used in severalpublished studies to estimate comparative effi-cacy of treatments for which head-to-head trialswere not available,[12-16] including in a recent studythat examined GXR versus ATX in children withADHD and comorbid oppositional defiant dis-order.[15] The MAIC method was applied in thisstudy to compare GXR versus ATX in childrenand adolescents with ADHD.A systematic reviewof double-blind, randomized, placebo-controlledtrials including GXR or ATX was conducted. Itidentified two GXR trials and one ATX trial thatmet the following selection criteria: (i) all patientswithin the age range of 6–18 years old (inclusive);(ii) trials not focusing on a subgroup of ADHD
patients, (e.g. patients with certain comorbiditiesor those who meet a specific severity threshold);(iii) GXR or ATX used as monotherapy; (iv) pres-ence of a common efficacy outcome with baselinescore reported, (in this case, ADHD rating scale,fourth edition [ADHD-RS-IV] total score); and(v) inclusion of the target weight-based dose(0.12mg/kg/day for GXR and 1.2mg/kg/day forATX) in a treatment group. These target doseswere selected based on the dosing levels, beyondwhich the package inserts state there is no addi-tional benefit demonstrated.[5,6] Detailed informa-tion on trial selection is included in Appendix 1 inthe Supplemental Digital Content, http://links.adisonline.com/APZ/A65. Summary results forpatients randomized to ATX 1.2mg/kg/day andplacebo arms were obtained from the publishedATX trial.[7] Individual patient data (IPD) wereavailable for GXR patients.[9,10] GXR patientswho met the inclusion/exclusion criteria used inthe ATX trial were included in the analysis. Inparticular, they were required to have an ADHD-RS-IV score ‡1.5 standard deviations above theage and gender norms at baseline.
GXR Patient Selection by Expected Dosing
Patients were selected based on their expectedweight-based dosing using the IPD from the twoGXR trials.[9,10] For patients randomized to theGXR arms, the expected weight-based dosing wascalculated as weight-based GXR dose= random-ized GXR dose (1, 2, 3 or 4mg/day)/body weight.Based on the expected weight-based dosing, pa-tients were classified into the following categories:0.09–0.12mg/kg/day, 0.075–0.09mg/kg/day and0.046–0.075mg/kg/day. Dosing ranges were usedto evaluate the efficacy of GXR because focusingon a particular dose (e.g. the target dose of0.12mg/kg/day) would have resulted in a smallsample size. Because some patients would neverachieve certain weight-based dose, even with thehighest fixed dose (4mg/kg), each placebo patientwas weighted according to his/her probability offalling into a weight-based dose category, assum-ing that the placebo patient had equal probabil-ity to be randomized into 1, 2, 3 or 4mg/day ofGXR. This would provide a comparable placebogroup for each weight-based GXR dose category.
Cost Effectiveness of GXR vs ATX 383
Adis ª 2012 Springer International Publishing AG. All rights reserved. Appl Health Econ Health Policy 2012; 10 (6)

Matching-Adjusted Indirect Comparison toEstimate the Comparative Efficacy
Baseline characteristics were matched if theywere reported in the ATX trial and were alsoavailable in the GXR trials. Trial populationswere matched by assigning weights to individualpatients in the GXR trials such that (i) theirweighted mean (and standard deviations for con-tinuous variables) baseline characteristics (age,gender, baseline ADHD-RS-IV, inattentive and hy-peractivity/impulsivity subscale scores, and ADHDsubtypes) and mean placebo group efficacy (changein ADHD-RS-IV total score from baseline) match-ed those reported for the ATX trial; (ii) weightswere a linear function of the baseline character-istics; and (iii) weights were required to be as‘close’ as possible to equal weighting across all pa-tients. This last condition was imposed by mini-mizing the Euclidian distance between the newweights and equal weighting. It also had the effectof preserving the largest effective sample size forthe re-weighted GXR data (i.e. it minimized thesum of the squared weights). This would avoidextreme outlying weights that would allow undueinfluence by a small number of data points. Theweights depended only on baseline characteristicsand not on the treatment to which patients wereassigned.
The purpose of the re-weighting was to bal-ance baseline characteristics and placebo effectbetween trial populations. Mean changes in theADHD-RS-IV total score from baseline to end-point were then compared between the balancedtrial populations. Statistical significance was as-sessed using the bootstrap method with 1000 itera-tions.[17] The comparisons were conducted betweeneach GXR dosing group and the ATX group.
Response Rate Estimation
Because the ATX trial included in the MAICdid not report response rate as an endpoint (anecessary model input for the cost-effectivenessanalysis [CEA]), a prediction model was devel-oped based on other published ATX trials in orderto translate the change in ADHD-RS-IV totalscore into response rate. This model was devel-oped using data from all treatment groups in theATX trials[8,18-22] that reported baseline ADHD-
RS-IV total score, change in ADHD-RS-IV totalscore and rate of treatment response defined as‡25% reduction in ADHD-RS-IV total score frombaseline to endpoint. Using data from these trials, ameta-regression analysis established the followingmodel to estimate treatment response rate based onchange in ADHD-RS-IV total score: predicted re-sponse rate= 0.52659 - 0.00979*(baseline ADHD-RS-IV total score) - 0.03206*(change in ADHD-RS-IV total score).
The model was further tested using IPD fromthe pooled GXR trials. The observed and pre-dicted response rates were compared for differentGXR dosing categories; the prediction errorswere generally small, ranging from 1.5% to 2.3%.The prediction model was then applied to esti-mate treatment response rate for the three GXRdosing groups and the ATX group based on theestimated mean change in ADHD-RS-IV totalscore from the MAIC.
Cost-Effectiveness Analysis
A Markov model was developed to assess thecost effectiveness of GXR compared with ATXfrom aUS third-party payer’s perspective (figure 1).Themodelled time horizon was 1 year, which con-sisted of a 4-week drug titration period[9,23] and a48-week maintenance period. The model includedthe following health states: response (to ADHDtreatment), no response, and treatment discontin-uation. The cycle length was 1 week for the entiremodel period. The time horizon and health statesused in the current study were consistent with priorpublished cost-effectiveness studies in ADHD.[11,24]
The target population in the model had the samecharacteristics as the trial population included inthe MAIC study. Only direct costs (drug costs anddirect medical costs) borne by a third-party payerwere considered in the model.
Model Assumptions
� At the end of the 4-week titration period, GXRpatients received the maximum weight-baseddosing allowed by their body weight and ATXpatients received 1.2mg/kg/day.
� At the end of each cycle during the 4-week titra-tion period in the model, patients transitionedfrom non-response to response at a constant rate.
384 Erder et al.
Adis ª 2012 Springer International Publishing AG. All rights reserved. Appl Health Econ Health Policy 2012; 10 (6)

� At the end of the 4-week titration period, non-responders discontinued the treatment; re-sponders remained in the response state andreceived treatment until the end of the modelperiod or when they discontinued treatment.
� To account for treatment persistence, themodel assumed that all patients on treatmentdiscontinued at a constant treatment-specificrate, which was applied for all patients duringthe first 4 weeks and for responders during therest of the model period.
� All non-responders incurred incremental med-ical costs associated with non-response (i.e. thecost difference between non-responders andresponders).
� Patients who discontinued treatment had thesame utility andmedical costs as non-responders.
� Adverse events (AEs) reduced the patients’health utilities during the titration period.
Model Parameter Inputs
Transition Probabilities
Transition probability from non-response toresponse in each cycle during the titration periodwas estimated using the predicted response ratesfor GXR and ATX (table I). The estimation as-sumed that response rates were achieved at the
end of the titration period (4 weeks) and that thetransition occurred at a constant rate. The con-stant discontinuation rate was estimated for eachtreatment based on the 2-year rate observed intheir respective long-term open-label trials.[32,35,36]
Costs
Unit drug costs (cost/pill) were obtained usingthe wholesale acquisition cost (WAC) for GXRand ATX, respectively (table I).[33] GXR had auniformWAC for different dosing strengths. Theunit cost for ATX was estimated as a weightedaverage of WACs for all dosing forms, weightedby the market share of each dosing form.[37] Dailyaverage consumption (DACON) was measuredas the number of pills consumed per day, and aDACON of 1.00 was used for both drugs in thebase-case scenario. This number was conservativefor ATXbecause the FDA-approved ATXdosingregimens include once-daily and twice-daily ad-ministration.[5] The CEA assumed that pharmacycosts consisted of only the treatment drug (i.e.GXR or ATX) costs.
Incremental medical cost associated with non-response was obtained from a study by Guevaraet al.[34] This study was selected because it esti-mated direct costs incurred by children and ado-lescents with ADHD from a third-party payer
Children and adolescentswith ADHD
Guanfacine extended-release
M
Response
Non-response (on treatment)
Titration(4 weeks)
Discontinuation
Response
Non-response (off treatment)
Discontinuation
Maintenance(48 weeks)
Response
Non-response (off treatment)
DiscontinuationResponse
Non-response (on treatment)
Discontinuation
Atomoxetine
M
M
M
Fig. 1. Model structure. ADHD =attention-deficit/hyperactivity disorder.
Cost Effectiveness of GXR vs ATX 385
Adis ª 2012 Springer International Publishing AG. All rights reserved. Appl Health Econ Health Policy 2012; 10 (6)

Table I. Model inputs for base case
Parameter Input
value
95% Confidence
interval
Source
Patient characteristics
Weight distribution Biederman et al.,[9] 2008: 96.0 lbs (54.0–271.0 lbs) [N =345]Sallee et al.,[10] 2009: 44 (SD =16) kg (25–108 kg) [N = 322]Lower bound: as observed in the GXR trial: 25 kg
Upper bound: for ATX to achieve 1.2mg/kg with maximum
labelled dose of 100mg (100/1.2 = 83 kg)
25–44 kg (could receive
0.09–0.12mg/kg/day)44.95%
44–53 kg (could receive
0.075–0.090mg/kg/day)23.88%
53–83 kg (could receive
0.046–0.075mg/kg/day)31.17%
Titration period (weeks)
GXR and ATX 4 Biederman et al.,[9] 2008;
Titration period supported by findings in Newcorn et al.[23]
2009: week 4 response was the best predictor of ultimate
clinical response
Utility
Utility for responder 0.837 Coghill et al.,[25] 2004
Utility for non-responder 0.773
ADHD-RS-IV score change and response rate
Change in ADHD-RS-IV score from baseline
GXR 0.09–0.12mg/kg/day -20.6 -23.7, -17.5 Results from MAIC
GXR 0.075–0.09mg/kg/day -19.6 -23.9, -15.3
GXR 0.046–0.075mg/kg/day -17.3 -19.9, -14.7
ATX 1.2mg/kg/day -13.6 -16.6, -10.6
Response rate
GXR 0.09–0.12mg/kg/day 80.3% 70.4, 90.3 Derived based on the change in ADHD-RS-IV score from
baselineGXR 0.075–0.09mg/kg/day 77.1% 63.3, 90.3
GXR 0.046–0.075mg/kg/day 69.7% 61.4, 78.1
ATX 1.2mg/kg/day 57.9% 48.3, 67.5
AEs
Duration (week) 4 The mean and median durations of sedative TEAEs in the
4mg/day group were 22.4 and 23.0 days, respectively.
Biederman et al.,[9] 2008
Disutilities associated AEs
Somnolence 0.10 Siddique et al.,[26] 2005
Headache 0.10 Evans[27] 1997
Fatigue 0.12 Butler et al.,[28] 2006; Lloyd et al.,[29] 2006
Abdominal pain 0.01 Anderson and Moser,[30] 1985
Vomiting 0.09 Selai et al.,[31] 2002
Nausea 0.09 Selai et al.,[31] 2002
Decreased appetite 0.09 Assumed to be the same as nausea
AEs associated with GXR GXR package insert[6]
Somnolence 38%
Headache 24%
Fatigue 14%
Abdominal pain 10%
Continued next page
386 Erder et al.
Adis ª 2012 Springer International Publishing AG. All rights reserved. Appl Health Econ Health Policy 2012; 10 (6)
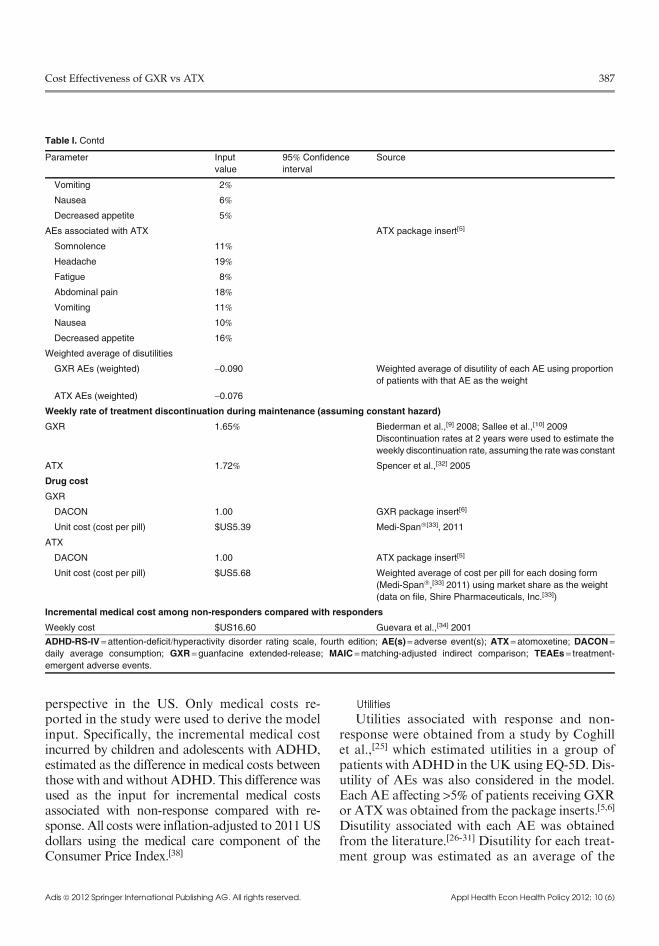
perspective in the US. Only medical costs re-ported in the study were used to derive the modelinput. Specifically, the incremental medical costincurred by children and adolescents with ADHD,estimated as the difference in medical costs betweenthose with and without ADHD. This difference wasused as the input for incremental medical costsassociated with non-response compared with re-sponse. All costs were inflation-adjusted to 2011USdollars using the medical care component of theConsumer Price Index.[38]
Utilities
Utilities associated with response and non-response were obtained from a study by Coghillet al.,[25] which estimated utilities in a group ofpatients with ADHD in theUKusing EQ-5D.Dis-utility of AEs was also considered in the model.Each AE affecting >5% of patients receiving GXRor ATXwas obtained from the package inserts.[5,6]
Disutility associated with each AE was obtainedfrom the literature.[26-31] Disutility for each treat-ment group was estimated as an average of the
Table I. Contd
Parameter Input
value
95% Confidence
interval
Source
Vomiting 2%
Nausea 6%
Decreased appetite 5%
AEs associated with ATX ATX package insert[5]
Somnolence 11%
Headache 19%
Fatigue 8%
Abdominal pain 18%
Vomiting 11%
Nausea 10%
Decreased appetite 16%
Weighted average of disutilities
GXR AEs (weighted) -0.090 Weighted average of disutility of each AE using proportion
of patients with that AE as the weight
ATX AEs (weighted) -0.076
Weekly rate of treatment discontinuation during maintenance (assuming constant hazard)
GXR 1.65% Biederman et al.,[9] 2008; Sallee et al.,[10] 2009
Discontinuation rates at 2 years were used to estimate the
weekly discontinuation rate, assuming the ratewas constant
ATX 1.72% Spencer et al.,[32] 2005
Drug cost
GXR
DACON 1.00 GXR package insert[6]
Unit cost (cost per pill) $US5.39 Medi-Span�[33], 2011
ATX
DACON 1.00 ATX package insert[5]
Unit cost (cost per pill) $US5.68 Weighted average of cost per pill for each dosing form
(Medi-Span�,[33] 2011) using market share as the weight
(data on file, Shire Pharmaceuticals, Inc.[33])
Incremental medical cost among non-responders compared with responders
Weekly cost $US16.60 Guevara et al.,[34] 2001
ADHD-RS-IV = attention-deficit/hyperactivity disorder rating scale, fourth edition; AE(s) =adverse event(s); ATX = atomoxetine; DACON =daily average consumption; GXR =guanfacine extended-release; MAIC =matching-adjusted indirect comparison; TEAEs = treatment-
emergent adverse events.
Cost Effectiveness of GXR vs ATX 387
Adis ª 2012 Springer International Publishing AG. All rights reserved. Appl Health Econ Health Policy 2012; 10 (6)
disutilities of the individual AEs weighted by theAE rates reported for each treatment group.[5,6]
Model Outputs
Model outputs included incremental cost perquality-adjusted life year (QALY) and incrementalcost per responder at 1 year. The cost effectivenessof GXR versus ATX was evaluated based on theestablished willingness-to-pay (WTP) threshold of$US50 000/QALY, which has been viewed as agenerally acceptable WTP threshold in the US.[39]
Univariate Sensitivity Analysis
To evaluate the uncertainty of model assump-tions and inputs, a univariate sensitivity analysiswas performed. The ranges for the response rates ofGXR and ATX were varied based on the 95% con-fidence intervals (CIs) of change in ADHD-RS-IVtotal score from the MAIC. Additionally, the GXRresponse rate was also varied, assuming that allpatients were in the lowest (0.046–0.075mg/kg/day)and highest dose (0.09–0.12mg/kg/day) categories,respectively. The utility associated with responsewas varied by –25% of the difference in utility be-tween response and non-response states in the basecase. Disutilities associated with AEs andGXR andATX drug unit costs were all varied by –25% of thecorresponding base-case values. In addition, thereal-world DACONs of 1.08 for GXR and 1.27 forATX, obtained from a largeUS pharmacy databaseanalysis, were used in the sensitivity analysis insteadof the base case of 1.00 for both treatments.[40]
Lastly, treatment discontinuation rates were variedin the sensitivity analyses in the following ways:(i) no discontinuation except for non-responders atthe end of the titration period, (ii) applying the base-case discontinuation rate forGXR to both treatmentgroups, and (iii) applying the base-case discontinua-tion rate for ATX to both treatment groups.
Results
Matching-Adjusted Indirect Comparison andResponse Rate Estimation
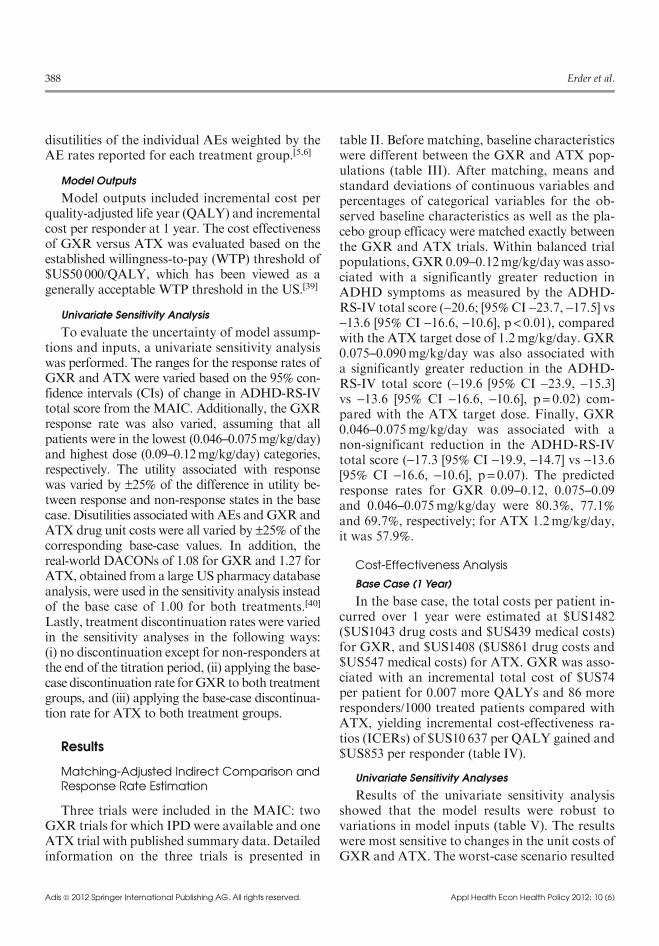
Three trials were included in the MAIC: twoGXR trials for which IPD were available and oneATX trial with published summary data. Detailedinformation on the three trials is presented in
table II. Before matching, baseline characteristicswere different between the GXR and ATX pop-ulations (table III). After matching, means andstandard deviations of continuous variables andpercentages of categorical variables for the ob-served baseline characteristics as well as the pla-cebo group efficacy were matched exactly betweenthe GXR and ATX trials. Within balanced trialpopulations, GXR 0.09–0.12mg/kg/daywas asso-ciated with a significantly greater reduction inADHD symptoms as measured by the ADHD-RS-IV total score (-20.6; [95%CI -23.7, -17.5] vs-13.6 [95% CI -16.6, -10.6], p < 0.01), comparedwith the ATX target dose of 1.2mg/kg/day. GXR0.075–0.090mg/kg/day was also associated witha significantly greater reduction in the ADHD-RS-IV total score (-19.6 [95% CI -23.9, -15.3]vs -13.6 [95% CI -16.6, -10.6], p= 0.02) com-pared with the ATX target dose. Finally, GXR0.046–0.075mg/kg/day was associated with anon-significant reduction in the ADHD-RS-IVtotal score (-17.3 [95% CI -19.9, -14.7] vs -13.6[95% CI -16.6, -10.6], p = 0.07). The predictedresponse rates for GXR 0.09–0.12, 0.075–0.09and 0.046–0.075mg/kg/day were 80.3%, 77.1%and 69.7%, respectively; for ATX 1.2mg/kg/day,it was 57.9%.
Cost-Effectiveness Analysis
Base Case (1 Year)
In the base case, the total costs per patient in-curred over 1 year were estimated at $US1482($US1043 drug costs and $US439 medical costs)for GXR, and $US1408 ($US861 drug costs and$US547 medical costs) for ATX. GXR was asso-ciated with an incremental total cost of $US74per patient for 0.007 more QALYs and 86 moreresponders/1000 treated patients compared withATX, yielding incremental cost-effectiveness ra-tios (ICERs) of $US10 637 per QALY gained and$US853 per responder (table IV).
Univariate Sensitivity Analyses
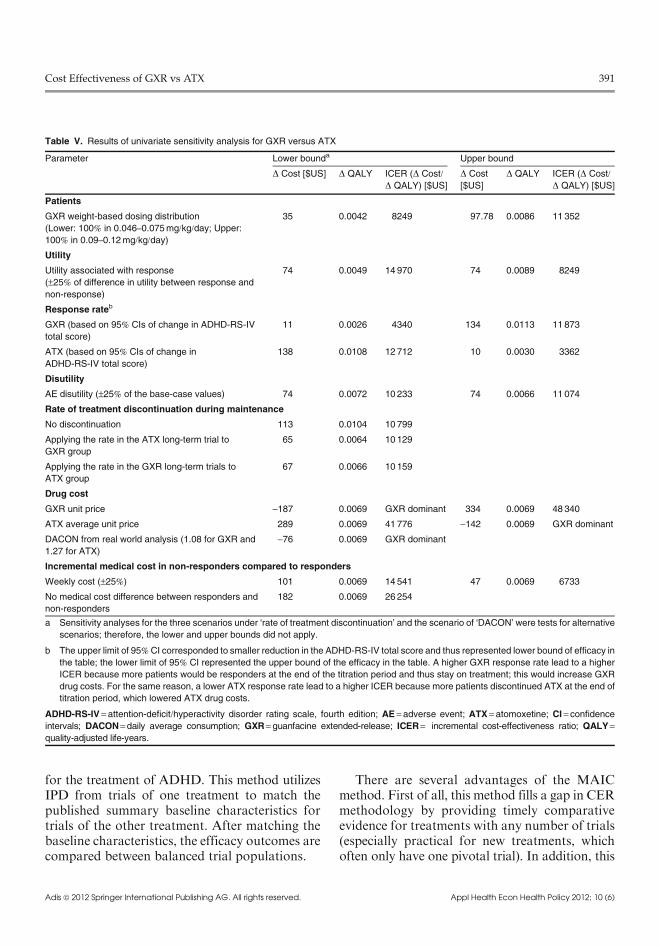
Results of the univariate sensitivity analysisshowed that the model results were robust tovariations in model inputs (table V). The resultswere most sensitive to changes in the unit costs ofGXR and ATX. The worst-case scenario resulted
388 Erder et al.
Adis ª 2012 Springer International Publishing AG. All rights reserved. Appl Health Econ Health Policy 2012; 10 (6)

Table
II.ComparisonofselectedGXRandATXtrials
Trial
GXR
ATX
Differencebetweentrials
Biederm
anetal.,[9
]2008
Salleeetal.,[10]
Michelsonetal.,[7
]2001
Keyinclusion
criteria
ADHDbasedontheDSM-IV
criteria
ADHDbasedontheDSM-IV
criteria
ADHDbasedontheDSM-IV
criteria
Atleast1.5
standard
deviations
abovetheageandgendernorm
s
fortotalA
DHD-R
S-IVscore
orits
subscale
ofinattentivescore
or
hyperactivity/im
pulsivityscore
GXRtrialsdid
notrequirecertain
baselineADHD-R
S-IVscore
level.
Suchdifferencewasaddressedby
selectingGXRpatients
basedon
thecriteriareportedin
theATXtrial
Age(years)
6–17
6–17
8–18
Inclusionof6–7yearoldsand
exclusionof18yearoldsin
the
GXRtrials.Suchdifferencemay
potentially
biasin
favourofGXR,
butmeanandSDofagewere
exactlymatched
Gender
(%female)
25.5
28.1
28.6
aThedifferencein
genderwassmall
andwasexactlymatchedin
MAIC
Dose
Randomizedto
fixeddoseof
2–4mg/day
Randomizedto
fixeddoseof
1–4mg/day
Randomizedto
aweight-based
doseof0.5,1.2
and1.8
mg/kg/day
GXRusedfixeddoseswhile
ATX
usedweight-baseddose.Weight-
baseddoseswere
compared
betweenGXRandATXin
MAIC
Followup
8weeks:5weeksofdose
escalation/m
aintenanceand
3weeksdownward
tapering
Patients’efficacywere
evaluated
weeklyin
thefirst5weeks
9weeks:3weeksofdose
escalation,3weeksofstable
dose
and3weeksofdosetapering
Patients’efficacywere
evaluated
weeklyin
thefirst6weeks
8weeksoftreatm
ent
Patients
were
evaluatedweeklyfor
thefirst4weeksandbiweekly
thereafter
ATXpatients
were
treatedlonger
withstable
dose(nodosetapering)
thanGXRpatients.Thedifference
maypotentially
biastheresultsin
favourofATX
Titration
Startingat1mg/w
eekandincrease
by1mg/w
eekuntiltherandomized
doseisreached
Startingat1mg/w
eekandincrease
by1mg/w
eekuntiltherandomized
doseisreached
Startingat0.5
mg/kg/dayforthe
firstweekandincreaseto
0.8
mg/kg/dayfor1weekandthen
1.2
mg/kg/day
Titratedonceaweekin
alltrials
Primary
outcome
measures
ADHD-R
S-IVtotalscore
ADHD-R
S-IVtotalscore
ADHD-R
S-IVtotalscore
Primary
efficacyoutcomewas
comparable
aPercentagepresentedforthetreatm
entgroupof1.2
mg/kg/day,whichwasincludedin
theMAIC.
ADHD=attention-deficit/hyperactivity-disorder;
ADHD-R
S-IV=ADHD
rating
scale,fourth
edition;ATX=atomoxetine;DSM-IV=Diagnostic
and
StatisticalManualofMental
Disorders,fourthedition;GXR=guanfacineextended-release;MAIC
=matching-adjustedindirectcomparison.
Cost Effectiveness of GXR vs ATX 389
Adis ª 2012 Springer International Publishing AG. All rights reserved. Appl Health Econ Health Policy 2012; 10 (6)

from increasing the unit cost of GXR to 125%of the base-case value, and yielded an ICER of$US48 340. When the ATX unit cost was at 75%of its base-case value, the ICER was $US41 776.GXR was dominant in three scenarios: (i) theDACON for GXR was 1.08 and for ATX was1.27 based on the real-world drug utilizationdata, (ii) ATX unit cost was at 125% of its base-case value, and (iii) GXR unit cost was at 75% ofits base-case value. GXR unit cost at 75% of thebase-case value was the best-case scenario withGXR associated with $US187 lower cost and0.007 more QALYs than ATX.
Discussion
Although head-to-head randomized clinical trialsare considered to be the gold standard in CER,[41]
such data are not always available because thesetrials are costly and time-consuming. Withouthead-to-head trials that directly compare two treat-ments, conventional CEA often relies on compara-tive effectiveness data from indirect comparisonswithout adjusting for baseline differences across
trials. Without a head-to-head direct comparison,this study applied the MAIC, a novel method inCER,[12] to compare the efficacy ofGXRandATX
Table III. Baseline characteristics before and after matching
Baseline characteristics GXR ATX
Low dose
(0.046–0.075mg/kg/day)[N =147]a
Mid dose
(0.075–0.09mg/kg/day)[N= 46]a
High dose
(0.09–0.12mg/kg/day)[N =82]a
As reportedb
(N =84)
Pre-match Post-match Pre-match Post-match Pre-match Post-match
Mean age, y (SD) 10.9 (2.5) 11.5 (2.4) 10.1 (2.0)* 11.5 (2.4) 9.0 (1.8)* 11.5 (2.4) 11.5 (2.4)
Female, % (SD) 26.5 (44.1) 28.6 (45.2) 19.6 (39.7) 28.6 (45.2) 24.4 (42.9) 28.6 (45.2) 28.6 (45.2)
ADHD subtype, % (SD)
Inattentive 26.5 (44.1) 27.4 (44.6) 23.9 (42.7) 27.4 (44.6) 18.3 (38.7) 27.4 (44.6) 27.4 (44.6)
Hyperactive-impulsive 3.4 (18.1) 1.2 (10.8) 2.2 (14.6) 1.2 (10.8) 2.4 (15.4) 1.2 (10.8) 1.2 (10.8)
Combined 70.1 (45.8) 71.4 (45.2) 73.9 (43.9) 71.4 (45.2) 79.3 (40.5) 71.4 (45.2) 71.4 (45.2)
Baseline outcomes, mean (SD)
ADHD-RS-IV total score 38.9 (8.7) 39.2 (9.2) 39.5 (8.6) 39.2 (9.2) 40.1 (7.7) 39.2 (9.2) 39.2 (9.2)
Inattention subscale score 22.1 (4.0)* 16.9 (4.0) 21.7 (4.4)* 16.9 (4.0) 21.9 (3.8)* 16.9 (4.0) 16.9 (4.0)
Hyperactivity/impulsivity
subscale score
16.8 (6.7)* 22.2 (7.1) 17.8 (6.1)* 22.2 (7.1) 18.2 (5.7)* 22.2 (7.1) 22.2 (7.1)
a The effective sample sizes of GXR dosing groups after matching were 49, 16 and 38 in 0.046–0.075mg/kg/day, 0.075–0.090mg/kg/dayand 0.09–0.12mg/kg/day, respectively.
b The GXR group was matched with the ATX group; therefore the baseline characteristics of the ATX group remained the same before and
after matching.
ADHD =attention-deficit/hyperactivity disorder; ADHD-RS-IV=ADHD rating scale, fourth edition; ATX =atomoxetine; GXR = guanfacineextended-release; SD = standard deviation. * p< 0.05.
Table IV. Results for base case
GXR ATX Incremental
(GXR – ATX)
Effectiveness
QALY 0.798 0.791 0.007
Number of responders
(per 1000 patients)a326 240 86
Costs ($US)
Drug 1043 861 182
Medical 439 547 -108
Total 1482 1408 74
ICER of GXR vs ATX
$US10 637/QALY
$US853/respondera Responders are defined as patients with ‡25% reduction in
ADHD-RS-IV total score from baseline to endpoint.
ADHD-RS-IV= attention-deficit/hyperactivity disorder rating scale,
fourth edition; ATX =atomoxetine; GXR =guanfacine extended-
release; ICER= incremental cost-effectiveness ratio; QALY= quality-adjusted life-years.
390 Erder et al.
Adis ª 2012 Springer International Publishing AG. All rights reserved. Appl Health Econ Health Policy 2012; 10 (6)
for the treatment of ADHD. This method utilizesIPD from trials of one treatment to match thepublished summary baseline characteristics fortrials of the other treatment. After matching thebaseline characteristics, the efficacy outcomes arecompared between balanced trial populations.
There are several advantages of the MAICmethod. First of all, this method fills a gap in CERmethodology by providing timely comparativeevidence for treatments with any number of trials(especially practical for new treatments, whichoften only have one pivotal trial). In addition, this
Table V. Results of univariate sensitivity analysis for GXR versus ATX
Parameter Lower bounda Upper bound
D Cost [$US] D QALY ICER (D Cost/D QALY) [$US]
D Cost
[$US]
D QALY ICER (D Cost/D QALY) [$US]
Patients
GXR weight-based dosing distribution
(Lower: 100% in 0.046–0.075mg/kg/day; Upper:100% in 0.09–0.12mg/kg/day)
35 0.0042 8249 97.78 0.0086 11 352
Utility
Utility associated with response
(–25% of difference in utility between response and
non-response)
74 0.0049 14 970 74 0.0089 8249
Response rateb
GXR (based on 95% CIs of change in ADHD-RS-IV
total score)
11 0.0026 4340 134 0.0113 11 873
ATX (based on 95% CIs of change in
ADHD-RS-IV total score)
138 0.0108 12 712 10 0.0030 3362
Disutility
AE disutility (–25% of the base-case values) 74 0.0072 10 233 74 0.0066 11 074
Rate of treatment discontinuation during maintenance
No discontinuation 113 0.0104 10 799
Applying the rate in the ATX long-term trial to
GXR group
65 0.0064 10 129
Applying the rate in the GXR long-term trials to
ATX group
67 0.0066 10 159
Drug cost
GXR unit price -187 0.0069 GXR dominant 334 0.0069 48 340
ATX average unit price 289 0.0069 41 776 -142 0.0069 GXR dominant
DACON from real world analysis (1.08 for GXR and
1.27 for ATX)
-76 0.0069 GXR dominant
Incremental medical cost in non-responders compared to responders
Weekly cost (–25%) 101 0.0069 14 541 47 0.0069 6733
No medical cost difference between responders and
non-responders
182 0.0069 26 254
a Sensitivity analyses for the three scenarios under ‘rate of treatment discontinuation’ and the scenario of ‘DACON’ were tests for alternative
scenarios; therefore, the lower and upper bounds did not apply.
b The upper limit of 95%CI corresponded to smaller reduction in the ADHD-RS-IV total score and thus represented lower bound of efficacy in
the table; the lower limit of 95% CI represented the upper bound of the efficacy in the table. A higher GXR response rate lead to a higher
ICER because more patients would be responders at the end of the titration period and thus stay on treatment; this would increase GXR
drug costs. For the same reason, a lower ATX response rate lead to a higher ICER because more patients discontinued ATX at the end of
titration period, which lowered ATX drug costs.
ADHD-RS-IV = attention-deficit/hyperactivity disorder rating scale, fourth edition; AE =adverse event; ATX = atomoxetine; CI = confidenceintervals; DACON= daily average consumption; GXR= guanfacine extended-release; ICER= incremental cost-effectiveness ratio; QALY=quality-adjusted life-years.
Cost Effectiveness of GXR vs ATX 391
Adis ª 2012 Springer International Publishing AG. All rights reserved. Appl Health Econ Health Policy 2012; 10 (6)

method allows for more extensive cross-trial ad-justment (by matching baseline characteristicsusing individual patient level data) compared withindirect comparison based only on aggregate data.
A recent publication by Signorovitch et al.[15]
also utilized the MAIC method to compare ATXand GXR in patients with ADHD and concomi-tant oppositional defiant disorder. The MAICmatching in that study was based on age, gender,height and weight and baseline ADHD-RS-IVtotal and subtype scores. Unfortunately, informa-tion on weight and height is not available in thepublished ATX trial[7] for our analysis. Thereforethe MAIC employed in this study could not matchon height and weight.
Another important difference is that the MAICmethod in the current study was adjusted forplacebo outcome during the matching whileSignorovitch et al.[15] did not adjust for placebo.When a small number of baseline characteristicsis available for matching, additional criteria, suchas balancing placebo outcomes, can help adjustfor differences between trial populations. Thisstudy incorporated the placebo arm data to im-prove the adjustment for potential unobservedcross-trial differences. That adjustment was un-necessary in Signorovitch et al.,[15] as the placebogroups were balanced between groups after theMAIC match was completed.
Lastly, other benefits of the MAIC approachinclude the fact that IPD have been a largely un-tapped resource for CER, due to prior lack ofappropriate methodology. MAIC requires IPDfrom trials of one treatment and not from theother(s) in the comparison; such IPD data are fre-quently available. Using these data, MAIC couldsubstantially increase the availability of reliablecomparative evidence for clinically and econom-ically relevant treatments.
After estimating the CER between the twodrugs, we assessed the cost effectiveness of GXRversus ATX using the comparative efficacy re-sults from MAIC. The base-case results showedthat GXR was cost effective compared with ATXat the end of the 1-year period with an ICER of$US10 637 per QALY gained. Despite the lowerWAC, GXR had an incremental drug cost of$US182 over ATX because more GXR patients
achieved response at the end of the titration periodand continued treatment. However, this incre-mental drug cost was partially offset by an averagemedical cost saving of $US108 among GXRpatients. Based on a WTP threshold of $US50000/QALY, which has been viewed as a generally ac-ceptableWTP threshold in the US,[39] GXR shouldbe considered cost effective compared with ATX inthis analysis.
Results of the univariate sensitivity analysissupported the robustness of the model as all sce-narios analysed in the current study yielded ICERsof less than $US50 000/QALY comparing GXRwith ATX. The scenario with the highest ICER($US48 340 per QALY) was when the unit costof GXR was 25% more than its base-case value.These results further support that GXR is costeffective compared with ATX for the treatment ofchildren and adolescents with ADHD.
In the current study, the results of the MAICwere applied as model inputs in the CEA model.To our knowledge, this is the first applicationof the MAIC to cost-effectiveness modelling. TheMAIC provides a more reliable comparison ofefficacy by adjusting for the differences in theobserved baseline characteristics, which results ina more reliable economic evaluation between thetwo treatments.
This is also the first CEA study comparing twonon-stimulants that are approved for once-dailydosing for the treatment of ADHD in the US. Inthe past decade, CEA has been increasingly usedto compare the values of different treatments inthe context of both clinical efficacy and economicvalues. The findings from this study could beinformative to payers as well as clinicians for as-sessing non-stimulant treatment options and se-lecting an effective and cost-effective option forchildren and adolescents with ADHD. Futureresearch should evaluate the findings from thisstudy by comparing them to the ones based onthe traditional direct and indirect comparisons.
Limitations
This study is subject to several limitations.First, as in any comparison of non-randomizedtreatment groups, MAIC assumes that there are
392 Erder et al.
Adis ª 2012 Springer International Publishing AG. All rights reserved. Appl Health Econ Health Policy 2012; 10 (6)

no unobserved confounding factors between trials.Unobserved confounding may bias the results,which can only be addressed in a head-to-headrandomized trial.
In addition, the age range included in GXRand ATX trials was different, with a younger agegroup (6–7 years) present in the GXR trials butnot the ATX trial. Although this could lead topotential bias, we do not expect that this differ-ence would have substantial impact on the resultsfrom this analysis because we matched exactly onthe mean and standard deviation of age and com-pared weight-based doses instead of fixed doses.
Another limitation, inherent in clinical trials,is the issue of generalizability. Because the MAICwas based on a few selected trials, the results maynot be generalizable to the entire ADHD pop-ulation. However, it does not affect the internalvalidity of the study.
Also, as in any CEA, the study had to makesome assumptions when deriving the model in-puts and had to populate the model with inputsfrom the existing literature that may not applyto this study population. For example, withoutdata on real-world discontinuation rates, we de-rived a weekly discontinuation rate in this 1-yearmodel based on the 2-year observed discontinua-tion rate reported in the long-term GXR andATX trials,[32,35,36] assuming a constant hazardof discontinuation. This assumption may under-estimate the discontinuation rate if patients onboth treatments are equally more likely to discon-tinue at the beginning of the treatment. However,alternative assumptions were tested in the sensi-tivity analyses, including no discontinuation andapplication of identical discontinuation rates toboth groups (in the base case, ATX had a higherdiscontinuation rate). In each case, the results wereconsistent with the base-case scenario (ranging from$US10 129 to $US10 799 per QALY comparedwith the base case of $US10 637), suggesting thatthe results are not sensitive to the discontinuationrate assumption.
Similarly, one could argue that the calculation ofdrug costs should be based on patients’ body weightinstead of market share. Unfortunately, weight wasnot reported in the ATX[7] trial, thus weight couldnot be used to estimate the dose needed for ATX.
Since this may have affected ATX costs, sensitivityanalysis accounted for this by varying the ATXunit price and daily average consumption. Theweight has less impact on GXR costs because GXRhas a uniform price for all dosing forms. Resultsfrom other univariate sensitivity analyses alsoshowed that the base-case results were robust. Therobustness of the results could be further assessedusing probabilistic sensitivity analyses.
Furthermore, the study did not consider thefollowing issues due to lack of data: (i) the sub-sequent treatments for non-responders and (ii) costeffectiveness in separate subgroups (e.g. patientswho fail or are intolerant of stimulants). Themodelcould be further improved when more data areavailable.
Finally, the study was conducted from a USthird-party perspective and therefore did not in-clude indirect costs, which are a major compo-nent of ADHD costs.[2] Future studies, adoptinga social perspective, should include indirect costsin the model to comprehensively assess the eco-nomic value of ADHD treatments.
Conclusions
This study is the first to compare the cost ef-fectiveness of GXR versus ATX in the treatmentof ADHD. To our knowledge, this is also the firstapplication of the novel comparative effectivenessmethod of MAIC to CEA. The MAIC resultsindicate that, in the trial population, GXRwithinthe dosing range of 0.075–0.12mg/kg/day was moreefficacious than ATX 1.2mg/kg/day, the highesteffective dose of ATX approved by the US FDA.The CEA results indicate that compared withATX, GXR was cost effective in the treatment ofADHD in children and adolescents at the WTPthreshold of $US50 000 per QALY gained. TheCEA results were robust as all univariate sensi-tivity analyses in this study yielded ICERs thatwere less than $US50 000/QALY. The findingscould inform treatment decisions for patients withADHD. The MAIC method used in the studyenhances the armamentarium of available meth-ods for CER and could become a useful approachfor timely economic evaluations in the future.
Cost Effectiveness of GXR vs ATX 393
Adis ª 2012 Springer International Publishing AG. All rights reserved. Appl Health Econ Health Policy 2012; 10 (6)

Acknowledgements
This research and writing support was funded by ShireDevelopment LLC. Shire develops and markets drugs to treatvarious conditions, including ADHD, and is a manufacturerof guanfacine extended release in the US. M. Haim Erder,Paul Hodgkins, and Vanja Sikirica are employees of ShireDevelopment LLC and own stock/options in Shire Develop-ment LLC. Jipan Xie, James E. Signorovitch,Mei Lu and EricQ. Wu are employees of Analysis Group, Inc., which wascontracted and funded by Shire Development LLC to partneron this research. Kristina S. Chen was an employee of Anal-ysis Group, Inc. when the manuscript was developed. Theauthors independently conducted all analyses and developedthe manuscript. MHE, JX, EQW, and VS participated in thestudy design of the matching-adjusted indirect comparison(MAIC) and the cost-effectiveness analysis (CEA); JES andML participated in the study design, conducted the analysesof theMAIC and interpreted the results; MHE, JX, KSC, PH,EQW and VS participated in different phases of model de-velopment; all authors participated in the manuscript devel-opment and revision. VS will act as the guarantor of thecontent. The contents of this manuscript, the ultimate inter-pretation and the final decision to submit it for publication inApplied Health Economics and Health Policy were madejointly by the authors.
References1. Centers for Disease Control and Prevention. Attention-
deficit/hyperactivity disorder (ADHD) data and statistics[online]. Available from URL: http://www.cdc.gov/ncbddd/adhd/data.html [Accessed 2012 Jan 06]
2. Doshi JA, Hodgkins P, Kahle J, et al. Economic impact ofchildhood and adult attention deficit hyperactivity disorderin the United States. J Am Acad Child Adolesc Psychiatry2012 Oct; 51 (10): 990-1002
3. Gilmore A, Milne R. Methylphenidate in children with hy-peractivity: review and cost-utility analysis. Pharmacoepi-demiol Drug Saf 2001 Mar-Apr; 10 (2): 85-94
4. Findling RL. Evolution of the treatment of attention-deficit/hyperactivity disorder in children: a review. Clin Ther 2008May; 30 (5): 942-57
5. Strattera� (atomoxetine hydrochloride) capsules for oral use[package insert]. Available from URL: http://pi.lilly.com/us/strattera-pi.pdf [Accessed on 2012 Oct 09]
6. INTUNIV� (guanfacine) extended-release tablets [packageinsert]. Available from URL: http://pi.shirecontent.com/PI/PDFs/Intuniv_USA_ENG.pdf [Accessed on 2012 Oct 09]
7. Michelson D, Faries D, Wernicke J, et al., AtomoxetineADHD Study Group. Atomoxetine in the treatment ofchildren and adolescents with attention-deficit/hyperactivitydisorder: a randomized, placebo-controlled, dose-responsestudy. Pediatrics 2001 Nov; 108 (5): E83
8. Michelson D, Allen AJ, Busner J, et al. Once-daily atomox-etine treatment for children and adolescents with attentiondeficit hyperactivity disorder: a randomized, placebo-controlled study. Am J Psychiatry 2002; 159: 1896-901
9. Biederman J, Melmed RD, Patel A, et al. A randomized,double-blind, control-controlled study of guanfacine ex-
tended release in children and adolescents with attention-deficit/hyperactivity disorder. Pediatrics 2008 Jan; 121 (1):E73-84
10. Sallee F, McGough J, Wigal T, et al., on behalf of theSPD503 Study Group. Guanfacine extended release in chil-dren and adolescents with attention-deficit/hyperactivitydisorder: a control-controlled trial. J Am Acad Child Ado-lesc Psychiatry 2009 Feb; 48 (2): 155-65
11. Wu EQ, Hodgkins P, Ben-Hamadi R, et al. Cost effective-ness of pharmacotherapies for attention-deficit hyper-activity disorder: a systematic literature review. CNSDrugs 2012; 26 (7): 1-20
12. Signorovitch JE, Wu EQ, Yu AP, et al. Comparative effec-tiveness without head-to-head trials: a method for match-ing adjusted indirect comparisons applied to psoriasistreatment with adalimumab or etanercept. Pharmacoeco-nomics 2010; 28 (10): 935-45
13. Signorovitch JE, Wu EQ, Betts KA, et al. Comparativeefficacy of nilotinib and dasatinib in newly diagnosedchronic myeloid leukemia: a matching-adjusted indirectcomparison of randomized trials. Curr Med Res Opin2011; 27 (6): 1263-71
14. Signorovitch JE, Wu EQ, Swallow E, et al. Comparativeefficacy of vildagliptin and sitagliptin in Japanese patientswith type 2 diabetes mellitus: a matching-adjusted indirectcomparison of randomized trials. Clin Drug Investig 2011;31 (9): 665-74
15. Signorovitch J, Erder MH, Xie J, et al. Comparative effective-ness research using matching-adjusted indirect comparison:an application to treatment with guanfacine extended releaseor atomoxetine in children with attention-deficit/hyperactivitydisorder and comorbid oppositional defiant disorder. Phar-macoepidemiol Drug Saf 2012; 21 (S2): 130-7
16. Signorovitch J, Sikirica V, Erder MH, et al. Matching-adjusted indirect comparisons: a new tool for timely com-parative effectiveness. Value Health 2012 Sep; 15 (6): 940-7
17. Efron B, Tibshirani R. An introduction to the bootstrap.Boca Raton, FL: Chapman & Hall/CRC Press, 1993
18. Kelsey DK, Sumner CR, Casat CD, et al. Once-daily atomox-etine treatment for children with attention-deficit/hyperactivitydisorder, including an assessment of evening and morningbehavior: a double-blind, placebo-controlled trial. Pedia-trics 2004; 114 (1): e1-8
19. Kaplan S, Heiligenstein J, West S, et al. Efficacy and safetyof atomoxetine in childhood attention-deficit/hyperactivitydisorder with comorbid oppositional defiant disorder.J Atten Disord 2004; 8 (45): 45-52
20. Spencer T, Biederman J, Heiligenstein J, et al. An open-label, dose-ranging study of atomoxetine in children withattention deficit hyperactivity disorder. J Child AdolescPsychopharmacol 2001; 11 (3): 251-65
21. Spencer T, Heiligenstein JH, Biederman J, et al. Results from2 proof-of-concept, placebo-controlled studies of atomox-etine in children with attention-deficit/hyperactivity dis-order. J Clin Psychiatry 2002; 63: 1140-7
22. Prasad S, Arellano J, Steer C, et al. Assessing the value ofatomoxetine in treating children and adolescents withADHD in the UK. Int J Clin Pract 2009; 63 (7): 1031-40
23. Newcorn JH, Sutton V, Weiss MD, et al. Clinical responsesto atomoxetine in attention-deficit/hyperactivity disorder:
394 Erder et al.
Adis ª 2012 Springer International Publishing AG. All rights reserved. Appl Health Econ Health Policy 2012; 10 (6)

the integrated data exploratory analysis (IDEA) Study.J Am Acad Child Adolesc Psychiatry 2009; 48 (5): 511-8
24. King S, Griffin S, Hodges Z, et al. A systematic review andeconomic model of the effectiveness and cost-effectivenessof methylphenidate, dexamfetamine and atomoxetine forthe treatment of attention deficit hyperactivity disorder inchildren and adolescents. Health Technol Assess 2006 Jul;10 (23): iii-iv,xiii-146
25. Coghill D, Spender Q, Barton J, et al. Measuring quality oflife in children with attention-deficit-hyperactivity disorderin the United Kingdom. Poster presented at the 16thWorldCongress of the International Association of Child andAdolescent Psychiatry and Allied Professions (IACAPAP);2004 Aug 23–26; Berlin
26. Siddique R, Markowitz J, Engelhart L. Impact of atypicalantipsychotic drug sedation on quality of life. Atlanta, GA:American Psychiatric Association, 2005
27. Evans KW. Economic evaluation of oral sumatriptan com-pared with oral caffeine/ergotamine for migraine. Pharma-coeconomics 1997; 12 (5): 565-77
28. Butler JM, Rapp SR, Shaw EG. Managing the cognitiveeffects of brain tumor radiation therapy. Curr Treat OptionsOncol 2006; 7 (6): 517-23
29. Lloyd A, Nafees B, Narwska J, et al. Health state utilities formetastic breast cancer. Br J Cancer 2006; 95: 683-90
30. Anderson JP, Moser RJ. Parasite screening and treatmentamong Indochinese refugees: cost-benefit/utility and theGeneral Health Policy Model. JAMA 1985; 253 (15): 2229-35
31. Selai C, Trimble M, Kaiser S, et al. New anti-epilipeticdrugs: clinical outcomes and utility scores [poster P330].5th European Congress on Epileptology; 2002 Oct 6-10;Madrid
32. Spencer TJ, Newcorn JH, Kratochvil C, et al. Effects ofatomoxetine on growth after 2-year treatment among pe-diatric patients with attention-deficit/hyperactivity dis-order. Pediatrics 2005; 116: e74-80
33. Medi-Span�. Master Drug Data Base v2.5 (MDDB�). In-dianapolis (IN): Medi-Span� [online]. Available fromURL: http://www.medispan.com/master-drug-database.aspx[Accessed 2011 Jul 22]
34. Guevara J, Lozano P, Wikizer T, et al. Utilization and costof health care services for children with attention-deficit/hyperactivity disorder. Pediatrics 2001; 108 (1): 71-8
35. Biederman J, Melmed RD, Patel A, et al. Long-term, open-label extension study of guanfacine extended release inchildren and adolescents with ADHD. CNS Spectr 2008Dec; 13 (12): 1047-55
36. Sallee F, Lyne A, Wigal T, et al. Long-term safety andefficacy of guanfacine extended release in children andadolescents with attention-deficit/hyperactivity disorder.J Child Adolesc Psychopharmacol 2009 Jun; 19 (3): 215-26
37. Market share of different dosing forms of atomoxetine.Wayne, PA: Shire Development LLC, 2011. (Data on file)
38. United States Department of Labor, Bureau of Labor Sta-tistics. Consumer price index databases [online]. Availablefrom URL: http://www.bls.gov/cpi/data.htm [Accessed2012 Jun 06]
39. Hlatky MA, Owens DK, Sanders GD. Cost-effectiveness asan outcome in randomized clinical trials. Clinical Trials2006; 3 (6): 543-51
40. Daily average consumption of guanfacine extended releaseand atomoxetine. Wayne, PA: Shire Development LLC,2011. (Data on file)
41. Teutsch SM, Berger ML, Weinstein MC. Comparativeeffectiveness: asking the right questions, choosing the rightmethod. Health Aff (Millwood) 2005; 24 (1): 128-32
Correspondence: Vanja Sikirica, PharmD, MPH, ShireDevelopment LLC, 725 Chesterbrook Boulevard, Wayne,PA 19087, USA.E-mail: [email protected]
Cost Effectiveness of GXR vs ATX 395
Adis ª 2012 Springer International Publishing AG. All rights reserved. Appl Health Econ Health Policy 2012; 10 (6)