Cost-effectiveness of different strategies of cytomegalovirus prophylaxis in orthotopic liver...
7
Cost-Effectiveness of Different Strategies of Cytomegalovirus Prophylaxis in Orthotopic Liver Transplant Recipients ANANYA DAS Cytomegalovirus (CMV) is an important cause of morbid- ity and mortality in liver transplant recipients and several different strategies of CMV chemoprophylaxis are in prac- tice. A cost-effective analysis was performed to compare these strategies. A hypothetical cohort of liver transplant recipients was followed up for a year posttransplantation in a Markov model, as they made possible transitions to different states of health with respect to CMV infection and disease. Different strategies of chemoprophylaxis were compared. Cost per patient, yield in terms of gain in quality-adjusted stages, amount of time spent in the state of CMV disease, and CMV-related mortality were the outcome measures compared. Oral ganciclovir administered univer- sally to all transplant recipients was the most favored strategy. Restricting prophylaxis to defined high-risk groups or extending the duration of prophylaxis beyond 3 months did not improve cost-effectiveness. The strategy of short- term, oral ganciclovir-based chemoprophylaxis for CMV in liver transplant recipients is cost-effective by current stan- dards of healthcare interventions. (HEPATOLOGY 2000;31:311- 317.) Cytomegalovirus (CMV), a commonly encountered patho- gen after liver transplantation, is a major cause of concern in the initial posttransplantation period accounting for signifi- cant morbidity, mortality, prolonged hospitalization, and increased cost. 1,2 Chemoprophylaxis of CMV infection in the posttransplantation period has recently received considerable attention and different chemoprophylactic regimens have been shown in controlled trials to be effective in preventing CMV-related mortality and morbidity. 3 Although chemopro- phylaxis of CMV infection has become the standard of care in orthotopic liver transplant recipients, in absence of compara- tive data, several different chemoprophylactic regimens are in practice. Ganciclovir, either in the parenteral and more recently available oral form, seems to be more effective than acyclovir based regimens, 4,5 but higher cost with ganciclovir remains a major concern. A comparative cost-effective analy- sis of different chemoprophylactic regimens against CMV is needed to identify the most cost-effective regimen. Natural history of CMV infection and disease in the posttransplanta- tion setting is well studied and several risk factors that particularly predispose to CMV-related morbidity have been identified. 6 It would be also of interest to evaluate if restrict- ing CMV chemoprophylaxis to these high-risk groups will improve cost-effectiveness of CMV chemoprophylaxis. PATIENTS AND METHODS To study and compare the cost-effectiveness of different strategies of chemoprophylaxis against CMV in orthotopic liver transplant recipients from a societal perspective, a Markov model (Fig. 1) was constructed with the help of decision analysis software (DATA 3.5; TreeAge Softwares, Williamstown, MA). The Markov model is a decision analysis tool widely used to study the impact of different health care interventions, particularly in the context of a prolonged time horizon and recurring risk of a particular disease. Briefly, in a Markov model, different states of health (with allocated reward values for being in that state), associated with a particular disease are defined. Transitional prob- abilities from one state to another are obtained from available information. The model is run for several cycles to simulate the natural history of the problem, and at the end of each cycle, cumulative reward values in terms of outcome measures are calculated. 7 In this model, a hypothetical cohort of 1,000 orthotopic liver transplant recipients in 7 different posttransplantation states of health with particular attention to CMV infection and disease was considered. These different states of health were healthy transplant recipients, those undergoing acute rejection and those with chronic rejection, transplant recipients with CMV infection but without any evidence of CMV disease, transplant recipients with CMV disease and those with CMV disease complicated by severe opportunistic infection(s); the seventh state was death either related or unrelated to CMV disease. For the purpose of this decision analysis, CMV infection was defined as isolation or identification of CMV from any site (blood, urine, sputum, or stool samples) or positive seroconver- sion (presence of CMV immunoglobulin M [IgM] or 4-fold increase in CMV IgG titers) in the absence of clinical symptoms. 6 In contrast, CMV disease was defined as invasive or symptomatic CMV infection with histopathological evidence of viral cytopathic effect or a positive CMV culture from a deep tissue specimen in the setting of suggestive clinical manifestations. CMV syndrome, as defined by positive markers of CMV infection accompanied by otherwise unexplained fever with leukopenia and disseminated CMV disease (multiorgan tissue invasive disease) were also included under the broad category of CMV disease. 6 The model allowed transition from one state to another depending on the transitional probabilities, which were obtained from literature (Fig. 2). For example, from the state of healthy transplant recipients, patients could make a transi- tion to any other states of health or they could remain in the same state in the next Markov cycle. Certain transitions were not allowed in this model; for example, chronic rejection was considered irreversible and patients could not make a transition from the state of chronic rejection to the healthy state. Transition to the dead state Abbreviations: CMV, cytomegalovirus; CMV Ig, CMV immunoglobulin. From the Division of Gastroenterology, University Hospitals, Case Western Reserve University, Cleveland, OH. Received April 20, 1999; accepted November 16, 1999, Address reprint requests to: Ananya Das, M.D., Division of Gastroenterology, University Hospitals of Cleveland, 11100 Euclid Ave., Wearn II, Cleveland, OH 44106. E-mail: [email protected]; fax: (216) 844-8011. Copyright r 2000 by the American Association for the Study of Liver Diseases. 0270-9139/00/3102-0009$3.00/0 311
-
Upload
ananya-das -
Category
Documents
-
view
213 -
download
1
Transcript of Cost-effectiveness of different strategies of cytomegalovirus prophylaxis in orthotopic liver...

Cost-Effectiveness of Different Strategies of CytomegalovirusProphylaxis in Orthotopic Liver Transplant Recipients
ANANYA DAS
Cytomegalovirus (CMV) is an important cause of morbid-ity and mortality in liver transplant recipients and severaldifferent strategies of CMV chemoprophylaxis are in prac-tice. A cost-effective analysis was performed to comparethese strategies. A hypothetical cohort of liver transplantrecipients was followed up for a year posttransplantation ina Markov model, as they made possible transitions todifferent states of health with respect to CMV infection anddisease. Different strategies of chemoprophylaxis werecompared. Cost per patient, yield in terms of gain inquality-adjusted stages, amount of time spent in the state ofCMV disease, and CMV-related mortality were the outcomemeasures compared. Oral ganciclovir administered univer-sally to all transplant recipients was the most favoredstrategy. Restricting prophylaxis to defined high-risk groupsor extending the duration of prophylaxis beyond 3 monthsdid not improve cost-effectiveness. The strategy of short-term, oral ganciclovir-based chemoprophylaxis for CMV inliver transplant recipients is cost-effective by current stan-dards of healthcare interventions. (HEPATOLOGY 2000;31:311-317.)
Cytomegalovirus (CMV), a commonly encountered patho-gen after liver transplantation, is a major cause of concern inthe initial posttransplantation period accounting for signifi-cant morbidity, mortality, prolonged hospitalization, andincreased cost.1,2 Chemoprophylaxis of CMV infection in theposttransplantation period has recently received considerableattention and different chemoprophylactic regimens havebeen shown in controlled trials to be effective in preventingCMV-related mortality and morbidity.3 Although chemopro-phylaxis of CMV infection has become the standard of care inorthotopic liver transplant recipients, in absence of compara-tive data, several different chemoprophylactic regimens are inpractice. Ganciclovir, either in the parenteral and morerecently available oral form, seems to be more effective thanacyclovir based regimens,4,5 but higher cost with ganciclovirremains a major concern. A comparative cost-effective analy-sis of different chemoprophylactic regimens against CMV isneeded to identify the most cost-effective regimen. Natural
history of CMV infection and disease in the posttransplanta-tion setting is well studied and several risk factors thatparticularly predispose to CMV-related morbidity have beenidentified.6 It would be also of interest to evaluate if restrict-ing CMV chemoprophylaxis to these high-risk groups willimprove cost-effectiveness of CMV chemoprophylaxis.
PATIENTS AND METHODS
To study and compare the cost-effectiveness of different strategiesof chemoprophylaxis against CMV in orthotopic liver transplantrecipients from a societal perspective, a Markov model (Fig. 1) wasconstructed with the help of decision analysis software (DATA 3.5;TreeAge Softwares, Williamstown, MA).
The Markov model is a decision analysis tool widely used to studythe impact of different health care interventions, particularly in thecontext of a prolonged time horizon and recurring risk of aparticular disease. Briefly, in a Markov model, different states ofhealth (with allocated reward values for being in that state),associated with a particular disease are defined. Transitional prob-abilities from one state to another are obtained from availableinformation. The model is run for several cycles to simulate thenatural history of the problem, and at the end of each cycle,cumulative reward values in terms of outcome measures arecalculated.7
In this model, a hypothetical cohort of 1,000 orthotopic livertransplant recipients in 7 different posttransplantation states ofhealth with particular attention to CMV infection and disease wasconsidered. These different states of health were healthy transplantrecipients, those undergoing acute rejection and those with chronicrejection, transplant recipients with CMV infection but without anyevidence of CMV disease, transplant recipients with CMV diseaseand those with CMV disease complicated by severe opportunisticinfection(s); the seventh state was death either related or unrelatedto CMV disease. For the purpose of this decision analysis, CMVinfection was defined as isolation or identification of CMV from anysite (blood, urine, sputum, or stool samples) or positive seroconver-sion (presence of CMV immunoglobulin M [IgM] or 4-fold increasein CMV IgG titers) in the absence of clinical symptoms.6 In contrast,CMV disease was defined as invasive or symptomatic CMV infectionwith histopathological evidence of viral cytopathic effect or apositive CMV culture from a deep tissue specimen in the setting ofsuggestive clinical manifestations. CMV syndrome, as defined bypositive markers of CMV infection accompanied by otherwiseunexplained fever with leukopenia and disseminated CMV disease(multiorgan tissue invasive disease) were also included under thebroad category of CMV disease.6 The model allowed transition fromone state to another depending on the transitional probabilities,which were obtained from literature (Fig. 2). For example, from thestate of healthy transplant recipients, patients could make a transi-tion to any other states of health or they could remain in the samestate in the next Markov cycle. Certain transitions were not allowedin this model; for example, chronic rejection was consideredirreversible and patients could not make a transition from the stateof chronic rejection to the healthy state. Transition to the dead state
Abbreviations: CMV, cytomegalovirus; CMV Ig, CMV immunoglobulin.From the Division of Gastroenterology, University Hospitals, Case Western Reserve
University, Cleveland, OH.Received April 20, 1999; accepted November 16, 1999,Address reprint requests to: Ananya Das, M.D., Division of Gastroenterology,
University Hospitals of Cleveland, 11100 Euclid Ave., Wearn II, Cleveland, OH 44106.E-mail: [email protected]; fax: (216) 844-8011.
Copyright r 2000 by the American Association for the Study of Liver Diseases.0270-9139/00/3102-0009$3.00/0
311

was allowed from any other states; however, death was consideredan absorbing state from which transition to no other state waspossible. The model was run for a total of 12 cycles, each cycle beingof a duration of 1 month; at the end of each cycle, the simulationmodel accrued units of utility and cost for each cohort member in agiven state of health. The cohort of transplant recipients accumu-lated cost and utility units until either death occurred or the totalnumber of cycles were completed. Utility for each health state wasadjusted by the quality of life associated with that state. Suchadjustment of the utility of different states of health with quality oflife values for that particular state, enables the model to estimate thenumber of quality-adjusted months gained with different strategies.
In the present model, estimated quality of life associated with thedifferent posttransplantation states of health (Table 2) were based onthe expert opinion of a group of physicians experienced in theposttransplantation care of orthotopic liver transplant recipients.
The model was limited to the first year after liver transplantationin view of the rarity of CMV-related morbidity and mortality beyondthis period in this particular clinical setting, and also because of thepaucity of data regarding CMV prophylaxis beyond this time-frame.In the first posttransplantation year, the incidence of acute rejectionand CMV infection and disease are not uniformly distributed withthe majority of these episodes occurring rather early in the posttrans-plantation period. To better simulate this differing incidence ofrejection episodes and CMV-related morbidity, the entire time-frameof the model was divided into 2 epochs. Epoch 1 encompasses thefirst 3 months after liver transplantation when most of the rejectionepisodes and CMV-related morbidity are encountered. Epoch 2encompasses the remaining 9 months in the first posttransplanta-tion year. Based on available literature, it was assumed that 90% ofprimary or secondary CMV infection, CMV disease, and also,episodes of acute rejection occur in the first 3 months after livertransplantation.
8 -11In the Markov model, the transitional probabili-
ties in epoch 1 and 2 were appropriately adjusted to reflect thistime-dependent variability in the incidence of rejection episodes,CMV infection, and disease. Stage-specific transitional probabilitieswere calculated by transforming rates to probabilities, accountingfor cycle length, using the standard formula.7
This decision analysis was performed in 2 parts. Initially, 5different strategies of chemoprophylaxis were compared in themodel. In this initial part of the analysis, chemoprophylaxis wasadministered to all patients undergoing liver transplantation. In thesecond part of the analysis, the best 2 strategies identified in theinitial analysis were further evaluated to determine if restrictingCMV chemoprophylaxis to those patients who were considered tobe at high risk for CMV-related disease after liver transplantationwould improve cost-effectiveness. Two high-risk groups were consid-ered in this model.6 Seronegative recipients of seropositive donorswere considered to be highly susceptible to CMV infection andconsequent CMV disease. The other high-risk group comprisedtransplant recipients who developed steroid-resistant rejection andwere treated with antilymphocyte antibodies (OKT3). Althoughretransplantation was another high-risk category, this was notconsidered in the present model.
In the second part of this analysis, the model was constructed insuch a way that all patients who were seronegative recipients ofseropositive donors would receive prophylaxis against CMV withthe chemoprophylactic regimen under consideration. The remain-der of the transplant recipients would receive CMV prophylaxis onlyif they developed an episode of steroid-resistant rejection requiringantilymphocyte antibody (OKT3) treatment. The duration of CMVprophylaxis was limited to 2 months starting on the day antilympho-cyte antibody (OKT3) was begun. Based on available litera-ture4,5,12,13 ganciclovir-based prophylaxis against CMV in the high-risk patients was assumed to be as effective as in the generalpopulation of transplant recipients. The different chemoprophylaxisregimens considered in this analysis along with dose, duration, routeof administration, cost, and effectiveness in preventing CMV infec-tion and disease are shown in Table 1. The data regarding thepreviously mentioned parameters were obtained from various pub-lished, randomized, controlled clinical trials.4,5,14-16
Probability estimates of clinical variables (Table 2) used in themodel were obtained from available literature; when sufficient datawere not available, estimates were made based on expert opinion.Cost estimates (Table 2) were obtained from a University Hospitalbased medium-sized liver transplantation program, which werecomparable to those published in literature. Hospital charges for atypical patient were calculated and to better approximate the actualcost, cost to charge ratio was used to derive the actual cost fromhospital charges. In view of the 1-year time horizon of this decisionanalysis, neither the cost estimates nor gain in quality-adjusted
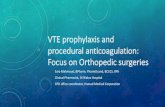
FIG. 1. Decision tree representing different strategies of prophylaxisagainst CMV in liver transplant recipients. (j) represents the decision nodewhere a particular strategy is chosen; (d) denotes chance nodes representingprobability of having a D1, R2* (seropositive donor and seronegativerecipient) status and probability of undergoing treatment with antilympho-cyte antibody for steroid-resistant rejection. At the right, the cohorts enterrespective Markov nodes, denoted by ‘‘M.’’
FIG. 2. Different Markov states of health after liver transplantation. Thearrows denote possible transitions from one state to another as allowed in themodel in a single Markov cycle. AR, acute rejection; CR, chronic rejection;CMVI, CMV infection; CMVD, CMV disease; Infect, CMV disease compli-cated by severe opportunistic infection(s).
312 DAS HEPATOLOGY February 2000

stages were discounted. Because in a Markov model, it is assumedthat all transitions occur at the end of a cycle whereas transitionsactually occur throughout the cycle, half cycle corrections weremade for both cost and utility values. All dollar values were adjustedto 1995 US dollars.
Cost-effectiveness ratio of different chemoprophylaxis strategiesin terms of cost and gain in quality-adjusted stages were the primaryoutcome measures studied in the model. Incremental cost-effectiveness ratio, percentage time of the first posttransplantationyear spent in CMV disease state, and mortality directly related toCMV disease were the secondary outcome measures comparedamong different strategies.
In addition to the baseline analysis, sensitivity analyses wereperformed with clinically important variables, particularly whendefinite estimates were not available to test the robustness of theconclusions of the baseline analysis. The data on the effectiveness ofdifferent prophylactic regimens were obtained from available con-trolled studies; these studies, however, are few in number andobviously reflect the experience of only a few large transplantationcenters. To adequately assess the effect of variability of theseassumptions, a second-order Monte Carlo simulation was per-formed using the hypothetical cohort of transplant recipientsconsidered in the model. In a Monte Carlo simulation, only onemember of the cohort enters the decision tree at one time; this
TABLE 1. Different Strategies of Chemo-prophylaxis Against CMV Considered in This Model
Strategy RegimenCost*
(range 6 25%) ($)Baseline Prob of CMV
Infection (range)Baseline Prob of
CMV Disease (range) References
1 GCV 6 mg/kg/d for 30 days, then 5 mg/kg/d, 5 days in a week for total100 days given IV
13,000 5%(1%-10%)
1%(0%-5%)
4
2 GCV 1,000 mg 3 times a day orally for 100 days 5,000 25%(10%-40%)
5%(1%-10%)
5
3 CMV Ig 150 mg/kg/IV within 72 h of transplant, then at 2, 4, 6, 8 wkand 100 mg/kg/IV at 12, 16 wk
9,000 57%(25%-75%)
19%(5%-30%)
14
4 ACV 800 mg orally 4 times/d for 6 mo 3,000 42%(20%-70%)
29%(10%-50%)
15
5 ACV 800 mg orally 4 times/d for 3 mo 1,500 61%(25%-75%)
28%(10%-50%)
16
Abbreviations: GCV, ganciclovir; ACV, acyclovir; IV, intravenous.*Cost includes cost of administration and is based on average wholesale price, data from Drug Topics Red Book. Montvale, NJ, Medical Economics Co, Inc,
1998.
TABLE 2. Probability Estimates of Important Clinical and Cost Variables Used in the Model
Clinical Variables Baseline (range) References
ProbabilityDonor positive, recipient-negative status (D1, R2) in a cohort of liver transplant recipients 0.1 (0-0.3) 19Acute rejection during the first year after transplant 0.65 (0.6-0.75) 10,11Patients developing steroid-resistant rejection requiring OKT3 treatment during the first year after transplant 0.3 (0.1-0.5) 10,11,20Chronic rejection during first year after transplant 0.05 (0.01-0.1) 10,21,221-year mortality after liver transplantation (from all causes) 0.12 (0.05-.20) 23Developing CMV disease after acquiring primary or secondary CMV infection in the first year after trans-
plant without chemo-prophylaxis 0.6 (0.5-0.7) 24Severe opportunistic infection in patients with CMV disease after liver transplantation 0.3 (0.1-0.5) 25-27Mortality from CMV disease in first year after transplant 0.2 (0.1-0.4) 28Recurrent CMV disease after a course of ganciclovir 0.2 (0.1-0.4) 29
Estimated quality of life associated with different posttransplant states of health EstimateHealthy 1.0 (0.9-1.0)Acute rejection 0.9 (0.85-1.0)Chronic rejection 0.5 (0.3-0.7)CMV infection 1.0 (0.9-1.0)CMV disease 0.75 (0.5-0.9)Severe opportunistic infection in patients with CMV disease 0.5 (0.3-0.7)
Cost variables ($)Standard follow-up care for the first year after liver transplant excluding initial transplant hospitalization
costs* 50,000 (25,000-100,000) Estimate, 30-33Diagnostic work-up of CMV disease (includes cost of diagnostic serological and virology tests and organ
specific tests viz. liver biopsy, endoscopy, bronchoscopy, etc.) 3,000 (2,000-10,000) EstimateTreatment of CMV disease over a period of 1 month (includes cost of medications viz. intravenous ganci-
clovir for a minimum period of 2 weeks, follow-up investigations to monitor treatment results and anypossible complications) 10,000 (5,000-20,000) Estimate† 34,35
Management of an episode of acute rejection (including diagnostic liver biopsy, cost of intravenous high-dose steroid therapy, etc.) 5,000 (3,000-10,000) Estimate
Additional cost of OKT3 (Orthoclone OKTR therapy; OthoBiotech, Raritan, NJ) 2,000 (1,000-3,000) Estimate†
*This includes cost of immunosuppressive and other medications, readmissions, office visits, and outpatient and inpatient procedures along with estimatedprofessional fees in the first year after transplant.
†Cost of drug includes cost of administration and is based on average wholesale price; data from Drug Topics Red Book, Montvale, NJ, Medical EconomicsCo, Inc, 1998.
HEPATOLOGY Vol. 31, No. 2, 2000 DAS 313

individual member travels down the tree guided by the assignedprobabilities at each node. At the initial decision node, the chance ofgoing down a particular branch is determined by a random numbergenerator. In second-order Monte Carlo simulation, some probabili-ties at each node are represented as distributions rather thanfixed-point estimates. During each individual simulation trial onevalue of the distribution is randomly sampled, thus enabling themodel to vary the input variables from one run to another andassessing the impact of such variability on the outcome variables.The second-order Monte Carlo simulation, in addition to serving thepurpose of a dynamic sensitivity analysis, also provides usefulstatistical estimates, e.g., confidence intervals of outcome variables.In the present model, probability estimates of developing CMVinfection and disease while receiving different prophylactic regi-mens were entered in the model as triangular distributions, with thebaseline values being the most likely probability estimates, and thelower and upper bounds of the distribution reflecting the possiblerange of the probability estimates. All statistical analyses wereperformed using statistical software (Statsoft; Statistica, Tulsa, OK).
Several assumptions were made in constructing the presentmodel. It was assumed that a CMV-seronegative patient could notdevelop CMV disease without transition through the state of CMVinfection. Also assumed was that to reduce the risk of transfusion-associated CMV infection, in the setting of a donor negative,recipient-negative matching, blood transfusions from CMV-seroposi-tive donors would be avoided and leukocyte-filtered blood productswould be used.9,17,18 It was also assumed that all patients diagnosedwith CMV disease would be treated with intravenous ganciclovir fora minimum period of 2 weeks and during the period of treatmentwould not receive any chemoprophylaxis. Another assumption wasthat non–CMV-related deaths were uniformly distributed over thefirst posttransplantation year. No extra cost was associated withtransition to a dead state. For purposes of dose calculation, a 70-kgpatient with normal renal function was considered.
RESULTS
The results of the baseline analysis comparing 5 differentchemoprophylaxis strategies against CMV are shown in Table3. The strategy of chemoprophylaxis with intravenous ganci-clovir, followed up closely by the strategy of chemoprophy-laxis with oral ganciclovir, were the most effective strategiesin terms of yield in quality-adjusted stages, decrease in time
spent in the state of CMV disease, and CMV-related mortality.The incremental cost-effectiveness ratio of strategy 1 overstrategy 2 was $ 7,523,478 per quality-adjusted life yeargained.
Strategy 3 was clearly dominated by strategy 1 and 2, i.e.,strategy 3 was more costly, and simultaneously less effective.Similarly, strategy 4 and 5 were also dominated by strategy 2.Between strategies 4 and 5, it was apparent that by extendingchemoprophylaxis up to 6 months (strategy 4), effectivenessis only marginally improved with an incremental cost-effectiveness ratio of $189,865 per quality-adjusted life yeargained.
Once the 2 best strategies were identified, they were furtheranalyzed in the second stage of the decision analysis. Basedon whether chemoprophylaxis should be restricted to thosetransplant recipients who were known to be at higher risk forCMV-related disease, or should be administered to all recipi-ents of liver transplantation irrespective of their risk status, atotal of 4 substrategies were compared (Table 4). Strategies ofuniversal chemoprophylaxis with either intravenous or oralganciclovir administered to all transplant recipients wereboth more effective and costly compared to those strategies inwhich chemoprophylaxis was restricted to the high-riskgroups. In terms of incremental cost-effectiveness ratio,universal oral ganciclovir prophylaxis was the most favoredstrategy.
One-way sensitivity analyses performed by varying theprobability estimates of proportion of donor positive, recipient-negative serological status in the cohort of transplant recipi-ents, probability of developing steroid-resistant rejectionduring the first year after transplantation, probability ofoverall mortality in the first posttransplantation year, andprobability of recurrent CMV disease did not change theconclusions of the baseline analysis. Similarly, the model wasinsensitive to changes in the different cost variables withinthe range used for this analysis viz. cost of standard follow-upcare in the first posttransplantation year, cost of diagnosticwork-up when CMV disease was suspected, and cost oftreatment of CMV disease. When a 2-way sensitivity analysis
TABLE 3. Results of the Baseline Analysis* Comparing Cost-Effectiveness of Different Strategies of Chemo-prophylaxis Against CMV in LiverTransplant Recipients
StrategyMean (CI†)
Cost ($)Mean (CI†)
Effectiveness (QAM)Mean (CI†)
C/E Ratio ($/QAM)Average Time Spent in the
CMV-Disease State (%)Annual CMV-Related
Mortality (%)
Strategy 1IV ganciclovir 58,933
(58,191-59,676)11.1079
(10.9586-11.2573)5,334
(5,255-5,375)0.66 0
Strategy 2Oral ganciclovir 53,165
(52,509-53,822)11.0987
(10.9529-11.2436)4,867
(4,828-4,906)3.32 0
Strategy 3CMV Ig 59,160
(58,225-60,095)11.0722
(10.9233-11.2212)5,472
(5,396-5,548)6.03 1
Strategy 4Acyclovir orally for 6 mo 55,243
(54,742-55,744)11.0694
(10.9227-11.2160)4,916
(4,844-5,039)5.76 1
Strategy 5Acyclovir orally for 3 mo 53,482
(52,351-54,613)10.9581
(10.8005-11.1156)4,851
(4,786-4,935)5.89 1
Abbreviation: QAM, quality-adjusted months.*Results from the second-order Monte Carlo simulation trial.†95% Confidence interval.
314 DAS HEPATOLOGY February 2000

was performed by simultaneously varying the probability ofsteroid-resistant rejection and proportion of the cohort withdonor positive, recipient-negative CMV-serological status,then also the strategy of oral ganciclovir administered to allpatients was the favored strategy over a wide area. Only whenthe proportion of patients with CMV status associated withthe highest risk of CMV disease comprised more than 90% ofthe cohort population, the strategy of intravenous ganciclovirrestricted to the high-risk groups was more cost-effective.
DISCUSSION
The incidence of CMV infection among patients whounderwent liver transplantation ranged from 23% to 85% andsymptomatic CMV disease developed in 15% to 40% of thesepatients.6 In addition to increased mortality, CMV disease isindependently associated with increased cost and longerlength of hospital stay in the first year after liver transplanta-tion.1,2 Although these facts underscore the importance ofeffective prophylaxis against CMV, no consensus exists on thebest prophylactic regimen in these patients. Although severalprophylactic regimens are in practice, it is almost impossibleto draw any inference on the comparative efficacy of theseregimens because of small number of controlled trials, vastdifference in study designs, and differences in subgroup riskstratification and immunosuppressive regimens used in thesestudies. Although preliminary comparative data tend tosupport the superiority of ganciclovir-based regimens interms of efficacy, no information exists on the cost-effectiveness of such a regimen. In fact, no cost-effectivenessanalysis using standard methodology has been performed toevaluate the overall cost-effectiveness of CMV prophylaxis inliver transplant recipients. Because liver transplantation is initself one of the costliest health care undertakings, anyadditional costly intervention in this setting should becost-effective by the standard of current healthcare interven-tions.
In the current decision analysis, using a Markov model,different commonly practiced prophylactic strategies werecompared in terms of cost and effectiveness in a hypotheticalcohort of liver transplant recipients. Of the various strategies,using oral ganciclovir administered universally to all trans-plant recipients had the best marginal cost-effectiveness ratio,acceptable by the standards of current health care interven-
tions.36 Although, the strategies using intravenous ganciclo-vir were more effective, the incremental cost-effectivenessratios for these strategies over those strategies using oralganciclovir were astronomically high. From the decisionanalysis it was apparent that by restricting acyclovir organciclovir-based CMV prophylaxis to a defined high-riskgroup markedly limits the effectiveness of such a strategy. Theincremental cost-effectiveness ratio of strategies in whichprophylaxis was administered to all transplant recipients overthose strategies where prophylaxis was restricted to only thehigh-risk groups was very modest (Table 4). Compared toganciclovir-based strategies, CMV Ig-based prophylaxis wasmore costly and less effective. Because of a lack of controlleddata in the setting of adult liver transplantation, CMV Igprophylaxis in combination with other antivirals was notconsidered in the current analysis. The conclusions of thisdecision analysis were unchanged over a broad range ofestimates of the clinical and cost variables; this is particularlytrue for those situations where definite data from controlledtrials were not available and assumptions were made based onexpert opinion.
Several limitations of this decision analysis exist. Onlydirect costs were considered in this model. Besides its directeffect, CMV may have a role in worsening the severity ofrecurrent hepatitis C disease in the transplanted liver.37 Thiswas not considered in the current decision analysis. Fewprophylactic regimens against CMV protect to a varyingextent against opportunistic infections with other herpesfamily viruses4,5 and such beneficial effect should ideally beconsidered in a cost-effectiveness analysis of such prophylac-tic regimens.
Preemptive therapy of CMV involves administration ofhighly effective antiviral therapy to a subgroup of patientsbefore appearance of disease as detected by sensitive markersof CMV viremia, viral shedding, or high-risk clinical determi-nants.3,11,38 Targeted preemptive therapy has recently at-tracted attention and is being used in few transplant centersacross the country because of its inherent advantages in termsof cost saving, low risk of emergence of resistant CMV strains,and minimal drug-related side effects. However, more con-trolled clinical and cost data in the setting of liver transplanta-tion are needed, particularly on the role of laboratory markerslike quantitative polymerase chain reaction (to assess viral
TABLE 4. Results of the Cost-Effective Analysis Comparing Strategies of Ganciclovir-Based Chemoprophylaxis Against CMV. Chemoprophylaxis IsEither Administered Universally to all Transplant Recipients or Restricted to Groups at High-Risk for CMV-Related Disease
StrategyMean (CI*)
Cost ($)Mean (CI*)
Effectiveness (QAM)Mean (CI*)
C/E Ratio ($/QAM)Incremental
C/E Ratio ($/QALY)
Ganciclovir1,000 mg orally 3 times a day for 100 days administered to high-risk†
patients only47,559
(46,987-47,876)8.5157
(8.4964-8.5235)5,569
(5,537-5,603)–
1,000 mg orally 3 times a day for 100 days administered to all patients 53,165(52,509-53,822)
11.0987(10.9529-11.2436)
4,867(4,828-4,906)
26,044
IV 6 mg/kg/d up to 30 days, then 5 mg/kg/d, 5 days in a week for atotal of 100 days to the high-risk† patients only
49,613(48,745-49,912)
8.5290(8.5073-8.5342)
5,791(5,743-5,847)
IV 6 mg/kg/d up to 30 days, then 5 mg/kg/d, 5 days in a week for atotal of 100 days to all patients
58,933(58,191-59,676)
11.1079(10.9586-11.2573)
5,334(5,255-5,375)
43,367
Abbreviations: QAM, quality-adjusted months; QALY, quality-adjusted life year.*95% Confidence interval.†High-risk patients who are seronegative recipients of liver transplant from seropositive donors and patients who develop steroid-resistant rejection and
receive treatment with antilymphocyte (OKT3) antibodies.
HEPATOLOGY Vol. 31, No. 2, 2000 DAS 315

load) in guiding preemptive therapy, before this strategy canbe realistically assessed in a comparative cost-effectivenessanalysis. In the current decision analysis, no extra cost ordysutility was considered because of side effects from prophy-lactic regimens. In controlled trials, most of the patients seemto tolerate the prolonged chemoprophylaxis without signifi-cant side effects.4,5 Based on available literature,39 quality oflife after liver transplantation was estimated as unity, al-though, arguably quality of life in the first posttransplanta-tion year may be lower than estimated. Also, estimates ofquality of life values used in the present analysis have notbeen validated in a population of transplant recipients,although sensitivity analyses performed using a wide range ofvalues for quality of life estimates did not alter the broadconclusions of the analysis. Emergence of resistant CMVstrains during prolonged prophylaxis remains a concern, butavailable data suggest that in the setting of liver transplanta-tion such occurrence is uncommon.40
In summary, within its limitations, this decision analysisestablishes the superiority of ganciclovir-based regimens, ingeneral, and the strategy of oral ganciclovir universallyadministered to all liver transplant recipients, in particular,for CMV prophylaxis from a point of cost-effectiveness. Thestrategy of targeted preemptive therapy is promising, andwell-designed controlled trials comparing this strategy withthat of oral ganciclovir-based prophylaxis are definitelywarranted.
REFERENCES
1. Falagas ME, Snydman DR, Griffith J, Ruthazer R, Werner BG, and theBoston Center for liver transplantation CMVIG study group. Effect ofcytomegalovirus infection status on first-year mortality rates amongorthotopic liver transplant recipients. Ann Intern Med 1997;126:275-279.
2. Falagas ME, Arbo M, Ruthazer R, Griffith J, Werner BG, Rohrer R,Freeman R, et al. Cytomegalovirus disease is associated with increasedcost and hospital length of stay among orthotopic liver transplantrecipients. Transplantation 1997;63:1595-1601.
3. Patel R, Snydman DR, Rubin RH, Ho M, Pescovitz M, Martin M, Paya CV.Cytomegalovirus prophylaxis in solid organ transplant recipients. Trans-plantation 1996;61:1279-1289.
4. Winston DJ, Wirin D, Shaked A, Busuttil. Randomised comparison ofganciclovir and high dose acyclovir for long-term cytomegalovirusprophylaxis in liver transplant recipients. Lancet 1995;346:69-74.
5. Gane E, Saliba F, Valdecasas GJC, O’Grady J, Pescovitz MD, Lyman S,Robinson CA. Randomised trial of efficacy and safety of oral ganciclovirin the prevention of cytomegalovirus disease in liver transplant recipi-ents. Lancet 1997;350:1729-1733.
6. Stratta RJ, Shaeffer MS, Markin RS, Wood RP, Langnas AN, Reed EC,Donovan JP, et al. Cytomegalovirus infection and disease after livertransplantation—an overview. Dig Dis Sci 1992;37:673-688.
7. Beck JR, Pauker SG. The Markov process in medical prognosis. MedDecis Making 1983;3:419-458.
8. Stratta RJ, Shaefer MS, Markin RS, Wood RP, Kennedy EM, Langnas AN,Reed EC, et al. Clinical patterns of cytomegalovirus disease after livertransplantation. Arch Surg 1989;124:1443-1450.
9. Wiesner RH, Marin E, Porayko MK, Steers JL, Krom RAF, Paya CV.Advances in the diagnosis, treatment, and prevention of cytomegalovirusinfections after liver transplantation. Gastroenterol Clin North Am1993;22:351-366.
10. Klintmalm GB, Nery JR, Husberg BS, Gonwa TA, Tillery GW. Rejectionin liver transplantation. HEPATOLOGY 1989;10:978-985.
11. Wiesner RH, Demetris J, Belle SH, Seaberg EC, Kalke JR, Zetterman RK,Everhart J, et al. Acute allograft rejection; incidence, risk factors, andimpact on outcome. HEPATOLOGY 1998;28:638-645.
12. Winston DJ, Imagwa DK, Holt CD, Kaldas F, Shaked A, Busuttil RW.Long-term ganciclovir prophylaxis eliminates serious cytomegalovirusdisease in liver transplant recipients receiving OKT3 therapy forrejection. Transplantation 1995;60:1357-1360.
13. Seu P, Winston DJ, Holt CD, Kaldas F, Busuttil W. Long-term ganciclovirprophylaxis for successful prevention of primary cytomegalovirus (CMV)disease in CMV-seronegative liver transplant recipients with CMV-seropositive donors. Transplantation 1997;64:1614-1617.
14. Snydman DR, Werner BG, Dougherty NN, Griffith J, Rubin RH, DienstagJL, Rohrer RH, et al. Cytomegalovirus immune globulin prophylaxis inliver transplantation—a randomized, double-blind, placebo-controlledtrial. Ann Intern Med 1993;119:984-991.
15. Singh N, Yu VL, Mieles L, Wagener MM, Miner RC, Gayowski T.High-dose acuclovir compared with short-course preemptive ganciclovirtherapy to prevent cytomegalovirus disease in liver transplant recipients-a randomized trial. Ann Intern Med 1994;120:375-381.
16. Martin M, Manez R, Linden P, Estores D, Torre-Cisneros J, Kusne S,Ondick L, et al. A prospective randomized trial comparing sequentialganciclovir-high dose acyclovir to high dose acyclovir for prevention ofcytomegalovirus disease in adult liver transplant recipients. Transplanta-tion 1994;58:779-785.
17. Kanj SS, Sharara AI, Clavien PA, Hamilton JD. Cytomegalovirus infec-tion following liver transplantation: review of the literature. Clin InfectDis 1996;22:537-549.
18. Sayers MH, Anderson KC, Goodnough LT, Kurtz SR, Lane TA, PisciottoP, Silberstein LE. Reducing the risk for transfusion-transmitted cytomega-lovirus infection. Ann Intern Med 1992;116:55-62.
19. Falagas ME, Paya C, Ruthazer R, Badley A, Patel R, Wiesner R, Griffith J,et al. Significance of cytomegalovirus for long-term survival afterorthotopic liver transplantation. A prospective derivation and validationcohort analysis. Transplantation 1998;66:1020-1028.
20. Klaus-Peter P, Mueller AR, Zytowski M, Lemmens P, Lobeck P, NeuhausP. Management of acute steroid-resistant rejection after liver transplanta-tion. World J Surg 1996;20:1052-1059.
21. Manez R, White LT, Linden P, Kusne S, Martin M, Kramer D, DemetrisAJ, et al. The influence of HLA matching on cytomegalovirus hepatitisand chronic rejection after liver transplantation. Transplantation 1993;55:1067-1071.
22. Lautensclager I, Hockerstedt K, Jalanko H, Loginov R, Salmela K,Taskinen E, Ahonen J. Persistent cytomegalovirus in liver allografts withchronic rejection. HEPATOLOGY 1997;25:190-194.
23. 1997 Center Specific Report. UNOS;DOT/HRSA/DHHS. htpp://www.unos.org/Data/.
24. Badley AD, Patel R, Portela DF, Harmsen WS, Smith TF, Ilstrup DM,Steers JL, et al. Prognostic significance and risk factors of untreatedcytomegalovirus viremia in liver transplant recipients. J Infect Dis1996;173:446-449.
25. George MJ, Snydman DR, Werner BG, Griffith J, Falagas ME, DoughertyNN, Rubin RH. The independent role of cytomegalovirus as a risk factorfor invasive fungal disease in orthotopic liver transplant recipients.Boston center for liver transplantation CMVIG-study group. Cytogam,Medimmune, Inc. Gaithersburg, Maryland. Am J Med 1997;103:106-113.
26. Van den Berg AP, Klompmaker IJ, Haagsma EB, Peeters PM, Meerman L,Verwer R, The TH, et al. Evidence for increased rate of bacterialinfections in liver transplant patients with cytomegalovirus infection.Clin Transplant 1993;10:224-231.
27. Paya CV, Wiesner RH, Hermans PE, Larson-Keller JJ, Ilstrup DM, KromRA, Retke S, et al. Risk factors for cytomegalovirus and severe bacterialinfections following liver transplantation: a prospective multivariatetime-dependent analysis. J Hepatol 1993;18:185-195.
28. de Otero J, Gavalda J, Murio E, Vargas V, Calico I, Llopart L, Rossello J, etal. Cytomegalovirus disease as a risk factor for graft loss and death afterorthotopic liver transplantation. Clin Infect Dis 1998;26:865-870.
29. Falagas ME, Snydman DR, Griffith J, Werner BG, Freeman R, Rohrer R,and the Boston Center for liver transplantation CMVIG study group.Clinical and epidemiological predictors of recurrent cytomegalovirusdisease in orthotopic liver transplant recipients. Clin Infect Dis 1997;25:314-317.
30. Geeverghese SK, Bradley AE, Wright K, Chapman WC, Feurer I, PayneJL, Hunter EB, et al. Outcomes analysis in 100 liver transplantationpatients. Am J Surg 1998;175:348-353.
31. Schulak JA, Ferguson RM, Hanto DW, Ryckman FC, Vogt DP, BohnengelA. Liver transplantation in Ohio. Surgery 1997;122:842-849.
32. Williams JW, Vera S, Evans LS. Socioeconomic aspects of hepatictransplantation. Am J Gastroenterol 1987;82:1115-1119.
33. Evans RW, Manninen DL, Dong FB. An economic analysis of livertransplantation. Costs, insurance coverage, and reimbursement. Gastro-enterol Clin North Am 1993;22:451-473.
316 DAS HEPATOLOGY February 2000

34. Paltiel AD, Scharfstein JA, Seage GR, Losina E, Goldie SJ, Weinstein MC,Craven DE, et al. A Monte Carlo simulation of advanced HIV disease:application to prevention of CMV infection. Med Decis Making 1998;18(Suppl):S93-S106.
35. Rose DN, Sacks HS. Cost-effectiveness of cytomegalovirus (CMV)disease prevention in patients with AIDS: oral ganciclovir and CMVpolymerase chain reaction testing. AIDS 1997;11:883-887.
36. Tengo TO, Adams ME, Pliskin JS, Safran DG, Siegel JE, Weinstein MC,Graham JD. Five-hundred life saving interventions and their cost-effectiveness. Risk Anal 1995;15:369-390.
37. Rosen HR, Chou S, Corless CL, Gretch DR, Flora KD, Boudousquie A,Orloff SL, et al. Cytomegalovirus viremia: risk factor for allograft
cirrhosis after liver transplantation for hepatitis C. Transplantation1997;64:721-726.
38. Mendez J, Epsy M, Smith TF, Wilson J, Wiesner R, Paya CV. Clinicalsignificance of viral load in the diagnosis of cytomegalovirus diseaseafter liver transplantation. Transplantation 1998;65:1477-1481.
39. Uchman SH, Cesar R. Yes, there is (quality of) life after liver transplanta-tion! HEPATOLOGY 1996;23:182-183.
40. Boivin G, Erice A, Crane DR, Dunn DL, Balfour HH. Ganciclovirsusceptibilities of cytomegalovirus (CMV) isolates from solid organtransplant recipients with CMV viremia after antiviral prophylaxis. JInfect Dis 1993;168:332-335.
HEPATOLOGY Vol. 31, No. 2, 2000 DAS 317