Cortical thickness analysis indicates a bipolar-ADHD...
1
C. Hegarty a , L.C. Foland-Ross b , K. L. Narr c , Y. Yang c , C. A. Sugar d,e , S. Y. Bookheimer a,e , J. McGough a,e , P.M. Thomp- son c , L.L. Altshuler a,e • Despite a relatively high prevalence of Attention-deficit/hyperactivity disorder (ADHD) in patients with Bi- polar Disorder (BP) 1 , few studies have addressed BP/ADHD comorbidity when interpreting MRI findings. • Recent studies of brain function and structure in BP and/or ADHD indicate that there are some abnormali- ties unique 2,3 to each disorder and some that overlap 4 , raising the question as to whether or not a combined (BP/ADHD) diagnosis is a subtype of either disorder. • Existing studies have proposed two models for the combined effect of BP and ADHD: (1) that the effects of the diagnosis are independent, so that the BP/ADHD comorbid group gets gets an additive impact of the two disorders 3 or (2) that there is an interaction whereby the effect of the combined diagnosis on brain structure is different from what would be expected based on the effects of the individual diagnoses. 4,5 • Using cortical pattern matching (CPM) registration procedures along with tools to measure cortical gray matter thickness, we sought to clarify the independent/overlapping contributions of BP and ADHD diagnoses to brain structure in comorbid BP/ADHD subjects. These methods improve upon traditional registration meth- ods by using sulcal landmarks to align corresponding anatomy across subjects. 6 • We hypothesized that the comorbid neural phenotype would reflect additive effects of ADHD and BP in some cortical regions, as well as an exacerbation of these effects in other regions. Given that the prefrontal cortex (PFC) and anterior cingulate cortex (ACC) are regions reported to be functionally 4,5,9 as well as structurally 3,7,8 abnormal in both BP and ADHD patients, we focused on these regions in our investigation of the ADHD impact on the BP neural phenotype. We fit a General Linear Model with a two by two Methods Cortical thickness analysis indicates a bipolar-ADHD interaction in comorbid adults Introduction • A total of 85 subjects were included in this study, consisting of 31 healthy controls (CON), 17 BP-only sub- jects, 19 ADHD-only subjects, and 18 BP/ADHD subjects. Subject groups did not differ significantly in age or gender distribution. • All subjects were scanned on a 1.5 Tesla (T) Siemens Sonata MRI scanner to obtain contiguous sagittal high-resolution three-dimensional magnetization-prepared rapid gradient echo (MPRAGE) T1-weighted images (160 slices; field of view=256mm; isotropic voxel size=1x1x1mm; TR/TE: 1900/4.38 ms). References Results from our interaction analyses, presented above in Figure 2, show: 1) In the right lateral orbitofrontal cortex (BA 47), BP was associated with corti- cal thinning in the absence of ADHD, while in the presence of ADHD there was no significant effect. (Figure 2b). 2) In subjects with ADHD, BP was associated with cortical thinning in the left subgenual cingulate (BA 25). There was no effect of BP in the absence of ADHD (Figure 2c). Results from our main effects analyses, presented below in Figure 3, show: 1) BP was associated with cortical thinning in bilateral PFC (BA10 and 11) and left ACC (BA 24 and 32), regardless of an ADHD comorbidity (Figure 3a). 2) ADHD was associated with both cortical thinning and thickening across brain regions. There were no main effects of ADHD in our a priori regions of interest (Figure 3b). a Semel Institute for Neuroscience and Human Behavior, University of California, Los Angeles b Stanford Mood and Anxiety Disorders Laboratory, Department of Psychology, Stanford University c Laboratory of Neuroimaging, Department of Neurology, University of California, Los Angeles d Department of Biostatistics, University of California, Los Angeles e Department of Psychiatry and Biobehavioral Sciences, David Geffen School of Medicine, University of California, Los Angeles Acknowledgments • The presence of ADHD significantly impacted the effect of bipolar disorder on cor- tical thickness, specifically in the right lateral orbital frontal cortex (BA 47) and left subgenual cingulate (BA 25). • Interactions were found in the anterior limbic circuit, which has been implicated in previous studies as a possible neurological basis for the characteristic emotional dysregulation associated with BP. Specifically, the cortical thinning in right BA 47 found in subjects with BP was not found in subjects with a combined BP/ADHD di- agnosis. • The magnitude and direction of the impact of ADHD on BP’s effect on cortical thickness was dependent upon the brain region in question. • These findings highlight the need for future studies of bipolar disorder to screen or control for ADHD comorbidity. 1. Wingo, A.P. and S.N. Ghaemi, A systematic review of rates and diagnostic validity of comorbid adult attention-deficit/hyperactivity disorder and bipolar disorder. J Clin Psychiatry, 2007. 68(11): p. 1776-84. 2. Brotman, M.A., et al., Amygdala activation during emotion processing of neutral faces in children with severe mood dysregulation versus ADHD or bipolar disorder. Am J Psychiatry. 167(1): p. 61-9. 3. Biederman, J., et al., Towards further understanding of the co-morbidity between attention deficit hyperactivity disorder and bipolar disorder: a MRI study of brain volumes. Psychol Med, 2008. 38(7): p. 1045-56. 4. Townsend, J., Sugar, C., Walshaw, P., Vasquez, R., Foland-Ross, L.C., Moody, T.D., Bookheimer, S.Y., McGough, J., Altshuler, L.L., Comorbid ADHD Impacts fMRI Findings in Bipolar Disorder During a Response Inhibition Task, Am J Psychiatry. 2010. Manuscript submitted for publication. 5. Adler, C.M., et al., Comorbid ADHD is associated with altered patterns of neuronal activation in adolescents with bipolar disorder performing a simple attention task. Bipolar Disord, 2005. 7(6): p. 577-88. 6. Thompson, P.M., et al., Mapping cortical change in Alzheimer's disease, brain development, and schizophrenia. Neuroimage, 2004. 23 Suppl 1: p. S2-18. 7. Foland-Ross, L.C., Thompson, P.M., Sugar, C., Madsen, S.K., Shen, J.K., Penfold, C., Ahlf, K., Rasser, P.E., Fischer, J., Yang, Y., Townsend, J., Bookheimer, S.Y., Altshuler, L.L., Investigation of Cortical Thickness Abnormalities in Lithium-Free Adults with Bipolar I Dis- order Using Cortical Pattern Matching, Am J Psychiatry. 2010. In Press. 8. Makris, N., et al., Cortical thinning of the attention and executive function networks in adults with attention-deficit/hyperactivity disorder. Cereb Cortex, 2007. 17(6): p. 1364-75. 9. Altshuler, L.L., et al., Blunted activation in orbitofrontal cortex during mania: a functional magnetic resonance imaging study. Biol Psychiatry, 2005. 58(10): p. 763-9. The authors would like to thank the Furlotti Family Foundation, the Swift Foundation, and the Na- tional Institute of Mental Health (K24MH001848 (LLA), R01MH084955 (LLA), R21MH075944 (LLA)) for their financial support of this research. The authors also wish to acknowledge the support of the staff at the UCLA Mood Disorders Research Program, Brain Mapping Medical Research Organiation, Brain Mapping Support Foundation, and the Pierson-Lovelace Foundation. Poster #247 Results Discussion Figure 2 (above): a) Significance maps show the interaction of ADHD and BP on cortical thickness . Average corti- cal thickness values (adjusted for age and sex) in b) right BA 47 and c) left BA 25. b) Figure 3 (above): Significance maps showing the main effect of a) BP and b) ADHD on cortical thickness. Negative p values indicate regions associated with cortical thinning.; positive p values indicate regions associated with in- creased cortical thickness. c & d) Significance maps showing post-hoc pairwise comparisons of c) BP-only vs. con- trols and d) BP/ADHD vs. ADHD-only. c) b) * Indicates significant differences (p<0.05) in cortical thickness between groups ‡ Indicates trend level differences (p<0.10) in cortical thickness between groups Figure 1. Outline of techniques used in preprocessing, cortical pattern matching, and statistical interpreta- tion of cortical thickness at each surface point 6 . • We fit a General Linear Model with a two by two design (BP diagnosis, ADHD diagnosis and their interac- tion) at each cortical surface point, adjusted for age and gender, to produce p-maps of the joint effects of the disorders. • We performed permutation analyses across brain regions to localize interaction effects in our a priori re- gions of interest (PFC and ACC), as well as other regions which were treated as exploratory. We then plotted the average cortical thickness in regions reflecting a significant interaction to detrmine the direction of the inter- actions. Table 1. Subject Demographics
Transcript of Cortical thickness analysis indicates a bipolar-ADHD...
C. Hegartya, L.C. Foland-Rossb, K. L. Narrc, Y. Yangc, C. A. Sugard,e, S. Y. Bookheimera,e, J. McGougha,e, P.M. Thomp-sonc, L.L. Altshulera,e
• Despite a relatively high prevalence of Attention-deficit/hyperactivity disorder (ADHD) in patients with Bi-polar Disorder (BP)1, few studies have addressed BP/ADHD comorbidity when interpreting MRI findings.
• Recent studies of brain function and structure in BP and/or ADHD indicate that there are some abnormali-ties unique2,3 to each disorder and some that overlap4 , raising the question as to whether or not a combined (BP/ADHD) diagnosis is a subtype of either disorder.
• Existing studies have proposed two models for the combined effect of BP and ADHD: (1) that the effects of the diagnosis are independent, so that the BP/ADHD comorbid group gets gets an additive impact of the two disorders3 or (2) that there is an interaction whereby the effect of the combined diagnosis on brain structure is different from what would be expected based on the effects of the individual diagnoses.4,5
• Using cortical pattern matching (CPM) registration procedures along with tools to measure cortical gray matter thickness, we sought to clarify the independent/overlapping contributions of BP and ADHD diagnoses to brain structure in comorbid BP/ADHD subjects. These methods improve upon traditional registration meth-ods by using sulcal landmarks to align corresponding anatomy across subjects.6
• We hypothesized that the comorbid neural phenotype would reflect additive effects of ADHD and BP in some cortical regions, as well as an exacerbation of these effects in other regions. Given that the prefrontal cortex (PFC) and anterior cingulate cortex (ACC) are regions reported to be functionally 4,5,9 as well as structurally3,7,8 abnormal in both BP and ADHD patients, we focused on these regions in our investigation of the ADHD impact on the BP neural phenotype. We fit a General Linear Model with a two by two
Methods
Cortical thickness analysis indicates a bipolar-ADHD interaction in comorbid adults
Introduction
• A total of 85 subjects were included in this study, consisting of 31 healthy controls (CON), 17 BP-only sub-jects, 19 ADHD-only subjects, and 18 BP/ADHD subjects. Subject groups did not differ significantly in age or gender distribution.
• All subjects were scanned on a 1.5 Tesla (T) Siemens Sonata MRI scanner to obtain contiguous sagittal high-resolution three-dimensional magnetization-prepared rapid gradient echo (MPRAGE) T1-weighted images (160 slices; field of view=256mm; isotropic voxel size=1x1x1mm; TR/TE: 1900/4.38 ms).
References
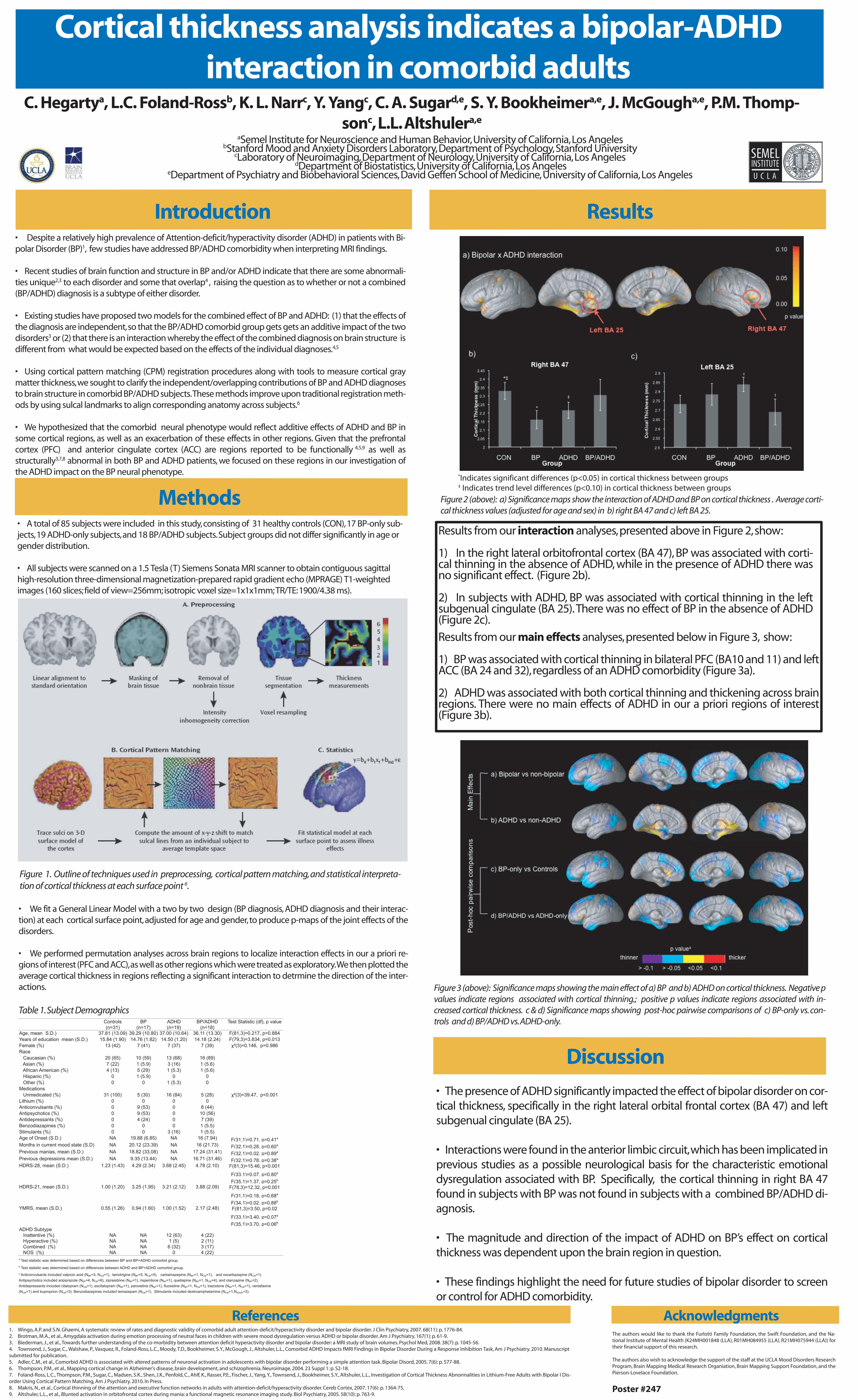
Results from our interaction analyses, presented above in Figure 2, show: 1) In the right lateral orbitofrontal cortex (BA 47), BP was associated with corti-cal thinning in the absence of ADHD, while in the presence of ADHD there was no significant effect. (Figure 2b). 2) In subjects with ADHD, BP was associated with cortical thinning in the left subgenual cingulate (BA 25). There was no effect of BP in the absence of ADHD (Figure 2c).
Results from our main effects analyses, presented below in Figure 3, show:
1) BP was associated with cortical thinning in bilateral PFC (BA10 and 11) and left ACC (BA 24 and 32), regardless of an ADHD comorbidity (Figure 3a).
2) ADHD was associated with both cortical thinning and thickening across brain regions. There were no main effects of ADHD in our a priori regions of interest (Figure 3b).
aSemel Institute for Neuroscience and Human Behavior, University of California, Los AngelesbStanford Mood and Anxiety Disorders Laboratory, Department of Psychology, Stanford University
cLaboratory of Neuroimaging, Department of Neurology, University of California, Los AngelesdDepartment of Biostatistics, University of California, Los Angeles
eDepartment of Psychiatry and Biobehavioral Sciences, David Geffen School of Medicine, University of California, Los Angeles
Acknowledgments
• The presence of ADHD significantly impacted the effect of bipolar disorder on cor-tical thickness, specifically in the right lateral orbital frontal cortex (BA 47) and left subgenual cingulate (BA 25).
• Interactions were found in the anterior limbic circuit, which has been implicated in previous studies as a possible neurological basis for the characteristic emotional dysregulation associated with BP. Specifically, the cortical thinning in right BA 47 found in subjects with BP was not found in subjects with a combined BP/ADHD di-agnosis.
• The magnitude and direction of the impact of ADHD on BP’s effect on cortical thickness was dependent upon the brain region in question.
• These findings highlight the need for future studies of bipolar disorder to screen or control for ADHD comorbidity.
1. Wingo, A.P. and S.N. Ghaemi, A systematic review of rates and diagnostic validity of comorbid adult attention-deficit/hyperactivity disorder and bipolar disorder. J Clin Psychiatry, 2007. 68(11): p. 1776-84.2. Brotman, M.A., et al., Amygdala activation during emotion processing of neutral faces in children with severe mood dysregulation versus ADHD or bipolar disorder. Am J Psychiatry. 167(1): p. 61-9.3. Biederman, J., et al., Towards further understanding of the co-morbidity between attention deficit hyperactivity disorder and bipolar disorder: a MRI study of brain volumes. Psychol Med, 2008. 38(7): p. 1045-56.4. Townsend, J., Sugar, C., Walshaw, P., Vasquez, R., Foland-Ross, L.C., Moody, T.D., Bookheimer, S.Y., McGough, J., Altshuler, L.L., Comorbid ADHD Impacts fMRI Findings in Bipolar Disorder During a Response Inhibition Task, Am J Psychiatry. 2010. Manuscript submitted for publication.5. Adler, C.M., et al., Comorbid ADHD is associated with altered patterns of neuronal activation in adolescents with bipolar disorder performing a simple attention task. Bipolar Disord, 2005. 7(6): p. 577-88.6. Thompson, P.M., et al., Mapping cortical change in Alzheimer's disease, brain development, and schizophrenia. Neuroimage, 2004. 23 Suppl 1: p. S2-18.7. Foland-Ross, L.C., Thompson, P.M., Sugar, C., Madsen, S.K., Shen, J.K., Penfold, C., Ahlf, K., Rasser, P.E., Fischer, J., Yang, Y., Townsend, J., Bookheimer, S.Y., Altshuler, L.L., Investigation of Cortical Thickness Abnormalities in Lithium-Free Adults with Bipolar I Dis-order Using Cortical Pattern Matching, Am J Psychiatry. 2010. In Press.8. Makris, N., et al., Cortical thinning of the attention and executive function networks in adults with attention-deficit/hyperactivity disorder. Cereb Cortex, 2007. 17(6): p. 1364-75.9. Altshuler, L.L., et al., Blunted activation in orbitofrontal cortex during mania: a functional magnetic resonance imaging study. Biol Psychiatry, 2005. 58(10): p. 763-9.
The authors would like to thank the Furlotti Family Foundation, the Swift Foundation, and the Na-tional Institute of Mental Health (K24MH001848 (LLA), R01MH084955 (LLA), R21MH075944 (LLA)) for their financial support of this research.
The authors also wish to acknowledge the support of the staff at the UCLA Mood Disorders Research Program, Brain Mapping Medical Research Organiation, Brain Mapping Support Foundation, and the Pierson-Lovelace Foundation.
Poster #247
Results
Discussion
Figure 2 (above): a) Significance maps show the interaction of ADHD and BP on cortical thickness . Average corti-cal thickness values (adjusted for age and sex) in b) right BA 47 and c) left BA 25.
b)
Figure 3 (above): Significance maps showing the main effect of a) BP and b) ADHD on cortical thickness. Negative p values indicate regions associated with cortical thinning.; positive p values indicate regions associated with in-creased cortical thickness. c & d) Significance maps showing post-hoc pairwise comparisons of c) BP-only vs. con-trols and d) BP/ADHD vs. ADHD-only.
c) b)
*Indicates significant differences (p<0.05) in cortical thickness between groups‡ Indicates trend level differences (p<0.10) in cortical thickness between groups
Figure 1. Outline of techniques used in preprocessing, cortical pattern matching, and statistical interpreta-tion of cortical thickness at each surface point 6.
• We fit a General Linear Model with a two by two design (BP diagnosis, ADHD diagnosis and their interac-tion) at each cortical surface point, adjusted for age and gender, to produce p-maps of the joint effects of the disorders. • We performed permutation analyses across brain regions to localize interaction effects in our a priori re-gions of interest (PFC and ACC), as well as other regions which were treated as exploratory. We then plotted the average cortical thickness in regions reflecting a significant interaction to detrmine the direction of the inter-actions.
Table 1. Subject Demographics








![arXiv:1406.5197v1 [q-bio.NC] 19 Jun 2014 · lability is greatest in rostral middle frontal, lateral orbitofrontal, frontal pole, medial orbitofrontal, superior frontal, and anterior](https://static.fdocuments.us/doc/165x107/5e032dbfd9e2ea2f20421fca/arxiv14065197v1-q-bionc-19-jun-2014-lability-is-greatest-in-rostral-middle.jpg)