Correlative201T1SPECT,MRIandExVivo201T1...
7
Key Words:SPECT; @°1Tl chloride; MRI; neckmetastases; squamouscell carcinoma JNucIMed1999;40:1414—1419 he assessment of cervical lymph node metastases in patients with squamous cell carcinoma of the head and neck is essential for the clinical management of the disease. Staging of the neck, which constitutes a diagnostic problem because of the large number of lymph nodes located in this area (1), determines the extent of treatment modalities such as surgery or radiotherapy. In addition to palpation, staging of the neck increasingly relies on imaging modalities such as CT and MRI that use lymph node size and central lucency as criteria for detection of metastatic disease (2—4). Although lymph nodes 10 mm in diameter are generally considered tobepositive(5), lymphnodeenlargement mayalsobethe result of reactive and inflammatory processes that may limit the accuracy of CT and MRJ. Moreover, detection of micro metastases in small nodes still remains a difficult issue (6,7). To overcome these limitations, ultrasound-guided fine needle aspiration cytology (USG-FNAC) was introduced in recent years. By combining detection by sonography with tissue characterization by microscopy (8,9), this technique has reached high accuracy levels in the diagnosis of regional spread in clinically negative necks and necks with lymphad enopathies. However, the accuracy of USG-FNAC depends on the skill of the sonographer and the cytopathologist, and the technique requires multiple aspirations. As an alternative modality, PET has been used for the staging of the neck. 18F-fluorodeoxyglucose (FDG) is able to detect metastases measuring 4 mm or more, but the relatively high false positive rate caused by uptake in reactive lymph nodes (10) has led to the use of other compounds, such as L-[―CH3]- methionine (11) and L-1-[―C]-tyrosine (12,13), that appear to be more accurate in differentiating cancerous from inflammatory cells. The value of SPECTwith @°1TI chloride, in combinationwith MRI (particularly short inversion-time inversion recovery [STIRI Se quences that suppress fat signals) to detect and characterize cervicalymphadenopathies (nodes @ 1cm),andexvivolymph node @°1Tl uptakewerestudiedin patientswithsquamouscell carcinomaofthe headand neck. Methods: PreoperativeSPECT and MRI, displayed in similar planes, were compared with the histologicfindingsin 15 neckdissectionspecimensfrom 12 patients with squamous cell carcinoma of the head and neck (9 with unilateraland 3 with bilateral neck dissection).Resultswere evaluatedtopographicallywith regardtothe lymphnodecompart ments (levels) of the neck. In addition, in 8 of these patients,the 20111 activity of dissected lymph nodes of 10 neck sides was measured immediately after surgery in a gamma counter and expressed as percentage of the injected dose per gram tissue (%lO/g). Resufts: Sixty-two lymph node levels were evaluated histologically. Thehighsensitivityof MRI(92%versus71%for @°1TI SPECT),whichcorrectlydetected lymphnodeinvolvement in 22of 24 levels,andthehighspecificityof @°1TI SPECT(92% versus 71% for MRI), which correctly characterizedas negative 35 of 38 lymph node levelswithout metastasison histology,led to acombined20111 SPECT/MRI accuracyof92%. @°1Tl SPECTwas particularly effective in excluding involvement in 9 tumor-free necklevelswithpathologically enlarged lymphnodesonMRIbut failed to confirminvolvement in 5 othertumor-positive levels. Mean 20111 uptake in 53 lymph nodes with confirmed histologic involvement was significantly higher than uptake in 145 tumor free lymph nodes (0.0043 ±0.0022 %lD/g versus 0.0023 ± 0.0014 %IO/g, P = 0.0001), muscle and fat tissue but clearly lower than salivary gland uptake. Conclusion: Although @°@Tl SPECT is not sensitive enough to be used as an independent imagingmodalityforstagingoftheneck,itscorrelativeapplica tion with MRI appears to be an accurate method for the assessmentof regional spread in head and neck squamouscell carcinoma. The ability of @°1Tl SPECT to characterize neck lymphadenopathiesdetectedby MRI appearsto be basedon the difference in @°1TI concentrationfound in lymph nodes with and withouttumor involvement. ReceivedJul.22,1998;revisionacceptedMar.5,1999. For correspondence or reprints contact: Renato A. ValdésOlmos, MD, Department ofNuclear Medicine, TheNetherlands Cancer InstItute, Plesman laan 121, 1066 CX Amsterdam, The Netherlands. 1414 THEJOURNAL OFNUCLEAR MEDICINE • Vol. 40 • No. 9 • September1999 Correlative 201T1SPECT, MRI andEx Vivo 201T1 Uptake in Detecting and Characterizing Cervical Lymphadenopathy in Head and Neck Squamous Cell Carcinoma Renato A.Valdés Olmos, Wim Koops, Barbara M. Loftus, lug H. Liem, Reinhold T. Gregor, Cornelis A. Hoefnagel, Frans J. M. Hilgers and Alfons J. M. Balm Departments ofNuclear Medicine, Diagnostic Radiology, Pathology and Otolaryngology/Head and Neck Surgery, The Netherlands Cancer Institute, Amsterdam, The Netherlands by on July 2, 2018. For personal use only. jnm.snmjournals.org Downloaded from
Transcript of Correlative201T1SPECT,MRIandExVivo201T1...

Key Words:SPECT; @°1Tlchloride;MRI; neckmetastases;squamouscell carcinoma
J NucIMed1999;40:1414—1419
he assessment of cervical lymph node metastases inpatients with squamous cell carcinoma of the head and neckis essential for the clinical management of the disease.
Staging of the neck, which constitutes a diagnostic problembecause of the large number of lymph nodes located in thisarea (1), determines the extent of treatment modalities suchas surgery or radiotherapy. In addition to palpation, stagingof the neck increasingly relies on imaging modalities such asCT and MRI that use lymph node size and central lucency ascriteria for detection of metastatic disease (2—4).Althoughlymph nodes 10 mm in diameter are generally consideredtobepositive(5), lymphnodeenlargementmayalsobetheresult of reactive and inflammatory processes that may limitthe accuracy of CT and MRJ. Moreover, detection of micrometastases in small nodes still remains a difficult issue (6,7).
To overcome these limitations, ultrasound-guided fineneedle aspiration cytology (USG-FNAC) was introduced inrecent years. By combining detection by sonography withtissue characterization by microscopy (8,9), this techniquehas reached high accuracy levels in the diagnosis of regionalspread in clinically negative necks and necks with lymphadenopathies. However, the accuracy of USG-FNAC dependson the skill of the sonographer and the cytopathologist, andthe technique requires multiple aspirations. As an alternativemodality, PET has been used for the staging of the neck.18F-fluorodeoxyglucose (FDG) is able to detect metastasesmeasuring 4 mm or more, but the relatively high falsepositive rate caused by uptake in reactive lymph nodes (10)has led to the use of other compounds, such as L-[―CH3]-methionine (11) and L-1-[―C]-tyrosine (12,13), that appear
to be more accurate in differentiating cancerous frominflammatory cells.
The value of SPECTwith @°1TIchloride, in combinationwith MRI(particularly short inversion-time inversion recovery [STIRI Sequences that suppress fat signals) to detect and characterizecervicallymphadenopathies(nodes@ 1cm),andexvivolymphnode @°1Tluptakewerestudiedin patientswithsquamouscellcarcinomaofthe headand neck.Methods: PreoperativeSPECTand MRI, displayed in similar planes, were compared with thehistologicfindingsin 15 neck dissectionspecimensfrom 12patients with squamous cell carcinoma of the head and neck (9with unilateraland 3 with bilateralneckdissection).Resultswereevaluatedtopographicallywith regardtothe lymphnodecompartments (levels)of the neck. In addition, in 8 of these patients,the20111 activity of dissected lymph nodes of 1 0 neck sides was
measured immediately after surgery in a gamma counter andexpressed as percentageof the injected dose per gram tissue(%lO/g). Resufts: Sixty-two lymph node levels were evaluatedhistologically.Thehighsensitivityof MRI(92%versus71% for@°1TISPECT),whichcorrectlydetectedlymphnodeinvolvementin 22of 24 levels,andthe highspecificityof @°1TISPECT(92%versus 71% for MRI), which correctly characterizedas negative35 of 38 lymphnodelevelswithoutmetastasison histology,ledtoacombined20111SPECT/MRIaccuracyof92%. @°1TlSPECTwasparticularly effective in excluding involvement in 9 tumor-freenecklevelswithpathologicallyenlargedlymphnodesonMRIbutfailedto confirminvolvementin 5 othertumor-positivelevels.Mean 20111uptake in 53 lymph nodes with confirmed histologicinvolvementwas significantly higher than uptake in 145 tumorfree lymph nodes (0.0043 ±0.0022 %lD/g versus 0.0023 ±0.0014 %IO/g, P = 0.0001), muscle and fat tissue but clearlylower than salivary gland uptake. Conclusion: Although @°@TlSPECT is not sensitive enough to be used as an independentimagingmodalityfor stagingof the neck,itscorrelativeapplication with MRI appears to be an accurate method for theassessmentof regionalspread in head and neck squamouscellcarcinoma. The ability of @°1TlSPECT to characterize necklymphadenopathiesdetectedby MRIappearsto be basedon thedifference in @°1TIconcentrationfound in lymph nodes with andwithouttumorinvolvement.
ReceivedJul.22,1998;revisionacceptedMar.5, 1999.For correspondence or reprints contact: Renato A. ValdésOlmos, MD,
DepartmentofNuclearMedicine,TheNetherlandsCancerInstItute,Plesmanlaan 121, 1066 CX Amsterdam, The Netherlands.
1414 THEJOURNALOFNUCLEARMEDICINE•Vol. 40 •No. 9 •September1999
Correlative 201T1SPECT, MRI and Ex Vivo 201T1Uptake in Detecting and Characterizing CervicalLymphadenopathy in Head and Neck SquamousCell CarcinomaRenato A.ValdésOlmos, Wim Koops, Barbara M. Loftus, lug H. Liem, Reinhold T. Gregor, Cornelis A. Hoefnagel,Frans J. M. Hilgers and Alfons J. M. Balm
Departments ofNuclear Medicine, Diagnostic Radiology, Pathology and Otolaryngology/Head and Neck Surgery, The NetherlandsCancer Institute, Amsterdam, The Netherlands
by on July 2, 2018. For personal use only. jnm.snmjournals.org Downloaded from

-Patientno.SexAge(y)Tumorlocation(staging)Neckdissection(&de)HistologyA/L@°1TlSPECTA/LMRIA/L+ + +
The effectiveness of SPECT with @-°‘Tl-chlorideto exdude neck lymph node involvement in patients with varioushead and neck malignancies in a previous study (14) led usto test the method in the characterization of cervicallymphadenopathies already detected by MRI in patientswith head and neck squamous cell carcinoma to ascertain itsvalue in staging the neck. In the previous study, the accuracyof 201Tl SPECT was determined only on the basis of datarecorded per dissected neck side. However, this studyincludes a topographical analysis considering six neck levelsper neck side to complete the evaluation ofthe test in stagingthe neck. Finally, on the basis of correlative ex vivo lymphnode 201T1uptake measurements and histologic findings, thisstudy evaluates differences in lymph nodes with and withouttumor involvement.
MATERIALSAND METHODS
PatientsTwelve consecutive patients (6 men, 6 women; age range 44—73
y; mean age 61.8 y) with histologically confirmed head and necksquamous cell carcinoma, scheduled for neck dissection, wereincluded in the study after having provided informed consent.Clinical assessment was performed by the head and neck surgeon;subsequently, patients underwent MRI and @°1TlSPECT. In 8patients, 201T1-chloridewas administered on the day of surgery toenable cx vivo lymph node counting after neck dissection andcomparison with histologic findings. Classification of the primarytumor and neck lymph nodes was based on the TNM system of theUnion Internationale Contre le Cancer (UICC, 1992). Clinical dataof patients are summarized in Table 1. Neck dissection wasunilateral in 9 patients and bilateral in 3 patients, which resulted ina total of 15 evaluated neck sides.
20111ImagingSPECT acquisition was performed according to a standardized
method of fixation to prevent head movements and to obtain aposition similar to MRI. SPECT studies were performed with a
Vertex dual-head gamma camera (ADAC, Milpitas, CA) equippedwith low-energy, high-resolution collimators 60 mm after intravenous injection of 150 MBq (4 mCi) 201Tl-chloride.Acquisition wasbased on 360°noncircular rotation, 6°step angles, 60 s per frame,64X 64X 16matrixandazoomfactorof1.85(pixelsize5mm).Reconstruction was performed with Butterworth filter (order 5,cutoff 0.35); reorientation of images was performed followingplanes similar to the MR images, with saginal, coronal andtransverse one-pixel slices and additional three-dimensional volume reconstruction to identify tumor sites with exact documentation of the region and neck level.
MRIMR images (Tl- and T2-weighted pulse sequences with trans
axial and sagittal slices of 3- to 5-mm thickness, field of view200—250cm, 256 X 256 matrix) were obtained with a SiemensMagnetom 63 SP4000 (Erlangen, Germany) l.5-T scanner beforeand after intravenous administration of gadolinium diethylenetriaminepentaacetic acid. In addition, coronal short inversion-timeinversion recovery (STIR) sequences, which suppress fat signals,were obtained with a slice thickness of 5 mm.
HistologicPreparationandExVivo @1TlLymphNodeUptakeMeasurements
After neck dissection lymph nodes and normal tissues wereprepared by the pathologist, and lymph nodes per neck level wereprecisely localized in the specimen. Subsequently, after meticulousexcision from the specimen, all lymph nodes received identificationlabels. For cx vivo 201'fluptake measurements, lymph nodes andnormal tissues were placed in single well-identified counting tubesand were weighed and measured in a gamma well counter. Datawere corrected for decay and converted to percentage of theinjected dose per gram tissue (%ID/g). After counting, lymphnodes were fixed, sectioned and stained routinely with hematoxylinand eosin. Multiple levels were examined microscopically for thepresence of tumor.
AnalysisSensitivity, specificity and accuracy were calculated for each
imaging modality and for the combination of both methods. MR
TABLE1Patient Characteristics, Tumor/Treatment Data, Histology and Imaging Results per Neck Side
+++++++/++1++1+—+—1M56Oropharynx (recurrence)AND(A)2F73Oropharynx
(T3N2b)RND(A)3M59Oropharynx(T3N2)AND(A)4F67Larynx
(T2N2c)AND(A/L)5F72Esophagus(tonguemetastasis)SOND(A)6M61Oropharynx(T2N3)AND(A)+++7M44MaxillaSOND
(A)ANO(L)+ ++ +++8F60Oropharynx
(T3NO)AND(A)——+9F60Larynx(T3N2)MRND (A)
AND(L)— +— +++10F59Hypopharynx(T3NI)MRND(A)+++11M59Oropharynx
(T2N2)MAND(L)+++12M63Larynx(T3NO)AND (A)++
AND = radicalneckdissection;+ = positive;SONO= supraomohyoidneckdissection;—= negative;MRND= modifiedradicalneckdissection.
20l'fl@ SPECT AND MRI mi NECK METASTASES •Valdés Olmos et al. 1415
by on July 2, 2018. For personal use only. jnm.snmjournals.org Downloaded from

as with normal tissue, were analyzed with a Wilcoxon signed-ranktest for equality of medians (2-tailed).
RESULTS201TISPECTandMRI
Histology demonstrated lymph node involvement in I 1neck sides and was negative in 4; both SPECT and MRIwere positive in all neck sides with lymph node metastases(Fig. 2). 201'fl SPECT was correctly negative in 2 neck sides
without lymph node involvement and MRI in 1. Falsepositives were two for 201Tl SPECT and three for MRI.Accuracy per side was 87% for 201'fl SPECT and 80% forMRI. Modalities used for neck dissection and outcome perside of the neck are given in Table 1.
Sixty-two neck levels were histologically evaluated, and
lymph nodes with tumor involvement were found in 24levels. 201'fl SPECT correctly identified metastases in 17levels (sensitivity 71%) and was true-negative in 35 levels(specificity 92%), leading to an accuracy of 84%. MRI wastrue-positive in 22 levels (sensitivity 92%) and true-negative in27 (specificity 71%) with an accuracy of 79%.
When MRI and 201'flSPECT were analyzed together,overall sensitivity was 92%, specificity was 92% andaccuracy was 92%. In the combined evaluation, 201'flSPECT was particularly effective in excluding involvementin 9 tumor-free neck levels with lymph nodes 10 mm onMRI STIR (Figs. 3 and 4); this included 2 level II, 4 level IIIand 3 level IV. Inversely, 201fl SPECT failed in confirminginvolvement in 1 lymph node with necrotic changes in levelIn and in another 4 (2 level IV, 2 level V) without irregularenhancement on MRI (Fig. 5). 201TlSPECT and MRI STIRwere both false-negative in 2 levels with lymph nodeinvolvement and were both false-positive in 2 levels withoutinvolvement; in 1 level without involvement, only 201'flSPECT was false-positive. Table 2 displays the findings ofhistology, SPECT and MRI STIR per neck level.
ExVivo @1TILymphNodeUptakeMeasurementsThe ex vivo 201T1uptake was calculated in dissected
lymph nodes of 10 neck sides in 8 patients. A total of 198lymph nodes were histogically prepared and analyzed.Metastatic involvement was found in 53 lymph nodes (range0.03—22.74g, meanweight 2.796 g); 145 lymph nodes(range 0.02—1.7g, mean weight 0.274 g) were free of tumor.Mean 201'fluptake in metastatic lymph nodes (0.0043 ±
FIGURE 1. Lymph nodegroupsdividedinto six levelsper neck side according toRobbins et al. (15). Level Iincludes submental and submaxillarynodes;levelsII/III/IV,jugular chain nodes; and levelv,lymphnodeslocalizedposteriorly to posterior border ofsternocleidomastoid muscle.Level VI includesjuxtaviscerallymphnodes.
and SPECT images were independently evaluated by two specialisis in head and neck radiology and nuclear medicine. Examinerswere unaware of the results of histology. Concerning SPECT,tumor uptake, visually assessed using a four-step score takingbackground activity of the neck as reference, was scored as intense(+ +), moderate(+), weaklypositive(±)or absent(—);onlyintense and moderate were considered conclusive for pathology.With respect to MRI, on Tl- and T2-weighted pulse sequences,lymph nodes with a diameter 10 mm and nodes that showedirregular enhancement and that were surrounded by a rim ofenhancing viable tumor or lymph node tissue were classified aspositive, according to well-established criteria (5); on coronal STIRsequences only lymph node size 10mm was used as a pathologiccriterion. For topographical evaluation, the findings of SPECT andMRI were recorded according to a standardized classification (15)that divideseach neck side into six levels(Fig. 1).Subsequently,resultswere correlated with histologic findings for every neck level.
The additional value of 201T1SPECT in the characterization ofenlarged lymph nodes detected by MRI STIR was evaluated bycorrelative analysis in joint panel sessions that included anotolaryngologist/head and neck surgeon, a head and neck radiologist and a nuclear medicine specialist. An enlarged lymph node onMRI STIR with no @°‘T1uptake on SPECT was considerednegative; if necessary a consensus was reached. SPECT coronalimages and coronal MRI STIR sequences were displayed onsimilar planes. To correct for small differences in the slice thicknessofSPECT and MR.!STIR.theevaluationwasperformedon thebasisofcorrespondingsets of images according to anatomic reference pointsfrom MRI.
Concerning cx vivo measurements, differences in 2OVfluptakebetween lymph nodes with and without tumor involvement, as well
A C
FIGURE2. (A) CoronalMRI STIR Sequence shows enlarged lymph nodes inboth neck sides (arrows) with intense uptake (arrows)oncorresponding @°@TISPECTimage (B) in neck levels II and III of patientwithsupraglotticlarynxcarcinoma,asshown(arrow) on transaxial SPECT image (C),and histologicallyconfirmedbilateralmetastases.
1416 THEJOURNALOFNUCLEARMEDICINE•Vol. 40 •No. 9 •September1999
by on July 2, 2018. For personal use only. jnm.snmjournals.org Downloaded from
C
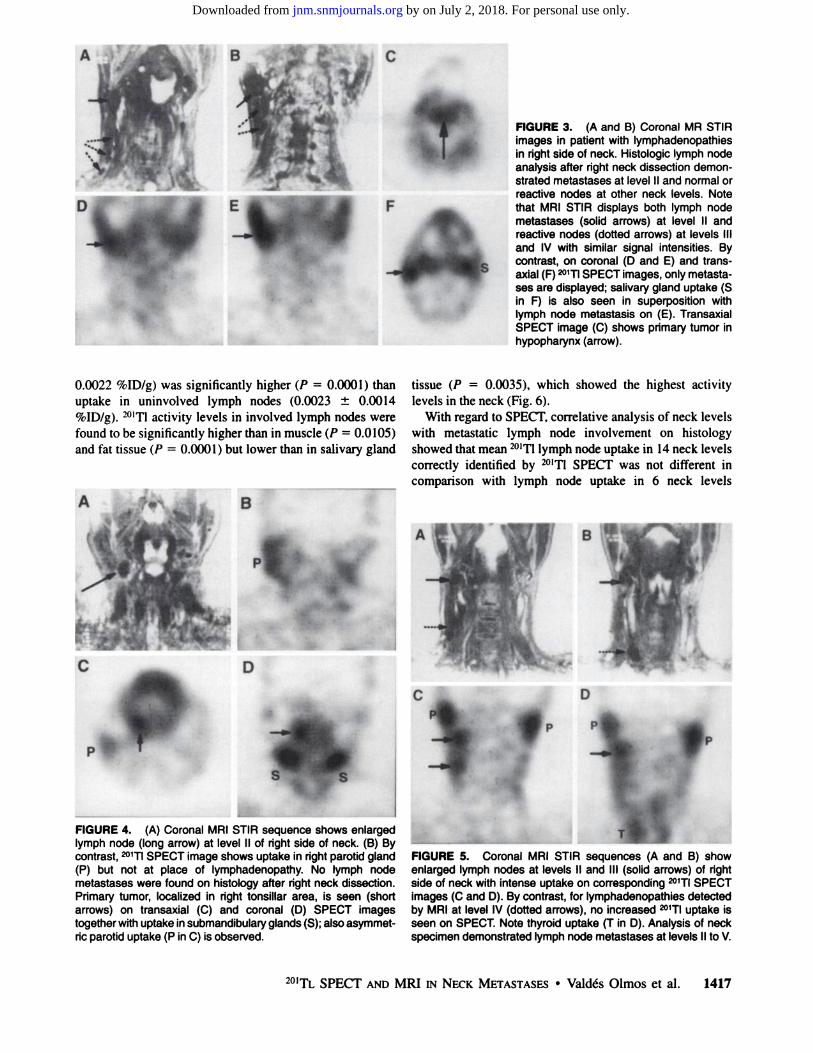
FIGURE3. (AandB)CoronalMRSTIRimages in patient with lymphadenopathiesin right side of neck. Histologic lymph nodeanalysis after right neck dissectiondemonstrated metastasesat level II and normalorreactive nodes at other neck levels. Notethat MRI STIR displays both lymph nodemetastases (solid arrows) at level II andreactive nodes (dotted arrows) at levels IIIand IV with similar signal intensities. Bycontrast, on coronal (D and E) and transaxial(F) @°1TlSPECTimages,onlymetastases are displayed;salivary gland uptake (Sin F) is also seen in superposition withlymph node metastasis on (E). TransaxialSPECT image (C) shows primary tumor inhypopharynx(arrow).
F
tissue (P = 0.0035), which showed the highest activitylevels in the neck (Fig. 6).
With regard to SPECT, correlative analysis of neck levelswith metastatic lymph node involvement on histologyshowed that mean 201'fllymph node uptake in 14 neck levelscorrectly identified by 201TI SPECT was not different in@—comparisonwithlymphnodeuptakein6necklevels
—@ @- __
FIGURE5. CoronalMRI STIRsequences(A and B) showenlarged lymph nodes at levels II and III (solid arrows) of rightside of neck with intense uptake on corresponding @°1TlSPECTimages (C and D). By contrast, for lymphadenopathiesdetectedby MRI at level IV (dotted arrows), no increased @°‘TIuptake isseen on SPECT.Note thyroid uptake (T in D). Analysis of neckspecimendemonstratedlymphnodemetastasesat levels II to V.
0.0022 %ID/g)was significantlyhigher (P = 0.0001)thanuptake in uninvolved lymph nodes (0.0023 ± 0.0014%ID/g). 201Tlactivity levels in involved lymph nodes werefound to be significantly higher than in muscle (P = 0.0 105)and fat tissue (P = 0.0001) but lower than in salivary gland
B
D
FIGURE4. (A)CoronalMRISTIRsequenceshowsenlargedlymphnode(longarrow)at levelII of rightsideof neck.(B)Bycontrast,20111SPECTimageshows uptake in right parotidgland(P) but not at place of lymphadenopathy. No lymph nodemetastaseswere found on histologyafter right neck dissection.Primary tumor, localized in right tonsillar area, is seen (shortarrows) on transaxial (C) and coronal (D) SPECT imagestogether with uptake in submandibulary glands (S); also asymmetric parotiduptake(P in C) is observed.
201TLSPECT ANDMRI m@NECKMETASTASES•ValdésOlmoset al. 1417
C)@ D
by on July 2, 2018. For personal use only. jnm.snmjournals.org Downloaded from

Patientno.No.
dissectednecklevelsNeck sideLevelsHistology@°1TI SPECTMAI(STIA)15RightVII/IIVIVN—++++—++—--—++++25RightVll/IIVIVN———+————+———++--35Rightl/Il/Ill/IVN—++—+—++———++—+48Right
LeftlI/lII/IVN ll/lll/IVN++—— +++—++—— ++——+++—+++—53RightI/Il/Ill————+————65RightI/lVllI/IVN+++—--—++———++——76Right
LeftI/Il/Ill I/Il/Ill++ —
—+++
+ —
++—+
+ +
+++85Rightl/II/lII/IVN—+———95Right
LeftIII II/lII/IVN— i-+——— +———++———105Rightl/lVlll/IVN+————+————++++—115Leftl/IIIIII/IVN—+————+————+———125RightI/li/llI/IVN—+————+—+—Total62True-positive1722False-negative72False-positive311True-negative3527STIR
= shortinversion-timeinversionrecovery.
:@1412
10p:O.0035.
.4-,p:O.0001 I
,@ p:[email protected]
I—p:O.0001----4
‘1:0@MLNSM
gland
:T@I±T@NLNMuscleFat
TABLE2Findings of Histology, @°1TISPECT and MRI (STIR) in Dissected Neck Levels
cant differences in tracer concentration in lymph nodes withand without involvement were found in the cx vivo measurements, the ability of 201'fl SPECT to localize metastasesappears not to depend on lymph node uptake weight, as seenin the correlative analysis of neck levels with histologicallyconfirmed tumor involvement of this study. The location of
metastases in the neck may play a more important role inlimiting the detectability of 2011'lSPECT, e.g., in areas of theneck with relatively increased uptake, such as levels IV andV that contain considerable muscular volume. Four of thefive false-negative 201Tl SPECT of this study concernedmetastases in these levels. Also, areas with intense concentration (salivary glands in level I) may hamper interpretation. Kostakoglu et al. (16) have suggested a decreasedactivity of the adenosinetriphosphatase pump in tumor cellswith low metabolism as a limiting factor for the sensitivityof 201'fl in detecting neck metastases, which tend to showlower proliferation rates than primary tumors. In comparison
(0.0043 ±0.0021 %IDIg versus 0.0039 ±0.0012 %ID/g,P = 0.9913) with false-negative 201T1SPECT. The differences in lymph node weight were greater (3.2 ±4.7 g versus1.8 ±3.5 g, P = 0.2542) but were also not significant.
DISCUSSION
The status of the cervical lymph nodes is an importanttumor-related prognostic factor for head and neck cancerpatients; both the incidence of locoregional recurrences andthe risk of distant metastases increase as the tumor burden inthe neck increases (4).
In a previous study of ours (14), based on data recordingper dissected neck side, the sensitivity of 201'fl SPECT was86%. In this study,basedon neck level recording,thesensitivity was lower. This leads to the conclusion that,although the method may be used for characterization of theneck as positive or negative, there are limitations to its use asa separate alternative for staging the neck. Although sigmfi
FIGURE6. Uptakeof @°1TIin 53 lymphnodes with metastatic involvement (MLN)and 145lymphnodeswithouttumor involvement(NLN).Alsoshownis uptakein muscle(n = 9), fat (n = 10) and submandibulary(SM)glands (n = 7).
1418 THEJoui@t OFNUCLEARMEDICINE•Vol. 40 •No. 9 •September1999
by on July 2, 2018. For personal use only. jnm.snmjournals.org Downloaded from

with 99mTc..MIBI, which, on the basis of spared membranepotentials and mitochondrial activity, can be concentrated bytumor cells with low metabolism, these researchers foundconsiderably fewer positive @°‘TlSPEC!' studies. Unfortunately,CT/Mffl was used as the gold standard (16), thus limiting thedifferentiation between metastatic and reactive lymph nodes, anaspect that may only be established by histology or cytology.
In this study, on the basis of data recorded per neck level,although 201T1SPECT was clearly less sensitive than MRIand could not detect other involved lymph nodes in the necknot already localized by this imaging modality, its higheffectiveness in excluding metastases in enlarged lymphnodes led to a combined SPECTIMRI accuracy of 92%.Because current diagnostic head and neck staging criteria ofMM (as well as CT) are based on the detection of lymphnodes with a size of about 1 cm, which is also considered thelimitof clinicaldetectabilityfor SPECT,the correlativeuseof SPECT and MRI for neck staging is attractive. MRI/SPECT may combine detection with characterization in thediagnosis of cervical lymphadenopathies, which is onlypossible today with USG-FNAC, a technique that demands ahigh degree of skill and multiple aspirations. Furthermore,the complementary use of combined MRI/SPECT mightpermit a more selective policy with USG-FNAC. However,only USG-FNAC is able to localize small metastases andaccurately upstage clinically positive patients with subsequent modification of the treatment (4). In addition, becauseof its potential for detecting small metastaSes (10), FDG PETmight play a role in selecting lymph nodes for aspirationcytologyor histology.The sensitivityand specificityof FDGPET to stage the neck has been found to be >90% (13,17) andits correlative use with MM may lead to an accuratecharacterization of lymph node metastases < 1 cm.
The satisfactory accuracy found for the correlative use ofSPECT and MRI reinforces the need for coregistration ofboth modalities with matched images that will permit notonly a better interpretation of SPECT by incorporation ofsuperior anatomic information but also a better characterization of enlarged lymph nodes found by MRI. At theNetherlands Cancer Institute, matching of MR. CT andSPECT (201Tl, @°@Tc-methoxyisobutylisonitrile) images isbeing performed for primary tumors localized in oropharynxand nasopharynx according to a chamfer method (18), whichenables automated three-dimensional correlation by outlining skull contours. However, because the neck presents amore cylindrical shape, image matching of this area willrequire additional reference points to obtain accuracy valuescomparable with those of the head. Despite these limitations,the use of correlative SPECT or PET with MRI or CT maybecome a useful modality for staging the neck in patientswith head and neck squamous cell carcinoma.
CONCLUSION
By combining detection with characterization, 201T1SPECTIMRI, in a correlative setting, appears to be anaccurate method for the assessment of regional spread in
patients with squamous cell carcinoma of the head and neck,especially in clinically positive necks. Because of its lowsensitivity in detecting neck metastases, the use of 201T1SPECT alone is not recommended as an alternative imagingmodality for staging the neck. Although the ability of 201T1SPECT to characterize cervical lymphadenopathies detectedby MRI appears to be based on significant differences inuptakebetweenlymphnodeswithandwithoutinvolvement,other factors such as location in neck and uptake in adjacentstructures (muscle, salivary gland) appear to limit thedetectability of the method for localization of metastases.
ACKNOWLEDGMENTS
We thank the technical staff of the Nuclear Medicine,Diagnostic Radiology, Pathology and Audiovisual departments of The Netherlands Cancer Institute for their support,as well as Harm van Tinteren of the department of Biometrics for the statistical analysis.
REFERENCES1. Som PM. Lymph nodes ofthe neck. Radiology. 1987:165:593—600.2. Stevens MH. Harnsberger HR. Mancuso AA, Davis RK. Johnson LP, Parkin JL.
Computed tomography of cervical lymph nodes: staging and management of headand neck cancer. Arch Otolaryngol. 1985:111:735—739.
3. Van den Brekel MWM, Castelijns JA, Croll GA. et al. Magnetic resonanceimaging vs palpation of cervical lymph node metastasis. Arch Otolaryngol HeadNeckSurg. 1991:117:666—673.
4. Vanden Brekel MWM, Bartelink H, Snow GB. The value of staging neck nodes inpatients treated with radiotherapy. Radiother Oncol. 1994:32:193—196.
5. Van den Brekel MWM, Stel HV, Castelijns JA. Cervical lymph node metastasis:assessment of radiologic criteria. Radiology. 1990:177:379—384.
6. DonDM,AnzaiY,LufkinRB,Fu Y-S,CalcaterraTC. Evaluationof cervicallymph node metastases in squamous cell carcinoma of the head and neck.Laryngoscope. 1995; 105:669—674.
7. Van den Brekel MWM, van der Waal I, Meijer CJLM. FreemanJL, Castelijns JA.Snow GB. The incidence of micrometastases in neck dissection specimensobtained from elective neck dissections. Laryngoscope. 1996;l06:987—991.
8. Van den Brekel MWM, Castelijns JA. Stel HV. et al. Occult metastatic neckdisease: detection with ultrasound and ultrasound-guided fine needle aspirationcytology. Radiology. 1991 ;117:666—673.
9. Takes RP, Knegt P. Manni JJ, et al. Regional metastasis in head and necksquamous cell carcinoma: revised value of US with US-guided FNAB. Radiology.1996:198:819—823.
10. Braams JW, Pruim J, Freeling NJM, et al. Detection of lymph node metastases ofsquamous-cell cancer of the head and neck with FDG PET and MRI. I NucI Med.1995:36:211—216.
11. Leskinen-Kallio S. NAgren K. Lehikoinen P. Ruotsalainen U, TerSs M, Joensuu H.Carbon-I 1-methionine and PET is an effective method to image head and neckcancer. J Nucl Med. 1992:33:691—695.
12. Linholm P,Leskinen5, LapelaM. Carbon-l 1-methionineuptakein squamouscellhead and neck cancer. JNuclMed. 1998:39:1393—1397.
I3. Braams JW, Pruim J, Nikkels PGJ, Roodenburg JLN, Vaalburg W, Vermey A.Nodal spread of squamous cell carcinoma of the oral cavity detected withPET-tyrosine. MRI and CT. I NucI Med. 1996:37:897—901.
14. ValdésOlmos RA, Balm AiM, Hilgers FJM, Ct al. Thallium-20l SPECT in thediagnosis of head and neck malignancies. J Nucl Med. 1997:38:873—879.
15. Robbins KT, Medina JE, Wolfe GT, Levine PA, Sessions RB. Pruet CW.Standardizing neck dissection terminology. Arch Otolaryngol Head Neck Surg.1991:117:601—605.
16. Kostakoglu L, Uysal U, Ozyar U. et al. Pre- and post-therapy thallium-201 andtechnetium-99m-sestamibi SPECT in nasopharyngeal carcinoma. I NucI Med.1996:37:1956-1962.
17. Laubenbauer C. Saumweber D, Wagner-Manslau C, et al. Comparison offluorine-18-fluorodeoxyglucose PET. MRI and endoscopy for staging head andneck squamous cell carcinomas. J NuclMed. 1995:36:1747—1757.
18. Van Herk M, Kooy M. Automatic three-dimensional correlation of CT-CT.CT-MRI. and CF-SPED' using chamfer matching. Med Phys. 1994:2 1:I 163—1178.
201TLSPECT ANDMRI mtNECKMETASTASES•ValdésOlmoset al. 1419
by on July 2, 2018. For personal use only. jnm.snmjournals.org Downloaded from

1999;40:1414-1419.J Nucl Med. J. M. Hilgers and Alfons J. M. BalmRenato A. Valdés Olmos, Wim Koops, Barbara M. Loftus, Ing H. Liem, Reinhold T. Gregor, Cornelis A. Hoefnagel, Frans CarcinomaCharacterizing Cervical Lymphadenopathy in Head and Neck Squamous Cell
Tl Uptake in Detecting and201Tl SPECT, MRI and Ex Vivo 201Correlative
http://jnm.snmjournals.org/content/40/9/1414This article and updated information are available at:
http://jnm.snmjournals.org/site/subscriptions/online.xhtml
Information about subscriptions to JNM can be found at:
http://jnm.snmjournals.org/site/misc/permission.xhtmlInformation about reproducing figures, tables, or other portions of this article can be found online at:
(Print ISSN: 0161-5505, Online ISSN: 2159-662X)1850 Samuel Morse Drive, Reston, VA 20190.SNMMI | Society of Nuclear Medicine and Molecular Imaging
is published monthly.The Journal of Nuclear Medicine
© Copyright 1999 SNMMI; all rights reserved.
by on July 2, 2018. For personal use only. jnm.snmjournals.org Downloaded from





![Carbon-11-Forskolin:ALigandforVisualization ...jnm.snmjournals.org/content/34/11/1944.full.pdf · forskolin.Thesynthesisof[“C]forskolinanditsanalogs willbereportedindetaillater.Theradiochemicalyieldsof](https://static.fdocuments.us/doc/165x107/5f79980b6c1748423b252668/carbon-11-forskolinaligandforvisualization-jnm-forskolinthesynthesisofacforskolinanditsanalogs.jpg)