Corporate Responsibility of Pharmaceutical Companies under conditions of market failure and failing...
22
Corporate Responsibility of Pharmaceutical Companies under conditions of market failure and failing states Third International Conference for Improving Use of Medicines, Antalya November 15 th , 2011 Klaus M. Leisinger Novartis Foundation for Sustainable Development
-
Upload
austin-page -
Category
Documents
-
view
212 -
download
0
Transcript of Corporate Responsibility of Pharmaceutical Companies under conditions of market failure and failing...

Corporate Responsibility of Pharmaceutical Companiesunder conditions of market failure and failing states
Third International Conference for Improving Use of Medicines,
Antalya November 15th, 2011
Klaus M. LeisingerNovartis Foundation for Sustainable Development

The social and economic context
Despite significant progress made in poverty alleviation and health-related Millennium Development Goals achievements
2.5 billion people continue to live in poverty (US$ 2.50 per day), thereof about 1.4 billion in extreme poverty (US$ 1.25 per day);
Their living conditions are characterized by nutritional deficiencies, lack of access to safe water and sanitation, squalid housing, insufficient knowledge about health, lack of access to preventive and curative medical services and lack of access to safe medicines, lack of voice and visibility – therefore lack of political power;
Due to neglected tropical diseases alone, • millions of children, women and men die prematurely,
• the number of disability-adjusted life years is in the dozens of millions, and
• the economic burden adds up to an amount beyond US$ 15 billion per year.
| Antalya ICIUM lecture| Klaus M. Leisinger | November 2011

Good health has a lot of influencing factors......and many stakeholders contributing to health care and prevention
Source: Dahlgren G. / Whitehead M. (1991): Policies and strategies to promote social equity in health, Stockholm
| Antalya ICIUM lecture| Klaus M. Leisinger | November 2011

The societal context
People all over the world rate “health” as one of their top personal concerns;
For people living in low-income countries HIV/AIDS, tuberculosis, malaria and other infectious diseases rates are most important (> 5 mio deaths p.a.), along with malnutrition, access to clean water, access to medical care, above all ante-natal, peri-natal and postnatal care;
Pharmaceutical products (medicines and vaccines) play an important role – along with well-trained and motivated staff medicines are the most important means available to prevent, alleviate and cure illnesses;
Lack of access to essential medicines and vaccines is seen to result in more than 10 million premature deaths;
Many NGOs and civil society media see patents and prices to be the most important obstacles for the access to medicines.
The access to medicines debate is a political debate, using methods and techniques of the political communication, including agitation;
| Antalya ICIUM lecture| Klaus M. Leisinger | November 2011

“Health” as an international political subject-matter:UN Millennium Development Goals
The Millennium Development Goals (MDGs) were adopted by 189 nations-and signed by 147 heads of state and governments during the UN Millennium Summit in September 2000.
Goal 1: Eradicate extreme poverty and hunger Goal 2: Achieve universal primary education Goal 3: Promote gender equality and empower women Goal 4: Reduce child mortality Goal 5: Improve maternal health Goal 6: Combat HIV/AIDS, malaria and other diseases Goal 7: Ensure environmental sustainability Goal 8: Develop a Global Partnership for Development
... to be achieved by 2015.
| Antalya ICIUM lecture| Klaus M. Leisinger | November 2011

Be successful in the core competencewith integrity and comply
with applicable laws and regulations
Corporate Responsibilitybeyond legality:
Legitimacy in thespirit of international norms
Corporatephilanthropyand pro bono
work
Desirable(can)
Expected(ought to)
Essentials(must)
Corporate responsibility excellence
Good management practices
What are companies competing with integrity responsible for?
| Antalya ICIUM lecture| Klaus M. Leisinger | November 2011

Corporate responsibility challenges Market failures and failing states
Who is in charge if markets fail due to the lack of purchasing power of patients and / or the state authorities not able or willing to deliver a basic package of primary health care goods and services?
Under which conditions can a pharmaceutical company be expected to do what for whom until when?
What is “appropriate” in a world with 2.5 billion people living in absolute poverty? How much is enough? Who has the legitimacy to determine this?
What medicines and vaccines should be offered with differential pricing?
What is a “fair” proportion of research dedicated to neglected diseases?
What would a “Stakeholder-Solution-Team” consist of, given the dimension and complexity of the global health problems?
| Antalya ICIUM lecture| Klaus M. Leisinger | November 2011

Access to medical care : A complex and multi-dimensional issue
Obrist B. et al. (2007): Access to health care in contexts of livelihood insecurity: A framework for analysis and action. In: PLoS Med 4( 0): e308.doi: 0. 37 /journal.pmed.0040308
Are there enough points of care to serve the population? Do drug supplies suffice?
What is the geographical distance between points of care and the homes of intended users?
Do the prices of services match patients‘ ability to pay?
Does the organisational set up meet patients‘ needs and expectations?
Does the information and treatment provided take local values into account?
| Antalya ICIUM lecture| Klaus M. Leisinger | November 2011

Differential (preferential) pricing;
Licensing for market failure;
Corporate philanthropy incl. donations;
Pro Bono research;
Screening of patent library;
Project and program co-operation with development institutions;
Management support (Human Resources, logistics, etc.);
Other innovative and creative private sector skills and methods as well as innovative business models.
Corporate responsibility tool box for „Access to Medicine“
| Antalya ICIUM lecture| Klaus M. Leisinger | November 2011

Political and Economic Preconditions for Differential Pricing
preferential prices (and donations!) can only benefit poor patients in the context of a functioning health care and supply system;
market segmentation and separation must be possible to prevent leakage of products that are offered at low prices to the poor into the “normal” market of insurance covered and well-to-do patients;
Differential prices must not be used as benchmark for reference price regulation schemes in industrialized countries;
Acceptance of governments, health insurances and patients in high-income counties for preferential pricing in low-income countries;
more (international) resources are needed even if all medicines would be given away at preferential prices.
| Antalya ICIUM lecture| Klaus M. Leisinger | November 2011

| Antalya ICIUM lecture| Klaus M. Leisinger | November 2011
Differential Pricing Controversial Issues
DifferentialPricing
· For what products? · For countries or for patients? · Who controls proper access?
Donations
Pro Bono Research
Constructiveuse of patents
· What products? · For Whom? · How long?
· What diseases?· Also Improved efficacy / side effect profiles?
· Access to patent library?· What products?· Who develops the medicines?

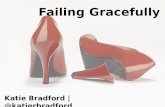
Example of stakeholder network for the supply of the anti-malarial Coartem
Procurement UNICEF
WHO
NGOs
Others
Funding organizations Global Fund (G8 countries)
UNITAID
USAID / US President‘s Malaria Initiative (PMI)
Artemisinin sourcing Chinese partners
External Chemical production
(USA, China)
Development and regulatory
WHO• Roll Back Malaria
Medicines for Malaria Venture (MMV)
Swissmedic
Local regulatory bodies
FDA
EMEA (European Medicines Evaluation Agency)
NovartisMalaria Initiative
Recipient countries Local ministries
National Malaria Control Program
Key opinion leaders
Media Key journalists

Complex issues require „multi-stakeholder-solution teams“
Different actors in society have different resources, skills, experience and networks: International community, national governments, local and international NGOs and the private sector
The entirety of all brought together in a constructive way is the best precondition for innovative and sustainable solutions.
Our overall experience is positive. (ICATT: WHO, Swiss Tropical & Public Health Institute, Sirius; Leprosy Work: WHO,
leprosy NGOs, etc., ACCESS:Swiss Tropical & Public Health Institute, Ifakara Health Institute, district authorities, Millennium Villages: UNDP, Millennium Promise, Millennium Villages Project)

Back up
| Antalya ICIUM lecture| Klaus M. Leisinger | November 2011

Health-related projects of the Novartis Foundation for Sustainable Development
| Access to Medicines UC Berkeley| Klaus M. Leisinger | October 2011

| Antalya ICIUM lecture| Klaus M. Leisinger | November 2011
Saved 10’000s of lives, particularly of children under 5, and improved livelihood of millions of people in low-income countries;
Contributed with new concepts towards bringing leprosy down from about 13 million patients in 1985 to less than 220’000 (2010) and helped to cure more than 5 million leprosy patients, preventing more than 4 million disabilities;
Developed innovative “Access to Medicines” systems (e.g. patient-based TB therapy) and did innovative research on obstacles to access (e.g. Malaria);
Developed and field-tested innovative “bare foot health insurance” as well as computer-based learning and diagnosis program for IMCI;
Developed and scaled up psychosocial support programs for vulnerable children;
Developed and field-tested performance-based funding system, measuring outcome rather than input;
Are in the process of setting new benchmark for telemedicine in Africa.
Overall results of the Novartis Foundation health projects and programs

In 2010 Novartis supported more than 85 million patients with access-to-medicine programs
1Novartis Institute for Tropical Diseases; 2Novartis Vaccines Institute for Global Health; 3Based on approximate market value
2010
Programs and research valued
at USD 1.5 bn
Coartem® subsidized > 82 million treatments shipped – cumulatively delivered > 380 million treatments, helping to save about 950,000 lives of mostly children under 5 years
Leprosy medication free of charge> 5 million patients cured since 2000
Tuberculosis medicine donations500,000 treatments committed, 50% delivered
Glivec® patient assistanceFree to >37,000 patients in about 80 countries
NITD1 in SingaporeFocus on tuberculosis, dengue fever and malaria
NVGH2 in Siena, ItalyVaccines research institute for neglected diseases
| Access to Medicines UC Berkeley| Klaus M. Leisinger | October 2011

We are helping to make a differenceKey indicators are showing progress
2004
* Estimate** 2009***2008
Every 30 secondsChildmortality
Every 45 seconds***
Malaria Cases
225 million**243 million
12 countries served
Coartem®deliveries
Patient shareof ACT market
Countriesserved
30% ACT market share 50% ACT market share*
60+ countries served
Average priceper treatment
USD 1.57 per treatment Price for public-sector buyers has dropped by over 50%
82 million treatments4 million treatments
2010
Novartis Malaria Initiative | June 201118

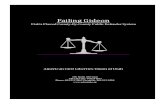
Tuberculosis(Prevalence/100,000 – WHO 2004)
Dengue Fever(Incidence/100,000 – WHO 2005)
NIBR Efforts to Address Medical Needs in the Developing World: Infectious Disease Examples (1/2)
Malaria(Prevalence/100,000 – WHO 2004)
| Antalya ICIUM lecture| Klaus M. Leisinger | November 2011
<1>250Known risk
<25>25000
<50>1000
Infectious Diarrhea
(Mortality rate/100,000- WHO 2002)
1-5>100
Chagas(Prevalence/100,000 – WHO 2002)
<1000>6000
Typhoid Fever(Incidence/100,000 – WHO 2004)
>10010-100<10

Malaria TBInfectious Diarrhea
Dengue Fever Typhoid FeverChagas Disease
Incidence250 million (Tropics, mostly Africa)
9 million (Developing World)
2.5 billion children(Dev World)
50 million(Tropics & Subtropics)
16-33 million(Developing World)
10 million(mostly Latin America)
Mortality (per year)
1 million(mostly children)
1.3 million (often AIDS patients)
1.6 million children (3-5 million total)
>100,000 (mostly children)
>200,000 (mostly children) >10,000
Organism Plasmodium Myco-bacterium
GI bacteria (incl. cholera) Flavivirus Salmonella Trypano-soma
Medical need/issue
Drug resistance (incl. Coartem)
Multi /extensive drug resistance;treatment length;HIV co-infection
Drug resistance; rapid dehydration
No effective treatment for hemorrhagic fever
Drug resistance;no pediatric vaccine (<2yrs)
No available treatment for chronic disease
CollaborationNITD, GNF & two European Research Centers
NITD, GNF & TB Alliance, NIAID Grand Challenges in Global Health (GC11) grantees
NIBR (RESP) & OneWorldHealth
Singapore Dengue Consortium (incl. NITD)
NVGH NIBR (ID), NITD and GNF
Outside Funding
MMV, Wellcome Trust & Singapore Gov
Gates Foundation & GC11 Grant
Gates Foundation
Singapore Government & Novartis Foundation
Wellcome Trust, Gates Foundation, Local Gov & Siena Foundation
NIH & Drugs for Neglected Disease initiative
Research Status
Drug candidate NITD609 entering clinic
Compound discovery
Lead optimization
Compound discovery
Vaccine vi-CRM197 in Phase II trials
Screening & biomarker discovery
NIBR Efforts to Address Medical Needs in the Developing World: Infectious Disease Examples (2/2)
| Antalya ICIUM lecture| Klaus M. Leisinger | November 2011

Why become involved in health and access issues beyond the conventional business model?
Because it is the right thing to
do!
You cannot have a first class economic performance and be perceived not to care about preventable mortality and morbidity, predominantly in children under 5 years of age.
| Antalya ICIUM lecture| Klaus M. Leisinger | November 2011

Plausible arguments for a “Business Case”
Engagement in corporate responsibility for the achievement of the health-related UN Millennium Development Goals mainly depends on top-management’s normative thinking. But
Saving lives, curing patients and preventing illness by providing innovative solutions is also likely to
Engender employees’ motivation and identification;
Enhance the attraction of the corporation as a partner for cooperation, ethical investment, excellent people, and critical customers);
Be positive from a political point of view as being “part of the solution” of one of the most difficult social issues ought to trigger good will and overcome negative stereotypical thinking.
| Antalya ICIUM lecture| Klaus M. Leisinger | November 2011