Coronary Heart #11 UK
40
Future of Cardiology For Managers Hot Topic Have the NICE guidelines altered your use of DES? Interview Dr Martyn Thomas, St Thomas’ Hospital Advanced Angioplasty Follow-up Site Visit King’s College Hospital, London Echocardiography in the community Education A review of lifesaving antithrombotic drugs coronaryheart.com March / April 200 Issue 11 E M P L O Y M E N T Subscribe Free Online
-
Upload
cardiologyhd -
Category
Documents
-
view
226 -
download
6
description
Coronary Heart March / April 2008
Transcript of Coronary Heart #11 UK

Future of CardiologyFor Managers
Hot TopicHave the NICE guidelines altered your use of DES?
InterviewDr Martyn Thomas,St Thomas’ Hospital
Advanced AngioplastyFollow-up
Site VisitKing’s College Hospital, London
Echocardiographyin the community
EducationA review of lifesaving antithrombotic drugs
coronaryheart.com
March / April 200�Issue 11 March / April 200�Issue 11
EMPL
OYMENT
Subscribe
Free
Online

2 CORONARY HEART ™
CONTENTS
Table of Contents
03 Editorial
04 Latest News
06 Interview‘Dr Martyn Thomas’
0� ECG Quiz
0� Journal Trawl
10 Hot Topic‘Have the NICE Guidelines Altered Your Use of DES?’
14 Equipment Review‘Contrast Media - Part 1’
16 CRM‘Leads to the Heart - An Extraction Evolution’
1� Conferences‘Advanced Angioplasty Review’
21 Echocardiography‘In the community’
23 Management‘Finger on the Pulse’
24 Future‘Managing the Future of Cardiology’
2� ECG Quiz Answer
2� Site Visit‘Kings College Hospital’
31 Education‘A Review of Lifesaving Thrombotic Drugs’
36 Prescription Pages‘from pages 14-15’
3� Events Diary & Employment
March / April 2008THIS EDITION
Interview with Dr Martyn ThomasPage : 6

From the Editor
EDITORIAL
CORONARY HEART ™ 3
Disclaimer:Coronary Heart should never be regarded as an authoritative peer reviewed medical journal. Coronary Heart has been designed as a guide only, to inform readers who work in the cardiology environment about latest news stories and the diff erent techniques used by others around the world. Whilst all care is taken in reviewing articles obtained from various companies and contributors, it is not possible to confi rm the accuracy of all statements. Th erefore it is the reader’s responsibility that any advice provided in this publication should be carefully checked themselves, by either contacting the companies involved or speaking to those with skills in the specifi c area. Readers should always re check claims made in this publication before employing them in their own work environment. Opinions expressed by contributors are their own and not necessarily those of their institution, Coronary Heart Publishing Ltd or the editorial staff .
Coronary Heart Publishing Ltd145 - 157 St John Street
London, EC1V 4PYUnited Kingdom
Email: [email protected]: +44 (0) 207 788 7967
Fax: +44 (0) 207 160 9334
Visit us online at
www.coronaryheart.com
Director / Chief EditorTim Larner
Clinical EditorDr Simon Redwood
Senior Consulting EditorsDr Richard Edwards
Dr Divaka PereraMr Ian Wright
Mr Stuart Allen
ADVERTISINGWendy Rose
Rose Media LtdEmail: [email protected]
CIRCULATION3171 Cardiac Professionals
Copyright 2006 by Coronary Heart Publishing Ltd. All rights reserved.
Material may only be reproduced by prior arrangement and with due acknowledgment of
Coronary Heart Publishing.The publication of an advertisement or product
review does not imply that a product is recommended by Coronary Heart Publishing Ltd.
Dr Simon RedwoodChief Clinical Editor
Dr Richard EdwardsAsst. Clinical Editor
Dr Divaka PereraAsst. Clinical Editor
Mr Stuart AllenCRM Editor
Mr Ian WrightEP Editor
Mr Tim LarnerDirector / Chief Editor
The fi rst two months of 2008 were certainly a busy time. I spent four days a week working at St Th o-mas’ Hospital in the Cath Lab helping out whilst
a staff member was on holidays. For those of you who are unaware, I am a qualifi ed radiographer, specialised in cardi-ac. Two years ago I saw a gap in the market for a publication specifi cally for us, veering away from the traditional corpo-rate style of cardiac publications which gather dust, to bring a fresh new approach. Today we have UK and US versions, with a total of 12,000 readers. Internationally via our online editions we have had visitors from over eighty countries.
Working at St Th omas’ gave me the privilege of working alongside Dr Martyn Th omas (see interview page 6) and Dr Simon Redwood, two of the leading cardiologists in the UK. However when Advanced Angioplasty (see page 18) came around I dropped the role of radiographer to be present as photographer during the live cases.
Th is is defi nitely one of the advantages of keeping my hand in radiography whilst working with our publishing team. I understand what is going on in the labs, from management through to staff . I know what aff ects you and infl uences you, and speaking with Cardiologists fi rst hand during cases, I ensure Coronary Heart can stay at the cutting edge of what is going on. I am sure you will enjoy this edition.
- Tim Larner
Staying in Touch

LATEST NEWS
What’s New?
Courtesy of B
IOTR
ON
IK
BIOTRONIK Release New Pacemakers
In early January 2008, BIOTRONIK announced the CE approval of their Cylos 990 family of cardiac pacemaker
devices. Th is new pacemaker diff erentiates itself from the competition due to a concept called Closed Loop Stimulation (CLS).
BIOTRONIK claim the CLS concept of-fers distinct clinical advantages over other rate-adaptive device algorithms because of its ability to restore a more natural physi-ologic heart rate therapy relative to the met-abolic needs of the individual patient. CLS functions within the natural cardiovascular control-loop, allowing it to mimic the sinus node.
It is also claimed that CLS initiates pacing earlier and more eff ectively during periods of emotional or mental stress, providing bet-ter heart rate response and variability, which
together improve haemodynamics, by imi-tating the ability of the sinus node to modu-late cardiac output.
Th e Cylos 990 also has a newly streamlined programming and follow-up capability, with new features including AV-AdVisor®, ProgramConsult® and Automatic Atrial Th reshold Testing.
Th e fi rst Cylos 990 pacemaker implanted in the world was at St Mary’s Hospital in Lon-don by Professor Richard Sutton on January 7.
New Technology Saves Man
A patient at the Manchester Royal Infi rmary had some luck recently after he had a severe allergic re-
action to the general anaesthetic during a routine biopsy, resulting in a cardiac arrest. He was rushed to the cath lab where he was diagnosed with apical bal-looning syndrome, commonly known as Tsubo-T Syndrome (meaning lobster pot in Japanese). Th e condition severely impairs the heart due to ballooning.
By chance Abiomed were trialling the Impella, a motorised catheter that pumps blood out of the left ventricle and into the aorta aiding blood circula-tion. Dr Fath-Ordoubadi, Consultant Cardiologist placed the artifi cial pump
into the heart, and within 24 hours of his cardiac arrest, his left ventricle was no longer dilated and 70% function had returned. Th is process normally takes several days.
Abiomed is currently undergoing dis-cussions with the NHS to fund this new technology.
Dr Fath-Ordoubadi with the Impella
Heart-Check Bed Being Developed
There is a project currently underway in Europe, funded by the EU and led by Philips
to develop a bed that has sensors that can measure heart rate, breath-ing rate and body movement while sleeping. But that’s not all. Th e bed will also have a blood pressure moni-tor and weight scales. As an extra, the patient could also wear a vest with woven-in electrodes to give a full ECG. Th e information could then be sent down a phone line to a doctors PDA.
Why is this a good idea? It is hoped the bed could reduce the need for emergency hospital treatment, help-ing spot problems several days before they become life-threatening.
Th e project, which was reported by the BBC, is expected to run for four years.
DES Perform Better in High Risk Patients
In a recent issue of the New England Journal of Medicine, researchers from the University of Pittsburgh School of
Medicine reported that “Th e use of drug-coated stents in patients with complex heart disease is associated with a lower rate of re-peat procedures without an increased risk of death or heart attacks compared to bare metal stents.”
Th e study was funded by the National Heart, Lung, and Blood Institute in the USA.
Courtesy of A
biomed
4 CORONARY HEART ™

LATEST NEWS
Research Shows iPods Do Not Interfere With Cardiac Pacemakers
Over the past twelve months there have been multiple reports that iPods
can interfere with pacemakers after ONE patient experienced dizziness. Now though this theory has been disproved.
Howard Bassen, a researcher with the U.S. Food and Drug Administration led a research team to measure the magnetic fi elds produced by four diff erent iPod models.
Th e cardiologists published their results in the medical journal, Heart Rhythm, and found that all measurements indicated no eff ects on users with cardiac pacemakers.
So now you can expect to see more old folks with pacemakers bopping along down the street listening to their favourite tunes.
With Cardiac
Howard Bassen, a researcher with the U.S. Food and Drug Administration led a research team to measure the magnetic fi elds produced by
Th e cardiologists published their results in the medical journal, Heart Rhythm, and found that all measurements indicated no eff ects on users with cardiac pacemakers.
So now you can expect to see more old folks with pacemakers bopping along down the street listening to their favourite tunes.
Courtesy of Apple
Researchers Create Beating Heart
Earlier this year researchers from the University of Min-nesota managed to create a
beating heart in their laboratory, By using a process called whole organ decellularization. Basically what they did was remove all of the cells from an animal cadaver heart, leav-ing only the extracellular matrix, the framework between the cells, intact.
Th is was followed by the hearts being injected with a mixture of progeni-tor cells that came from neonatal or newborn rat hearts, and then left in a sterile environment to grow. Af-ter only four days contractions were observed. After eight days the heart was actually seen pumping.
“We just took nature’s own building blocks to build a new organ,” said Harald C. Ott, M.D., co-investi-gator of the study and a former re-search associate in the center for car-diovascular repair, who now works at Massachusetts General Hospital. “When we saw the fi rst contractions we were speechless.”
“We used immature heart cells in this version, as a proof of concept. We pretty much fi gured heart cells in a heart matrix had to work,” said Doris Taylor, Ph.D., principal inves-tigator of the research. “Going for-ward, our goal is to use a patient’s stem cells to build a new heart.”
Th e research was published online in the January 13 issue of Nature Medicine.
Siemens Launch New CT and MRI
Unveiled at the Science Museum in London, Siemens recently offi cially
launched their latest innovations in the fi eld of CT and MRI imaging. Set against a back-drop of the spectacular Space exhibit, Siemens’ experts proudly introduced the new technology.
Th e MAGNETOM Verio is a 3T fi eld strength MRI which can be used for cardiac imaging. It features a wider than normal open bore (70cm) and features Tim™ (Total imaging matrix) in one powerful system. It is also the shortest 3T magent available and the lightest.
Th e SOMATOM Defi nition AS is the world’s fi rst adaptive CT scanner. Th is sim-ply means they can adapt to any patient or clinical need in routine diagnostic work and complex examinations including cardiol-ogy.
CAUTION: Some products within this magazine may be restricted to specific regional usage, and may not be available in your region. Always check with the manufacturer to determine availability.
The MAGNETOM Verio launched at the Science Museum in London
Courtesy of S
iemens
CORONARY HEART ™ 5

INTERVIEW
Interview:Dr Martyn Thomas
Why did you decide to become an Invasive Cardiologist?
I had a good memory, was very competi-tive, and I could play golf! Just to explain, I became a doctor because I thought “Doc-tor in the House”, a television programme in the 70’s, made it look like fun and I had a reasonable memory allowing me to pass ex-ams…….sadly a prerequisite to follow this path. Th e golf bit is because to become an interventional cardiologist you require a de-gree of hand eye co-ordination. Th erefore, in my opinion, one of the indications of a good interventional cardiologist is someone with a good memory (I’m not so sure “intel-ligence” is important!) who can play golf (or a similar sport).
Where did you train?
I was a medical student at St Bart’s Hospital, a cardiology trainee and consultant at Kings College Hospital, and have only recently moved to St Th omas’ Hospital.
What are some of your career highlights?
Having come from a small town in Wales a highlight was to have ever become a Con-sultant Cardiologist! To now be have been a Consultant in two important cardiology centres is beyond my wildest dreams. Fi-nally to have had the honour to have been President of our National Angioplasty So-ciety (BCIS) is somewhat surreal for some-one who spends his whole life wondering how he got to where he is??………..maybe that’s the point………..a degree of paranoia might just be healthy??
What is your most interesting case?
Th e joy of interventional cardiology means every day is interesting. I suspect my most interesting case will be tomorrow!
What does your role of BCIS president entail and how does the BCIS benefi t members?
Th e role of BCIS President is complex and changes with time. I chose during my time to concentrate on the international profi le of UK interventional cardi-ology. To this end I chose to make Advanced Angioplasty our “fl ag-ship” event with a 3 day meet-ing including live cases. Th is was introduced against a degree of reluctance but thankfully has been a great success. I believe this helped BCIS become “em-bedded” in the 2 major worldwide PCI meetings, EuroPCR and TCT. In 2008 BCIS will have a specifi c ses-sion at EuroPCR and TCT, and a live UK centre for TCT is now a settled part of the programme. I am very proud of this achieve-ment but acknowledge the huge contri-bution of Keith
Dawkins (the previous BCIS President) to this process. I am sure the next President, Dr Mark de Belder, will continue this push toward international recognition along with refocusing on national issues, which have had increased importance
What does your role of BCIS president entail and how does the BCIS benefi t members?
Th e role of BCIS President is complex and changes with time. I chose during my time to concentrate on the international profi le of UK interventional cardi-ology. To this end I chose to make Advanced Angioplasty our “fl ag-ship” event with a 3 day meet-ing including live cases. Th is was introduced against a degree of reluctance but thankfully has been a great success. I believe this helped BCIS become “em-bedded” in the 2 major worldwide PCI meetings, EuroPCR and TCT. In 2008 BCIS will have
sion at EuroPCR and TCT, and a live UK centre for TCT is now a settled part of the programme. I am very proud of this achieve-ment but acknowledge
Dr Martyn Thomas
Director of Cardiology and Cardiothoracic Services,
St Thomas’ Hospital, London
6 CORONARY HEART ™

INTERVIEW
The Advanced Angioplasty conference becomes more popular each year. What are the plans over the next few years in regards to growth, and will it soon be held in a bigger venue like the BCS Annual Meeting?
Advanced Angioplasty has, I hope, devel-oped while I have been BCIS President. I will now take a back step as I step down as BCIS President. I do hope the concept of a 3 day meeting persists. I think the asso-ciation with BSET (the British Society of Endovascular Therapies) is important and I hope this will continue. I think the current numbers attending Advanced Angioplasty, from 750-800, is ideal. For the meeting to grow larger than this would mean consid-ering making the meeting international in its target audience. I think this would not be a good idea. The strengths of the meet-ing are that there are no parallel sessions and generally every session is well attended. The angiography review sessions are very “Brit-ish” and I think are the major strength of Advanced Angioplasty. I think it is time for new ideas and I will step aside from the or-ganising committee for a couple of years to allow this to happen.
What do you believe will be the biggest change in cardiology within the next 5-10 years?
British cardiology faces a major challenge over the next 5 years. I belive this involves the “justification” of “major/surgical” cen-tres. Many of the procedures that identified a “tertiary” centre can now be performed in DGH/non surgical centres. This is right and proper and demonstrates the maturity and safety of many of these procedures, in-cluding angioplasty. This does, however, threaten the stability of many major centres throughout the country. The major chal-lenge is now to debate the “added value” of large volume/tertiary/surgical centres. I be-lieve there is value to these institutions in terms of service development, R+D, train-ing, teaching, and the development of new procedures. This argument has to be won centrally if these centres are not to disap-pear. At the moment finances and market
forces are dictating the development of serv-ices and strategic thought has been lost, in my view. An example would be a “network” with 10 hospitals that requires 4,000 angi-oplasties. Currently, and in a market forces driven health care enviroment all hospitals would do 400 cases each. I would argue this lacks strategic thought and a better model would be 5 centres doing 400 cases and 1 centre doing 2,000……………someone should create an environment where this is allowed to happen.
Are you pleased with the outcome of the NICE study? If it had gone the other way, would it have changed your decision making when choosing a stent?
The recent NICE review of the cost effective-ness of drug eluting stents was an exhaust-ing process. I am delighted that eventually the NICE committee decided to reverse the decision of their draft guidance. This was
Dr Martyn Thomas (left) alongside Dr Simon Redwood (middle) and radiographer Alex Harrington during a live case for Advanced Angioplasty
CORONARY HEART ™ �

INTERVIEW
� CORONARY HEART ™
only because of a vast amount of work which took place in the background from a number of individuals. BCIS and the BCS were actively involved in this process. I just hope that when members use these devices in the future they, at least, have some idea of how hard certain people worked to achieve this. The attitude of “I’m sure it will be fine in the end” which I heard on so many occa-sions is naïve and complacent. We were very close to a disaster and anyone who did not help (by “hitting” the NICE website with comments on the draft guidance) should be ashamed of themselves. If the guidance had continued to deny the UK the use of DES I planned to write to BCIS members asking them to refer all multi-vessel patients back to surgery……….and then stand back and watch the mayhem! Although you may think this hard on patients it would have
been intellectually sound and would have demonstrated to NICE that the UK com-munity was amongst the most “evidence-based” in the world and they had seriously underestimated us if they assumed we would default to bare metal stents.
What are your thoughts on cardiac CT? Do you use this imaging modality?
Cardiac CT is “just around the corner” and has been for a while! I have ordered very few studies to date. The radiation dose has been a concern. However, I think with improved technology we are nearly there. My own institution is in the process of purchasing a state of the art scanner. My worry is the possibility of the demand from asympto-matic patients for such a scan and all of the
implications of this. Still, you cannot stop progress we will just have to manage this po-tential problem.
What are your hobbies and passions outside of work?
Outside work sport is my main passion. I am a season ticket holder with Crystal Palace FC and also attend most England football internationals. I may be the problem with the England team, having attended both quarter final losses to Portugal on penalties in the European Championships in Lisbon and the World Cup in Germany. Maybe if I stopped going we would win. In addition, I love going to cricket test matches and my son and I travelled to Melbourne to attend the last Boxing Day Ashes Test match.
INTERVIEW: DR MARTYN THOMAS (cont...)
ECG QUIZ Provided by: Ian Wright, Technical Head EP, St Mary’s Hospital, London, UK
What is the ECG rhythm?
What is the relationship between atrial and ventricular complexes?
1.
2.Answer: Page 27

JOURNALS
CORONARY HEART ™ �
It is interesting how once a treatment enters officially sanctioned guidelines it ceases to be questioned. In this way amiodarone has replaced lignocaine as
first line treatment for stable VT in seeming-ly unopposed. Researchers in Oxford noted this and looked back at its record at their centre. Only 29% of patients cardioverted within an hour and 17% became haemody-namically compromised to the extent that electrical cardioversion was required. They noted that this experience of amiodarone compares unfavourably with sotalol and procainamide in historical controls.Tomlinson and others, Emerg Med J. 2008 Jan;25(1):15-8.
Sucking the clot out of the artery causing a heart attack is an attractive concept. Its now backed by evidence, primary PCI patients randomised to normal techniques or throm-bus aspiration. Aspiration was associated with better myocardial blush grade which in turn was associated with better medium term outcomes.Svilaas and others. N Engl J Med 358;6
I don’t know what we used to call Japanese octopus trap shaped ventricles before we were allowed to start calling it Tako-Tsubo to pretend we’d actually made a diagnosis. The echo features and short term follow up are nicely described in a small follow up study. Functional assessments improved dramatically over medium term follow up.Bahlmann and others. Int J Card 124 (2008) 32–39
Antiplatelet resistance has entered the con-sciousness of cardiologists largely as a result of its contribution to major morbidity fol-lowing PCI. The phenomenon however has much wider consequences potentially affect-ing any patient with cardiovascular risks. A meta analysis of trials examining outcomes in aspirin non responders (the trialists pre-ferred term) found an incidence of 28% with four fold increase in cardiovascular events in this group compared with aspirin sensitive individuals. Somewhat depressingly the as-pirin non responders weren’t helped by al-ternative/adjunctive antiplatelet agents. An accompanying editorial discusses whether aspirin non response is truly an independent risk factor or really a marker of other uncon-trolled cardiovascular risk. There is clearly a lot more work to be done in this area to an-swer questions including what the mecha-nism is and how to treat these patients.Krasopoulos and others, Brit Med J. epub ahead of print.Biondi-Zoccai and Lotrionte, Brit Med J. epub ahead of print.
It must be odd living in Frammingham, PhD students roaming the streets assaulting unsuspecting residents with sphygmoma-nometers and chylomicron subtype assays.
Can’t argue with the output though, this time it’s a new risk calculator based on a scoring system with positive and negative points awarded for age, HDL, BP, total cho-lesterol , diabetes and smoking. The system is simple(ish) and suitable for use in primary care-its target setting.D’Agostino and others. Circulation 2008;117;743-753
One of the problems associated with im-planting ICDs is that they do what they’re supposed to - deliver shocks (and patients seldom enjoy the experience). An approach in patients with primary prevention ICDs is to perform a prophylactic ablation, at least in those with clear ischaemic scar as a po-tential focus. In a trial of this process 128 patients were randomised to VT ablation vs. none at the time of ICD implant. Ablation cut the incidence of all ICD therapies and shock therapies specifically by about a two thirds over two year follow up. There were no serious adverse events.Reddy and others. N Engl J Med 357;26
At the other end of the spectrum are patients presenting with electrical storms. The larg-est series to date in this group provided en-couraging results regarding value and safety of ablation in this group. In 95 consecu-tive patients ablated for VT storms 85 had their clinical VT rendered non inducible (of which 68 had no inducible VT of any morphology) and this was associated with a significantly better outcome than those with procedural failure.Carbucicchio and others. Circ 2008;117;462-469
Journal Trawl
Dr John PaiseyClinical Fellow in Electrophysiology
John Radcliffe Hospital, Oxford
- Dr John Paisey scans the world’s cardiology journals

HOT TOPIC
Adam de Belder MD FRCP Consultant Cardiologist, Brighton and Sussex University Hospitals, Brighton
What is NICE for? Who is NICE for?
Some would say that it is to implement best practice after consideration of the current literature? Others see it as a cost-restricting organisation to prevent profl igation? Some advocate that it is a useful tool by which the NHS/Government can restrict funding of expensive drugs/devices. Certainly it causes a lot of consternation for diff erent patient groups, particularly if the NICE guidelines do not support the use of a device or a drug.
Let’s take the example of drug eluting stent technology. Th e original guideline highlighted the benefi t of this technology, particularly for small long lesions, and although there were fl aws in this, it was a pragmatic indicator that all operators could
work by. My main concern was that there was no guideline towards to the use of DES for patients whose clinical risk of in-stent restenosis was very high eg left main disease.
And now we have a guideline saying that the advice they gave previously was OK only if the price diff erential between a DES and a BMS is £300, with a pre-specifi ed price for BMS. What will the lawyers think of this? Technology which has cost millions to develop being marketed purely on the basis of a directive from an outside agency. I’m not an expert on the intricacies of trade practice but this seems very restrictive.
Some see the hand of Government and the Tsar on these documents, but of course, what conversations go on in the corridors of power will never be clear.
Enough of this – what of the patients who might benefi t from this technology? I suppose that will depend on contractual negotiations between the companies and the Trusts. Th e Trusts will now hide behind NICE guidance as their framework for negotiation, and what will the companies do…..well we’ll have to wait and see. Presumably the profi t margins will fall substantially…perhaps only the bigger companies will survive….perhaps the
market will not be of suffi cient interest to them, and their eff orts will be redirected to more profi table markets abroad….I don’t know, but what I do know is that many of my patients have benefi ted hugely from DES technology, having avoided bypass surgery and its associated morbidity.
Have The NICE Guidelines Altered Your Use Of DES?
the advice they gave previously was OK only if the price diff erential between a DES and a BMS is £300, with a pre-specifi ed price for BMS. What will the lawyers think of this? Technology which has cost millions to develop being marketed purely on the basis of a directive from an outside agency. I’m not an expert on the intricacies of
benefi t from this technology?
the Trusts. Th e Trusts will now hide behind NICE guidance as their framework for negotiation,
do…..well we’ll have to wait and see. Presumably the profi t margins will fall substantially…perhaps only the bigger companies will survive….perhaps the
associated morbidity.
with Dr Adam de Belder, Dr Sundip Patel, Dr Andreas Baumbach, Dr Jagdip Sidhu
10 CORONARY HEART ™

HOT TOPIC
CORONARY HEART ™ 11
Dr Sundip J PatelConsultant Cardiologist, Queen Elizabeth Hospital NHS Trust, Woolwich, London & Honorary Consultant Cardiologist, St Thomas’ Hospital, Guy’s and St Thomas’ NHS Foundation Trust, London
No, not particularly!
Th e “preliminary recommendations” from the initial appraisal consultation document for the use of drug eluting stents (DES) for coronary artery disease, from the National Institute of Clinical Excellence (NICE) in July 2007, were undoubtedly a surprise to the cardiology community as a whole. Th e inference appeared to be in stark contrast to the recommendations released in the tech-nology appraisal of October 2003, when DES were recommended for patients with
a target artery calibre of < 3mm or a le-sion length >15mm. Th e im-
plications of this guid-ance, if approved, were potentially
dramatic to the treatment of our patients
with coro-nary artery d i s e a s e , related is-c h a e m i c symptoms and le-sions sat-i s f y i n g the “3 or 15” cri-teria. To
s c e p t i c a l c l i n i c i a n s
like myself, there seemed to
be a possibility that the guidance being given was driven predominantly by relatively small-sized, single-centre fi nancial/ cost-eff ectiveness models
rather than on a peer-reviewed international evidence-base supporting the clinical eff ec-tiveness of DES as an optimal therapy, above and beyond conventional bare metal stents (BMS), in particular subsets of patients.
Clearly, a signifi cant proportion of patients that we meet in our clinical practice, partic-ularly in the catchment areas where I work, fall outside the often purist limited inclusion criteria defi ned by the (randomised control, RCT) trials comparing DES and BMS. Th e patients in our local population have a high burden of diabetes mellitus, diff use/ exten-sive, relatively small calibre vessel disease. Percutaneous coronary intervention (PCI) in this setting, when appropriate, intuitively mandates the use of DES. Consequently, this raises 2 issues as drawn upon by NICE: (i) clinical safety, in particular related to stent thrombosis with the use of DES “off -label” and (ii) fi nancial/ cost eff ectiveness.
Th ere is however a large database providing useful information into the safety of DES in a much broader and heterogeneous real-world population than “prescribed” by clini-cal trials and to some extent by NICE. Two such recent registries1, 2 have been reassuring about the placement of DES in an off -label fashion. In the NHLBI Dynamic Registry of over 6000 patients, not surprisingly both BMS and DES when used off -label were as-sociated with a higher rate of mortality and/ or MI, compared to on-label use at 1 year. However, in addition to the expected lower rates of repeat target vessel revascularisation (TVR), MI rates were signifi cantly lower for DES than for BMS. Th e Winston-Salem-USA registry of almost 2500 patients paint-ed a similar picture comparing on versus off -label DES and BMS cases. Once again, off -label usage irrespective of stent type was associated with a signifi cantly higher event rate. Off -label DES against off -label BMS results showed a signifi cant reduction in MI/ death/ all-cause mortality in the order of 20-25% at 2 years, in addition to the expected 30% reduction in the need for repeat TVR. Th e benefi t was also seen in specifi c high-risk subgroups such as patients with acute myocardial infarction, renal failure and dia-betes. Reassuringly, there was no signifi cant diff erence in stent thrombosis rates at 2 years although there were several cases of late stent
thrombosis after 1 year compared to zero in the BMS group (0.8% incidence).
Clearly there are limitations to such registry studies, with RCTs being the gold stand-ard for comparing the effi cacy of 2 thera-pies. Nonetheless they do provide valuable clinical information on the various eff ects, benefi cial and harmful, of the therapies on a broader population of patients, particularly when cohorts are followed up for longer pe-riods of time.
Th e Final Appraisal Determination from NICE in February 20083, demonstrated that there clearly was a positive response to the concerns raised by the cardiology com-munity across the country. Th e “3 or 15” statement was reinstated but restricted by a cost-diff erential ceiling of no more than a £300 diff erence between DES and BMS. Th is will have implications not only for the device companies but also for local primary care trusts, hospitals, regional cardiac net-works and strategic health authorities. Lo-cal tendering processes will be potentially very interesting let alone challenging for all stakeholders!
Ultimately, in my clinical practice the deci-sion process for when to use a DES is un-changed, based not alone on lesion char-acteristics and cost, but also on patient characteristics e.g. co-morbidities, the abil-ity to take prolonged courses of dual an-tiplatelet therapy etc., ensuring that therapy is patient tailored to maximize clinical ben-efi t with minimisation of risk.
References:
Marroquin OC, Selzer F, Mulukutla SR, et al. A comparison of bare-metal and drug-eluting stents for off -label indications. N Engl J Med 2008; 358:342-352Applegate RJ, Sacrinty MT, Kutcher MA, et al. “Off -label” stent therapy: 2-year comparison of drug-eluting versus bare-metal stents. J Am Coll Cardiol 2008; 51:607-614NICE. Ischaemic Heart Disease – Coro-nary Stents (Review): Final Appraisal Determination (FAD) February 2008. http://www.nice.org.uk/guidance/index.jsp?action=folder&o=39067
1.
2.
3.
the recommendations released in the tech-nology appraisal of October 2003, when DES were recommended for patients with
a target artery calibre of < 3mm or a le-sion length >15mm. Th e im-
plications of this guid-ance, if approved, were potentially
dramatic to the treatment of our patients
with coro-nary artery d i s e a s e , related is-c h a e m i c symptoms and le-sions sat-i s f y i n g the “3 or 15” cri-teria. To
s c e p t i c a l c l i n i c i a n s
like myself, there seemed to
be a possibility that the guidance being given was driven predominantly by relatively small-sized, single-centre fi nancial/ cost-eff ectiveness models
CORONARY HEART ™ 11

HOT TOPIC
12 CORONARY HEART ™
Dr Andreas Baumbach, MD, FRCP, FESC
Consultant Cardiologist, hon. Reader in Cardiology
Clinical Lead for CardiologyDivision of Specialised Services
Bristol Royal Infirmary
The answer to this question is short and simple: not at all.
Th e fi nal version of the NICE guidance on the use of drug eluting stents does not dif-fer from the clinical recommendations that we have already followed over the last cou-ple of years. I have always thought that the initial NICE recommendations were very sound and took into account that some patients will have a larger benefi t from the use of drug eluting stents than others. In our Unit we have followed the NICE guidance and we are currently implanting around 60% drug eluting stents. Th e new guidance has simply been amended by an economical clause which says that drug eluting stents should only be used if the price diff erential between bare metal stents and drug eluting stents does not exceed £300.
Does that mean that the clinical benefi t we thought to give our patients by choosing a drug eluting stent is now not cost eff ective, just because bare metal stents have become
so cheap?
An adjustment of the prices of drug eluting stents has already happened prior to the publication of the NICE issues. Th is is, of course, a welcome development for our departmental budgets and we may fi nd that this competitive market will self-adjust towards NICE compliance.
Hence, I neither see a clinical nor economi-cal need to change my practice based on the new NICE guidance. A future change in clinical practice would be based on new clinical data on effi ciency, especially in diabetic patients, which has not been recognised by NICE. Finally, of course, the ongoing debate about late stent thrombo-sis must be followed and may result in a change of my utilisation of drug eluting stents in certain sub-groups or in a change in the choice of stent.
For now, however, I continue just as before the recent NICE publication.
Dr. Jagdip Sidhu Consultant Cardiologist Dartford & Gravesham NHS Trust and Honorary Consultant Cardiologist Guy’s & St. Thomas’ NHS Foundation Trust.
If the recent draft of the NICE Final Appraisal Determination relating to the use of DES is approved then my
use of DES will not change. I am relieved that the draft guidance approves their use, albeit with contentious stipulations. Th e recent draft only has two changes from the previous guidance published in 2003 and neither of these will alter my use of DES.
Firstly, DES are recommended for the treatment of coronary artery disease “within their instructions for use”. Th e implication is that the use of DES for
off -label reasons that do not meet the standard criteria for the particular DES should be avoided. I use DES in patients with lesions at high risk of restenosis and these often include off -label indica-tions such as the treatment of in-stent restenosis, bypass graft lesion, left main disease, ostial, bifurcated, or totally oc-cluded lesions. Recent data show that among patients with off -label indications, DES implantation leads to signifi cantly reduced restenosis without an increase in death or non-fatal MI, when compared to BMS.1,2 Th erefore, I will continue to use my best judgement and implant DES in off -label indications where I believe it is the optimal therapy for a specifi c patient. Secondly, the draft guidance recommends that DES only be used where the price diff erence between DES and BMS is no more than £300. Again, this will not in-fl uence my decision to implant a DES in a given patient where clinically indicated.
Th e impact of this statement will clearly be felt outside the catheter laboratory. Th e onus will be on industry and those involved in purchasing/tendering to secure the best possible deals. Th e cost of stents can vary widely according to locally negotiated procurement discounts. Th e guidance might be an incentive for indus-try and the NHS to agree on a national procured price for DESs and ensure that they are available to all patients who need them at a reasonable price.
ReferencesMarroquin et al. N Engl J Med 2008; 358(4): 342-352
Roy et al. Am J Cardiol. 2008;101(3):293-9. Epub 2007 Dec 21
1.
2.
HAVE THE NICE GUIDELINES ALTERED YOUR USE OF DES? (cont...) Better outcomes for more patients
1. Suwaidi et al. Am Heart J 2004;147:815-822. 2. Babapulle et al. Lancet 2004;364:583-591. 3. Stone G.W. PCR 2007. 4. Hamm C. Da VINCI Registry. EuroPCR 2005. 5. Sangiorgi G. RISICO Registry. Poster Presentation, GISE Congress, Italy 2006.
This product is intended for use by or under the direction of a physician. Prior to use, it is important to read the packageinsert thoroughly for instructions for use, warnings and potential complications associated with use of this device. Information contained herein for distribution outside the U.S. and Japan only. Please check the regulatory status of the device before distribution in areas where CE marking is not the regulation in force. For more information, visit our website at abbottvascular.com© 2007 Abbott Laboratories. All rights reserved. EHQ 1382-01 10/2007
Results from different clinical trials are not directly comparable. Information provided for educational purposes only.
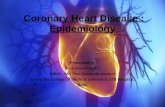
Out of every 100 patients treated with…
0 5 10 15 20 25 30
… will have a MACE
ML VISION4,5
1st Gen DES2,3
XIENCE V3
ML VISION andDesigned to reduce MACE
POBA1
BMS1,2
12 CORONARY HEART ™

Better outcomes for more patients
1. Suwaidi et al. Am Heart J 2004;147:815-822. 2. Babapulle et al. Lancet 2004;364:583-591. 3. Stone G.W. PCR 2007. 4. Hamm C. Da VINCI Registry. EuroPCR 2005. 5. Sangiorgi G. RISICO Registry. Poster Presentation, GISE Congress, Italy 2006.
This product is intended for use by or under the direction of a physician. Prior to use, it is important to read the packageinsert thoroughly for instructions for use, warnings and potential complications associated with use of this device. Information contained herein for distribution outside the U.S. and Japan only. Please check the regulatory status of the device before distribution in areas where CE marking is not the regulation in force. For more information, visit our website at abbottvascular.com© 2007 Abbott Laboratories. All rights reserved. EHQ 1382-01 10/2007
Results from different clinical trials are not directly comparable. Information provided for educational purposes only.
Out of every 100 patients treated with…
0 5 10 15 20 25 30
… will have a MACE
ML VISION4,5
1st Gen DES2,3
XIENCE V3
ML VISION andDesigned to reduce MACE
POBA1
BMS1,2

EQUIPMENT REVIEW
14 CORONARY HEART ™
Uses:X-Ray contrast medium for use in adults (cardioangiography, cerebral angiography, peripheral arteriography, abdominal an-giography, urography, venography, CT-enhancement, studies of the upper GI tract, arthrography, hysterosalpingography and endoscopic retrograde cholangiopancreatography, lum-bar, thoracic and cervical myelography) and children (cardio-angiography, urography, CT-enhancement and studies of the upper GI tract)
Basic Overview:Isosmolar Visipaque is the only x-ray contrast medium avail-able for intravascular use with an osmolality equal to blood at all iodine concentrations and formulated with Na and Ca. It gives excellent diagnostic results and is particularly suited to the newer cardiac CTA procedures1.
Advantages:Due to its unique physicochemical properties, Visipaque is an excellent choice for use in patients at high-risk for con-trast-induced nephropathy2,3,4 and major adverse cardiac events5,6. It provides better patient comfort compared to a range of low-osmolar contrast media and it is isosmolar with blood7,8,9,10,11.
Contact Details:GE Healthcare (Medical Diagnostics)Amersham Place, Little Chalfont, Bucks, HP7 9NAwww.visipaque.com
1. Tsai I et al. Am J Radiol 2008; 190: W47-53.2. Aspelin P et al. N Engl J Med 2003; 348: 491-9.3. Jo S-H et al. J Am Coll Cardiol 2006; 48(5): 924-30.4. Hernandez F, et al. Eur Heart J 2007; 28 (Abstract Supplement): Abs 454.5. Davidson CJ et al. Circulation 2000; 101: 2172-7.6. Harrison JK et al. Circulation 2003; 108 (Suppl. IV): Abstract 1660.7. Verow P et al. Brit J Radiol 1995; 68: 973-8.8. Manke C et al. Acta Radiologica 2003; 44: 590-6.9. Tveit K et al. Acta Radiologica 1994; 35: 614-8.10. Palmers Y et al. Eur J Radiol 1993; 17: 203-9.11. Justesen P et al. Cardiovasc Intervent Radiol 1997; 20: 251-6.
Uses:X-ray contrast medium for use in adults and children for urography, phlebography, i.v. DSA, CT, arteriography, car-dioangiography and i.a. DSA. myelography. For use in body cavities: arthrography, endoscopic retrograde cholangiopancreatography, herniography, hysterosalpingog-raphy, sialography and use in the GI tract.
Basic Overview:Used since 1982 in over 100 countries in over 330 million procedures1, examined in over 40 doctoral theses and 6,500 clinical studies, and subject to large safety surveillance studies on diff erent continents, Omnipaque is set to be as reliable a component of future advances in radiology as it has been of those of the past.
Advantages:Omnipaque is indicated for oral use and has better taste and tolerability versus oral high-osmolar contrast media2,3.
Both Omnipaque and Visipaque are available in +PLUS-PAK™ polymer packaging. Th is gives the advantages of en-hancing workplace safety (no sharp alloy ring pull, easy-open polypropylene ring pull avoids cuts from sharp metal edges and removes risk of injuries from glass breakages). +PLUS-PAK may also improve workplace effi ciency through quick-opening screw top, integral hanger, triple labels with peel-off stickers and effi cient storage with +PLUSPAK bottles being less bulky and heavy to store than their glass counterparts.
Contact Details:GE Healthcare (Medical Diagnostics)Amersham Place, Little Chalfont, Bucks, HP7 9NAwww.omnipaque.com and www.pluspak.com
1. Data on fi le, GE Healthcare.2. Smevik B, Westvik J. Acta Radiol 1990; 31: 601-4.3. Diederichs G et al. Fortschr Röntgenstr 2007; 179: 1061-7.
Contrast Media in Cardiology
Visipaque™ (iodixanol)
Omnipaque™ (iohexol)
in Cardiologyin Cardiology

EQUIPMENT REVIEW
Prescribing Information for all products featured can be found on pages 36-37.
CORONARY HEART ™ 15
UsesLow Osmolar non-ionic X-Ray contrast media for angiocar-diography, aortography – retrograde, arthrography, cerebral angiography, CT enhancement, coronary arteriography, DSA, intravenous urography, left ventriculography, lumbar myelography, peripheral arteriography, selective renal angi-ography, selective visceral angiography, thoraco cervical my-elography, venography & ventricular angiography.
Basic OverviewNiopam® was the fi rst ready to use non-ionic contrast agent on the market and has been the subject of over 3000 clinical publications. Recently Niopam® has been the subject of an important clinical study published comparing a low Osmolar and an Iso-osmolar on the topic of Contrast Induced Neph-ropathy (CIN) in Cardiac Angiography and PCI examina-tions1.
AdvantagesNiopam® is available in a wide range of presentations includ-ing high concentration 370mgI/ml.
Niopam has low osmolality and low viscosity contributing to its profi le making it a superb contrast media choice both routine patients and those at high risk of developing CIN.
Contact Details:Bracco UK, Mercury Park, Wycombe Lane, High Wycombe, Buckinghamshire, HP10 [email protected]
1 Solomon et al (Circulation 2007;115(25):3189-3196)
Part 1 of a Two-Part Series
UsesX-Ray contrast media for angiocardiography, aortography, arthrography, cavernosography, cerebral angiography, CT en-hancement, coronary arteriography, dacrocystography, DSA, endoscopic retrograde cholangiopancreatography, fi stulogra-phy, galactography, hysterosalpingography, left ventriculog-raphy, myelography, peripheral arteriography, sialography, urography, venography & visceral arteriography
Basic OverviewIomeron® is the latest non-ionic monomer contrast agent to be introduced onto the market and has the lowest osmolality and viscosity of all monomeric contrast agents, which con-tribute to the acceptance of the molecule.
AdvantagesIomeron® is available in the highest concentration (400mgI/ml) which allows clinicians the delivery of necessary iodine load with normal injection rates but without unnecessary os-motic load, to provide good contrast enhancement and image quality.
Contact Details:Bracco UK, Mercury Park, Wycombe Lane, High Wycombe, Buckinghamshire, HP10 [email protected]
Niopam® (Iopamidol)
Iomeron® (Iomeprol)

Over the last two years, since the disclosure of safety issues re-garding heart defibrillators, de-vice designers, manufacturers
and the regulators have paid closer attention to tracking device performance once they reach the market.
Pacing leads, which connect pacemakers and defibrillators to the heart, have received particular attention from regulators and the media. These leads are intended to deliver an electric shock, when necessary, to stabilise a dangerously erratic heartbeat and as such are a major component to the set-up of a pace-maker or defibrillator.
In Europe over 750,000 leads to pacemakers and defibrillators are implanted into patients every year. Of these leads it is estimated that between 4 and 7 per cent will have to be removed at some point due to damage, in-fection or the inability to implant new leads due to the presence of existing ones.
Since the commercial introduction of im-planted transvenous pacing leads, a wide variety of methods for removing leads have been developed and today the main lead extraction technologies are either laser pow-ered or mechanical.
Evolving Technology and Techniques
In the years following the introduction of chronically implanted transvenous pacing leads, a variety of methods for lead removal were trialled, the simplest being traction, often also called the “drag through” tech-nique. For patients with significant fibrous overgrowth, more aggressive methods had to be developed, including traction applied by weights and elastic bands among other methods.
Nonetheless, complications and difficulties encountered when using traction for lead removal led some investigators to surgical approaches, whereby the heart and great veins were exposed via sternotomy or thora-cotomy allowing extraction of a lead via an incision in the atrium or ventricle. In greatly experienced hands, these techniques pro-duced high success rates, but required high-ly specialized skills gained through years of training. In addition, these techniques were associated with morbidity and the heavy economic impact of open surgery.
The desire for safe and more economically viable extraction techniques led to the de-velopment of intravascular counter-pres-
sure and counter-traction – using telescopic sheaths made of polymer and /or steel mate-rial, which would slide over the lead body. This technique removes the fibrotic tissue that develops over time and entraps the im-planted lead in the veins. As the sheaths are advanced over leads to tear and peel away the encapsulating tissue they achieve a trans-venous removal of leads with minimised risk to the patient compared with previous methods.
Today’s Choices
The procedure of lead removal has matured into a definable, teachable art with its own
Leads to The Heart – An Extraction Evolution
In this article, Barry Norlander, Global Marketing Manager for Cook Vascular Strategic Business Unit, outlines current treatments and best practice lead extraction techniques and technology.
CRM
16 CORONARY HEART ™

specific tools and techniques. Today’s tech-nology offers two main technology options for surgeons performing extractions – laser and mechanical.
Laser extraction requires a 600 pound (250kg) stand alone unit to interface and power an SLS laser sheath, with each sheath requiring complex calibration before each use. Heavy machinery like this requires sup-port by way of annual maintenance and biomedical inspection as well as the require-ment to employ an on-site laser officer. Put simply, it’s bulky, costly both in terms of op-eration, training and maintenance. The other option is to use a mechanical ap-proach. This offers benefits in that it requires less surgical finesse and is more intuitive to use than laser powered systems. It is also de-signed to negotiate chronic, heavily fibrosed and calcified lesions without requiring the ‘brute strength’ of traction.
An enhanced mechanical extraction ap-proach doesn’t have the forward depth of cut like laser extraction sheaths. With this
in mind, mechanical extraction historically has had a lower adverse event rate than that experienced using powered sheaths.
Today’s mechanical lead extraction technol-ogy has been designed to be as intuitive as possible for the surgeon specialist during a procedure. Lead extraction, which goes a long way in addressing device-related com-plications, has progressed, particularly as clinicians are more aware of the risks and complications associated with some of the techniques previously used. Mechanical techniques allow for greater success rates, thus making the patient’s journey also a much safer and enjoyable one.
Devices like the EVOLUTION® Mechanical Dilator Sheath Set consists of a flexible rotating sheath that succinctly separates fibrous binding sites from the leads that need extracting. The inner, exotic braided polymer sheath, shielded by an out-er telescoping polymer sheath, connects to a handle, or trigger, which rotates it mechani-cally. It’s this mechanical trigger that allows
the user to better feel progress along the lead and through lesions, thereby maximising physician control.
While extraction of chronically implanted leads has been difficult in the past, this seems to have been addressed with mechani-cal techniques, which have been proven to remove the scar tissue along the vein that is often the primary reason for partial or failed removal of a lead.
An Exciting Evolution
Lead extraction device manufacturers have a responsibility to provide the best, most ver-satile devices that provide safe, timely and effective treatment for the patient, and are easy-to-use devices for surgeons. Addition-ally, the need to reduce the financial burden of acquiring the best possible technology on health organisations has to be reduced. It’s exciting to see the benefits that the lead ex-traction evolution will deliver to health pro-viders, doctors and patients.
CRM
CORONARY HEART ™ 1�

CONFERENCES
The combined Advanced Angi-oplasty and Left Main 6 plus meeting was held this January in the familiar surroundings of the
Hilton London Metropole Hotel in Pad-dington, with live cases broadcast on the first day from St Thomas’ Hospital, London. The outgoing British Cardiovascular Interven-tional Society (BCIS) President, Dr. Mar-tyn Thomas, led an invited panel of experts through the 3-day course of lectures, live cases, angio review sessions and up-to-date trial results, with an international line-up of speakers including Professor Martin Leon (Cardiovascular Research Foundation, New York), Dr. William Wijns (Aaalst, Belgium) and Professor Bernie Meier (Bern, Switzer-land). BCIS also welcomed to the Chair Dr. Mark de Belder, who takes over this year as President of the society at an important time in British cardiology. The review of drug-eluting stents by the National Insti-tute of Clinical Excellence (NICE), evolving nationwide training programmes for inter-ventional fellows, and the ongoing debate of service-provision for interventional services throughout the country have all been high-lighted as key issues which will dominate the political horizon in the forthcoming period.
BCIS was joined this year by members of the recently founded British Society of Endovascular Therapies (BSET). This pre-dominantly surgical-led body was founded in 2007 in response to the developing role
of percutaneous strategies to deal with pe-ripheral vascular pathologies. Ordinar-ily, surgeons of any denomination are only brought to this conference for the purpose of general bear-baiting, but the joint session on managing aortic dissection provided an excellent forum for promoting existing and future therapeutic strategies, and the need for closer collaboration between cardiolo-gists, vascular surgeons and interventional radiologists.
The Left Main 6+ live intervention cases were transmitted across the Thames from St Thomas’ Hospital, London, under the di-rectorship of Dr. Simon Redwood. He was joined by guest operators Dr. Keith Oldroyd (Glasgow), Dr. Adrian Banning (Oxford), Dr. David Hildick-Smith (Brighton) and Dr. Martyn Thomas (St Thomas’ London), with in-house support from Dr. Brian Clapp and Dr. Aldo Rinaldi. A total of five cases were broadcast, demonstrating a case mix of
Written by: Dr Ian WebbSt Thomas’ Hospital, London
Advanced Angioplasty and Left Main 6+ Course
1� CORONARY HEART ™

CONFERENCES
left mainstem lesions, complex bifurcation disease and rotablation-dependent revascu-larisation. A straw poll of delegates in one case presented strongly favoured surgical revascularisation over PCI – a first at a UK Advanced Angioplasty meeting! – but, ul-timately reflecting the complexity of cases now presenting to interventional cardiolo-gists.
The day proved a great success with all cases running smoothly and important discus-sion points raised in the areas of invasive coronary lesion assessment, evidence-based interventional strategy and complimentary pharmacological therapy. Commenting the following day on events, Dr Simon Redwood was quick to praise the skill and success of all the visiting clinicians in what was designed to be ‘a challenging and debatable forum’. He went on to highlight the ‘changing and increasingly complex anatomy presenting for percutaneous therapy in the present era’, and the current role of high-risk angioplasty in managing symptomatic patients turned down for surgery. Forthcoming data from Syntax, CARDia and other contemporary trials will hopefully provide further insight into these patient groups.
Keynote lectures were given by Dr. Wil-liam Wijns, co-Director of the Cardiovas-cular Centre in Aalst, Belgium, and current President of the European Association for Percutaneous Cardiovascular Interventions
(2006-2009), and Professor Martin Leon, Chairman Emeritus of the Cardiovascu-lar Research Foundation and Professor of Medicine at Columbia University Medi-cal Centre in New York. Dr Wijns gave an elegant summary of the role for drug-elut-ing stents in modern practice, highlighting some of the ongoing concerns regarding late in-stent thrombosis, optimum dura-tion of anti-platelet therapy and use in acute myocardial infarction. This subject was par-ticularly pertinent to UK cardiologists, of course, in advance of NICE’s final verdict on drug-eluting stents which was sched-uled for publication during the course of the meeting. Professor Leon was given the
broader remit of ‘Interventional Cardiol-ogy – the unanswered questions’, and did not fail in delivering a superb overview of both interventional coronary affairs as well as his experience and more recent advances in percutaneous aortic valve replacement. This theme was taken up later in the confer-ence by Dr. Martyn Thomas in a brief over-view of the UK centres currently providing percutaneous programmes. He predicted a significant expansion of services over the coming 5 years, but cautioned that progress ‘must be taken forward responsibly by the medical community together with ongoing support from Industry in order to advance this exciting technology safely for patients’.
Feeling the heat:Dr Keith Oldroyd from Glasgow during a
live case at St Thomas’ Hospital
CORONARY HEART ™ 1�

CONFERENCES
Professor Martin Rothman (London Chest Hospital) also provided an interesting and personal account of the development of percutaneous coronary intervention in the UK. This was particularly relevant as BCIS marks it’s 20th Birthday this year, of which Prof Rothman was a founding member and former President. He also paid respect to the late Dr.Raphael Balcon (formerly of the London Chest Hospital and BCIS Presi-dent, 1995-1997) and his significant contri-bution towards UK cardiology and coronary intervention.
Angiogram case-reviews continued to play an important educational role in the meeting, encouraging lively debate and discussion. The final session of the course was dedicated to four selected ‘Best of the Best’ registrar case reports, with exciting demonstrations of complex retrograde CTO revascularisation and laser angioplasty techniques. However, the judges’ prize was awarded to Dr. Cara Hendry (Manchester) and her presentation of a tricky coronary perforation in a heav-ily calcified LAD bifurcation lesion. She was awarded with sponsorship to this year’s TCT meeting in Washington and the chance to present her case again at the BCIS-spon-sored session.
This brought to a conclusion a very success-ful 2008 Advanced Angioplasty meeting, but concluding remarks were hastily interrupted by breaking news from Dr.Martyn Thomas that the NICE draft guidance on DES had just been published on-line, endorsing their continued use in the UK for coronary lesions of <3mm diameter and >15mm length, but only if the cost did not exceed £300 of a bare-metal stent. Whilst this news was par-ticularly well received by BCIS, which has worked so hard with other bodies to peti-tion NICE in the run-up to this judgement, it importantly excludes diabetic patients for which BCIS is now considering further ap-peal. This is likely to remain a key issue in the forthcoming year for UK intervention.
ADVANCED ANGIOPLASTY AND LEFT MAIN 6+ COURSE (cont...)
Having a joke with the audienceFrom left: Dr Keith Oldroyd, Dr Brian Clapp,
and Radiographer Rizwan Rashid
Master and Apprentice?Dr Martyn Thomas (left) with assistance
from Dr Simon Redwood (middle). Radiographer: Alex Harrington | Nurse: Richard Carrier
20 CORONARY HEART ™

ECHOCARDIOGRAPHY
Echotech Ltd was established in 2001 to provide echocardiography services to NHS patients across the UK in the community setting. This flexible, patient-led service depends on nine point-of-care ultrasound tools to assess patients in a variety of com-munity-based locations, delivering a rapid, quality-assured service that is drastically reducing echocardiography waiting lists.
Heart failure affects an average of eight people in every 1,000 of the UK population1 and studies have clearly demon-
strated that prevalence increases with age1,2. Once diagnosed, appropriate treatment and ongoing support can improve the quality of life for heart failure patients, and help to reduce morbidity and mortality.
Echocardiography provides a painless, non-invasive method to image the heart using ultrasound, giving detailed information on the structure of the heart and the direc-tion of blood flow through its chambers. Current echocardiography systems allow the function of the heart’s muscle tissue and blood flow to be objectively assessed with relative ease, and both the UK Depart-ment of Health3 and NICE guidelines4 require echocardiography to be carried out
on all patients with suspected heart failure. With many cardiology departments at full capacity, there are long waiting lists for these diagnostic procedures, however the NHS Improvement Plan5 pledges that, by the end of 2008, no one will wait longer than 18 weeks from GP referral to hospital treatment.
The Portsmouth-based company Echotech Ltd, which provides diagnostic services for patients with suspected heart failure in the community, offers a potential solution for this daunting target and its service model has real implications for the future of cardiology. By streamlining the diagnostic process, and using the latest technologi-cally advanced point-of-care visualisation tools, the company can reduce a hospital’s cardiology appointments to only those patients known to require specialist hospital services. NHS resources can be more cost-
effectively distributed, waiting times are drastically reduced and hospital doctors are able to concentrate on patient treatment.
Echotech depends on nine Sonosite Mi-croMaxx® ultrasound systems to provide high performance echocardiography within the primary care setting. The point-of-care systems offer sufficiently high quality imaging and resolution for thorough and accurate cardiac assessment6, and bring about massive cost-savings to the NHS, as a few machines can be used safely across a large number of sites. They also ensure the robustness, flexibility and reliability needed for the mobile service. Echotech records all scans using a medical DVD recorder that connects directly to the ultrasound system, allowing easy transfer of patient files to GPs or hospital cardiology departments as necessary.
Written by: Tracey Byard, SonoSite and Dominic Elton, Echotech.
Echocardiography in the community
- taking the strain off the NHS
CORONARY HEART ™ 21

ECHOCARDIOGRAPHY
22 CORONARY HEART ™
Keli Glover, Clinical Operations Direc-tor and cardiac physiologist at Echotech explained, “We provide echocardiography services to many regions across England, such as London, Portsmouth, the Isle of Wight, Worthing, East Surrey and the West Midlands. The service varies according to the primary care trust (PCT)’s require-ments. For example, we often provide clinics for open-access GP referrals: the GP refers the patient for the echo, which we carry out, then the report goes back to the GP. Alternatively, we provide cardiology clinics, where a cardiologist from the local hospital runs a clinic in the community and we provide echocardiography and electro-cardiograms for the patients before they go in to see the cardiologist.”
Echotech is exclusively contracted to the NHS and its British Society of Echocardi-ography-accredited cardiac physiologists ensure high standards of quality when investigating patients. “We use a variety of NHS centres within the community, and we have some mobile units that allow us to provide evening and weekend services, which make it easier for many younger patients to come to appointments,” Keli continued. “We have now scanned over 10,000 patients, and we see 90 per cent of our patients within 14 days of referral.”
After each patient investigation, Echotech sends a report that is made available to the referring clinician on the day of the scan, with details such as the degree of LV function (systolic and diastolic) and any other abnormality. Serious problems can be instantly dealt with by contacting the GP while the patient is present, for immediate follow-up or hospital admission if neces-sary.
Echotech’s service offers several benefits to patients and healthcare professionals, in particular by offering early and accurate diagnosis of heart failure, while simulta-neously helping to reduce waiting lists. Echotech allows the right patient to receive the appropriate treatment at the optimal time, improving health and helping with risk stratification such as early identifica-tion of those patients requiring specialist as-sessment. A proportion of the patients that Echotech has seen appear to have normal cardiac function and a recent audit of the company’s study database (cohort 10,000 patients) revealed that fewer than 20 per cent of investigations led to the patient requiring specialist referral, demonstrat-ing a significant sparing effect on NHS resources7.
Improved access to echocardiography may also result in higher rates of optimal pharmacological intervention8, such as with ACE inhibitors and beta-blockers, and could, as a consequence, lead to decreases in morbidity, mortality and hospital admis-sions9,10. Importantly, the service conforms to the NHS Plan11, which highlights the need to improve access to services by rede-signing care pathways around the needs and convenience of the patient.
“Previously, it could take up to a year for a patient to go from an initial GP’s referral for an echo to actually receiving the test results – which is far from ideal, particu-larly if the patient is seriously ill. All of our patients appreciate the fast turnaround
times and many of them feel more com-fortable coming to a local clinic or mobile unit than travelling to a large hospital. We recently carried out a survey of our patients in East London and found that the patients were 99 per cent happy with all aspects of the service, which is a brilliant outcome,” Keli added.
References
Majeed A, Williams J, de Lusignan S, et al. (2005) Management of heart failure in primary care after implementation of the National Service Framework for Coronary Heart Disease: a cross-sectional study. Public Health 119: 105-111.
Davis RC, Hobbs FD, Lip GY (2000) ABC of heart failure. History and epidemiology. British Medical Journal 320: 39-42.
Department of Health (March 2000) National Service Framework for Coronary Heart Disease: chapter 6, standard 11.
NICE Clinical Guideline 5 (July 2003) Chronic Heart Failure: Management of chronic heart failure in adults in primary and secondary care.
Department of Health (June 2004) The NHS Improvement Plan: Putting people at the heart of public services.
Senior R, Galasko G, McMurray JV, Mayet J (2003). Screening for left ventricular dysfunc-tion in the community: role of hand held echocardiography and brain natriuretic peptides. Heart 89(Suppl 3): iii24-iii28.
Catterall V. Echocardiography in primary care: evaluating an open access service. http://www.somerset-health.org.uk/pdf/ha_reports/echocar-diography.pdf
Lillis S, Vickers J. Assessment and treatment of heart failure in general practice. http://www.priory.com/fam/heart.htm
CIBIS II (1999) The cardiac insufficiency bisoprolol study II: a randomised trial. Lancet 353: 9-13.
SOLVD investigators (1991) Effect of enalapril on survival in patients with reduced left ven-tricular ejection fractions and congestive heart failure. New England Journal of Medicine 325: 293-302.
Department of Health (July 2000) The NHS Plan: A plan for investment, a plan for reform.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
ECHOCARDIOGRAPHY IN THE COMMUNITY (cont...)

MANAGEMENT
CORONARY HEART ™ 23
As manager of a multidisciplinary team of Cardiac Physiologists covering a wide range of diagnos-tic and interventions, there are
several areas that will impact on us in the future. I would like to highlight briefl y just three that I feel will impact on our depart-ment.
Firstly new innovations and techniques in Interventional Cardiology, such as Percu-tanoeus Aortic Valve Replacements will require even more of a multi-skilled work-force who can lay their hand to these many advancing techniques. Th e challenge for us is continue to build our multi-skilled team to provide adequate cover when the work demands it.
Secondly there is the ever growing need for fl awless Data Management. Th e ability
to view results of both diagnostic and in-terventional techniques is becoming even more common on both the ward and in out patients. Physicians are becoming increas-ingly reliant on fast and effi cient retrieval of results for planning patient management and of sharing of their working experiences. Th e challenges to provide this for us include securing funding to establish and maintain the data management, and to develop the time within the operational service to main-tain the system.
Th irdly I feel one of the greatest challenges to our department in the future is the re-
cruitment and retention of the workforce that have the necessary skills to achieve both the demand for shorter waiting lists and providing new skills to keep abreast of advancing technology. Our department sup-ports the recruitment and development of trainees utilising the local university Clinical Physiology Degree. For the existing work-force it is important to support Continual Professional Development by providing continuing CPD. Th is will ensure the devel-opment of new advancing techniques and also increasing workforce motivation that will hopefully leads to better retention of our existing physiologists.
Mrs Karen Nicholas,Clinical Manager,Cardiac Investigations Department,Heart and Lung Centre,New Cross Hospital.Wolverhampton.
Finger on the Pulse
Over the next few years what changes/developments do you believe will have the biggest impact to your cardiology department?What are you doing to address this?

MANAGEMENT
24 CORONARY HEART ™
How well I remember my Respiratory Therapist ex-perience with my first open heart. In 1973 at Wesley Medical Center in
Wichita, Kansas, I helped Cardiac Surgeon Dr. George Farha, remove the intubation tube on his post-op open heart patient. This began his patient’s successful recovery and their next step in care. This patient, along with all the other cardiac surgery and MI patients, stayed many days in the hospital recovering.
In late 1978 I moved on to a new career as a Physician Assistant assisting in open heart surgery. My first presentation as a CV Ad-ministrator, in 1986, was on Developing Ef-fective Product Lines in Cardiology for the American Hospital Association. I followed with two articles in 1992 on Managing the Cardiology Product Line.
The “Product Line Management” concept emerged in the healthcare industry in the early 1980s as an organizational effort to deal with prospective reimbursement, a tight economic environment and declining reve-nues, along with intense competition. Hos-pital executives needed a way to improve the cardiology business line. This management process for cardiology has gone through nu-merous promotion and role changes. In the late 1980s hospitals became overwhelmed with the assignment of DRGs, Diagnostic Related Groups the rise of managed care, integrated healthcare systems, restructuring, total quality management and cost reduc-tion, along with the need to build volume and thus profit.
Product Line management was not a new theme to the healthcare industry. Johns Hopkins Hospital, Baltimore, Md., turned to product line management in 1974. This 1,380 bed facility created clinical centers and called them “decentralized functional units.” St. Luke’s Hospital, Kansas City, MO., turned to product line management in 1983, when it restructured its depart-ments along specialty lines. Other organiza-tions have followed their product line man-agement techniques to better meet customer needs. I had administrative responsibility for the product line development at, East
Jefferson General Hospital; The Gulf South Heart Centre; Orlando Regional Medical Centre, Orlando, Florida; St. Joseph Re-gional Heart Centre, Albuquerque, New Mexico, and many others across the United States.
Now is the time to discuss the rapid evolu-tion and business success of this most dy-namic service. What unprecedented tech-nological breakthroughs! The business road to success and the increasing demands for service have made this world of cardiology a journey with many turns. The obstacles include increased competition, skyrocket-ing cost, decreasing revenue and the ever growing level of disease along with the new cardiac patients - here we come, the 1950s Baby Boomers.
In the 90s, as technological advances im-proved diagnostic and therapeutic capa-bilities, smaller hospitals were able to get into the cardiovascular business and com-pete more effectively with the full-service programs. Percutaneous and transcatheter interventions became standard in the 90s. Cardiac ERs and quick response teams in the field with Para-Medics changed the car-diac event. Acute MI to cath times were reduced and more patients were diagnosed needing intervention procedures.
Managing The Future of Cardiology
Written by: Robert D. Lunt, RRT., PA., MBA, President, The LUNT Group, Kansas City
- Past, Present And Future Of Healthcare’s Crown Jewel
Mr Robert Lunt

MANAGEMENT
CORONARY HEART ™ 25
All of these advancements, diagnostic and therapeutic, impacted on the complexity and patient mix of cardiovascular services.
The care model has developed into Pathways, and we move the CV patients quickly out of the hospital. Length of stays has dropped to amazing levels and the role of CV Product Line manager began to emerge to manage, market and promote their Heart Centre’s capabilities.
Out of the CABG Patch.
2007 marked the 30 years since the father of interventional cardiology, Dr. Andreas Gruentzig, performed the first coronary angioplasty. Today, cardiovascular services delivery represents a $300 billion plus per year industry; cardiovascular care remains the #1 service line of all medical/surgical in-stitutions throughout the US. However, the delivery of cardiovascular care is more com-plicated to organize that any other type of medical service. Looking back on the evolu-tion of cardiovascular services in the 1990s, we had a growth business on all fronts. As the disease care model increased, so did the number of diagnostic and treatment break-throughs that resulted in tremendous pro-
gramme growth. It used to be that most car-diovascular services were confined to tertiary settings.
2008 Strategic Perspective
Strong Medical Staff leadership is critical. CV service lines need strong medical lead-ers and champions, physicians willing to go face-to-face with their peers, challenge the status quo and support unpopular decisions. The CV service line administrator must de-velop strong relationships with physicians, sharing information and keeping them in the Business Loop.
Facilities
Major investments have been made in the Heart and Vascular Centers for faster serv-ices that achieve economies of scale and centralize CV services. The Heart Hospital, inside or attached to the medical centre, cre-ates and attracts physicians looking for better services delivery and optimized time. Ease of practice and state-of-the-art faculties are also key to attracting clinical staff when there are already critical shortages that are expected to worsen in the future. All one needs to do is
look at the new Heart and Vascular Centers that have recently opened or the ones that are on the drawing boards with full plans to be built or redesigned.
Human Capital
Attracting and retaining Physicians and Clinical Support Staff will be the most critical element; this major element must be monitored. Product Line managers must watch turnover and burnout. High demand physicians and group changes also are a ma-jor concern. Cardiologist and CV Surgeons are aging just like the rest of the 50s baby boomers. Planning for the CV MD staff-ing is strategic, as attractive new facilities and salary benefits are changing. High de-mand for specialists allied to short supply make this process a key concern that must be planned and managed.
Volume will continue to be the major in-dicator for service and patient mix, and for financial performance. Volume affects skill sets for physicians and staff, supports reten-tion and helps to monitor quality and out-comes. It certainly affects the financial per-formance and costs.

MANAGEMENT
26 CORONARY HEART ™
Running a service line
CV service line managers are not alone now. There are other service-line managers in Or-thopedics, Rehabilitation, Women’s Serv-ices, Children’s Services, Oncology Services and Neurology Services.
Future of Cardio-Vascular
A CV service provider must become unique. Do not let the past be the guide; it is a new business world of cost control, negative mar-gins and trends. You now need to manage “50,000 ft big picture” perspectives on the enterprise, and a 100 ft focused perspective for managing a service line day to day. It is a tough job. No “one size fits all” model works.
Good data and cost accounting systems should be put in place and costs must be watched. Share data with physicians on outcomes, cost, profit, market data, and referrals. It makes good sense to take CV services and run them as a Product Line. It has become a big business and Key Business Indicators must be monitored.
The new technology evolution:
Cardiovascular Information Systems (CVIS): merging data into images and networking it into CV-PACS. This new comprehensive imaging and information systems is grow-ing and will continue to grow. The need for more interconnected departments that move the CV information along will merge with the imaging needs. All this will help cardiologists and CV surgeons make clinical decisions through data mining.
The new cardiac leader:
Running a cardiovascular service line re-quires business tools and a tough decision maker to manage and build a business, make tough business decisions, utilize knowledge of market and business strategy and run at a profit. The difficulty with this is often the inability to make difficult but necessary de-cisions, and poor relationship building with physicians. Many organizations have yet to realize the value a good CV service line man-ager can bring to the organization. This is re-flected in the compensation offered, which is not consistent with the demands of the position. Many organizations also struggle to allow sufficient operating control for the CV manager. Control of decision making is
necessary to make a significant impact. The advantages of Service Line Management are demonstrated by: strong leadership, staying focused on strategy, and looking at both the local and global markets.
The disease is now the whole body…..the baby boomers are coming
Stents vs. Bypass Surgery will be the new review. The financial and clinical usage of stenting is reaching an impasse. The data supporting bypass surgery over stenting will begin to increase. The growing aging popu-lation will overwhelm the industry.
Hospitals will see the “sickest of the sick”. Planning on past performance will not be a good idea. Past growth and margins will not be the future experience. It will be neces-sary to keep the focused on strategic plans, ensure numbers are realistic, and watch costs and margins, which will be more negative.
It is an exciting time: Welcome to the ever-changing dynamic world of cardiovascular medicine and the CV healthcare market 2008 and beyond.
MANAGING THE FUTURE OF CARDIOLOGY (cont...)
Planning on past performance will not be a good idea. Past growth and margins will not be the future experience. It will be necessary to keep the focus on strategic plans, ensure numbers are realistic, and watch costs and margins, which will be more negative.

ECG
CORONARY HEART ™ 2�
ECG Quiz Answer from Page 8
The ventricular rate appears at fi rst sight fairly irregular and this could lead to a misdiagnosis of atrial fi brilla-tion. Atrial fi brillation is “irregularly irregular” i.e. cha-
otic whereas the QRS complexes in this ECG have an underly-ing order to them as they are instigated by a regular atrial rhythm. Discrete, identical and repetitive atrial depolarisations (marked as F for fl utter wave)
can be identifi ed. Th ese are conducted to the ventricular in a predominantly one to one fashion but with Wenkebach – oc-casional fl utter waves are not conducted as the atrial rate is just a fraction too fast for the AV node to conduct one to one. Th ere are groups of regular beats separated by longer intervals – this is sometimes referred to as “group beating”.
One to one (or near one to one) conduction of fl utter usual-ly occurs where the fl utter rate is slower than the typical 300 b.p.m. (as in this example). Th e rate may be slower due to anti-arrhythmic medication, slow atrial conduction or a grossly di-lated right atrium.
Th is tachycardia was terminated by ablation of the cavo tricus-pid isthmus (CTI) and was demonstrated to be counter clock-wise isthmus dependent fl utter. Th e patient had right atrial scars from previous surgical incisions but these were not implicated in the arrhythmia.
ECG Quiz Answer

SITE VISIT
2� CORONARY HEART ™
Kings College Hospital is recognised internationally as a world leading cardiac facility and is one of London’s largest
and busiest teaching hospitals. Opened in 1840 and today with 950 beds, Kings continues to expand with a new wing opened in 2003 by Her Majesty Th e Queen.
For those whom attended the Transcatheter Cardiovascular Th erapies (TCT) confer-
ence in 2007, you may have seen the live case telecast from here when the consultant cardiologist Dr Philip MacCarthy per-formed the fi rst coronary angioplasty using the Sprinter Legend Balloon Catheter from Medtronic.
Kings is also the fi rst lab in the UK to use the Edwards Lifesciences balloon for aortic valve stenosis. In August 2007, King’s staff carried out the fi rst two successful transapi-cal aortic valve replacements in the UK and
two percutaneous aortic valve replacements.
Th e department is also a central hub for patients coming from local district general hospitals and therefore a large portion of patients performed are extra complicated.
Special thanks must be given to Mr Greg Cuickshank, Radiographer Manager of the cath labs for answering the following questions.
Kings College Hospital
ADDRESS
MAP
Cardiac Cath LabKing’s College HospitalNHS Foundation TrustDenmark HillLondon SE5 �RSUnited Kingdom
Internationally Recognised
Kings College Cath Lab Team
Starting left foreground: Junior Sister Emma Saunders; Research Sister Michelle Andrews; Specialist Registrar Dr John Byrne; Cardiac Technician Raghunath Behera; Consultant
Cardiologist Dr Phil MacCarthy; Senior Radiographer Matt Trevail; Senior Sister Hannah Kent; Student Radiographer Tudor Kennard; Staff Nurse Zoe Duke; Cardiac Technician Sandip Vias; Junior Charge Nurse Jonathan Breeze; Staff Radiographer Fiona Desmond; Superintendent
Radiographer Greg Cruickshank; Junior Sister Maricel Paguyo; Staff Nurse Cristina Fernandez-Gonzales; Staff Nurse Lucy Barwick; Staff Nurse Rajashree Khandagale.

SITE VISIT
CORONARY HEART ™ 2�
Size of hospital and department:
King’s College Hospital is a 950 bed teach-ing Hospital in South East London. There are 3 labs; 1 EP and pacing, 2 are diagnos-tic and interventional. There is also mobile unit with floating table used for temporary pacing on our Coronary Care Unit.
Staff Numbers:
9 Nurses (currently only cover 4 on-call)
8 Cardiac Technicians,
1 fulltime Radiographer, 20 rotating Radiographers from Radiology Dept,
1 fulltime Radiography Assistant Practitioner.
Procedures:
Full range of diagnostic and interventional electrical and arterial procedures, as well as trans-apical and trans-femoral aortic valve replacements.
Procedures performed per year:
Approximately 3600 cases per year, includ-ing 1500 PCI’s, and 240 pacing devices.
Day Procedures:
Yes, routine elective diagnostic and inter-ventional coronary procedures as well as EP cases.
Equipment:
Two Philips Allura Flat Panel labs
1 Siemens Coroskop lab
1 Siemens Cathcor Haemo-dynamic system
2 Axiom Sensis Haemo-dynamic systems
•
•
•
•
•
•
•
•
Radi Pressure Wire facilities in both Interventional labs
3 IVUS machines
1 Ziehm Vista Mobile Image Inten-sifier and mobile floating table top examination couch used in Coronary Care Wing for temporary pacing cases.
Haemostasis Management:
Angioseals, occasionally Star-close, digital pressure and Fem-stops.
New procedures implemented:
Trans-femoral and trans-apical aortic valve replacements.
Cross-Training of staff:
There is overlap between the 3 support staff groups. For on-call purposes, each role can
•
•
•
be covered by at least one other Health Pro-fessional or Medic, so we can start urgent cases when Consultant Cardiologist and 3 of the following four staff are in; Specialist Registrar, Radiographer, Cardiac Technician and Nurse. Note this is done only in the case of absolute necessity – not done rou-tinely.
Inventory Management: Materials management for most products. Drug eluting stents + other irregularly used products are ordered by nursing staff. We use the pen and paper method however will be investigating other options soon.
Alliances with other hospitals for treatment of patients:
We have close relationships with a number of local district general hospitals and per-form procedures on a treat and return/keep/discharge basis.
Cath Lab Control RoomCardiac Tech Sandip Vias (back turned) and Staff Radiographer Fiona Desmond

SITE VISIT
30 CORONARY HEART ™
Challenges:
Recruitment and retention of staff, as London becomes a more expensive place to live.
Big increase in emergency out of hours work over the past two years.
Increase in complexity of cases.
•
•
•
Training for new employees:
Radiographers: Full training in all aspects of Cardiac Radiography from scratch.
Nurses: Cardiac rotation involving all car-diac departments over the course of a week, supernumerary status for two weeks, full mentorship support until scrubbing inde-pendently, shadow on-calls until compe-tent/confident to do on-call independently.
Continuing education programs for staff: In-house weekly cardiac teaching sessions with Practice Development Nurse, regular morning industry training sessions, access to national conferences/study days, access to KCL post-registration courses/study days, mandatory in-house training, other in-house professional development courses. Also weekly 1 hour talks by SHO’s, and monthly Journal club.
Competency checks for staff:
Radiographers: have bi-annual competen-cy checks signed off in all areas.
Nurses: extensive trust-wide nursing com-petency document that is regularly updated and reviewed. On-call competency check-list.
Training facility for cardiac registrars:
Yes
Private cases:
Yes, private cases are fitted in around NHS patients when done. The hospital has one private ward however we limit cases to two per session.
What is the best part of working at your facility?
Friendly department, with a patient focused approach, at the cutting edge of Cardiol-ogy.
KINGS COLLEGE HOSPITAL (cont...)
Staff Nurse Zoe Duke (foreground) and Dr Phil MacCarthy

EDUCATION
CORONARY HEART ™ 31
Beep beep beep. It’s 3 am and your pager is going off again. It’s Dr. Bound’s patient in the Emergency Department (ED). You call for a report: 60 year old woman, chest pain 10/10, ST elevations in the ante-rior leads, hemodynamically unstable with a heart rate of 110 and BP of 90/50. She has no previous cardiac history. Th e ED says, “She doesn’t look good, she’s cool and clam-my, nauseated and short of breath.”
You know this is a typical presentation for a patient with myocardial infarction. But do you know the physiology behind the presentation? You anticipate the need for blood pressure (BP) support, and you know dopamine and Neosynephrine® -- aka phenylephrine -- both support BP. But do you know how these drugs work and why one may be a better choice in a given set of circumstances?
Aspirin has been given, but what other an-tithrombotic medications should be used? How do these meds actually work? How does the physician choose among the agents available? And what are the latest Ameri-can College of Cardiology/American Heart Association guidelines for antithrombotic therapy?
In a fi eld changing as fast as ours, it’s never been more important to keep up-to-date on the answers to these questions. And that’s the goal of this article: to give members of the cath lab team a better understanding of symptom presentation and the mechanisms of action of the hemodynamic support drugs commonly used in the cath lab. We’ll also review the major antithrombotic medi-cations, their modes of action, and 2007 ACC/AHA recommendations.
To understand the why of the medications we give, we’ll start with a short physiology refresher in Part I. Part II will cover the medications themselves, their actions and indications.
All about the Autonomic Nervous System
Th e autonomic nervous system (ANS) provides an autoregulatory function to maintain the body’s hemodynamic homeos-tasis. Th ese maintenance activities are pri-marily performed without conscious control or sensation: we don’t need to consciously think about breathing or making our hearts beat.
Much of this regulatory function is located in the medulla oblongata in the brain stem. Th is explains why patients who are declared brain dead continue to have a heartbeat, and why other elemental body functions remain intact: they’re regulated by the autonomic nervous system and don’t require the higher brain function of conscious thought in or-der to continue.
Th e ANS has two opposing (or complimen-tary) divisions: the sympathetic and para-sympathetic systems. Th e sympathetic sys-tem provides the “fi ght or fl ight” response when immediate action is required: it’s the gas pedal. Th e parasympathetic system is the “rest and digest” mechanism. It calms our nerves and slows things down. It’s the brake pedal.
By Charlene Shellenberger, BS, RN, Clinical Education Specialist,
Healthworks, Inc.
And The Beat Goes On… - A Review of Lifesaving and
Antithrombotic Drugs
Part 1 of a Two-Part Series

EDUCATION
32 CORONARY HEART ™
All about the Sympathetic Nervous System
The sympathetic nervous system’s “fight or flight“ response is often explained as an evo-lutionary protective mechanism that devel-oped to help us escape the saber-tooth tigers that were chasing us. Although we’re no longer being chased by tigers, the stressors of modern life stimulate our sympathetic nerv-ous system and cause catecholamine release.
The catecholamines and neurotransmitters of the sympathetic system, noradrenalin (norepinephrine) and adrenalin (epine-phrine) have specific receptor sites and elicit a specific response. The sympathetic receptors are alpha, beta (1 and 2) and dopaminergic. Refer to Figure 1.
Alpha receptors are located in peripheral arteries. When stimulated, they cause vaso-
constriction, thereby increasing blood pres-sure and systemic vascular resistance (SVR). Think of water running through a pipe four inches in diameter: if the amount of water remains the same but the pipe is now only two inches in diameter, the water pressure will be greater.
A common cath lab drug that exhibits pure alpha effects is Neosynephrine®(phenylephrine). This is an alpha agonist that raises blood pressure without causing an increase in heart rate. It’s typically the drug of choice in septic shock when the patient has a heart rate of 120 and BP of 80/40.
Other vasopressor agents like dopamine have both alpha and beta 1 properties. They cause an increase in heart rate as well as BP, thereby increasing myocardial oxygen de-mand. So if our patient is in cardiogenic shock with a heart rate of 40 and a BP of
80/40, dopamine is a logical choice as a va-sopressor since it supports blood pressure and augments the heart’s pumping capabil-ity,
Helpful hint: Before any form of va-sopressor is administered, the patient should be adequately hydrated: it’s counterproductive to squeeze an empty container. Remember: without adequate hydration (preload) we can’t attain the stretch on the muscle fibers of the heart. And that can lead to inadequate pump-ing. Starling’s Law of the Heart states that increasing the stretch on muscle fib-ers will increase the force of contraction. Think of it as a rubber band: the farther you pull it back (or stretch it) the farther it will fly (and the more it stings if it hits you!).
Sympathetic Receptors
Alpha
Located in peripheral arteries
Beta 1
Located in the heart
Beta 2
Located in the lungs and arterial walls
Dopaminergic
VasoconstrictionIncrease in heart rate
Bronchiolar dilation arterial vasodilation
Located in coronary arteries, renal & mesenteric blood
vessels
Increase in arterial pressure
Increases contractility,
conduction, and irritability
DilationKidneys
Mesenteric
Figure 1: Sympathetic Receptors
AND THE BEAT GOES ON (cont...)

EDUCATION
CORONARY HEART ™ 33
Beta 1 receptors are located within the myocardial tissues of the heart. Stimula-tion of these receptors causes an increase in heart rate (chronotrophy) and contractility (inotrophy). The increase in heart rate and contractility causes a subsequent increase in cardiac output, with the unwanted side effect of increased myocardial irritability (think arrhythmias).
Isuprel® (isoproterenol hydrochloride) is a medication with pure beta properties to increase heart rate and contractility. It’s commonly utilized as an ectopy stimulating agent in electrophysiology studies, thereby earning its reputation as a “chemical pace-maker.” It also demonstrates the beta 2 properties of vasodilatation, which can lead to a drop in blood pressure.
In contrast, Levophed® (norepinephrine) is a drug with both alpha and beta proper-ties. It increases BP, systemic vascular resist-ance (SVR), cardiac output and heart rate. It provides excellent hemodynamic support in critically ill patients.
Beta 2 receptors, located in the lungs, cause bronchodilatation and arterial dilatation when stimulated. Albuterol and terbuta-line -- two types of prescribed inhalers -- are beta 2 agonists used to treat bronchos-pasm in patients with chronic obstructive pulmonary disease (COPD).
As we’ve already noted, beta 1 stimulation works on the heart. And that’s why, when a patient receives a respiratory treatment, his heart rate increases. In most nebulized agents, the medication contains both beta 1 and beta 2 agonists. So we end up with nicely opened lower airways, but an in-creased heart rate compared to baseline.
Dobutrex® (dobutamine), which is used for heart failure patients, has both beta 1 and beta 2 properties. The beta 1 side increases contractility, or positive inotropic effect, to improve cardiac output, while the beta 2 arterial dilatation effect causes a decrease in preload and afterload. In other words, the two-inch pipe is now four inches.
This reduction in afterload yields less pres-sure for a failed heart to pump against, de-
creasing its workload while simultaneously increasing its ability to contract.
Helpful hint for remembering receptor sites: you have one heart: so beta 1. You have two lungs: thus beta 2.
Beta blockers are an entire class of medi-cations dedicated to blocking beta receptor sites. They’re routinely indicated for acute coronary syndrome (ACS) patients. Beta blockers decrease cardiac arrhythmias, heart rate and blood pressure, thereby decreasing myocardial oxygen demand. For this rea-son they’re also used for blood pressure and heart rate control.
Helpful hint: beta blockers should be used with caution in patients with COPD and asthma: remember if you block beta 2, bron-chodilitation bronchospasm could be life-threatening in the presence of beta blockade. Beta blockers should not be used in the pres-ence of any atrioventricular (AV) block.
Another example of beta blockade: when one of my friends has to speak publicly, she develops a redness that begins at her chest and incrementally creeps up her neck to her face. It looks as if her heart is literally pounding out of her chest! People like her
benefit from prophylactic beta blockade: she took Inderal® (propanolol) before mak-ing speeches and also before her wedding.
Lopressor® (metropolol) is the beta blocker most commonly administered to patients in the cath lab or ED as part of the acute coro-nary syndrome (ACS) protocol.
Helpful hint for remembering which meds are beta blockers: most end in “lol.”
Now that we’ve explored the sympathetic receptors and actions of alpha and beta stimulation, it’s clear why epinephrine -- a sympathomimetic drug -- is the first-line advanced cardiac life support (ACLS) medi-cation. Let’s assume your patient has cardiac-ar-rested: there’s no perfusing rhythm, no BP, no cardiac output. Epinephrine will vaso-constrict peripheral arterioles and venules, shunt peripheral blood back to the heart in an attempt to raise blood pressure/systemic vascular resistance, and stimulate the beta properties of increasing heart rate and stroke volume.
Epinephrine is also the first-line treatment for anaphylaxis, either in the cath lab for contrast allergy, or as an Epi-Pen® for people who are allergic to bee stings.
Generic Brand Name
Metropolol Lopressor®
Labetelol Trandate®
Esmolol Breviblock®
Propanolol Inderal®
Atenolol Tenormin®
Sotalol Betapace®
Figure 2: Commonly Used Beta Blockers

EDUCATION
34 CORONARY HEART ™
Dopaminergic receptors, located in coro-nary arteries and renal and mesenteric blood vessels, cause dilation of kidney and me-senteric arteries.
Inotropin® (dopamine) is one medication with dose-dependent action. At low dose (0.5-2 mcg/kg/min), dopaminergic recep-tors are stimulated and renal perfusion is increased. At median dose range (2-10 mcg/kg/min), Inotropin exerts beta effects of in-creased heart rate and contractility. At the highest doses,(>10mcg/kg/min), the effect is alpha, with peripheral vasoconstriction that raises blood pressure. At this dose Inotropin
will have vasopressor, inotropic and chrono-tropic effects and may increase myocardial oxygen demands on the heart.
Helpful hint: if an IV line infiltrates with Inotropin it can cause sloughing of the skin due to its alpha peripheral constrictive properties. To prevent tissue necrosis, treat as soon as possible with a Regitine® (phentolamine mesylate) in-jection around the periphery of the in-filtration.
A sympathetic wrap-up. Think about the appearance and vital signs of acute MI pa-tients: they’re afraid they’re going to die, so their “fight or flight” response is stimulated and their sympathetic system is in over-drive.
This is first evidenced by cool, clammy skin caused by alpha stimulation and peripheral vasoconstriction: that’s why their skin is cold, not hot. They may even have a gray or ashen color.
Second, their heart rate (HR) is elevated in part by beta 1 stimulation. The infarcted
The Autonomic Nervous System
Structure Sympathetic Stimulation Parasympathetic Stimulation
Iris (eye muscle) Pupil dilation Pupil constriction
Salivary Glands Saliva production reduced Saliva production increased
Oral / Nasal Mucosa Mucus production reduced Mucus production increased
Heart Heart rate and force increased Heart rate and force decreased
Lung Bronchial muscle relaxed Bronchial muscle contracted
Stomach Peristalsis reducedGastric juice secreted; motility increased
Small Intestine Motility reduced Digestion increased
Large Intestine Motility reduced Secretions and motility increased
LiverIncreased conversion of glycogen to glucose
Kidney Decreased urine secretion Increased urine secretion
Adrenal MedullaNorepinephrine and epinephrine secreted
Bladder Wall relaxed and sphincter closedWall contracted and sphincter relaxed
Figure 3: The Autonomic Nervous System
AND THE BEAT GOES ON (cont...)

EDUCATION
CORONARY HEART ™ 35
portion of the myocardium (the ventricular muscle mass) results in a diminished ability to pump effectively, decreasing the stroke volume (SV) and myocardial oxygen sup-ply.
Our bodies work hard to maintain home-ostasis and adequate cardiac output (CO). The equation CO = HR x SV says that or-gan perfusion pressure or blood pressure must remain adequate to perfuse the brain, heart and major organs. If there’s a drop in stroke volume due to myocardium injury, heart rate must increase to compensate for the decreased stroke volume.
Oxygen is required each time the heart beats. A compromised myocardium is al-ready in oxygen deficit, and an increase in heart rate from beta stimulation puts further oxygen demands on the heart. That’s why your acute MI patient benefits from the ad-ministration of a beta blocker like Lopres-sor®: the beta-blocking action lowers the heart rate, allows for more ventricular filling time, decreases myocardial oxygen demand, improves cardiac output, and may help with arrhythmia suppression.
All about the Parasympathetic Nervous System
The parasympathetic nervous system is the “rest and digest” or “feed and breed” part of the autonomic nervous system. The parasympathetic system innervates the heart via the vagus nerve, or cranial nerve X. The neurotransmitter responsible for parasym-pathetic stimulation is acetylcholine.
This innervation is limited to the sinoatrial
(SA) node and the atrioventricular (AV) junction. There’s very little influence on the ventricles or blood vessels. Parasympa-thetic stimulation causes a decrease in heart rate and impulse conduction in the heart. Figure 3 details parasympathetic effects else-where in the body.
We see the effect of stimulation of the para-sympathetic system in the cath lab and recov-ery area every day. It may happen when the physician is gaining vascular access, sheaths are being pulled, or pressure is being applied to the groin. The heart rate drops and BP falls. The patient becomes diaphoretic and nauseated. And we say the patient is having a vagal response.
What should we do first? Administer a drug to block the parasympathetic stimulation. The drug of choice is atropine, a parasym-pathetic blocker. Atropine is usually dosed at 0.5-1 mg IV per physician’s order (A caution: doses of less than .5 mg or more than 2.5 mg can cause a third-degree heart block).
This is why having atropine readily available at the bedside is part of many institutions’ sheath-pulling policies. It should be the first mode of action in a vagal response, followed by placing the patient in Trendelenburg po-sition and fluids.
Remember groin anatomy of nerve (vagus), artery, vein, ligament. Releasing pressure is not an option until hemostasis is accom-plished. Atropine is indicated in sympto-matic bradycardia, asystole, and pulseless electrical activity (PEA). Patients who re-ceive atropine will experience dry mouth and pupil dilatation.
You’ll be interested to learn that atropine occurs naturally in the deadly nightshade plant, or Atropa belladonna. The plant gets its name from the Italian word for “beautiful lady” (bella donna): Renaissance-era women used an extract of its berries to dilate their pupils for cosmetic reasons. And US sol-diers carry atropine as the antidote for nerve gas exposure.
In Part II in the next issue we’ll re-view the major antihrombotic medi-cations, their mode of action, and 200� ACC/AHA recommendations. And we’ll find out what happened to the patient we talked about at the beginning of this article.
Editor’s Note: The information presented in this article is intended to serve as an ed-ucational aid only and provide the reader with a reference; it is not intended to of-fer medical advice nor substitute medical practice, diagnosis and/or treatment. The ultimate responsibility for patient care resides with the health care professional using his or her professional license, ex-perience, and knowledge of the patient. All products are registered trademarks by their respective manufacturers, and are approved for use in the United States. Please check with your local government or regulatory agency for additional infor-mation. Dosing and/or pricing informa-tion is direct from manufacturers; please consult with appropriate package inserts or information before administering any medication or pharmacologic agent listed in this article.
All references used for this series will appear in Part 2 of this series.
You’ll be interested to learn that atropine occurs naturally in the deadly nightshade plant... The plant gets its name from the Italian word for “beautiful lady.”

PRESCRIBING INFO
36 CORONARY HEART ™
PRESCRIBING INFORMATION VISIPAQUE™ iodixanolPlease refer to full national Summary of Product Characteris-tics (SPC) before prescribing. Indications and approvals may vary in diff erent countries. Further information available on request.
PRESENTATIONAn isotonic, aqueous solution containing iodixanol, a non-ionic, dimeric contrast medium, available in three strengths containing either 150 mg, 270 mg or 320 mg iodine per ml.
INDICATIONSX-ray contrast medium for use in adults in cardioangiography, cerebral angiography (conventional and i.a. DSA), peripheral arteriography (conventional and i.a. DSA), abdominal angiog-raphy (i.a. DSA), urography, venography, CT enhancement, studies of the upper gastrointestinal tract, arthrography, hys-terosalpinography (HSG) and endoscopic retrograde cholan-giopancreatography (ERCP). Lumbar, thoracic and cervical myelography in adults.In children for cardioangiography, urography, CT enhance-ment and studies of the upper gastrointestinal tract.
DOSAGE AND ADMINISTRATIONAdults and children: Dosage varies depending on the type of examination, age, weight, cardiac output, general condition of patient and the technique used (see SPC and package leafl et).
CONTRAINDICATIONSManifest thyrotoxicosis. History of serious hypersensitivity re-action to VISIPAQUE.
WARNINGS AND PRECAUTIONSA positive history of allergy, asthma, or reaction to iodinated contrast media indicates need for special caution. Premedica-tion with corticosteroids or H1 and H2 antagonists might be considered in these cases. Although the risk of serious reactions with VISIPAQUE is regarded as remote, iodinated contrast media may provoke serious hypersensitivity reactions. Th ere-fore the necessary drugs and equipment must be available for immediate treatment. Patients should be observed closely for at least 15 minutes following administration of contrast medium, however delayed reactions may occur. Non-ionic contrast media have less eff ect on the coagulation system in vitro, compared to ionic contrast media. When per-forming vascular catheterization procedures one should pay meticulous attention to the angiographic technique and fl ush the catheter frequently (e.g. with heparinised saline) so as to minimize the risk of procedure-related thrombosis and embo-lism. Ensure adequate hydration before and after examination
especially in patients with renal dysfunction, diabetes mellitus, paraproteinemias, the elderly, children and infants. Particular care is required in patients with severe disturbance of both re-nal and hepatic function as they may have signifi cantly delayed contrast medium clearance. For haemodialysis patients, correla-tion of time of contrast media injection with the haemodialy-sis session is unnecessary. To prevent lactic acidosis in diabetic patients treated with metformin, administration of metformin should be discontinued at the time of administration of con-trast medium and withheld for 48 hours and reinstituted only after renal function has been re-evaluated and found to be nor-mal. (Refer to SPC). Special care should also be taken in pa-tients with hyperthyroidism, serious cardiac disease, pulmonary hypertension, patients predisposed to seizures (acute cerebral pathology, tumours, epilepsy, alcoholics and drug addicts), and patients with myasthenia gravis or phaeochromocytoma. One should also be aware of the possibility of inducing transient hypothyroidism in premature infants receiving contrast media. All iodinated contrast media may interfere with laboratory tests for thyroid function, bilirubin, proteins, or inorganic substanc-es (e.g. iron, copper, calcium, and phosphate). An increased risk of delayed reactions (fl u-like or skin reactions) has been associated with patients treated with interleukin-2 up to two weeks previously.
PREGNANCY AND LACTATIONTh e safety of VISIPAQUE in pregnancy has not been estab-lished. Contrast media are poorly excreted in breast milk and minimal amounts are absorbed by the intestine. Breast feeding may be continued normally.
UNDESIRABLE EFFECTS Intravascular use: Usually mild to moderate, and transient in nature. Th ey include discomfort, general sensation of warmth or cold, pain at the injection site or distally. Serious reactions and fatalities are only seen on very rare occasions. Nausea and vomiting are rare, and abdominal discomfort is very rare. Hy-persensitivity reactions occur occasionally with symptoms such as rash, urticaria, erythema, pruritus, dyspnoea or angioedema (immediate or delayed). Hypotension or fever may occur. Severe reactions such as laryngeal oedema, bronchospasm, pulmonary oedema and anaphylactic shock are very rare. Neurological reac-tions such as headache, dizziness, seizures, and transient motor or sensory disturbance (e.g. taste or smell alteration) are very rare. Also reported very rarely: vagal reactions, cardiac arrhyth-mia, depressed cardiac function, ischaemia, and hypertension. “Iodide mumps” is a very rare complication. Arterial spasm may follow injection into coronary, cerebral or renal arteries. A minor transient rise in S-creatinine is common. Renal failure is very rare. Post phlebographic thrombophlebitis or thrombosis
is very rare. Arthralgia is very rare. Severe respiratory symptoms and signs (including dyspnoea and non-cardiogenic pulmo-nary oedema), and cough may occur. Intrathecal use: Mening-ism, photophobia or chemical meningitis. Transient motor or sensory dysfunction. Confusion. Paraesthesia. Seizures. EEG changes. Local pain. Headache, nausea, vomiting or dizziness.Use in body cavities: Endoscopic Retrograde Cholangiopan-creatography (ERCP): Elevation of amylase levels, pancreatitis. Oral use: diarrhoea, nausea, vomiting, abdominal pain. Hyster-osalpingography (HSG): Transient pain in the lower abdomen. Vaginal bleeding/discharge, nausea, vomiting, headache, fever. Arthrography: Pressure sensation and post procedural pain.
PHARMACODYNAMIC PROPERTIES.In 64 diabetic patients with serum creatinine levels of 115 - 308 µmol/L, VISIPAQUE use resulted in 3% of patients ex-periencing a rise in creatinine of ≥ 44.2 µmol/L and 0% of the patients with a rise of ≥ 88.4 µmol/L.Th e release of enzymes (alkaline phosphatase and N-acetyl-ß-glucosaminidase) from the proximal tubular cells is less than after injections of non-ionic monomeric contrast media and the same trend is seen compared to ionic dimeric contrast media. VISIPAQUE is also well tolerated by the kidney.
INSTRUCTIONS FOR USE AND HANDLINGLike all parenteral products, VISIPAQUE should be inspected visually for particulate contamination, discolouration and the integrity of the container prior to use. Th e product should be drawn into the syringe immediately before use. Containers are intended for single use only, any unused portions must be discarded. VISIPAQUE may be warmed to body temperature (37°C) before administration.
MARKETING AUTHORISATION HOLDER GE Healthcare AS, Nycoveien 1-2, Postboks 4220 Nydalen, N-0401 Oslo, Norway.
CLASSIFICATION FOR SUPPLYSubject to medical prescription (POM).
MARKETING AUTHORISATION NUMBERSPL 0637/0017-19 (Glass vials/bottles and polypropylene bot-tles with stopper and screw cap) PL 0637/0026-28 (Polypropylene bottles with a twist-off top)
DATE OF REVISION OF TEXT19 October 2007
PRICEVisipaque 320mgI/ml, 10x50ml: £246.03
Niopam® Iopamidol
Abbreviated Prescribing Information - for full prescribing information, including side eff ects, precautions and contra-indications, see Summary of Product Characteristics (SPC).
Presentation: Aqueous sterile solution of iopamidol. Niopam 150, iopamidol 30.62% w/v (150mg iodine/ml); Niopam 200, 40.8% w/v (200mg I/ml): Niopam 300, 61.2% w/v (300mg I/ml); Niopam 340, 69.4% w/v (340mg I/ml); Niopam 370, 75.5% w/v (370mg I/ml). Uses: X-ray contrast medium. Dosage and Administration: Do not exceed 250 ml. Myelography: Niopam 200, 5-15ml or 300, 5-10ml; Angiog-raphy and Arteriography: Niopam 300, 340 or 370, dosage according to procedure (see SPC); DSA Niopam 150, 340 or 370, dosage according to procedure; CT Niopam 200, 300 or 340, 40-100ml; IV urography: Niopam 300, 340 or 370, 40-80ml (up to 1.5ml/kg); Arthrography: Niopam 300 or 340, 1-10ml. Children: according to procedure, body size and age (see SPC). Elderly: as for adults; use lowest eff ective dose.Contra-indications: Hypersensitivity to iodine. Do not imme-diately repeat myelography. Precautions and Warnings: Resus-citative measures should be available. Observe patients for at least one hour after treatment. Care in the elderly and patients with history of allergy, asthma, increased intracranial pres-sure, suspected intracranial tumour, abscess or haematoma, severe impairment of liver, kidneys or myocardium, chronic alcoholism, multiple sclerosis, Waldenströms macroglobuli-naemia, myeloma, epilepsy, diabetes, pulmonary hyperten-sion, hyperthyroidism, myasthenia gravis, Graves’ disease. Correct abnormalities of fl uid and electrolytes, particularly in small children, babies and renal impairment. During
cardiac procedures ventricular arrhythmias may frequently occur. Angiography: right heart insuffi ciency and pulmo-nary hypertension may precipitate bradycardia and systemic hypotension (ensure proper catheter placement). Sickle cell disease: iv injection may promote sickling in homozygotes. Phaeochromocytoma: iv administration may cause severe hypertensive crisis (pre-medicate with an alpha blocker). Avoid in homocystinuria, thromboangiitis obliterans or ascending infections with ischaemia. Possible interference with tests of thyroid function and for bilirubin, proteins, inorganic substances. To minimise risk of thromboembolism, avoid con-tact with blood in the syringe; fl ush catheters frequently. Do not mix with other drugs. Venography: caution in suspected phlebitis, serious ischaemia, local infections, complete venous occlusion. Urography: care in patients with impaired renal function. Check thyroid function in neonates after adminis-tration. Pregnancy and Lactation: If possible, use only during the pre-ovulation phase of the menstrual cycle; avoid during pregnancy. Only use during lactation if essential. Interactions: Vasopressors potentiate the neurological eff ect of intra-arte-rial contrast media. Papaverine: interaction may cause arterial thrombosis. Metformin: stop at the time of examination; reinstate after renal function is normal. Avoid neuroleptics, analgesics, anti-emetics, antihistamines, phenothiazine-type sedatives. Anticonvulsants should not be discontinued. Side Eff ects: Nausea, vomiting, erythema, heat sensation, fever, sweating, headache, rhinitis, laryngeal oedema, asthenia, dizziness, pallor, dyspnoea, hypotension, rash and blisters. Occasionally, anaphylaxis or other manifestations of allergy (may take up to several days to develop). Reactions involving cardiovascular system (vasodilatation with hypotension, tachy-cardia, dyspnoea, agitation, cyanosis, loss of consciousness). Infrequently, ventricular arrhythmias during intracardiac
and/or coronary arteriography. Rarely, myocardial ischaemia, infarction, cardiac failure/arrest, Steven-Johnson syndrome, renal impairment, thrombocytopenia, asthma, pulmonary oedema, recurrence of hyperthyroidism in patients treated for Graves’ disease. After cerebral angiography: confusion, stupor, coma, paresis, (transient) cortical blindness, convulsions may occur. In myelography: rarely, seizures, transient confusion or transient motor or sensory dysfunction, meningism and men-ingitis (consider possibility of infection), headaches, dizziness, nausea, vomiting, pain in limbs, back or neck. Local pain and swelling at injection site may occur. Overdose: Support vital functions, maintain hydration. Iopamidol is haemodialyzable. Pharmaceutical Precautions: Protect from light. Discard if solution contains particulate or crystalline matter. Use imme-diately after opening. Discard unused solution. Avoid contact with metallic surfaces containing copper. Legal Category: POM. Authorisation Numbers: Niopam 150 PL 18920/0007; Niopam 200 PL 18920/0008; Niopam 300 PL 18920/0009; Niopam 340 PL 18920/0010; Niopam 370 PL 18920/0011. NHS list prices per single unit: Niopam 150 50ml vial £10.00; Niopam 200 50ml vial £12.00; Niopam 300 50 ml vial £18.00; Niopam 340 50ml vial £21.00; Niopam 370 50 ml vial £23.00. Full prescribing information is available on request from Bracco UK Ltd, Bracco House, Mercury Park, Wycombe Lane, Wooburn Green, High Wycombe, Bucks HP10 0HH, United Kingdom. Date of preparation: December 2007.
Information about adverse event reporting can be found at www.yellowcard.gov.uk. Adverse events should also be reported to Bracco on 01628 851500.
BUK120703
Refer to pages 14-15

PRESCRIBING INFO
CORONARY HEART ™ 3�
PRESCRIBING INFORMATION OMNIPAQUE™ (io-hexol) Please refer to full national Summary of Product Characteris-tics (SPC) before prescribing. Indications and approvals may vary in diff erent countries. Further information available on request.
PRESENTATION Aqueous solution for injection containing iohexol, a non-ionic, monomeric, triiodinated X-ray contrast medium, and available in fi ve strengths containing either 140 mg, 180 mg, 240 mg, 300 mg or 350 mg iodine per ml.
INDICATIONS X-ray contrast medium for use in adults and children for urography, phlebography, i.v. DSA, CT, arteriogra-phy, cardioangiography and i.a. DSA. Myelography. For use in body cavities: Arthrography, ERP/ERCP, herniography, hyste-rosalpingography, sialography and use in the G-I tract.
DOSAGE AND ADMINISTRATIONS Adults & children: Dosage varies depending on the type of examination, age, weight, cardiac output and general condition of patient and the technique used (see SPC and package leafl et).
CONTRAINDICATIONS Manifest thyrotoxicosis. History of serious reaction to OMNIPAQUE.
WARNINGS AND PRECAUTIONS Allergy, asthma, or pre-vious reactions to contrast media are risk factors for develop-ing hypersensitivity reactions/anaphylactic reactions. Necessary drugs and equipment must be available for immediate treat-ment, should a serious reaction occur. It is advisable always to use an indwelling cannula or catheter for quick intravenous access throughout the entire X-ray procedure. After contrast medium administration the patient should be observed closely for at least 15 minutes, since the majority of serious side eff ects occur within this time. However, delayed reactions may occur. To prevent acute renal failure, special care should be exercised in patients with preexisting renal impairment, diabetes melli-tus, paraproteinemias (myelomatosis and Waldenström’s mac-roglobulinemia), dehydrated patients, or patients who receive concurrent treatment with nephrotoxic drugs. To prevent lactic acidosis in diabetic patients treated with metformin, admin-istration of metformin should be discontinued at the time of administration of contrast medium and withheld for 48 hours
and reinstituted only after renal function has been re-evaluated and found to be normal. (Refer to SPC). Patients with acute cerebral pathology, tumours or a history of epilepsy, alcohol-ics and drug addicts are predisposed to seizures. Adequate hy-dration should be assured. Young infants (age < 1 year) and especially neonates are susceptible to electrolyte disturbance and haemodynamic alterations. Patients with serious cardiac disease and pulmonary hypertension may develop haemody-namic changes or arrhythmias. Special care should be exercised in patients with hyperthyroidism. One should also be aware of the possibility of inducing transient hypothyroidism in prema-ture infants receiving contrast media. Symptoms of myasthenia gravis may be aggravated. Extravasation of contrast media may on rare occasions give rise to local pain, and oedema, which usually recedes without sequelae. However, infl ammation and even tissue necrosis have been seen. Elevating and cooling the aff ected site are recommended as routine measures. Surgical decompression may be necessary in cases of compartment syn-drome. Following myelography the patient should rest with the head and thorax elevated by 20° for one hour. Th ereafter he/she may ambulate carefully but bending down must be avoided. Th e head and thorax should be kept elevated for the fi rst 6 hours if remaining in bed. Patients suspected of having a low seizure threshold should be observed during this period. Out-patients should not be completely alone for the fi rst 24 hours. A few patients have experienced a temporary hearing loss or even deafness after myelography.
PREGNANCY AND LACTATION Th e safety of OMNI-PAQUE in human pregnancy has not been established (see SPC). Omnipaque should not be used in pregnancy unless considered essential. Breast feeding may continue normally.
UNDESIRABLE EFFECTS All routes of administration: Hypersensitivity reactions with mild respiratory or cutaneous symptoms or anaphylactic reactions with more severe manifes-tations. Vagal reactions causing hypotension and bradycardia, headache. Abdominal discomfort/pain, nausea, vomiting or diarrhoea, transient metallic taste. Iodism or “iodide mumps” resulting in swelling and tenderness of the salivary glands. Feeling of warmth, fever, rigors, hypertension. Intravascular use (Intraarterial and Intravenous use) Neurological reactions, including seizures or transient motor or sensory disturbances. Cortical blindness. Serious cardiac complications, including
cardiac arrest, arrhythmia, depressed cardiac function or signs of ischaemia. A transient increase in S-creatinine, followed by renal failure in rare occasions. Distal pain or heat sensation in peripheral angiography.Transient ischaemia after injection into coronary, cerebral or renal arteries. Post phlebographic thrombophlebitis or thrombosis. Arthralgia. Severe respiratory symptoms and signs (dyspnoea, bronchospasm, laryngospasm, non-cardiogenic pulmonary oedema), cough. Th yrotoxicosis, fl ushing, injection site reaction.Intrathecal use: Meningism or chemical meningitis. Photopho-bia. Transient blindness, motor or sensory dysfunction. Confu-sion. Paraesthesia. Seizures. EEG changes. Local pain, cramp-ing and pain in the lower limbs, neck pain. Headache, nausea, vomiting or dizziness. Injection site reaction.Use in Body Cavities Endoscopic Retrograde Cholangiopan-creatography (ERCP): Elevation of amylase levels, pancreatitis. Oral use: Gastrointestinal upset. Hysterosalpingography (HSG): Transient pain in the lower abdomen. Arthrography: Post procedural pain. Frank arthritis. Herniography: Mild post-procedural pain.
INSTRUCTIONS FOR USE AND HANDLING Like all parenteral products, OMNIPAQUE should be inspected visu-ally for particulate contamination, discolouration and the in-tegrity of the container prior to use. Th e product should be drawn into the syringe immediately before use. Containers are intended for single use only, any unused portions must be dis-carded. OMNIPAQUE may be warmed to body temperature (37°C) before administration.
MARKETING AUTHORISATION HOLDER GE Health-care AS, Nycoveien 1-2, P.O. Box 4220 Nydalen, N-0401 Oslo, Norway.
CLASSIFICATION FOR SUPPLY Subject to medical pre-scription (POM).
MARKETING AUTHORISATION NUMBER PL 00637/0034-0038.
DATE OF REVISION OF TEXT 15 February 2007.
PRICE Omnipaque 350mgI/ml, 10x50ml: £208.01
IOMERON® Iomeprol
Abbreviated Prescribing Information - for full prescribing information, including side eff ects, precautions and contra-indications, see Summary of Product Characteristics (SPC).
Presentation: Sterile, aqueous solution of iomeprol. Iomeron 250, 51.03% w/v (250mg I/ml); Iomeron 300, 61.24% w/v (300mg I/ml); Iomeron 350, 71.44% w/v (350mg I/ml); Iomeron 400, 81.65% w/v (400mg I/ml). Uses: X-ray contrast medium for DSA (intra-arterial and intravenous); CT brain/body; Urography; Cavernosography; Arthrography; Myelography; Aortography; Angiocardiography; Arteriogra-phy (cerebral, coronary etc); Venography; Dacryocystography; Sialography; Fistulography; Galactography; ECRP. Dosage and Administration: Dosage and route often depend on the procedure and/or product (see SPC). Do not exceed 250ml. Intravascular administration should be given to the patient lying down; X-ray up to 60 min following injection. Lumbar injection: over 1-2 min; delay CT spine for ~4 hr. Elderly: as adult; use lowest eff ective dose. Children: according to procedure, body size and age (see SPC). Contra-indications: Hypersensitivity to similar, iodine-containing products. Intrathecal: concomitant intrathecal/epidural corticosteroids. Precautions and Warnings: Resuscitative measures should be available. Observe patients for at least 1 hr. May provoke anaphylaxis or other manifestations of allergy; allergic reac-tions may take several days to develop. Care in children and the elderly. Correct abnormalities of fl uid and electrolytes before administration, particularly in patients with myeloma, polyuria, oliguria, hyperuricaemia, sickle cell disease, diabetes, renal impairment, and in babies, small children and the elderly. Avoid extravasation during injection. Care in patients with history of allergy, severe asthma, functional impairment of liver, kidneys or myocardium, in particular, combined renal and hepatic impairment (use only if absolutely necessary), severe cardiac disease, particularly heart failure and coronary artery disease, epilepsy, diabetes, pulmonary hypertension, hyperthyroidism or goitre, acute cerebral infarction, acute
intracranial haemorrhage, conditions with damage to blood-brain barrier, cerebral oedema, acute demyelination, history of intracranial tumours or metastases, acute and chronic alcohol-ism, suspected thrombosis, phlebitis, severe ischaemic disease, local infection or arterio-venous obstruction. Increased risk of reaction in severe cardiac disease. Increased risk of transient neurological complications in patients with symptomatic cerebrovascular disease. Some neurological symptoms may be exacerbated. Increased risk of renal damage in patients with severe chronic hypertension. Possibility of ventricular arrhyth-mias during cardiac procedures. Check renal function before re-administration in patients with moderate or severe impair-ment of renal function. May interfere with thyroid function tests. May aggravate myasthenia gravis. Phaeochromocytoma: premedicate with an alpha blocker. Possible reduced seizure threshold in drug addicts and alcoholics. Pregnancy and Lacta-tion: Avoid in pregnancy. Discontinue breast-feeding before iomeprol; do not recommence for at least 24 hr. Interactions: Metformin; stop at the time of examination, do not reinstate for 48 hr and then only if renal function is regained. Anti-convulsant therapy should not be discontinued. Discontinue treatment with drugs that lower seizure threshold (analgesics and phenothiazine anti-emetics) and neuroleptics 48 hr before examination; do not resume for 24 hr. Do not administer vasopressor agents before iomeprol. Non-ionic contrast media have less anticoagulant activity in-vitro than ionic media, so particular attention must be paid to angiographic technique. Following intrathecal use the patient should rest with elevated head and chest for 6 hr or 1 hr bed rest then walk remaining upright; observe patients with lower seizure threshold. Driving or operating machinery should be avoided for 24 hr after administration as delayed reactions may occur. Side Eff ects: Usually mild to moderate but severe life-threatening reactions have been reported. Reactions usually occur within minutes of dosing but may occur up to 24 hr later. Anaphylaxis may manifest with cardiovascular, respiratory or cutaneous symp-toms typically in 1-15 min but up to 2 hr; primary circulatory collapse can occur with or without signs or symptoms. Severe reactions involving the cardiovascular system can occur rapidly (vasodilatation with pronounced hypotension, tachycardia,
dyspnoea, agitation, cyanosis, loss of consciousness progressing to respiratory and/or cardiac arrest and may be fatal). Give full and aggressive cardio-pulmonary resuscitation. Commonly; injection site warmth and pain, headache, pallor, nausea. Uncommonly: agitation, dizziness, paralysis, bradycardia, tachycardia, hypo-/hyper-tension, dyspnoea, nasal congestion, laryngeal oedema, vomiting, rash, erythema, wheals, pruritus, sweating, back pain, chest pain, rigors, injection site haemor-rhage, pyrexia. Rarely: tremor, confusion, loss of conscious-ness, visual disturbance, syncope, aphasia, convulsions, coma, cyanosis, vasodilatation, circulatory collapse, muscle spasms, renal failure, oliguria, proteinuria, asthenia, increased blood creatinine, anaphylaxis. For additional details, see SPC. Overdose: Eff ects on pulmonary and cardiovascular systems may become life-threatening. Support vital functions and treat symptomatically. Iomeprol is dialyzable. Pharmaceuti-cal Precautions: Store below 30oC. Protect from light. Do not mix with other drugs. Discard if container is damaged, or solution is discoloured or contains particulate matter. For single use only. Use sterile technique. Withdraw medium into syringe immediately before use. Solutions for intravascular and intrathecal use should be at body temperature when injected. Discard unused solution. Legal Category: POM. MA Numbers: Iomeron 250 PL 18920/0003; Iomeron 300 PL 18920/0004; Iomeron 350 PL 18920/0005; Iomeron 400 PL 18920/0006. NHS list prices per single unit: Iomeron 250 50ml £15.00; Iomeron 300 50ml £22.00; Iomeron 350 50ml £26.00; Iomeron 400 50ml £28.00. Further information is available from the Marketing Authorisation holder: Bracco UK Ltd., Bracco House, Mercury Park, Wycombe Lane, Wooburn Green, High Wycombe, Bucks, HP10 0HH, UK. Date of review: December 2007.
Information about adverse event reporting can be found at www.yellowcard.gov.uk.Adverse events should also be reported to Bracco on 01628 851500.
BUK120702
Refer to pages 14-15

DIARY
Diary
March
ACC 2008 + i2 Summit29 March - 1 April, 2008Chicago, IL, USAWeb: www.acc08.acc.org
May
EuroPRevent 20081-3 May, 2008Paris, FranceWeb: www.escardio.org
EuroPCR13-16 May, 2008Barcelona, SpainWeb: www.europcr.com
Heart Rhythm 2008 - 29th Annual Scientific Sessions14-17 May, 2008San Francisco, CA, USAWeb: www.hrsonline.org
XVI World Congress of Cardiology18-21 May, 2008Buenos Aires, ArgentinaWeb: www.worldheart.org
June
BCS Annual Scientific Conference2-5 June, 2008Manchester, UKWeb: www.bcs.com
Arrhythmia Awareness Week 20089-15 June, 2008Email: [email protected]
Heart Failure 2008 Congress14-17 June, 2008Milan, ItalyWeb: www.escardio.org
Cardiostim 200818-21 June, 2008Nice, FranceWeb: www.cardiostim.fr
August
ESC Congress 200830 August - 3 September, 2008Munich, GermanyWeb: www.escardio.org
3� CORONARY HEART ™
Medical Recruitment
Locum and permanent positions, domesticallyand internationally for Cardiac Physiologists,Cath Lab staff and Sonographers. Trainee rolesare also available.
Specialists in Cardiology and RadiographyCall now to register your interest if you
are seeking work or staff
Australia freephone 1300 36 23 37 tel +612 9994 8074
New Zealand Freephone 0800 508 [email protected]
Call the our specialist team direct
020 7426 [email protected]
For clients and candidates in Australiaand New Zealand please contact

EMPLOYMENT
Upcoming Issues
May / June 2008
Cardiac CT
Contrast Media (Part 2)
Cardiovascular Pharmacology (Part 2)
Beginner Series (Part 1): Sheaths
Hot Topic: Unprotected Left Main Stenting
Full sized Echo Ultrasound units
July / August 2008
Mobile Cath Labs
Contrast Induced Nephropathy
Beginner Series (Part 2): Wires
Cardiac Image Management Systems
Embolic Protection for Saphenous Vein Graft Interventions
September / October 2008
Cardiac MRI and PET
Cardiac ECG Monitoring Systems
Hybrid Cardiac X-ray Systems
Beginner Series (Part 3): Catheters
For advertising please contact Wendy Rose:[email protected]
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
CORONARY HEART ™ 3�CORONARY HEART ™ 3�
Radi Medical Systems AB develops, manufactures and sells medical devices that improve patient care. Our pioneering work within the field of interventional cardiology has resulted in market leading
intravascular sensors and hemostasis management devices. We continue to work closely with medical practitioners to refine techniques and find new uses for our devices, as well as provide
unrivaled education and support. Based in Uppsala, Sweden, Radi Medical Systems was founded in 1988. Today, we employ more than 320 people globally with representation in 42 countries.
Our UK subsidiary is currently looking for new employees:
3 clinical product specialists/sales reps
£27,000 - £36,300 + bonus & benefits
1. North Thames/London2. South West England/South Wales3. Midlands
The role: To provide excellent educational support as a ClinicalProduct Specialist, taking sales responsibility withinone year.
Essential job requirements:Excellent written and verbal English/communicationskills, reliability, enthusiasm and flexibility. Driving license and able to regularly stay away overnight.
Preferred skills: Coronary Catheter Lab experience, presentationskills, commercial experience.
Please contact us for further information or apply directly with CV:
Radi Medical Systems Ltd.Att. Cecilia Hawthorne 8G Godalming Business Centre, Woolsack Way GodalmingSurrey, GU7 1XW
E-mail: [email protected]: 01483 – 412 706More info at www.radi.se
Closing date: April 11, 2008
No agencies

MKT01422_Clinical_Services_1007.indd 1 18/10/07 4:21:51 pm