Coronary Artery Imaging: Don’t have a Heart Attack
23
Briana Olson, RDCS, AE, PE 09/25/2021 Cardiology Coronary Artery Imaging: Don’t have a Heart Attack
Transcript of Coronary Artery Imaging: Don’t have a Heart Attack

Enter department name hereEnter department name here
Briana Olson, RDCS, AE, PE09/25/2021Cardiology
Coronary Artery Imaging:
Don’t have a Heart Attack

Enter department name hereEnter department name here
I do not have any disclosures

Enter department name here
Why Should We Look at Coronaries?
• Current guidelines published by ASE list imaging
of coronary arteries (CA) as standard component
of a pediatric echocardiogram*
• Abnormal CA origins are associated with an
increased risk of sudden cardiac death**
• Detailed CA imaging of pediatric patients
presenting with syncope, chest pain with
exercise, exercise-induced arrythmias, and
Kawasaki disease is necessary**
• High-quality diagnostic imaging of coronaries can
present a significant challenge for sonographers* Wyman, JASE, 2006
** Brown et al, JASE, 2015

Enter department name here
What We Will Discuss Today
• Coronary artery anatomy
• Knobology and image optimization
• What is important to show the reading
physicians
• Look at normal coronary images
• Brief look at selected coronary artery pathology

Enter department name hereEnter department name here
• Know your coronary artery anatomy!
• Know the limitations of imaging CA using
ultrasound
• Can use non-standard views at times
Where to Start

Enter department name hereEnter department name here
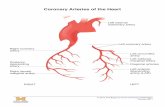
Coronary Artery Anatomy
• Left main coronary artery originates from the left
coronary sinus
• Gives rise to the left anterior descending and
circumflex
• Right coronary artery from the right coronary
sinus
source: https://sems-journal.ch/6297
Enter department name hereEnter department name here
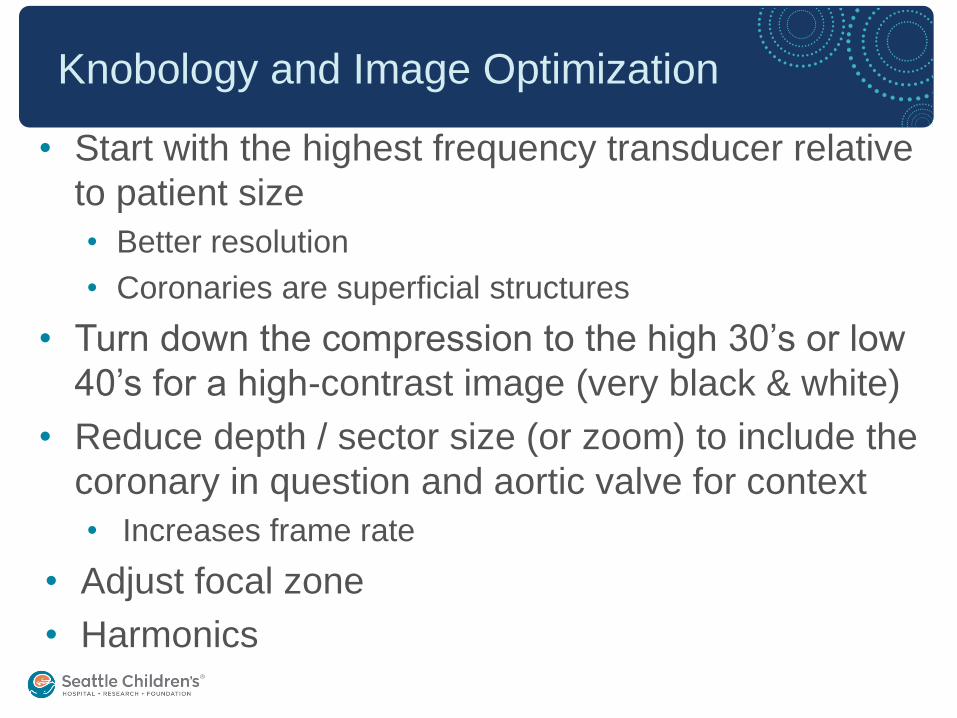
Knobology and Image Optimization
• Start with the highest frequency transducer relative
to patient size
• Better resolution
• Coronaries are superficial structures
• Turn down the compression to the high 30’s or low
40’s for a high-contrast image (very black & white)
• Reduce depth / sector size (or zoom) to include the
coronary in question and aortic valve for context
• Increases frame rate
• Adjust focal zone
• Harmonics

Enter department name hereEnter department name here
Knobology and Image Optimization
• Turn your Color Doppler setting to ‘high flow’
optimization and start with a Nyquist of about 30
cm/sec
• Velocity within coronaries is very low so this will color fill
the coronaries more easily
• Only turn the scale as low as needed so the direction of
flow does not alias
• Use a small sector color box only over the area of interest
• Persistence
• Turn your EKG on!
diastole
• Coronaries fill in predominantly in diastole
• Have it gained enough to see
the cardiac cycle

Enter department name hereEnter department name here
• Interrogate the left and right independently
• Prove the origin of each coronary arises from the
appropriate aortic Sinus of Valsalva
• Prove they have a normal proximal course
• Confirm direction of flow by color Doppler
What Are You Trying to Show the Reading
Physicians?
Enter department name hereEnter department name here
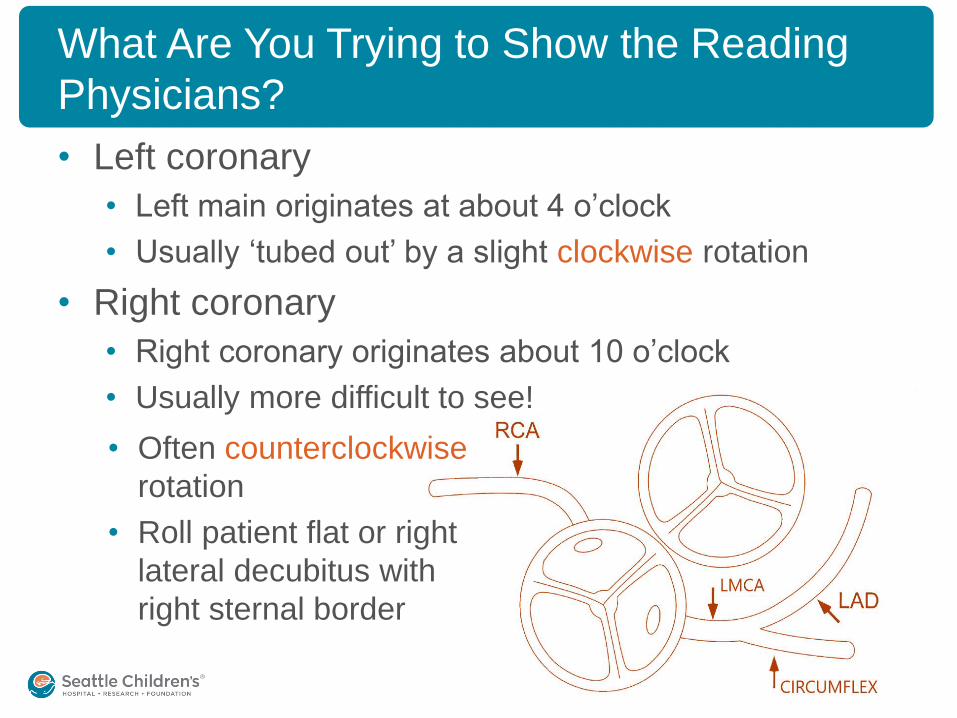
What Are You Trying to Show the Reading
Physicians?
• Left coronary
• Left main originates at about 4 o’clock
• Usually ‘tubed out’ by a slight clockwise rotation
• Right coronary
• Right coronary originates about 10 o’clock
• Usually more difficult to see!
• Often counterclockwise
rotation
• Roll patient flat or right
lateral decubitus with
right sternal border
Enter department name hereEnter department name here
What Are You Trying to Show the Reading
Physicians?
• Demonstrate in 2D as well as with color Doppler• Color compare is an excellent tool
• Show color originating from the lumen of the
aortic root into the coronary artery • Keep color sector small, only over area of interest
• Parasternal short axis at or just superior to the level of the aortic
valve
• Keep in mind your angle of interrogation. Sometimes moving
up/down or medial/lateral on the chest will help the coronary fill
with color
• Avoid clipping still-frames alone. Always store a
moving clip first and then a still-frame when
appropriate

Enter department name hereEnter department name here
Left Coronary Artery

Enter department name hereEnter department name here
Right Coronary Artery

Enter department name here
Let’s see some pathology!

Enter department name hereEnter department name here
Is This Normal?
• Anomalous right coronary artery from the
left coronary cusp
• Incidence of <1% of the population

Enter department name hereEnter department name here
Is This Normal?
• Anomalous left coronary artery from the
right coronary cusp
• Incidence of 0.15% of the population

Enter department name hereEnter department name here
Is This Normal?
• ALCAPA (anomalous left coronary artery
from pulmonary artery)
• Flow reversal confirmed by color cine loop
• Absence of left coronary artery ostium

Enter department name hereEnter department name here
Is This Normal?
• Large coronary artery aneurysms, as can be seen with
Kawasaki disease
Enter department name hereEnter department name here
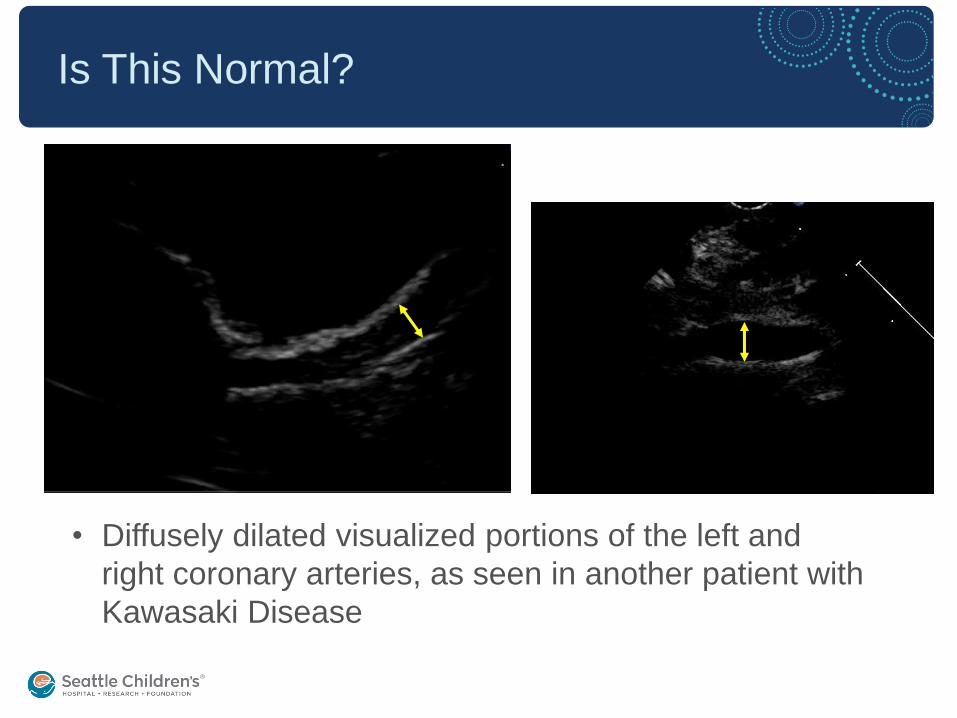
Is This Normal?
• Diffusely dilated visualized portions of the left and
right coronary arteries, as seen in another patient with
Kawasaki Disease
Enter department name hereEnter department name here
Conclusions
• Know your CA anatomy, machine settings, and
views to obtain the best quality images
• Use critical thinking to answer the study question
• Practice! Practice imaging CAs in compliant
patients on a regular basis
• Can save patients from more invasive or costly
diagnostic tests

Enter department name here
References
• Brown LM, Duffy CE, Mitchell C, & Young L. A Practical Guide to
Pediatric Coronary Artery Imaging with Echocardiography. JASE.
2015;28(4):379-391. doi:10.1016/j.echo.2015.01.008.
• Wyman WL, Tal G, Girish SS, et al. Guidelines and Standards for
Performance of a Pediatric Echocardiogram: A Report from the Task
Force of the Pediatric Council of the American Society of
Echocardiography. JASE. 2006;19(12):1413-1430.
doi:10.1016/j.echo.2006.09.001.
Enter department name here
Thank You!

Enter department name here