Coronary Artery Disease Ischemic heart disease.
57
Coronary Artery Disease Ischemic heart disease
-
Upload
juliet-ferguson -
Category
Documents
-
view
236 -
download
0
Transcript of Coronary Artery Disease Ischemic heart disease.

Coronary Artery DiseaseIschemic heart disease


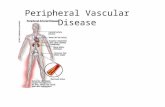
2 coronary arteries branch from the main aorta just above the aortic valve. “No larger than drinking straws, they divide and encircle the heart to cover its surface with a lacy network that reminded physicians of a slightly crooked crown (coronary comes from the Latin coronarius, belonging to a crown or wreath). They carry out about 130 gallons of blood through the heart muscle daily.” (Clark, 119)
Blood Supply To The Heart

Coronary Artery DiseaseCoronary Artery Disease Coronary artery disease is one of the most Coronary artery disease is one of the most
common and serious effects of aging. Fatty common and serious effects of aging. Fatty deposits build up in blood vessel walls and narrow deposits build up in blood vessel walls and narrow the passageway for the movement of blood. The the passageway for the movement of blood. The resulting condition, called atherosclerosis often resulting condition, called atherosclerosis often leads to eventual blockage of the coronary arteries leads to eventual blockage of the coronary arteries and a “heart attack”.and a “heart attack”.


“Cardiovascular disease claimed 39.4 percent of all deaths or 1 of every 2.5 deaths in the United States in 2000. CVD was about 60 percent of “total mention mortality.” This means that of over 2,400,000 deaths from all causes, CVD was listed as a primary or contributing cause on about 1,415,000 death certificates.” (American Heart Disease)


•Since 1900, CVD has been the No. 1 killer in the United States every year but 1918.
•Nearly 2,600 Americans die of CVD each day, an average of 1 death every 33 seconds.
•CVD claims more lives each year than the next 5 leading causes of death combined, which are cancer, chronic lower respiratory diseases, accidents, diabetes mellitus, influenza and pneumonia.
•Almost 150,000 Americans killed by CVD each year are under age 65.

Signs and SymptomsSigns and Symptoms None: This is referred to as None: This is referred to as
silent ischemia. Blood to your silent ischemia. Blood to your heart may be restricted due to heart may be restricted due to CAD, but you don’t feel any CAD, but you don’t feel any effects.effects.
Chest pain: If your coronary Chest pain: If your coronary arteries can’t supply enough arteries can’t supply enough blood to meet the oxygen blood to meet the oxygen demands of your heart, the demands of your heart, the result may be chest pain called result may be chest pain called angina.angina.
Shortness of breath: Some Shortness of breath: Some people may not be aware they people may not be aware they have CAD until they develop have CAD until they develop symptoms of congestive heart symptoms of congestive heart failure- extreme fatigue with failure- extreme fatigue with exertion, shortness of breath and exertion, shortness of breath and swelling in their feet and ankles.swelling in their feet and ankles.
Heart attack: Results when an Heart attack: Results when an artery to your heart muscle artery to your heart muscle becomes completely blocked and becomes completely blocked and the party of your heart muscles the party of your heart muscles fed by that artery dies.fed by that artery dies.
Signs & Symptoms
NoneChestPain
ShortnessOf Breath
HeartAttack

can, and does, occur in almost any artery in the body. But in the heart it’s effects can be crucial. “The body depends on a strong pumping heart to circulate life-giving blood, and this includes to the heart muscle itself. If the coronary arteries become blocked, the cardiac muscle begins to fail, and so the blood circulation decreases, which includes the circulation to the heart muscle itself.” (Thibodeau, 494)


High blood cholesterolHigh blood cholesterol High blood pressureHigh blood pressure SmokingSmoking ObesityObesity Lack of physical Lack of physical
activityactivity

Screening and DiagnosisScreening and Diagnosis
StressStressTestTest
measures
measures
bloo
dbl
ood
supplysupply
to h
eart
to h
eart
CoronaryCoronaryAngiographyAngiography
spec
ific
spec
ific
showsshows
coro
nar
ies
coro
nar
ies
Narrowing inNarrowing in
Sites of
Sites of
Electro-Electro-cardiogramcardiogram
measures
measures
elec
tric
alel
ectr
ical
impulses
impulses






Cholesterol
Diet Liver
Cholesterol Metabolism
15% 75%

Blood Lipid Classification Cholesterol: <200 mg/dl 200-239 mg/dl >240 mg/dl
Desirable Borderline high-risk High-risk
HDL Cholesterol <40 mg/dl >60 mgl/dl
Low High, negates one risk factor
LDL Cholesterol <100 mg/dl 100 – 129 mg/dl 130-159 mg/dL >160 mg/dl
Desirable Above optimal Borderline High High Risk

Treatment in CHD Treatment in CHD PatientsPatients
LDL-C Levels
Diet & Life Habits
Drug Therapy
<100 mg/dL Yes No
100-129 mg/dL
Yes Clinical J udgment
>130 mg/dL Yes Yes







Economic impact:
Despite age adjusted decline in CVD mortality, there is paradoxic increase in economic burden due to:
1) aging population causing actual number of CVD cases to remain stable
2) technologic advances causing more aggressive andextensive treatment


DyslipidemiaDyslipidemia
Better term than hyperlipidemia as it includes the risk of having low HDL
Serum total cholesterol (TC) is a composite of:LDL cholesterol- directly related to CVDHDL cholesterol- inversely related to CVDVLDL cholesterol- related to CVD in patients with
DM and low HDL
Best single predictor for CVD risk is TC/HDL ratio. Ideal ratio is <3, intermediate 3-5, high risk >5This ratio is also the best predictor of treatment benefits

0
25
50
75
100
125
150
Gotto AM Jr, e t al . Ci rcula ti on. 1990;81:17 21-1733 .
Ca ste lli WP. Am J Med. 1984;76:4-12.
Relationship Between Cholesterol and CHD Risk:Epidemiologic Trials
10-y
ear
CH
D d
eath
ra
te(D
eat
hs/
100
0)
Serum cholesterol (mg/dL)
1% reduct ion in total cholesterolresulted in a 2% decrease in CHD risk
CH
D i
ndic
atio
ns
per
100
0Each 1% increase in total cholesterol level isassociated with a 2% increase in CHD risk
Serum cholesterol (mg/100 mL)
Framingham Study (n=5209)Multiple Risk Factor Intervention Trial
(MRFIT) (n=361,662)
204 205-234 235-264 265-294 295150 200 250 3000
50
40
30
20
10

HypertensionHypertension
Potent risk factor for all CVD and dominant risk factor for stroke.
Graded relationship between level of BP and outcomes.
SBP rises with age, whereas DBP plateaus in the late middle life and decreases somewhat then.
Trials for isolated systolic hypertension have shown benefits for both stroke and CHD

Systolic and diastolic hypertension increase the RR for CVDby 1.6 times
For combined Systolic and diastolic HTN the RR is 2.0
The risk for CVD is increased even in individuals with “high normal BP” (130-39/85-89 mm Hg)

SmokingSmoking
This habit increases the risk of vascular outcomes by 2 fold.
Both, regular and filter cigarettes have same adverse effects.
Low tar/low nicotine products have not been shown to reducethe risk
Unlike other modifiable risk factors, cigarette smoking can be eliminated entirely
Benefits of quitting smoking are dramatic. Risk in ex-smokers falls to near non-smoking levels in 2 yrs.

ObesityObesity
It contributes independently to CVD risk and also aggravates known CVD risk factors.
Measures of obesity include: BMI Waist: hip ratio.


Synergy of risk factors:
The CHD death risk in men who smoke, have DBP>90 mm Hg, TC>250 mg/dl, the actual risk is 82/1000 v/s
43/1000 if all the three risk factors are added
Thus there is multiplicative effect of multiple risk
factors acting in concert. Also control of one risk factor provides
substantial benefit in persons with multiple risk factors


(Circulation 1998;97:1837)

10/00 medslides.com 2

Clinical presentation of CHD depends on age and gender
Women:Angina is most common first CHD eventfollowed by MI
Men:MI is the most common first event followed byangina. Sudden cardiac death is not uncommon

Acute myocardial infarction (AMI)
One of the most common diagnosis in hospitalized patients in industrialized nations
Mortality of acute MI is 30% and one-half of thesedeaths occur before hospitalization
Mortality after admission has decreased by 30% in last2 decades
1 in 25 pts (4%) who survive till hospital discharge diewithin one year

PTCA, percutaneous transluminal coronary angioplasty.
0
5
10
15
20
25
30
35
30-D
ay
Mo
rta
lity
(%
)
5.0%- 6.5%5.0%- 6.5%
13%-15%13%-15%
30%30%
Defibrillation
Hemodynamicmonitoring
-Blockade
Defibrillation
Hemodynamicmonitoring
-BlockadeAspirin, PTCA,
Lysis Aspirin, PTCA,
Lysis
BedrestBedrest
Pre-CCU Era CCU Era Reperfusion Era
Improvement in MortalityImprovement in MortalityImprovement in Mortality

Pathophysiology
AMI results when thrombus (occlusive/nonocclusive)develops at the site of ruptured plaque
Vulnerable plaque
Rupture
Coagulation cascade platelet adhesion, activationactivation,aggregation Fibrin and platelet clot
Coronary occlusion
MI

Antman EM. In: Braunwald E, ed. Heart Disease: A Textbook in Cardiovascular Medicine, 5th ed. Philadelphia, Pa: WB Saunders; 1997.
Angiographic thrombus 0%-1% 75% >90%
Increased FPA/TAT 0%-5% 60%-80% 80%-90%
Activated platelets 0%-5% 70%-80% 80%-90%
Acute coronary occlusion 0%-1% 10%-25% >90%
Mortality 1%-2% 3%-8% 6%-15%
Stable anginaStable angina UnstableUnstableanginaangina
Non–Q-waveNon–Q-waveAMIAMI
Q-waveQ-waveAMIAMI
Spectrum of Acute Coronary Syndromes: HematologicFindings in Q-Wave AMISpectrum of Acute Coronary Syndromes: HematologicSpectrum of Acute Coronary Syndromes: HematologicFindings in Q-Wave AMIFindings in Q-Wave AMI



STEMI
ASA, beta blockers, antithrombin therapy
<12 hrs >12 hrs
Eligible forLytic therapy
Lytic C/I Not a candidateFor reperfusion
Persistentsymptoms
Thrombolysis Primary PCI no yes
Other medical therapy Consider reperfusion(ACEI, nitrates, beta blockers, antiplatelets, antithrombin,statins)

Time is muscle

Adapted from Tiefenbrunn AJ, Sobel BE. Circulation. 1992;85:2311-2315.
Time-Dependent Benefit of Reperfusion TherapyTime-Dependent Benefit of Reperfusion TherapyTime-Dependent Benefit of Reperfusion Therapy
0
20
40
60
80
100
0 2 4 6 8 10 12
Reperfusion Time (hours)
% B
enef
it
Reimer/Jennings 1977
Bergmann 1982
GISSI-I 1986

Adapted from Lee KL, et al. Circulation. 1995;91:1659-1668.
Importance of Time-to-Treatment: Results of GUSTO-IImportance of Time-to-Treatment: Results of GUSTO-IImportance of Time-to-Treatment: Results of GUSTO-I
0
2
4
6
8
10
12
0 1 2 3 4 5 6 7 8 9 10 11 12
Time From Onset of Symptoms to Treatment (hours)
2=149 (1 df )
30-D
ay M
ort
alit
y (
%)

Time of OnsetTime of OnsetTime of Onset
ED Time Point 1:DOOR
ED Time Point 1:ED Time Point 1:DOORDOOR
ED Time Point 2:DATA
ED Time Point 2:ED Time Point 2:DATADATA
ED Time Point 3:DECISION
ED Time Point 3:ED Time Point 3:DECISIONDECISION
ED Time Point 4:DRUG
ED Time Point 4:ED Time Point 4:DRUGDRUG
Time Interval IIIDecision to drug
Time Interval IIECG to decision to treat
Time Interval IDoor to ECG
NHAAP Recommendations. U.S. Department of Health NIH Publication: 1997:97-3787.
The Four DsThe Four DsThe Four Ds

Unstable angina/NSTEMI
Aspirin, antithrombin, nitrates, GP IIb-IIIa antagonistBetablockers(calcium channel blockers)
Assess clinical status
High risk/unstable Stable
(Recurrent ischemia, LV dysfunctionWidespread EKG changes, positive
enzyme markers)
Cardiac catheterization Severe ischemia
Revascularization (PCI/CABG) Medical therapy
Stress test
yes
no

Circulation 2004;110:227-239

Smoking cessation:
In FHS, smoking was found to increase the risk for CAD,stroke, heart failure, and peripheral vascular diseaseat all levels of blood pressure
Smoking cessation in hypertensive patients who smoke 1 ppd was estimated to reduce cardiovascular risk by 35-40%
2-3 yrs after cessation, the risk for CAD declines to that ofsubjects who have never smoked

Lung Health Study
Annals of Internal Med, 2005