Copyright Dr Andrew Dean Pain Classification and Opioid Physiology A Review.
53
Copyright Dr Andrew Dean Pain Classification and Opioid Physiology A Review
-
Upload
owen-shepherd -
Category
Documents
-
view
214 -
download
0
Transcript of Copyright Dr Andrew Dean Pain Classification and Opioid Physiology A Review.

Copyright Dr Andrew Dean
Pain Classification and Opioid Physiology
A Review

Copyright Dr Andrew Dean
Analgesic LadderAnalgesic Ladder
• Non-Opioid
• Non-Opioid + Adjuvant Analgesic
• Weak Opioid
• Weak Opioid + Adjuvant Analgesic
• Strong Opioid
• Strong Opioid + Adjuvant Analgesic

Copyright Dr Andrew Dean
Visceral Pain• Pain from abdominal & thoracic viscera
• Deep, squeezing, pressure.
• Poorly localised.
• Sometimes referred.
• Liver, pancreas, lung
Mechanisms of PainMechanisms of Pain

Copyright Dr Andrew Dean
Mechanisms of PainMechanisms of Pain
Somatic Pain• ‘Nociceptive’
• Pain from nerve endings in tissues & bones
• Aching, gnawing.
• Well localised.
• eg Bone Metastases

Copyright Dr Andrew Dean
Neuropathic Pain• Pain from nerve irritation/damage.
• Flashing, sharp, electric, burning.
• Often follows nerve pathway.
• Plexus pain.
Mechanisms of PainMechanisms of Pain

Copyright Dr Andrew Dean
Pain Pathway
Receptors
Cortico-Spinal
Peripheral Nerve
Spino-thalamic
5HTNA

Copyright Dr Andrew Dean
Synapse
SpinalNerve
Peripheral Nerve
Synaptic Cleft

Copyright Dr Andrew Dean
Synapse
Impulse
Impulse
Depolarisation

Copyright Dr Andrew Dean
The Busy Gate
Cortico-Spinal
Sympathetic
Other

Copyright Dr Andrew Dean
Opioid Receptors
MuMu
CaCa2+2+
--
----
--

Copyright Dr Andrew Dean
Receptors
MuMu
K/CaK/CaTo
Spino-thalamic
tract
Excitatoryreceptors
Inhibitoryreceptors

Copyright Dr Andrew Dean
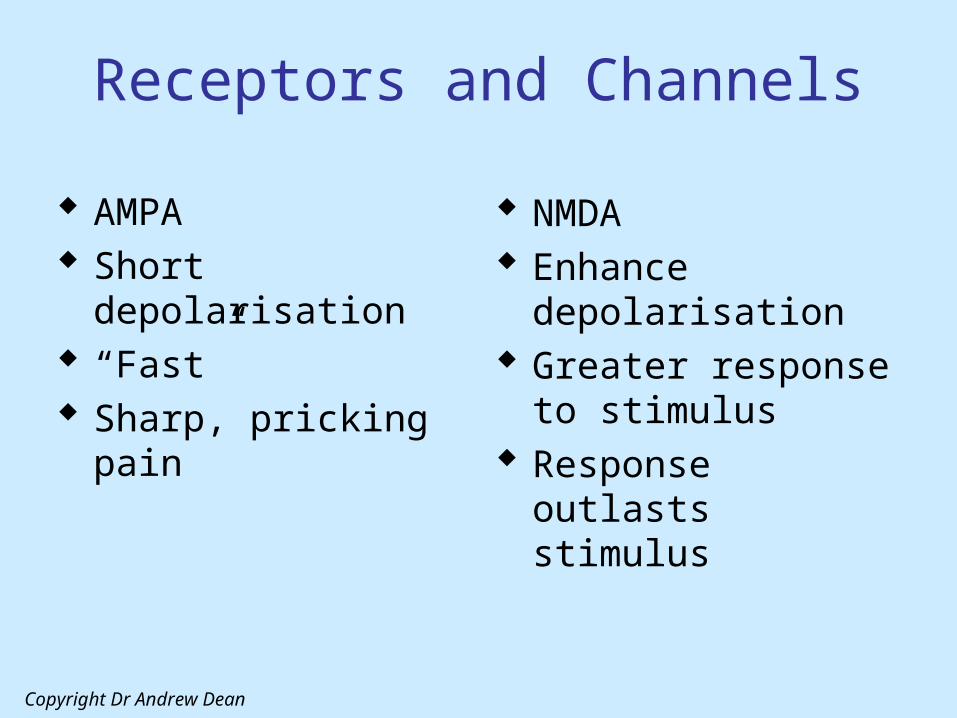
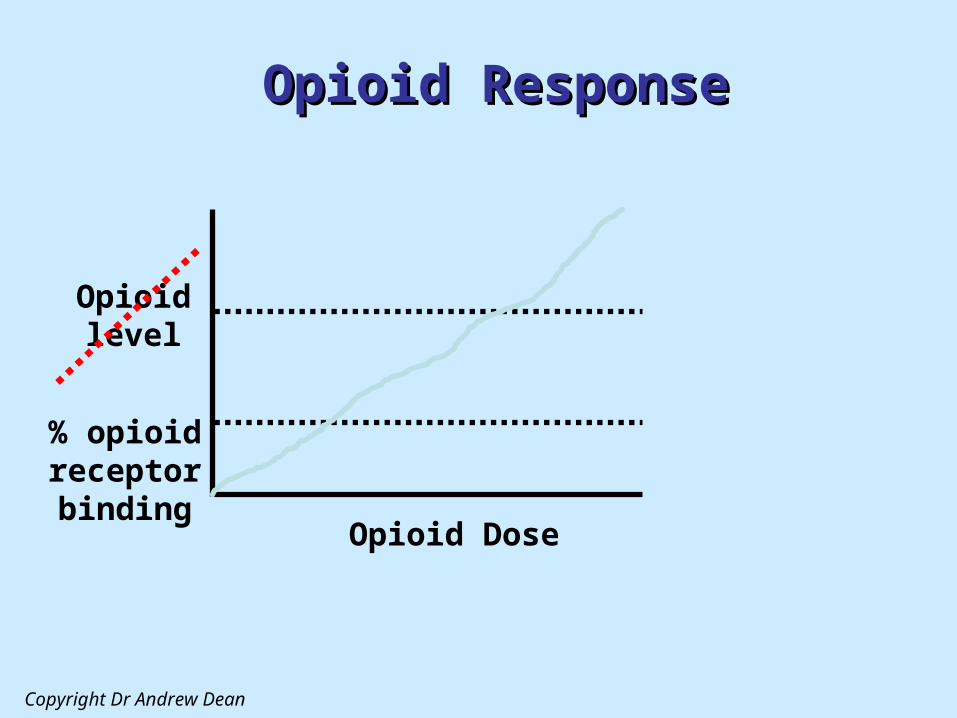
Opioid ResponseOpioid Response
Opioidlevel
Opioid Dose
% opioidreceptorbinding
100%

Copyright Dr Andrew Dean
Opioid ResponseOpioid Response
Opioidlevel
Opioid Dose
% opioidreceptorbinding
100%
Maximumopioid
analgesia
SideEffects

Copyright Dr Andrew Dean
Opioid Receptor Sites
Receptors
Cortico-Spinal
Peripheral Nerve
Spino-thalamic
5HTNA

Copyright Dr Andrew Dean
Peripheral Action of Morphine
MuMu
K/CaK/Ca
Nociceptor
Inflammatorycell

Copyright Dr Andrew Dean
Pain wind up
Copyright Dr Andrew Dean
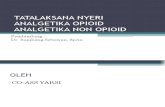
Receptors and Channels
AMPA Short depolarisation “Fast” Sharp, pricking pain
NMDA Enhance
depolarisation Greater response to
stimulus Response outlasts
stimulus

Copyright Dr Andrew Dean
Receptors
MuMu
K/CaK/CaTo
Spino-thalamic
tract
ExcitatoryReceptors
AMPA

Copyright Dr Andrew Dean
NMDA feedback
K/CaK/CaTo
Spino-thalamic
tract
NMDAreceptors
NMDAreceptors

Copyright Dr Andrew Dean
Receptor responses
Impulses Impulses
AMPA NMDA
Stimulus Stimulus
Time Time

Copyright Dr Andrew Dean
Receptor co-operation
AMPANK 1-2
NMDA
C-fibreresponse
Stimulus number

Copyright Dr Andrew Dean
NMDA Antagonists
Very weak Paracetamol
Weak Some NSAID’s Methadone Pethidine Valproate Amantidine

Copyright Dr Andrew Dean
NMDA Antagonists
Moderate Ketamine Dextromethorphan
Strong Experimental Lethal
Copyright Dr Andrew Dean
Opioid ResponseOpioid Response
Opioidlevel
Opioid Dose
% opioidreceptorbinding

Copyright Dr Andrew Dean
Opioid Receptor Sites
Receptors
Cortico-Spinal
Peripheral Nerve
Spino-thalamic
5HTNA

Copyright Dr Andrew Dean
Receptors
MuMu
K/CaK/CaTo
Spino-thalamic
tract
ExcitatoryReceptors
AMPA

Copyright Dr Andrew Dean
Sodium Channels
K/CaK/CaTo
Spino-thalamic
tract

Copyright Dr Andrew Dean
Receptors
K/CaK/CaTo
Spino-thalamic
tract
3. Receptors next to synapse bind opioids which stop chemical
transmission of impulse
Inhibitoryreceptors
1. Cell body receives
electrical impulse producing
Mu receptor
2. Mu receptors migrate down
nerve cell membrane

Copyright Dr Andrew Dean
Sodium Channel Blockers
• Valproate
• Gabapentin
• Carbamazepine

Copyright Dr Andrew Dean
Pain Pathway
Receptors
Cortico-Spinal
Peripheral Nerve
Spino-thalamic
5HTNA

Copyright Dr Andrew Dean
Paracetamol
Receptors
Cortico-Spinal
Peripheral Nerve
Spino-thalamic
5HTNAParacetamol acts here

Copyright Dr Andrew Dean
NSAID’s
Receptors
Cortico-Spinal
Peripheral Nerve
Spino-thalamic
5HTNANSAIDs acts here

Copyright Dr Andrew Dean
Morphine
Receptors
Cortico-Spinal
Peripheral Nerve
Spino-thalamic
5HTNAMorphine acts here
5%
25%
70%
Copyright Dr Andrew Dean
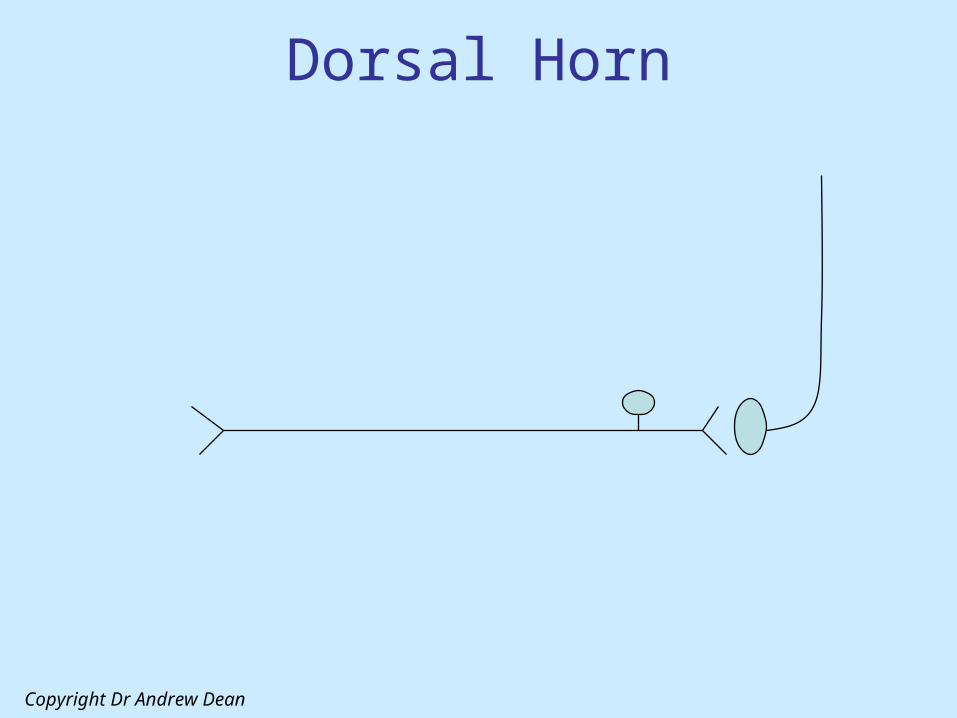
Dorsal Horn

Copyright Dr Andrew Dean
Dorsal Horn

Copyright Dr Andrew Dean
Neuropathic Pain
• Has many mechanisms
• Therefore illogical to expect one drug to work every time
• Often need combination therapy

Copyright Dr Andrew Dean
Pain Pathway
Receptors
Cortico-Spinal
Peripheral Nerve
Spino-thalamic
5HTNA

Copyright Dr Andrew Dean
Opioid Receptors
MuMu
CaCa2+2+
--
----
--

Copyright Dr Andrew Dean
Opioid ResponseOpioid Response
Opioidlevel
Opioid Dose
% opioidreceptorbinding

Copyright Dr Andrew Dean
Side Effect ThresholdSide Effect Threshold
Opioidlevel
Opioid Dose
High threshold

Copyright Dr Andrew Dean
Side Effect ThresholdSide Effect Threshold
Opioidlevel
Opioid Dose
Low threshold

Copyright Dr Andrew Dean
Methadone
• Potent Mu agonist
• NMDA receptor activity
• No active metabolites

Copyright Dr Andrew Dean
Methadone• Formulation
– Oral liquid, tablets– Injection, SC, IM, IV
• Not predicable– Large inter-individual variation– 1-2 hours onset, lasts 6-12 hours– t 1/2 <120 hrs, Steady state 2-10 days.

Copyright Dr Andrew Dean
Methadone• Formulation
– Oral liquid, tablets– Injection, SC, IM, IV
• Not predicable– Large inter-individual variation– 1-2 hours onset, lasts 6-12 hours– t 1/2 <120 hrs, Steady state 2-10 days.

Copyright Dr Andrew Dean
Opioidlevel
Opioid Dose
Side Effect ThresholdSide Effect Threshold
Morphineside effect threshold
Methadoneside effect threshold
Copyright Dr Andrew Dean
Methadone Study
• Retrospective
• Case study - 68 patients
• Morphine side effects
• Co-analgesics unchanged
• Opioid changed to methadone

Copyright Dr Andrew Dean
Methadone Study
Pain Types Somatic 28 Neuropathic 2 Visceral 11 SV 3 SN 22 SVN 1

Copyright Dr Andrew Dean
Methadone Study
Side Effects
• Confusion 20
• Drowsiness 34
• Hallucinations 13
• Nausea 24
• Pruritis 2

Copyright Dr Andrew Dean
Methadone Study
Case study - 68 patientsResolution of adverse effects in 56 (82%)Side effects same or changed in 12

Copyright Dr Andrew Dean
Morphine/Methadone Conversion
1 1
9
13
23
4
10
1 1
0
5
10
15
20
25
1 2 3 4 5 6 7 8 9 10 11 12
Conversion ratio
No
Pe
op
le
Average = 6.34

Copyright Dr Andrew Dean
Methadone Study
Ratios
Neuropathic Pain
• Ratio 7.06
Non-Neuropathic Pain
• Ratio 5.78
Does this reflect NMDA antagonism?

Copyright Dr Andrew Dean
Dose Regimen
Dose Regimen
• bd 57
• tds 11

Copyright Dr Andrew Dean
Methadone Study
Conclusions
• Methadone is a suitable alternative to morphine for cancer pain
• Suggested ratio Suggested regimen May be better for neuropathic pain
6:1
bd
Consider threshold theory