Copyright © 2010 by Nelson Vergel Nelson Vergel Program for Wellness Restoration PoWeRUSA.org...
29
Copyright © 2010 by Nelson Vergel Nelson Vergel Program for Wellness Restoration PoWeRUSA.org Decreasing Metabolic Decreasing Metabolic Problems in People with Problems in People with HIV- HIV- What you can do as an activist What you can do as an activist
Transcript of Copyright © 2010 by Nelson Vergel Nelson Vergel Program for Wellness Restoration PoWeRUSA.org...

Copyright © 2010 by Nelson Vergel
Nelson VergelProgram for Wellness Restoration
PoWeRUSA.org
Decreasing Metabolic Decreasing Metabolic Problems in People with HIV-Problems in People with HIV-What you can do as an activistWhat you can do as an activist
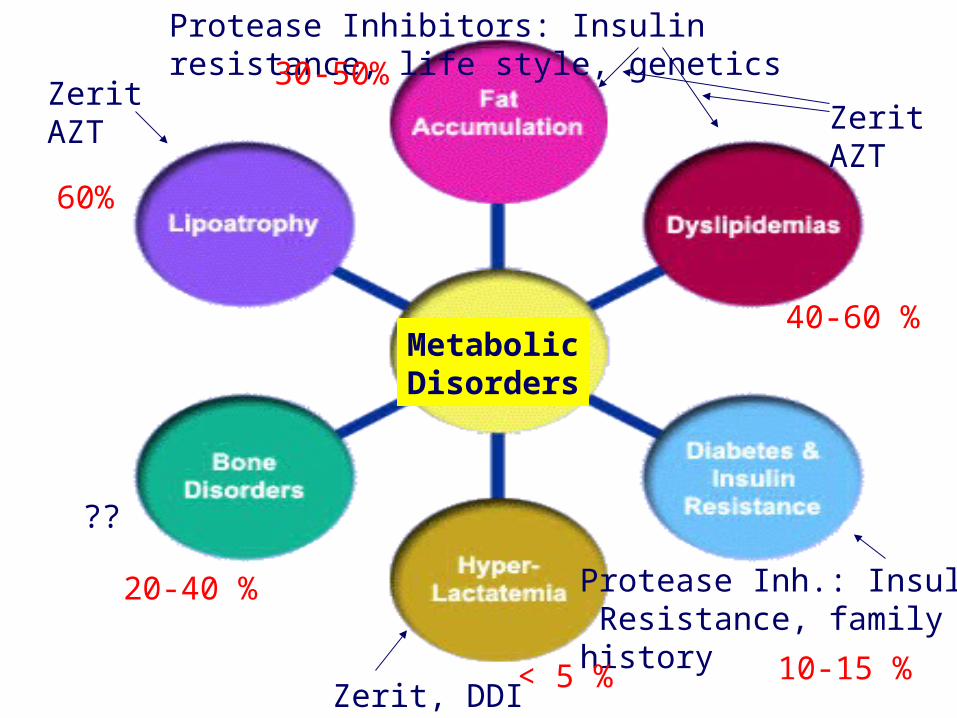
MetabolicDisorders
Protease Inhibitors: Insulin resistance, life style, genetics
ZeritAZT
ZERIT,AZT
Protease Inh.: Insulin Resistance, familyhistory
Zerit, DDI
??
ZeritAZT
60%
30-50%
20-40 %
10-15 %
40-60 %
< 5 %
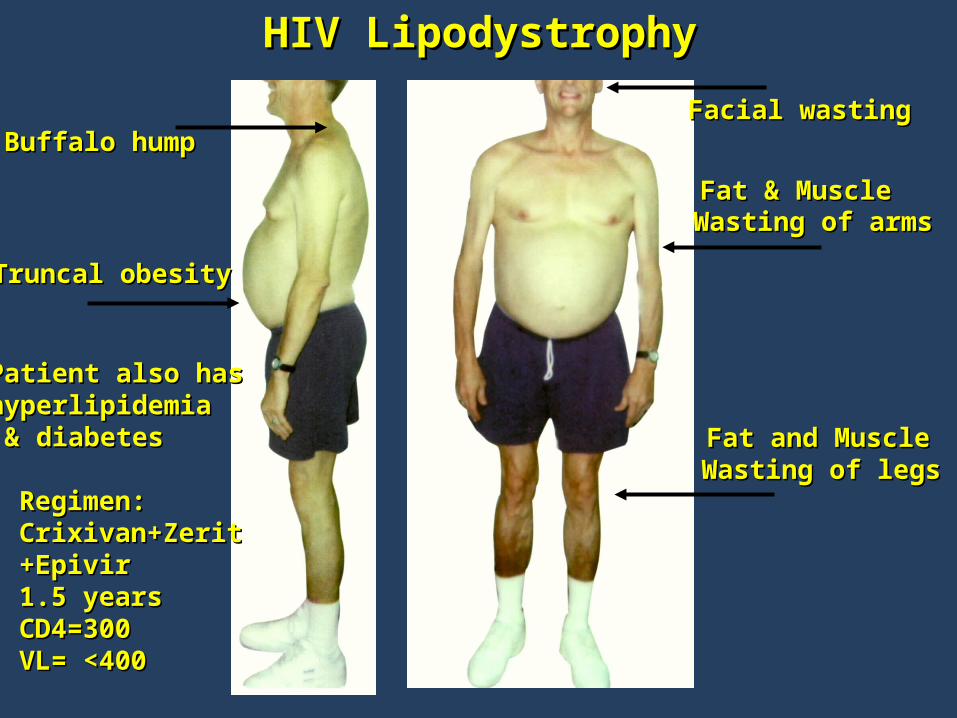
HIV LipodystrophyHIV Lipodystrophy
Truncal obesityTruncal obesity
Facial wastingFacial wasting
Wasting of armsWasting of arms
Wasting of legsWasting of legs
Patient also hasPatient also hashyperlipidemiahyperlipidemia & diabetes& diabetes
Buffalo humpBuffalo hump
Regimen:Regimen:Crixivan+ZeritCrixivan+Zerit+Epivir+Epivir1.5 years1.5 yearsCD4=300CD4=300VL= <400VL= <400
Fat and MuscleFat and Muscle
Fat & MuscleFat & Muscle
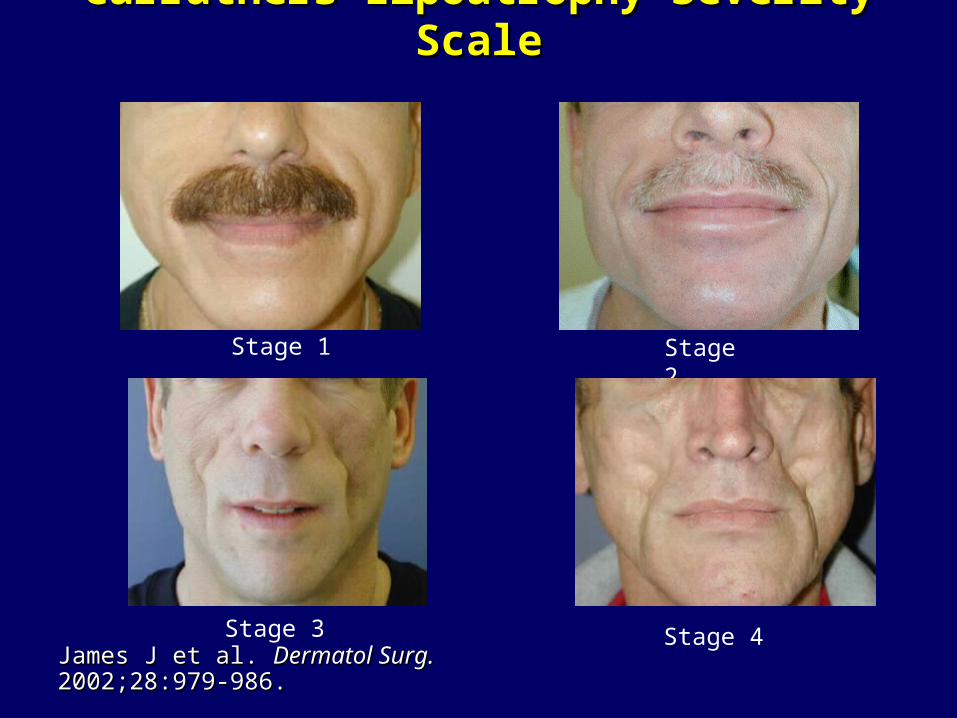
Carruthers Lipoatrophy Severity Carruthers Lipoatrophy Severity ScaleScale
Stage 1 Stage 2
Stage 3 Stage 4James J et al. James J et al. Dermatol Surg.Dermatol Surg. 2002;28:979- 2002;28:979-986. 986.

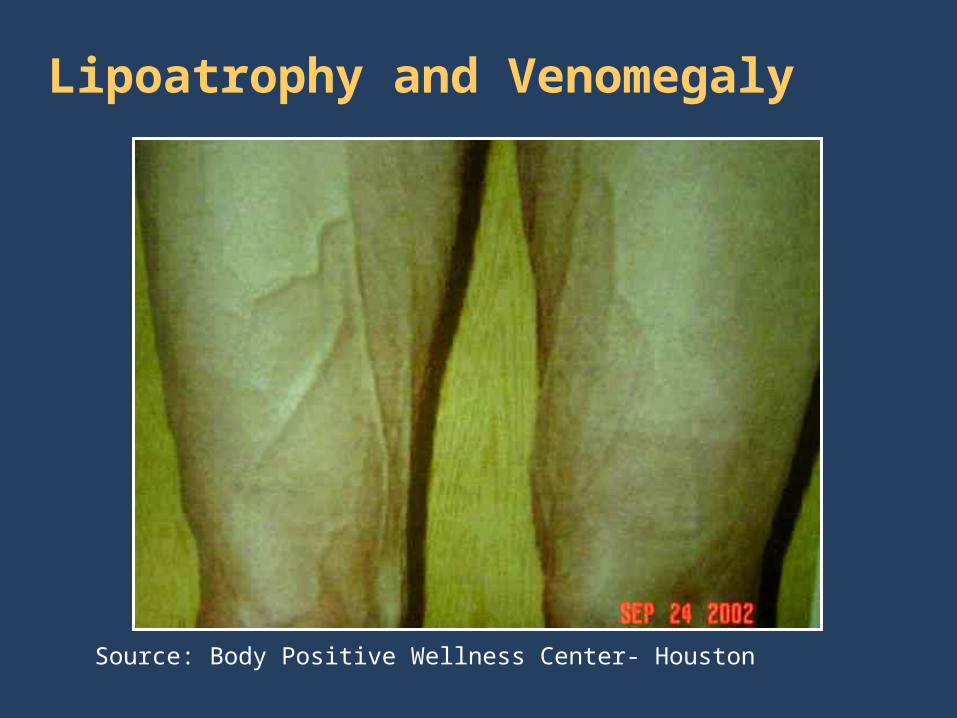
Lipoatrophy and Venomegaly
Source: Body Positive Wellness Center- Houston
What Have We Learned Since 1997 ?
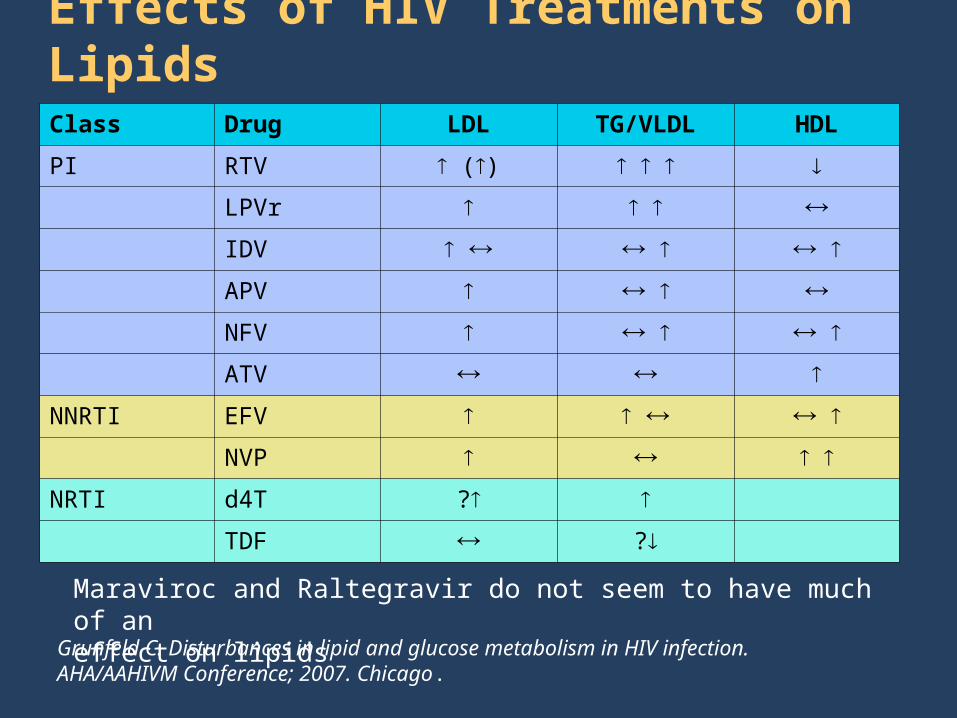
Effects of HIV Treatments on Lipids
Grunfeld C. Disturbances in lipid and glucose metabolism in HIV infection. AHA/AAHIVM Conference; 2007. Chicago.
Class Drug LDL TG/VLDL HDL
PI RTV ()
LPVr
IDV
APV
NFV
ATV
NNRTI EFV
NVP
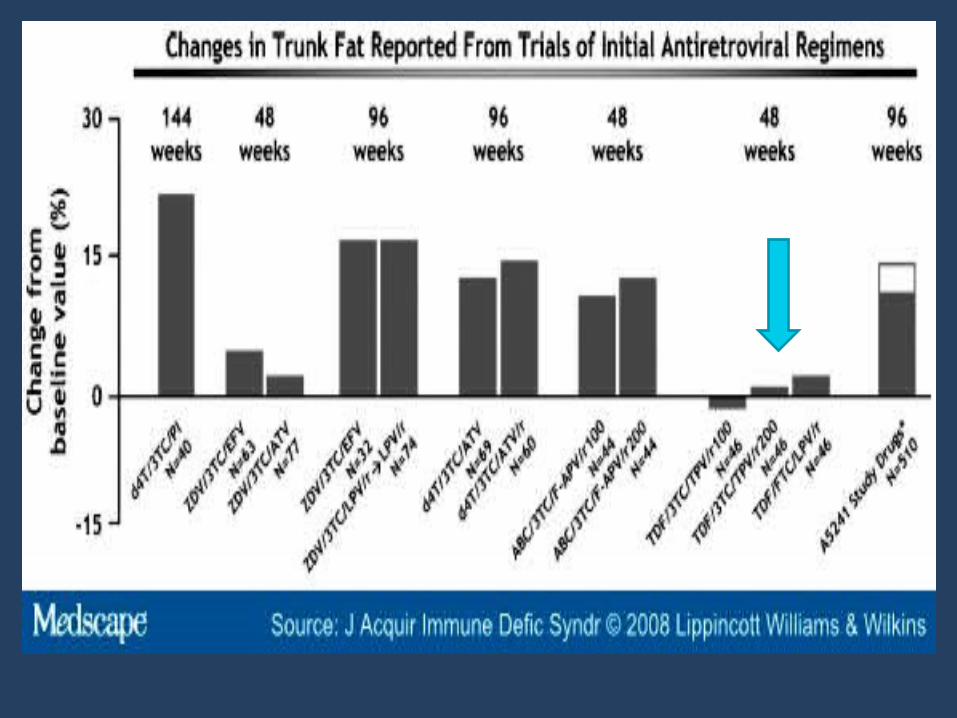
NRTI d4T ?
TDF ?
Maraviroc and Raltegravir do not seem to have much of an effect on lipids
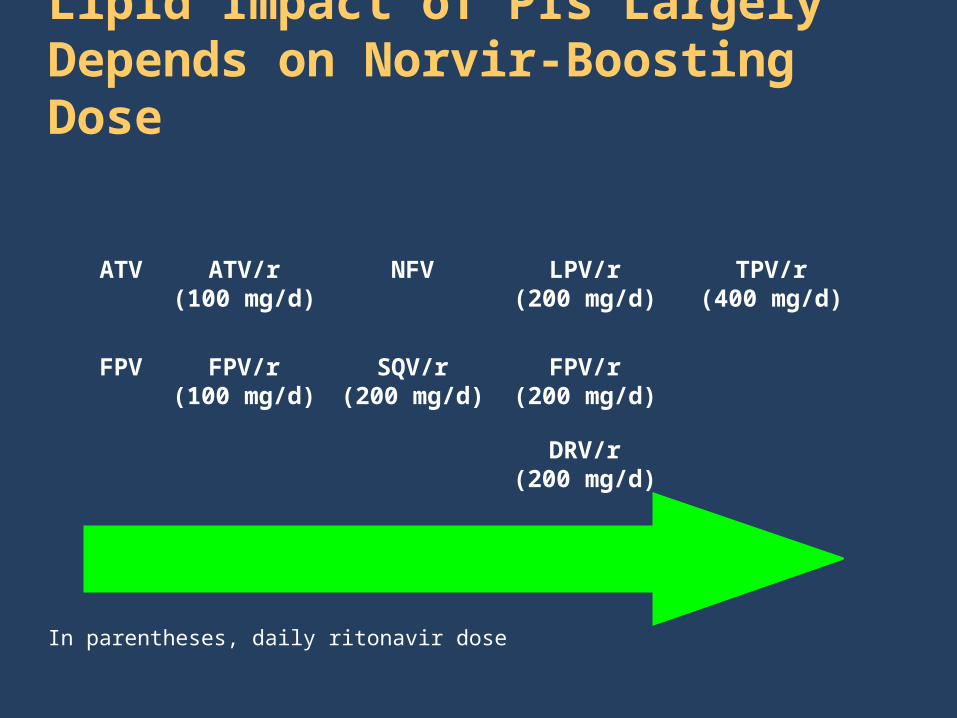
ATV ATV/r(100 mg/d)
FPV/r(100 mg/d)
NFV
SQV/r(200 mg/d)
LPV/r(200 mg/d)
FPV/r(200 mg/d)
DRV/r(200 mg/d)
TPV/r(400 mg/d)
FPV
In parentheses, daily ritonavir dose
Lipid Impact of PIs Largely Depends on Norvir-Boosting Dose
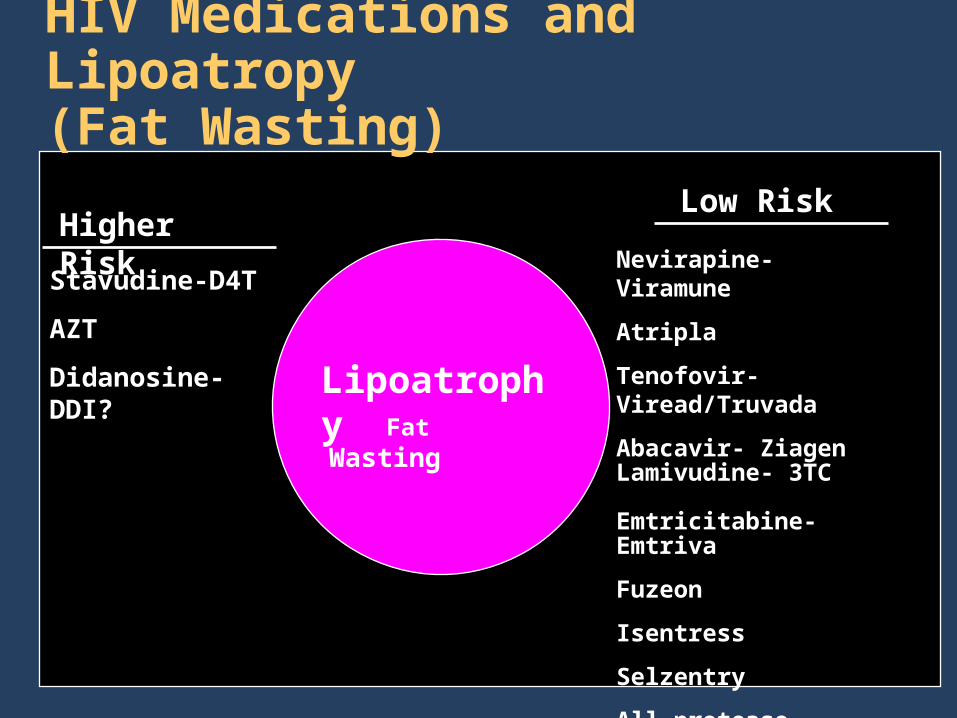
HIV Medications and Lipoatropy (Fat Wasting)
Lipoatrophy Fat Wasting
Higher Risk
Stavudine-D4T
AZT
Didanosine-DDI?
Low Risk
Nevirapine- Viramune
Atripla
Tenofovir- Viread/Truvada
Abacavir- ZiagenLamivudine- 3TC
Emtricitabine- Emtriva
Fuzeon
Isentress
Selzentry
All protease inhibitors
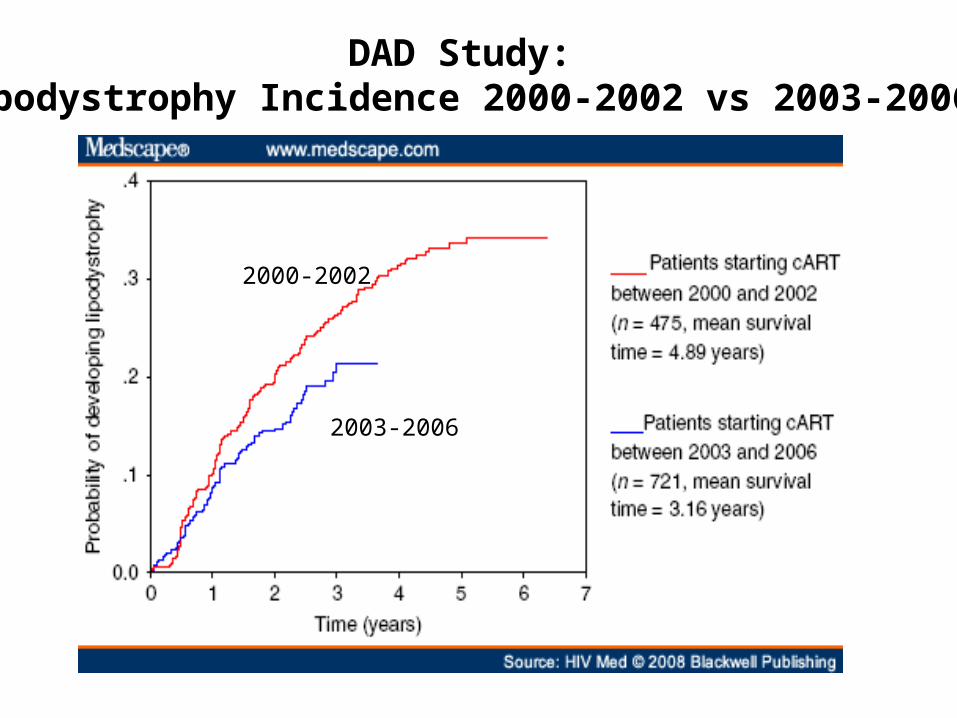
DAD Study: Lipodystrophy Incidence 2000-2002 vs 2003-2006
2000-2002
2003-2006
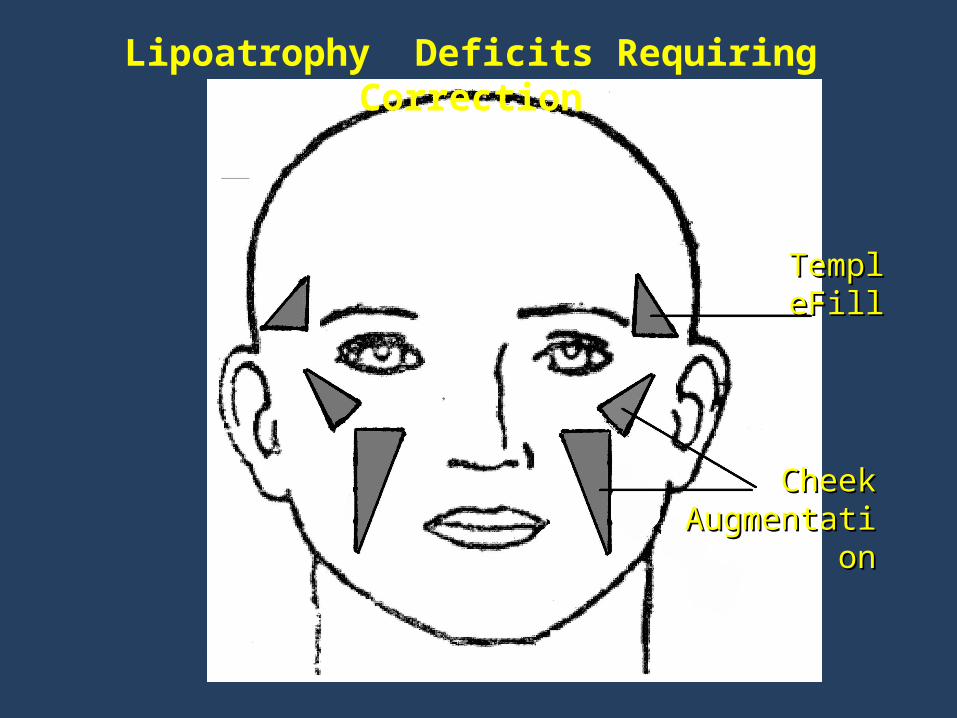
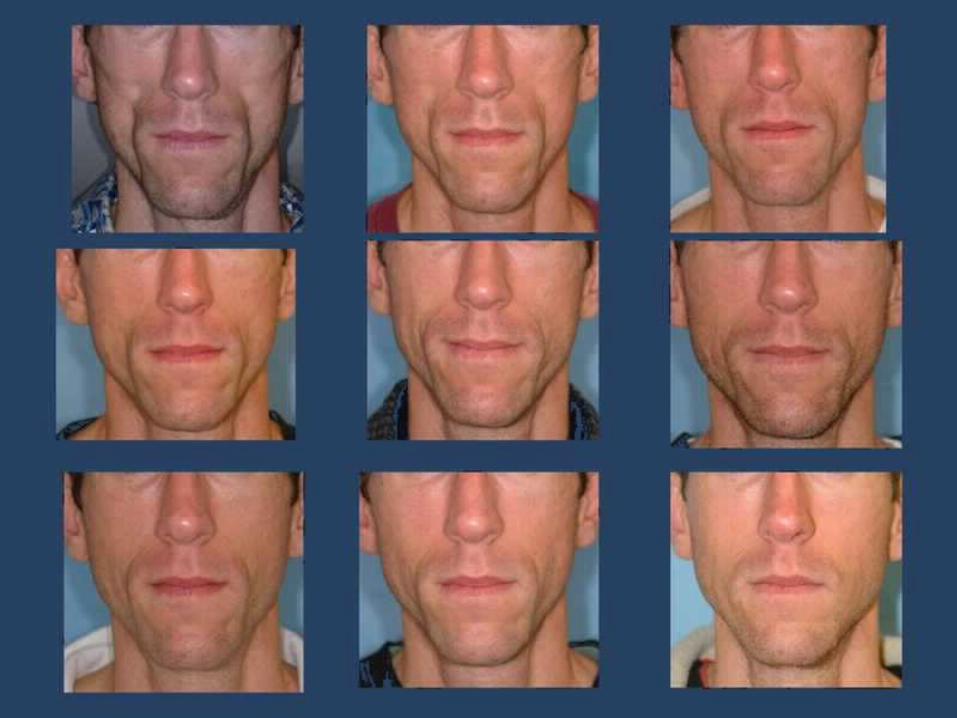
TemplTempleFilleFill
Cheek Cheek AugmentatiAugmentati
onon
Lipoatrophy Deficits Requiring Correction
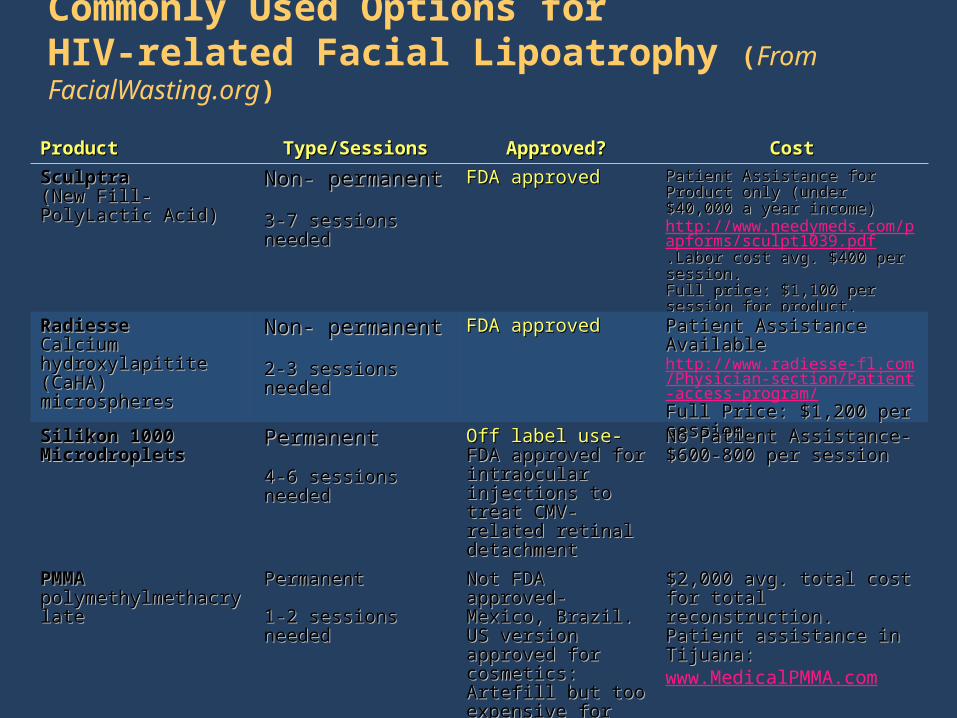
Commonly Used Options forHIV-related Facial Lipoatrophy (From FacialWasting.org)
ProductProduct Type/SessionsType/Sessions Approved?Approved? CostCost
SculptraSculptra(New Fill-PolyLactic (New Fill-PolyLactic Acid)Acid)
Non- permanentNon- permanent
3-7 sessions needed3-7 sessions needed
FDA approvedFDA approved Patient Assistance for Product only Patient Assistance for Product only (under $40,000 a year income) (under $40,000 a year income) http://www.needymeds.com/papforms/sculpt1039.pdf.Labor cost avg. $400 per session. .Labor cost avg. $400 per session. Full price: $1,100 per session for Full price: $1,100 per session for product. product.
RadiesseRadiesseCalcium hydroxylapitite Calcium hydroxylapitite (CaHA) microspheres(CaHA) microspheres
Non- permanentNon- permanent
2-3 sessions needed2-3 sessions needed
FDA approvedFDA approved Patient Assistance AvailablePatient Assistance Availablehttp://www.radiesse-fl.com/Physician-section/Patient-access-program/Full Price: $1,200 per session. Full Price: $1,200 per session.
Silikon 1000Silikon 1000MicrodropletsMicrodroplets
PermanentPermanent
4-6 sessions needed4-6 sessions needed
Off label use-Off label use-FDA approved for FDA approved for intraocular injections intraocular injections to treat CMV- related to treat CMV- related retinal detachmentretinal detachment
No Patient Assistance-No Patient Assistance-$600-800 per session$600-800 per session
PMMAPMMApolymethylmethacrylate polymethylmethacrylate
PermanentPermanent
1-2 sessions needed1-2 sessions needed
Not FDA approved-Not FDA approved-Mexico, Brazil.Mexico, Brazil.US version approved US version approved for cosmetics: Artefill for cosmetics: Artefill but too expensive for but too expensive for volume requiredvolume required
$2,000 avg. total cost for total $2,000 avg. total cost for total reconstruction. Patient reconstruction. Patient assistance in Tijuana: assistance in Tijuana: www.MedicalPMMA.com
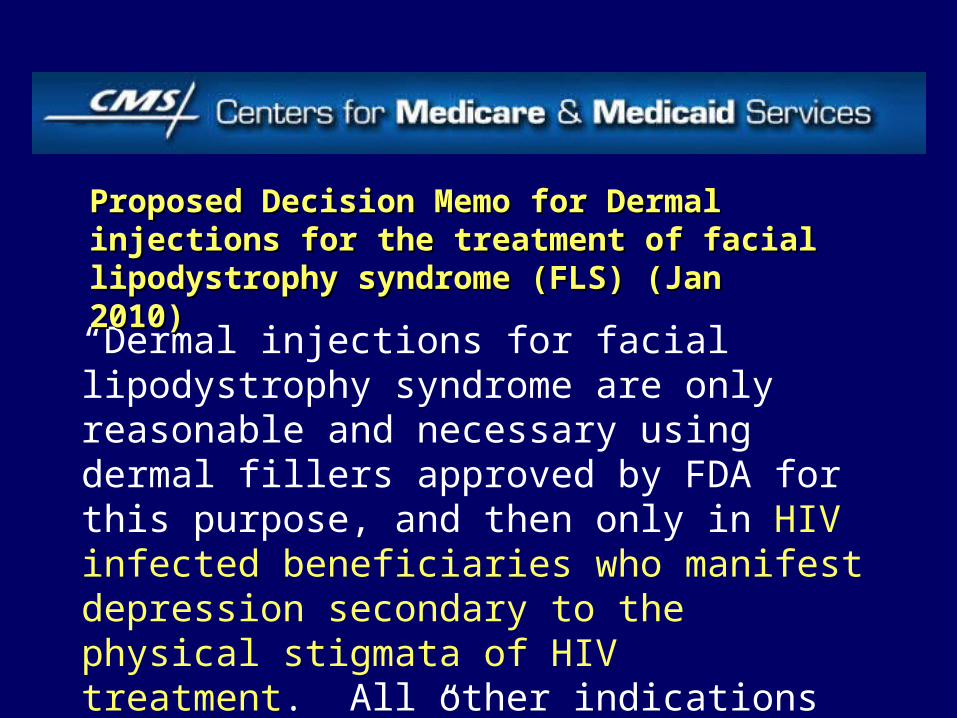
“Dermal injections for facial lipodystrophy syndrome are only reasonable and necessary using dermal fillers approved by FDA for this purpose, and then only in HIV infected beneficiaries who manifest depression secondary to the physical stigmata of HIV treatment. All other indications are noncovered.”
Proposed Decision Memo for Dermal injections Proposed Decision Memo for Dermal injections for the treatment of facial lipodystrophy for the treatment of facial lipodystrophy syndrome (FLS) (Jan 2010)syndrome (FLS) (Jan 2010)
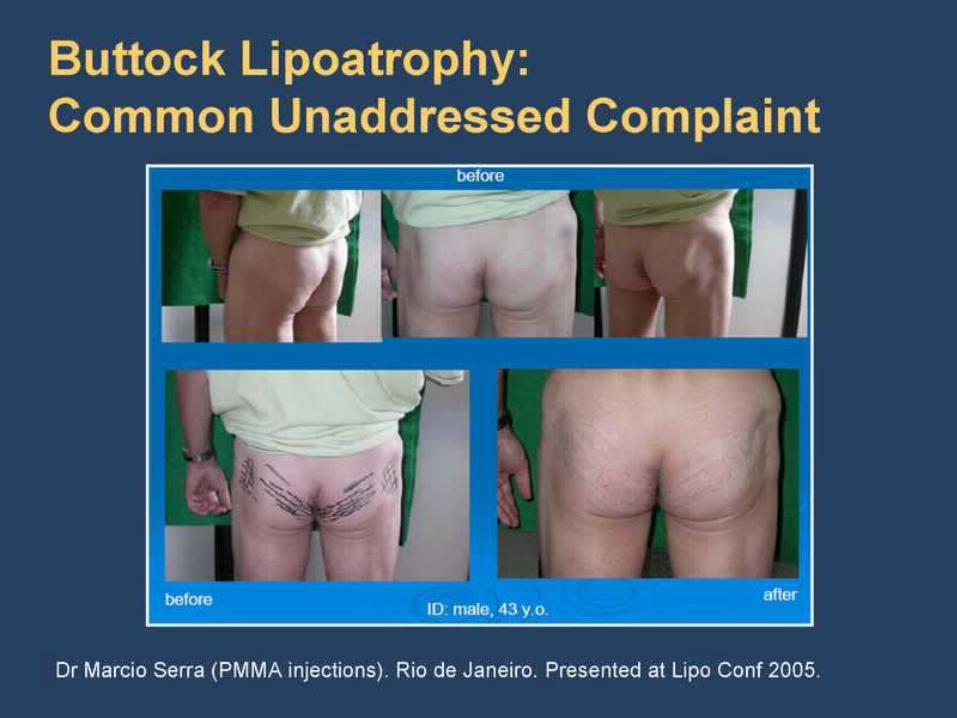
Buttock Lipoatrophy: Common Unaddressed Complaint
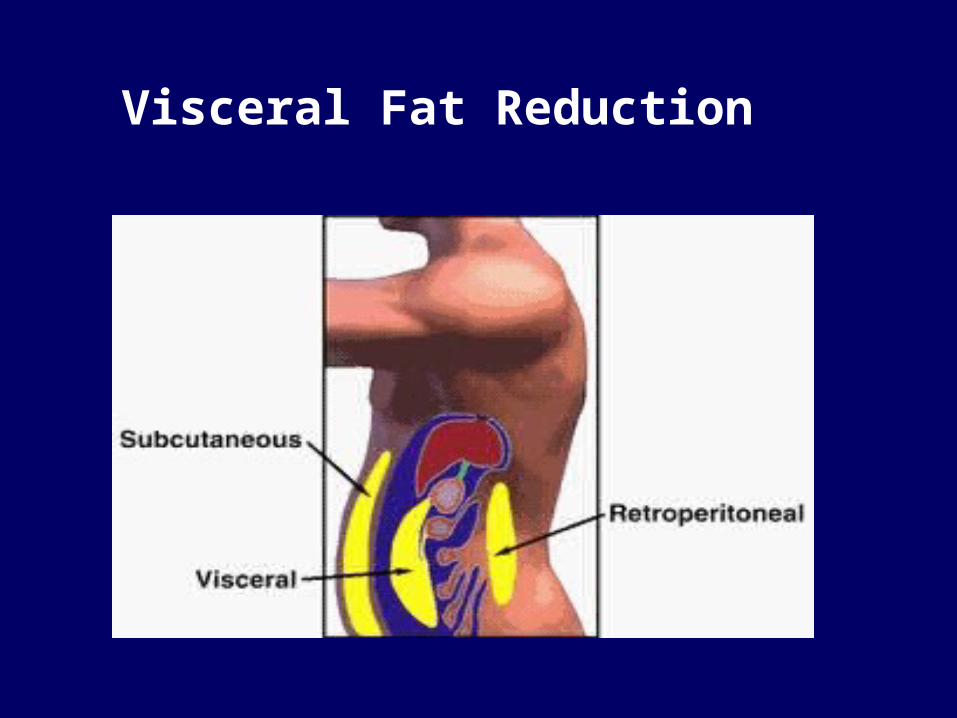
Visceral Fat Reduction
Potential Interventions for Decreasing Potential Interventions for Decreasing Abdominal FatAbdominal Fat (visceral adipose tissue- (visceral adipose tissue-
VAT)VAT) Diet- Diet- Lower carb?- Lower carb?- No data available in HIVNo data available in HIV ExerciseExercise- cardiovascular and resistance training- - cardiovascular and resistance training- Some pilot Some pilot
data with good resultsdata with good results Weight reduction- Weight reduction- non HIV datanon HIV data Anti-diabetic drugs: Anti-diabetic drugs: Metformin (Glucophage)- Metformin (Glucophage)- conflicting conflicting
and inconclusive dataand inconclusive data Testosterone gel- Testosterone gel- subcutaneous fat loss onlysubcutaneous fat loss only Anabolic steroids- Anabolic steroids- Oxandrin, nandrolone?- Oxandrin, nandrolone?- limited VAT data limited VAT data Human Growth Hormone (Serostim)- Human Growth Hormone (Serostim)- highly effective. FDA highly effective. FDA
declined approval due to side effectsdeclined approval due to side effects Human Growth Hormone Releasing Hormone- Human Growth Hormone Releasing Hormone- Tesamorelin-Tesamorelin-
Not approved yet- Pending issues. Slow actionNot approved yet- Pending issues. Slow action Modification or cessation of HAART?- Modification or cessation of HAART?- Not effectiveNot effective SurgerySurgery- - Liposuction of visceral fat very difficult and riskyLiposuction of visceral fat very difficult and risky
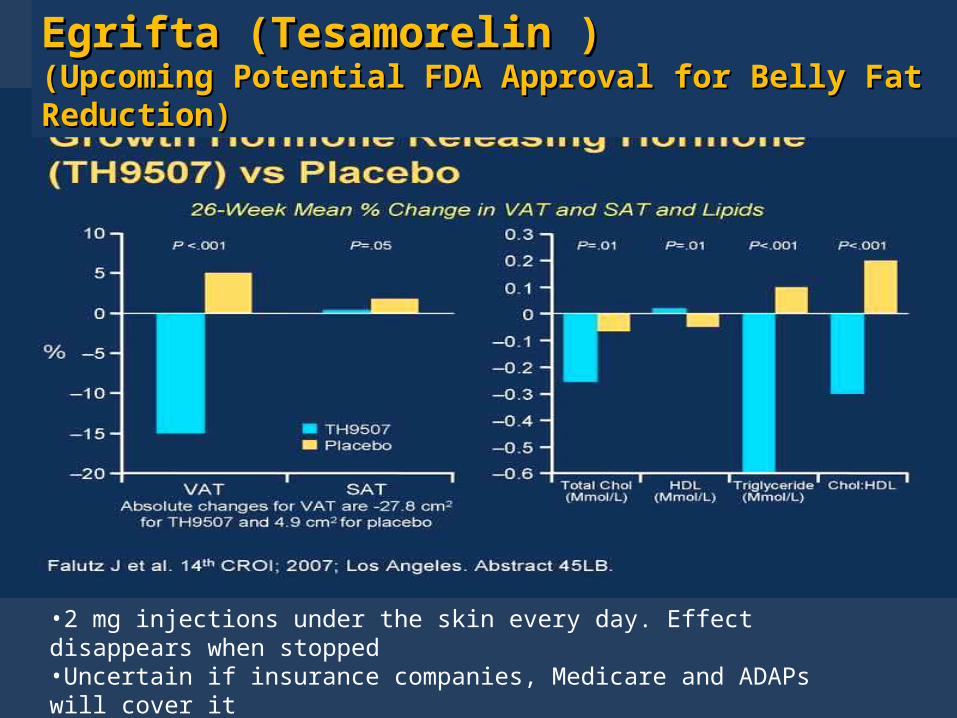
Growth Hormone Releasing Hormone (TH9507) vs Placebo
Egrifta (Tesamorelin )Egrifta (Tesamorelin )(Upcoming Potential FDA Approval for Belly Fat Reduction)(Upcoming Potential FDA Approval for Belly Fat Reduction)
•2 mg injections under the skin every day. Effect disappears when stopped•Uncertain if insurance companies, Medicare and ADAPs will cover it•A patient assistance program is being designed
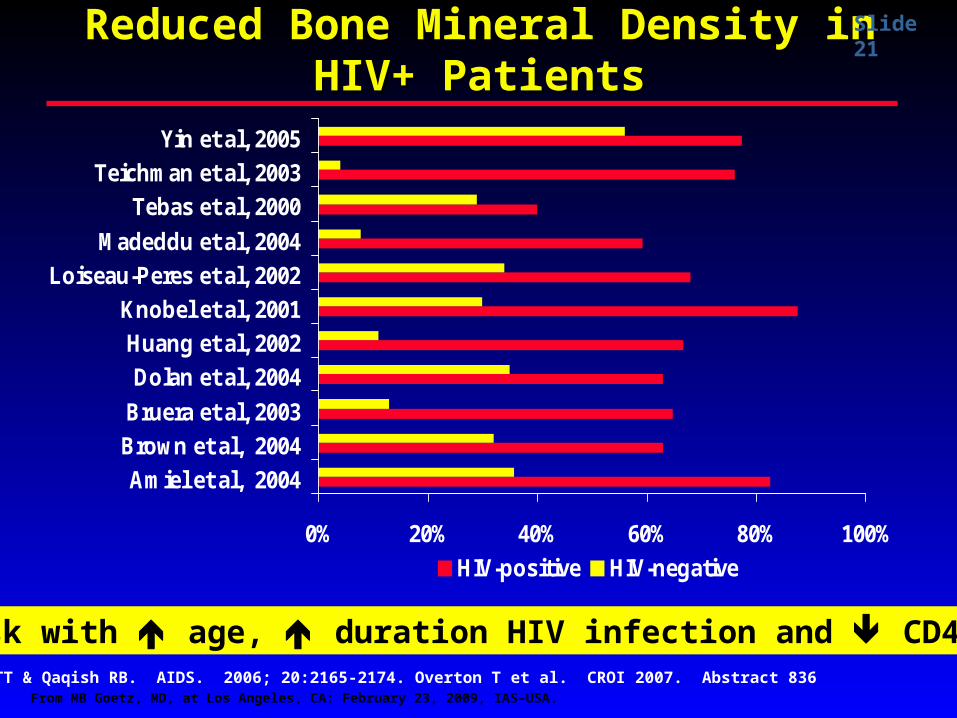
Reduced Bone Mineral Density in HIV+ Reduced Bone Mineral Density in HIV+ PatientsPatients
0% 20% 40% 60% 80% 100%
Amiel et al, 2004
Brown et al, 2004
Bruera et al, 2003
Dolan et al, 2004
Huang et al, 2002
Knobel et al, 2001
Loiseau-Peres et al, 2002
Madeddu et al, 2004
Tebas et al, 2000
Teichman et al, 2003
Yin et al, 2005
HIV-positive HIV-negative
Brown TT & Qaqish RB. AIDS. 2006; 20:2165-2174. Overton T et al. CROI 2007. Abstract 836
risk with age, duration HIV infection and CD4 nadir
Slide 21
From MB Goetz, MD, at Los Angeles, CA: February 23, 2009, IAS–USA.
Slide 15
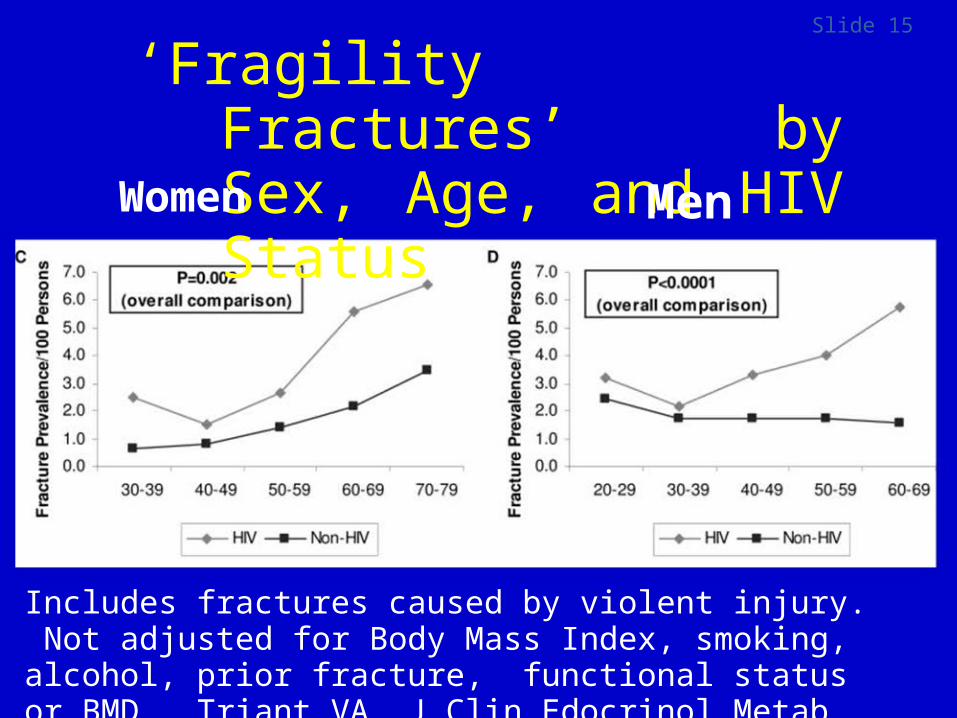
‘Fragility Fractures’ by Sex, Age, and HIV Status
Women Men
Includes fractures caused by violent injury. Not adjusted for Body Mass Index, smoking, alcohol, prior fracture, functional status or BMD. Triant VA. J Clin Edocrinol Metab 93:3499-3504, 2008
Should Dual Energy X-ray Absorptiometry (DEXA) Be Used in HIV Aging Patients?
• Developed to measure bone density• Can measure bone density, non-bone density, and fat density• Standard assessment for limb fat (normal >7 kg-8 kg)• Does not tell if truncal fat is subcutaneous or visceral• Comparison
– Error = ±1%-5%• Software and calibration• Body sections differences
– $150-$300– Quick, subject-friendly– Low radiation exposure
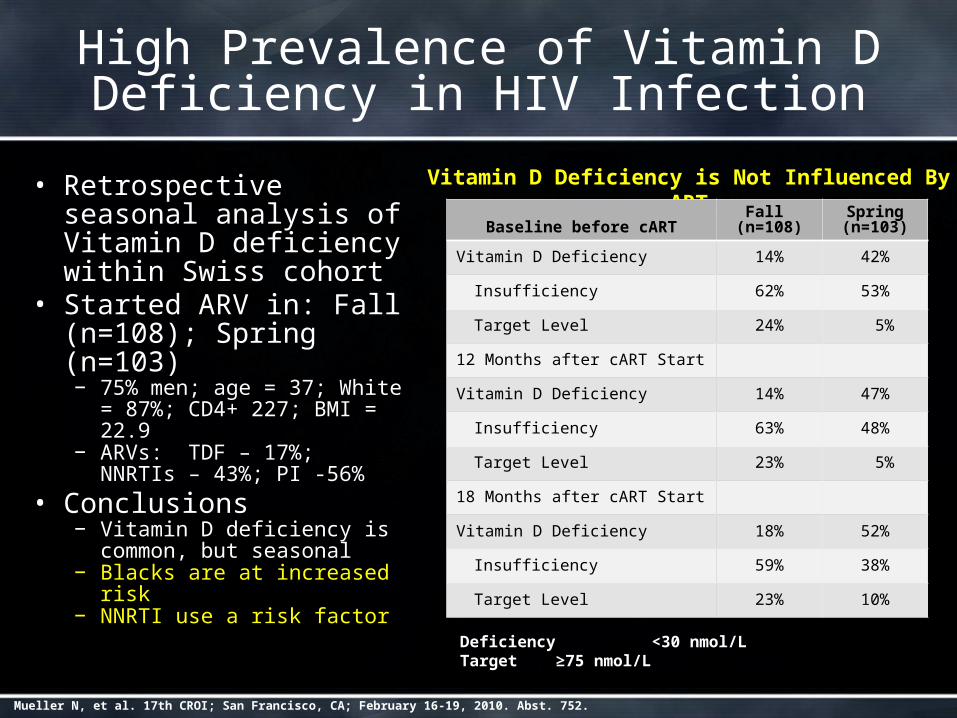
High Prevalence of Vitamin D Deficiency in HIV Infection
• Retrospective seasonal analysis of Vitamin D deficiency within Swiss cohort
• Started ARV in: Fall (n=108); Spring (n=103)
− 75% men; age = 37; White = 87%; CD4+ 227; BMI = 22.9
− ARVs: TDF – 17%; NNRTIs – 43%; PI -56%
• Conclusions− Vitamin D deficiency is
common, but seasonal− Blacks are at increased risk− NNRTI use a risk factor
Vitamin D Deficiency is Not Influenced By ART
Baseline before cARTFall
(n=108)Spring (n=103)
Vitamin D Deficiency 14% 42%
Insufficiency 62% 53%
Target Level 24% 5%
12 Months after cART Start
Vitamin D Deficiency 14% 47%
Insufficiency 63% 48%
Target Level 23% 5%
18 Months after cART Start
Vitamin D Deficiency 18% 52%
Insufficiency 59% 38%
Target Level 23% 10%
Deficiency <30 nmol/LTarget ≥75 nmol/L
Mueller N, et al. 17th CROI; San Francisco, CA; February 16-19, 2010. Abst. 752.
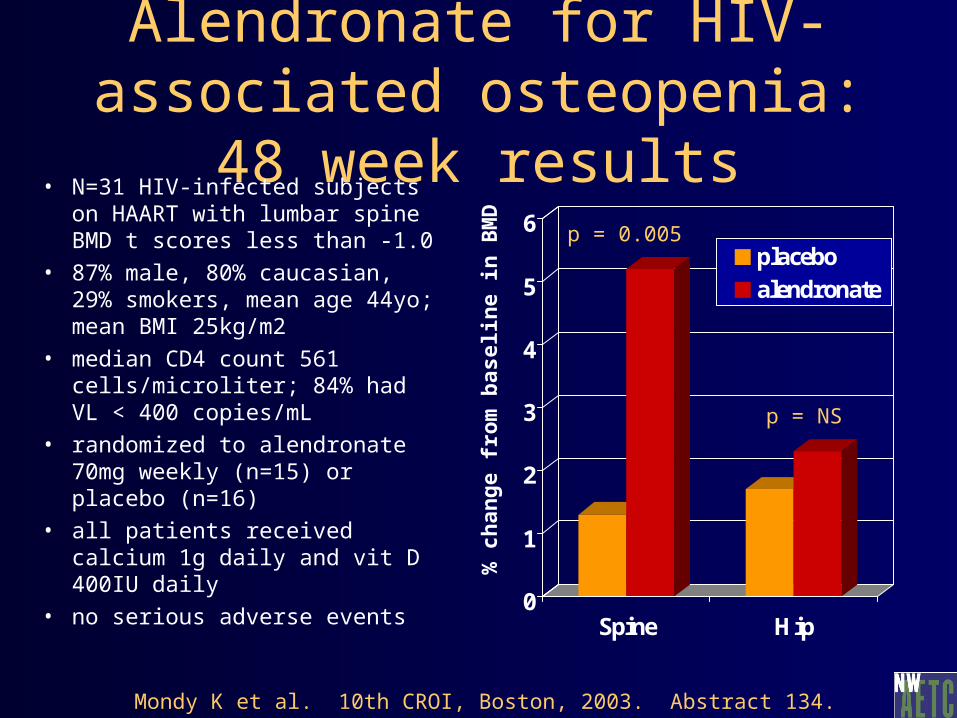
Alendronate for HIV-associated osteopenia: 48 week results
• N=31 HIV-infected subjects on HAART with lumbar spine BMD t scores less than -1.0
• 87% male, 80% caucasian, 29% smokers, mean age 44yo; mean BMI 25kg/m2
• median CD4 count 561 cells/microliter; 84% had VL < 400 copies/mL
• randomized to alendronate 70mg weekly (n=15) or placebo (n=16)
• all patients received calcium 1g daily and vit D 400IU daily
• no serious adverse events
0
1
2
3
4
5
6
Spine Hip
placeboalendronate
p = 0.005
% c
han
ge f
rom
bas
elin
e in
BM
D
Mondy K et al. 10th CROI, Boston, 2003. Abstract 134.
p = NS
What Can You Do to Help NOW?Follow Nelson’s blog : survivingHIV.blogspot.com for all of the
following action items:
Sign a letter to advocate for the inclusion of HIV as a risk factor for bone density testing for those under 50 years of age.
Monitor how Medicare will set up reimbursement of product and labor for lipoatrophy correction. Follow up petitions may be needed if this process is not done well.
Advocate for interventional therapeutic studies to reverse bone loss in HIV (vitamin D/calcium, prescription drugs, exercise, hormones). Letters to private investigators, ACTG?
Monitor how Egrifta’s reimbursement or patient assistance program is set up if approved for visceral fat reduction.
Advocate for research on the use of permanent facial lipoatrophy options like Artefill.
What Can You Do to Help NOW? Advocate for research on the use of leptin to decrease visceral fat.
Advocate for the FDA to require small sub -studies to study metabolic and body effects of drugs before approval (Phase 4 studies take too long or are never done)
Advocate for exercise/diet, vitamin D research to the NIH and private investigators in your area. Lower glycemic index diets have not been investigated in HIV. Also, help create and advocate for wellness programs that include comprehensive approaches (diet/exercise, smoking cessation, patient empowerment)
Educate your peers about metabolic issues related to different HIV medications (lipids, fat gain/loss, bone) to passify fears of naïve patients
Keep reminding investigators and congress people that physical changes in HIV are disease or drug related!
What you can do for YOU:• Manage your lipids by natural ways, with HIV medication changes
and/or lipid lowering medications.• Avoid Zerit , AZT, and higher doses of Norvir if you can• Try to minimize sugars and processed carbs to your best abilities• Maximize soluble fiber (fruits & vegetables), lean protein and good fats• Exercise 3 to 4 times a week for an hour combining resistance and
cardiovascular exercise• Take a vitamin complex twice a day• Check your hormones and supplement if needed• Research your hump liposuction and facial reconstruction options
before making a decision• Stop smoking if you do. Minimize alcohol to 1-2 drinks a day max.
For More For More InformationInformation• Email:Email:
[email protected]@yahoo.com
• Websites:Websites: www.powerusa.org
• www.medibolics.com
www.facialwasting.org
• Internet Discussion GroupInternet Discussion Group: send a blank email to : send a blank email to
[email protected]@yahoogroups.com