COPD Update Chronic Obstructive Pulmonary Disease David Henke MD, MPH N Engl J Med 356;8 Feb. 2007.
13
COPD Update Chronic Obstructive Pulmonary Disease David Henke MD, MPH N Engl J Med 356;8 Feb. 2007
-
date post
21-Dec-2015 -
Category
Documents
-
view
217 -
download
1
Transcript of COPD Update Chronic Obstructive Pulmonary Disease David Henke MD, MPH N Engl J Med 356;8 Feb. 2007.

COPD UpdateChronic Obstructive Pulmonary Disease
David Henke MD, MPHN Engl J Med 356;8 Feb. 2007

Kurosawa, H. et al. N Engl J Med 2004;350:1036
Dynamic Narrowing
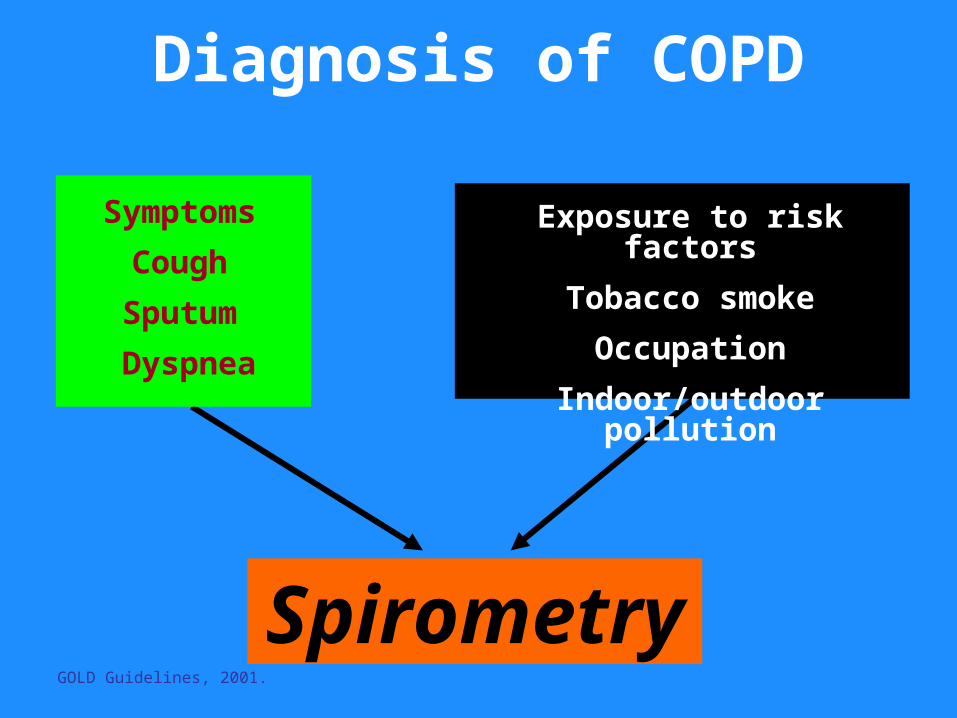
Diagnosis of COPD
Symptoms
Cough
Sputum
Dyspnea
Exposure to risk factors
Tobacco smoke
Occupation
Indoor/outdoor pollution
SpirometryGOLD Guidelines, 2001.

What Happens To Smokers?Doll-BMJ. 2004 June 26;328(7455):1519
50% of Persistent Smokers Killed By Their Habit - 25% age 35-69
Full Impact On National Mortality Takes > 50 Years To Realize
Smoking Doubles Age Specific Mortality In Middle & Old Age
Longevity Has Improved Rapidly But Not For Smokers
Stopping At 50 Y.O. Halved The Hazard
Stopping At 30 Y.0. Avoided Most Of the Risk
Smokers Die About 10 YRS. Younger
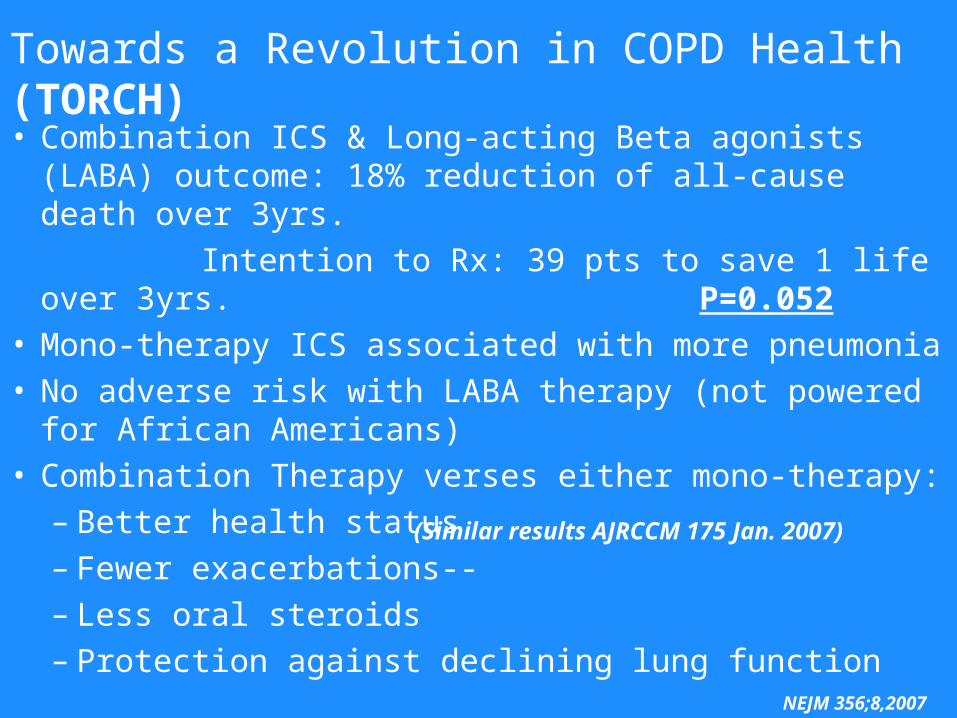
• Combination ICS & Long-acting Beta agonists (LABA) outcome: 18% reduction of all-cause death over 3yrs.
Intention to Rx: 39 pts to save 1 life over 3yrs. P=0.052
• Mono-therapy ICS associated with more pneumonia• No adverse risk with LABA therapy (not powered for
African Americans)• Combination Therapy verses either mono-therapy:
– Better health status– Fewer exacerbations--– Less oral steroids– Protection against declining lung function NEJM 356;8,2007
(Similar results AJRCCM 175 Jan. 2007)
Towards a Revolution in COPD Health (TORCH)
Clinic Patient
65 y.o. white female (60p/y smoker)w/o sx’s . Concerned about smoking, husband insisted she see MD.
Performs ADLs, worked as hostess in son’s restaurant
No SOB/DOE.
Mildly obese/ normal physical

What Do I Tell My Patient With A Concerned Husband Who Denies
Symptoms?
• I Don’t Care If You Have COPD Because You Smoke And If You Have It You Deserve It
• I’ll Give You A Valium Prescription So You Can Sedate Your Hyper-Vigilant Husband
• You May Have COPD Because You Smoke Even Though You’re Not Aware Of Symptoms. The Only Way To Be Sure Is To Perform
Spirometry.

Spirometry
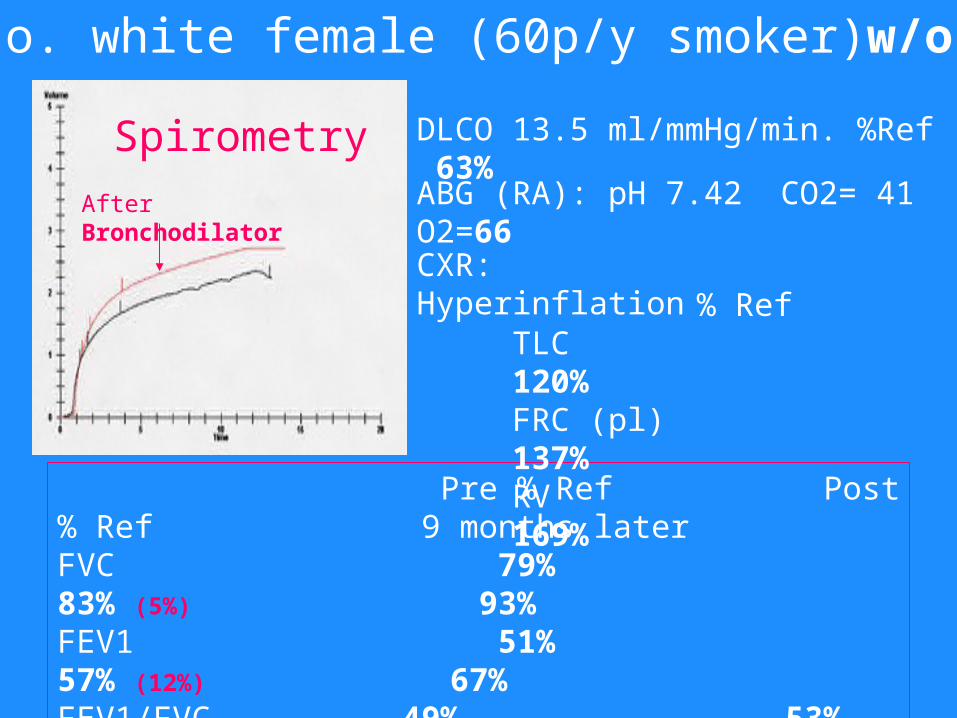
65 y.o. white female (60p/y smoker)w/o sx’s
After Bronchodilator
Pre % Ref Post % Ref 9 months laterFVC 79% 83% (5%) 93%FEV1 51% 57% (12%) 67%FEV1/FVC 49% 53% 55%25-75% 16% 30% (92%) 32%PEFR L/sec 3.67 3.97 home 2.10 4.57 home 3.75
DLCO 13.5 ml/mmHg/min. %Ref 63%
ABG (RA): pH 7.42 CO2= 41 O2=66
% RefTLC 120%FRC (pl) 137%RV 169%
Spirometry
CXR: Hyperinflation

86 y.o. male with 90 py smoking D/Ced 1968 with worsening: CRI (Cr.4.7), chronic diarrhea (?etiology), HTN, s/p CVA, s/p biliary stent.
CC: 7months of progressive DOE; new supplemental O2 need
HPI: Still active and into his business office daily without dyspnea until 7 mos. PTA developed SOB walking from the car to office. Patient now wheelchair dependent and unable to work.
Progressive Dyspnea In COPD
Page 1/3: case 84084-3
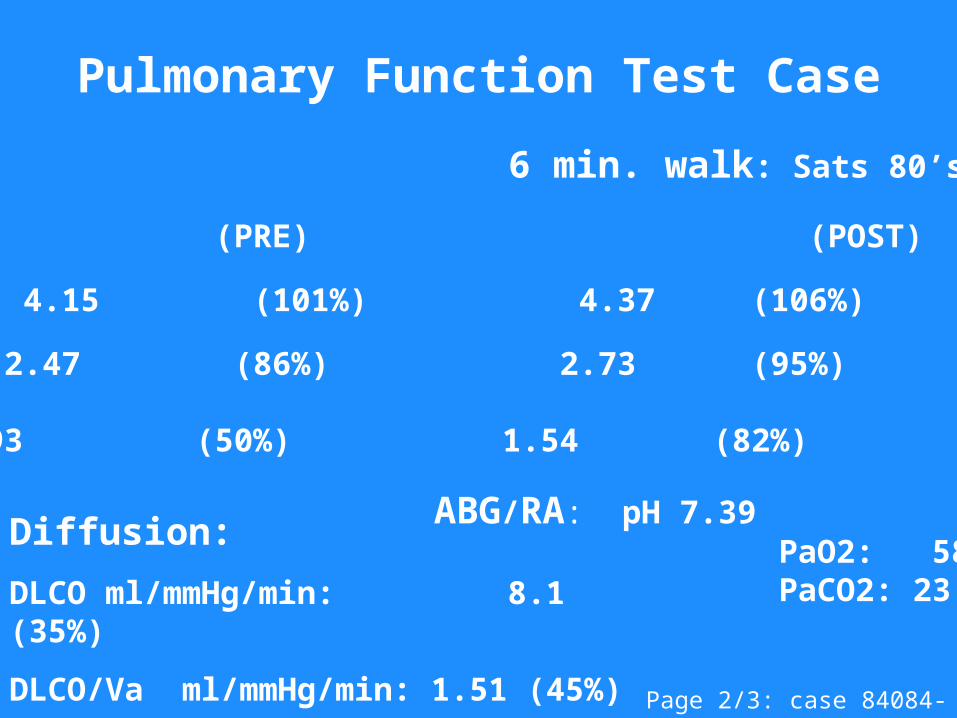
Spirometry: (PRE) (POST)
FVC 4.15 (101%) 4.37 (106%)
FEV1 2.47 (86%) 2.73 (95%)
FEF25-75 0.93 (50%) 1.54 (82%)
Pulmonary Function Test Case
Page 2/3: case 84084-3
Diffusion:
DLCO ml/mmHg/min: 8.1 (35%)
DLCO/Va ml/mmHg/min: 1.51 (45%)
6 min. walk: Sats 80’s%
ABG/RA: pH 7.39 PaO2: 58 mmHg PaCO2: 23 mmHg

High Probability VQ For
Pulmonary Embolus
Page 3/3: case 84084-3
Most COPD ptsdie from extra-pulmonary dz,e.g., 25% of severe exacerbationsw/o clear cause& resulting in hospitalizationshad PEs.(Ann Intern Med.2006;144:390)

Summary• Relay on Risk & Spirometry (symptoms) to dx COPD
•Therapeutic cornerstone in smokers with COPD:
Smoking Cessation•Only smoking cessation and maintaining
Hgb sats. > 90% prolong life•Early detection & Rx for COPD can preserve & improve lung function (Combination vs ICS or B-agonist mono-RX: may be the more effective)
•Most COPD patients die from non-pulmonary dz