Coordinated Pharmaceutical Therapy in Chronic Care Pharmaceutical... · congestive heart failure...
46
Coordinated Pharmaceutical Therapy in Chronic Care Five Innovative Programs September 2000
Transcript of Coordinated Pharmaceutical Therapy in Chronic Care Pharmaceutical... · congestive heart failure...
CoordinatedPharmaceutical Therapyin Chronic Care
Five Innovative Programs
September 2000
The National Pharmaceutical Council
is an education association supported
by the leading research-based
pharmaceutical companies.
NPC conducts research on the
appropriate use of pharmaceuticals
and the clinical, fiscal and
economic aspects of pharmaceutical
care. The Council prepares education
and information resources for
public and private payers and health
care policy makers.
© 2000 by the National PharmaceuticalCouncil. All rights reserved.

Coordinated Pharmaceutical Therapy in Chronic Care 3
Numerous studies indicate the limitations of a component-based, line item approach to the management of pharmaceuti-cals. Although some savings in the drug budget may occur,treatment outcomes may be compromised and overall expendi-tures are often increased.
A much greater potential for improved treatment and overallcost savings lies in the direction of improved coordination ofpharmaceutical care, especially for elderly and other chroniccare patients. These groups consume a disproportionate shareof health care expenditures, including pharmaceuticals. Theyusually have several coexisting diseases and are at risk foradverse consequences due to their compromised physiologicalstatus, and for interactions of prescriptions from several physi-cians. Their pharmacological needs require access to a broadrange of medications and an individualized approach to care.
Successful models of coordinated pharmaceutical care forthese and other patients at high risk for suboptimal treatmentmust be identified. This collection of five diverse approachesillustrates that coordinated pharmacotherapy can be imple-mented effectively across a variety of health care organizations.Many of the programs have resulted in improved outcomesand/or reduced overall costs of care.
This report provides detailed descriptions of the developmentand operation of these programs. These approaches may, withappropriate modifications, be applicable at other care sites,and can represent a blueprint for organizations wishing toimplement coordinated pharmaceutical care.
O V E R V I E W
Overview ....................................................................................................................................................................................... 3
Introduction ................................................................................................................................................................................. 5
Case Studies
Protecting the Vulnerable Elderly During Transition from In-patient to Home CareCrozer-Keystone Health System ................................................................................................................................................... 6
New Technologies in Burn Care Require Coordination of Pharmaceutical TherapyAlta Bates Hospital Burn Care Center .........................................................................................................................................16
Coordination of Pharmaceutical Care in High-Risk Patients with Coagulation DisordersJohns Hopkins Bayview Medical Center ......................................................................................................................................24
Centralized Accountability for Coordinated Pharmaceutical Care in a Multi-Specialty ClinicPalo Alto Medical Foundation Clinic ..........................................................................................................................................32
Education Improves Medication Management, Regimen Knowledge, and Outcomes in HIV/AIDS PatientsSan Francisco Department of Public Health...............................................................................................................................40
What the Case Studies Have Taught Us ....................................................................................................................................46
T A B L E O F C O N T E N T S

Coordinated Pharmaceutical Therapy in Chronic Care 5
Pharmaceutical innovation has greatly improved treatment out-comes and quality of life for many patients. However, the fullpotential of pharmaceutical therapy is seldom reached due to theprevalence of uncoordinated care. Chronic care patients, especial-ly the elderly, are most affected by uncoordinated care due to thecomplexity and multiplicity of their conditions and drug regimens,and their reliance on multiple care providers.
The Need for Coordinated Pharmaceutical Care
As the pace of innovation in pharmaceuticals, diagnostics, andmedical practice quickens, the “practice gap” between the avail-ability of important innovations and their most effective use iswidening. The advent of “disease management,” which hasbrought many important advances beyond episodic and uncoordi-nated care, has resulted in increased cooperation and informa-tion-sharing among providers. However, additional coordination ofpharmaceutical care is often required because disease-by-diseaseapproaches may neglect interactions among diseases and theirtreatments.
Additional factors contributing to the increased need for coordi-nated pharmaceutical care include increased numbers of medicalspecialists and sub-specialists, and the rising population of fragile,elderly patients with comorbidities. Complicating the situation fur-ther is the movement by patients through different services andsites of care of newly merged health systems.
Principles of Coordinated Pharmaceutical Care
One impediment to the realization of coordinated pharmaceuticalcare is the ambiguity regarding the definition of this concept andits principles. In 1999, the National Pharmaceutical Council (NPC)joined with the National Chronic Care Consortium (NCCC), analliance of the nation’s leading non-profit health systems, to articu-late a vision and framework for coordinated pharmaceutical care,and to outline some key principles. Ten of the most importantprinciples are as follows:
• Commitment, leadership, and support for coordinated phar-maceutical care from upper management
• Alignment of financial incentives and clinical goals across sitesof care and service sectors
• Management by interdisciplinary teams of physicians, pharma-cists, and other care providers
• Centralized responsibility and accountability for the totality ofpharmaceutical care for the individual patient
• A system for identifying patients at high risk for undiagnoseddisease and suboptimal therapy
• Ongoing assessment of drug regimens and proper prescribingand use of drugs
• Centralized knowledge of the patient’s full medical history andall currently prescribed medications
• Effective communication and feedback among care providers,especially across sites of care
• Education and involvement of the patient in the treatment plan• Evaluation of the effectiveness of coordinated care programs
These and other aspects of coordinated pharmaceutical care arefurther described in a NPC/NCCC brochure entitled IntegratingPharmaceutical Care: A Vision and Framework, which is available free of charge from NPC (www.npcnow.org).
Case Studies
The challenge now is to put these principles into practice in thereal world of care delivery. Clearly, resource constraints limit whatcan be accomplished in mounting new programs that may requirecoordinating activities across sites of care, building teams, andassembling patient-level databases. Despite this, a variety of innov-ative coordinated care programs have sprouted up across thecountry. Five of these programs are profiled here, as examples ofsuccessful approaches taken by different types of provider organi-zations. These programs embody many of the principles of coordi-nated pharmaceutical care developed by NPC and NCCC.
These case study profiles were based on interviews with individu-als who designed, championed, managed, or participated in theprograms. These individuals also provided written descriptions ofprogram details as well as information on program results. Theirsense of pride and accomplishment in launching these programswas apparent during these communications. NPC is grateful fortheir help in codifying this information. Through distribution ofthis booklet, we hope to make these innovative programs morewidely known so that others may be encouraged to implementprograms of their own.
Contributors include: Sydney Hecker, MD, Robert Scheidtman, PharmD,Bruce Bienenstock, MD, Lori Reisner, PharmD, Kathy Korbholz, EdwardC a s e y, RPh, Peter Daley, RPh, Alan J. Ross, Jerold T. Kaplan, MD, JuneM. Buckle, ScD, Mary G. Meyers, RN, MS, Phillip Zieve, MD, BurtFinkelstein, PharmD, Charles Twilley, PD, MBA, and Mathew Sharp.
I N T R O D U C T I O N
Case 1
P r o t e c t i n g t h e V u l n e r a b l eE l d e r l y D u r i n g Tr a n s i t i o n f r o mI n - p a t i e n t t o H o m e C a r e
C r o z e r - K e y s t o n e H e a l t h S y s t e mD e l a w a r e C o u n t y , P Aw w w. c r o z e r. o r g

Coordinated Pharmaceutical Therapy in Chronic Care 7
Overview................................................................................. 8
Pharmaceutical Care Assessment Program.............................. 8
Disease Management and Home Care Create Program Need... 8
The Program’s Genesis............................................................ 9
An Innovative Partnership with a Pharmacy School................. 9How the Program Works......................................................... 9
Rotation Training.............................................................. 9The Pharmacy Risk Assessment – A Standardized Tool..... 11In-Home Pharmaceutical Regimen Assessments............... 11
Intake and Planning.................................................... 12Recommendation Documentation, Communication,
and Follow-up....................................................... 13Program Results...................................................................... 13
Three Case Examples.............................................................. 14
Lessons Learned and Keys to Success...................................... 14Physician and Nurse Manager Acceptance........................ 14Anticipate Growth and Maintain Flexibility........................ 15Assessment and Data Collection Tools............................... 15
The Crozer-Keystone Health System......................................... 15
C O N T E N T S

8 Coordinated Pharmaceutical Therapy in Chronic Care
Overview
The Pharmaceutical Care Assessment Program at Crozer-KeystoneHealth System provides a real world approach to delivering coordinated pharmaceutical services to patients with complexdrug regimens. The Program’s focus is on serving elderly patientsduring their time of greatest need: the transition from in-patientcare to home care. The Program is staffed through an innovativearrangement with a nearby pharmacy school and providesenhanced coordinated pharmaceutical services for no additionalcost to patients or the health care system.
This Program reflects many principles of coordinated pharmaceu-tical care. Coordinated therapy for high-risk elderly patients isprovided during their transition from hospital to home care. In-home visits allow patients and pharmacists to work together toassess the patient’s pharmaceutical coordination requirements andindividual pharmaceutical needs. A complete medical history isretrieved from the health system’s computer. A tailored treatmentplan is developed which considers the patient’s self-care capabili-ties, medication regimens, and needs for education. Prescriptionand non-prescription drug regimens are confirmed, patientknowledge of drug regimens and diseases is determined, andappropriate education is provided. A comprehensive drug interaction and medication management review is also conducted.The results of the visit are entered into Crozer’s computer systemto become part of the patient’s permanent medical record. Afterthe visit, a telephone follow-up is conducted to review any medication or regimen changes, and to answer additional questions. An interdisciplinary management team has integratedthe program into the operations of Crozer’s home care agencies.Comprehensive education and training of the pharmacists makingin-home visits ensures a consistent standard of service.
Pharmaceutical Care Assessment Program
The Pharmaceutical Care Assessment Program was developed toaddress pharmaceutical coordination issues for high-risk, elderlypatients transferring from inpatient facilities to home care status.High-risk patients include those with multiple diseases and whorequire multiple medications. Special attention is given to potentialinteractions among prescribed medications and between these medications and over-the-counter (OTC) products. Patients entering any of Crozer-Keystone’s three home care programs areeligible for this assessment program.
An initial pharmacy assessment is made by the home care admitting nurse during the first visit to the home. Patients with high-risk scores on a standardized risk assessment intake tool arereferred to the Program for a more complete in-home assessment
by a pharmacist or board-eligible fifth year Doctor of Pharmacystudent. During this (voluntary) home visit, the patient’s pharma-ceutical care plan, self-care capabilities, medication regimens, andpharmaceutical education needs are assessed.
The results of the assessment and any pharmaceutical coordina-tion recommendations are reported to the primary care nurse andthe patient’s admitting physician on a written form or throughCrozer-Keystone’s home care medical record system. The Programteam, consisting of the Program Preceptor (a clinical pharmacistwho is the Program manager) and all current pharmacy students,reviews the results and recommendations and makes appropriateregimen modifications and education interventions, or enrolls thepatient in additional disease management programs (see below).
Disease Management and Home Care Create Need
During the 1990’s, Crozer-Keystone, like most integrated delivery systems, implemented a broad-based disease management and wellness program offering individuals and their families the latesttreatment options, technology, education, and resources. Primarycare physicians are provided with updated information from spe-cialists and specialty professional organizations regarding new treatments, medications, and care guidelines for specific diseases.
Developing these disease management and wellness programsspanning the entire care continuum highlighted the need forincreased focus on effective transitions between inpatient care and home care. The multidisciplinary team that implemented the congestive heart failure (CHF) program included physicians, inpatient nurses, and home care nurses. The CHF team quickly recognized the need for pharmaceutical coordination during thetransfer to home care.
Furthermore, in 1997, Medicare regulations required non-pharmacy-trained health care professionals (e.g., physical,speech, and occupational therapists) to provide a completeassessment of patient care, including pharmaceuticals. These regulations strengthen the need for pharmacy-trained personnel to participate or intervene when necessary in cases where nonursing involvement is present.
The Program’s Genesis
The CHF team, together with Edward Casey, RPh, Director ofPharmacy Services, worked with one of Crozer-Keystone’s threehome care agencies to launch a pilot program, staffed by a phar-macist from Crozer-Keystone and a pharmacy student from thePhiladelphia College of Pharmacy and Science.
The pilot program was, in part, a response to the launch and pro-jected growth of Crozer-Keystone’s Medicare Risk program. Underthe program, the health system was assuming global financial responsibility for an elderly patient population with many complexmedical and pharmaceutical needs. The pilot program fit the goalsand objectives of total quality improvement and cost managementrequired to build a successful Medicare Risk program.
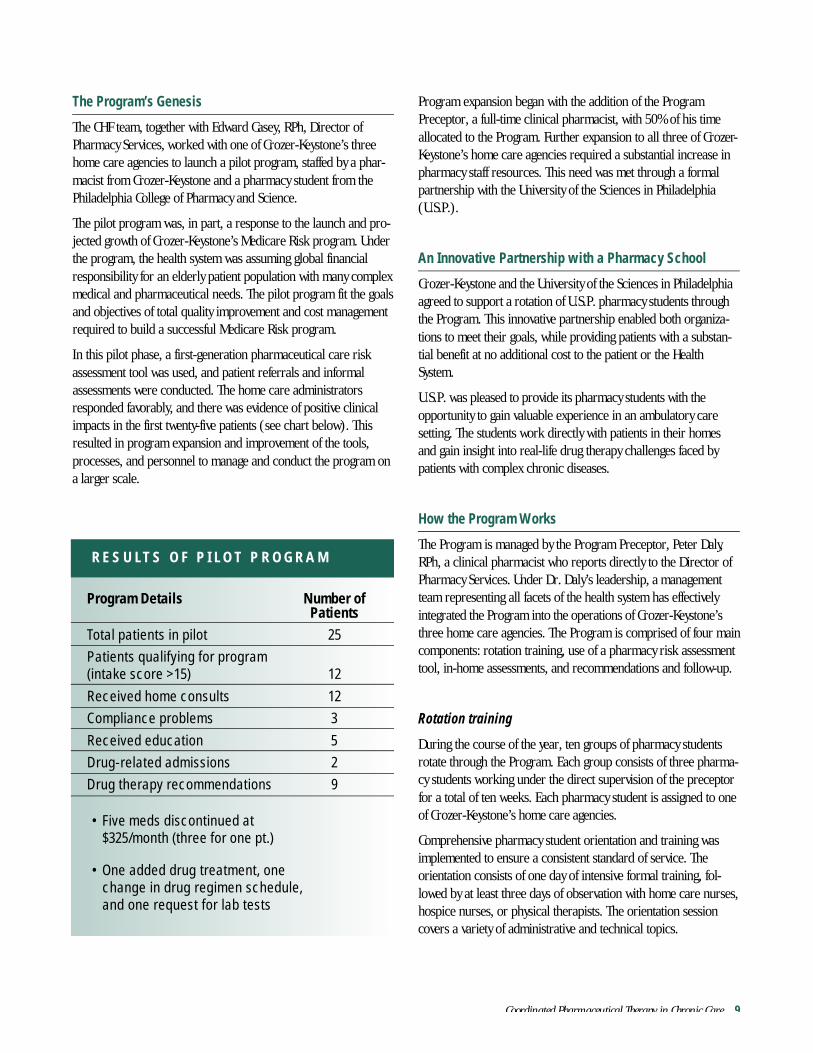
In this pilot phase, a first-generation pharmaceutical care riskassessment tool was used, and patient referrals and informal assessments were conducted. The home care administratorsresponded favorably, and there was evidence of positive clinicalimpacts in the first twenty-five patients (see chart below). Thisresulted in program expansion and improvement of the tools,processes, and personnel to manage and conduct the program ona larger scale.
Program expansion began with the addition of the ProgramPreceptor, a full-time clinical pharmacist, with 50% of his time allocated to the Program. Further expansion to all three of Crozer-Keystone’s home care agencies required a substantial increase inpharmacy staff resources. This need was met through a formalpartnership with the University of the Sciences in Philadelphia(U.S.P.).
An Innovative Partnership with a Pharmacy School
Crozer-Keystone and the University of the Sciences in Philadelphiaagreed to support a rotation of U.S.P. pharmacy students throughthe Program. This innovative partnership enabled both organiza-tions to meet their goals, while providing patients with a substan-tial benefit at no additional cost to the patient or the HealthSystem.
U.S.P. was pleased to provide its pharmacy students with theopportunity to gain valuable experience in an ambulatory care setting. The students work directly with patients in their homesand gain insight into real-life drug therapy challenges faced bypatients with complex chronic diseases.
How the Program Works
The Program is managed by the Program Preceptor, Peter Daly,RPh, a clinical pharmacist who reports directly to the Director ofPharmacy Services. Under Dr. Daly’s leadership, a managementteam representing all facets of the health system has effectivelyintegrated the Program into the operations of Crozer-Keystone’sthree home care agencies. The Program is comprised of four maincomponents: rotation training, use of a pharmacy risk assessmenttool, in-home assessments, and recommendations and follow-up.
Rotation training
During the course of the year, ten groups of pharmacy studentsrotate through the Program. Each group consists of three pharma-cy students working under the direct supervision of the preceptorfor a total of ten weeks. Each pharmacy student is assigned to oneof Crozer-Keystone’s home care agencies.
Comprehensive pharmacy student orientation and training wasimplemented to ensure a consistent standard of service. The orientation consists of one day of intensive formal training, fol-lowed by at least three days of observation with home care nurses,hospice nurses, or physical therapists. The orientation sessioncovers a variety of administrative and technical topics.
Coordinated Pharmaceutical Therapy in Chronic Care 9
Program Details Number of Patients
Total patients in pilot 25Patients qualifying for program (intake score >15) 12Received home consults 12Compliance problems 3Received education 5Drug-related admissions 2Drug therapy recommendations 9
• Five meds discontinued at $325/month (three for one pt.)
• One added drug treatment, one change in drug regimen schedule, and one request for lab tests
R E S U LT S O F P I L O T P R O G R A M
10 Coordinated Pharmaceutical Therapy in Chronic Care
Administrative topics include:• The Program’s mission, vision, and philosophy
• Risk and safety management strategies
• Clinical information systems
• Confidentiality guidelines
• Program documentation requirements
• Hospice program objectives and services
Technical topics include:• Supportive care
• Heart Success Program
• Medication administration and medication errors
• Adverse drug reactions
• Pain management
• Intravenous and parenteral therapy at home
• Infection control
• Disease management guidelines for gastroesophogeal reflux disease, asthma, arthritis, CHF pain management, and other diseases
• Drugs to be used with caution in the elderly
Screening Tool
Coordinated Pharmaceutical Therapy in Chronic Care 11
Upon completion of the orientation, the student enters field training under the supervision of the home care nurses and guid-ance of the Preceptor. The student is required to complete tenfield visits to pass the rotation. Recommendations or changes inpatient therapy require prior discussion and/or approval of thepreceptor.
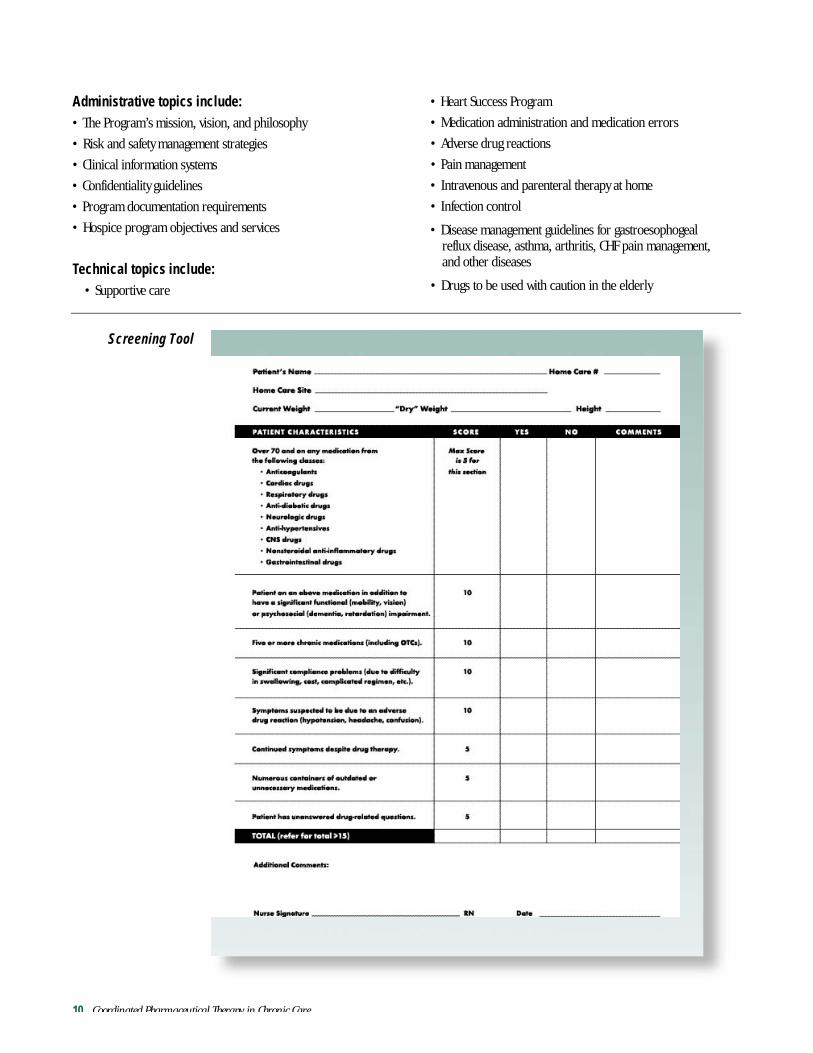
Pharmacy risk assessment: a standardized intake screening tool
The interdisciplinary team that developed the Program also developed a standardized intake screening tool to assist homecare nurses in assessing the patient’s pharmaceutical regimencomplexity and determining the need to refer a patient to theProgram.
The basic home care Pharmaceutical Care Assessment Screen(PCAS) shown on page 10 uses eight primary categories to assessa patient’s overall pharmaceutical regimen risk profile. Any patientscoring fifteen or more total points is referred to the Program foran in-home pharmacy assessment.
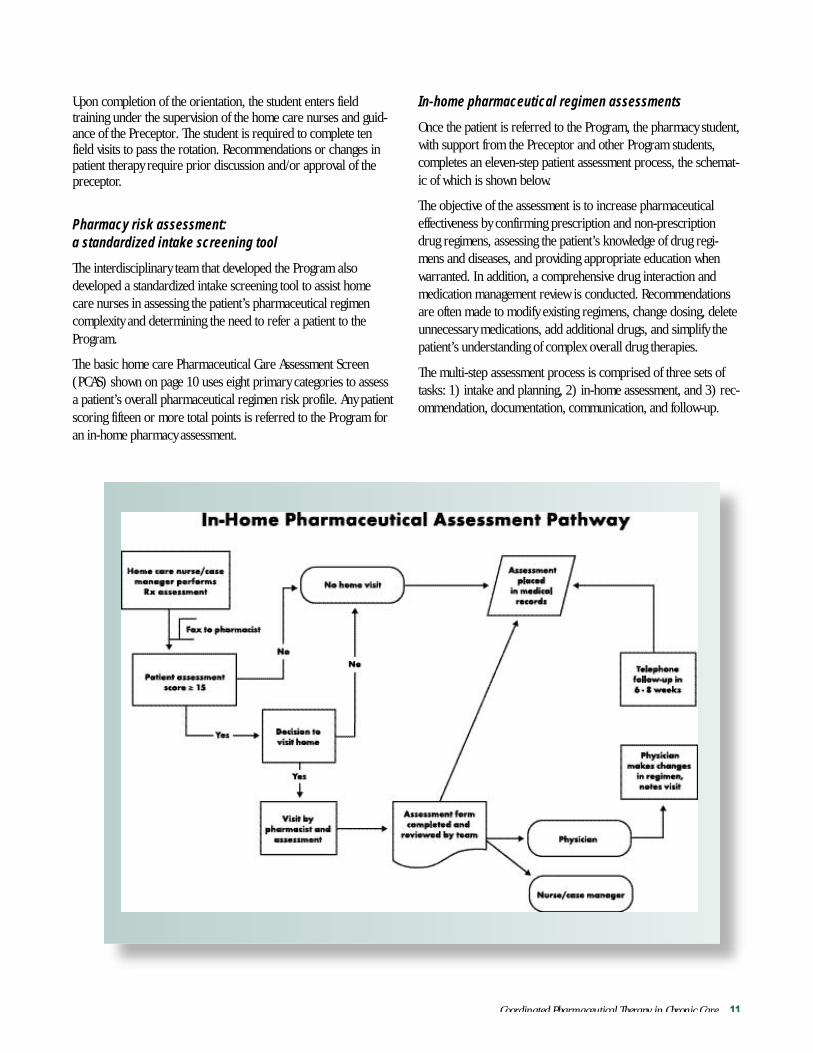
In-home pharmaceutical regimen assessments
Once the patient is referred to the Program, the pharmacy student,with support from the Preceptor and other Program students, completes an eleven-step patient assessment process, the schemat-ic of which is shown below.
The objective of the assessment is to increase pharmaceuticaleffectiveness by confirming prescription and non-prescriptiondrug regimens, assessing the patient’s knowledge of drug regi-mens and diseases, and providing appropriate education whenwarranted. In addition, a comprehensive drug interaction andmedication management review is conducted. Recommendationsare often made to modify existing regimens, change dosing, deleteunnecessary medications, add additional drugs, and simplify thepatient’s understanding of complex overall drug therapies.
The multi-step assessment process is comprised of three sets oftasks: 1) intake and planning, 2) in-home assessment, and 3) rec-ommendation, documentation, communication, and follow-up.
12 Coordinated Pharmaceutical Therapy in Chronic Care
1. Intake and planning
a. The referral is logged into the program tracking system andthe patient is assigned to a pharmacy student or programpharmacist.
b. The pharmacy student uses the Health System’s Delta computer system to retrieve a complete medical history andall patient demographic information.
c. The pharmacy student contacts the patient to schedule an in-home appointment for the pharmaceutical assessment. The student inquires about anyone assisting the patient with medication administration (friend, relative, etc.) and if
necessary includes that person in the appointment. Oncescheduled, the student notifies the primary care nurse of theappointment date and time.
d. If the patient refuses the visit, the student prepares a refusalform and submits it to the Preceptor. The refusal is thencopied to the home care nurse making the referral and documented in the electronic medical record.
e. Prior to the visit, the student prepares a patient review planhighlighting specific issues for discussion. Educational materials are assembled and potential drug interactions arechecked based on known existing prescriptions.
Coordinated Pharmaceutical Therapy in Chronic Care 13
2. In-home assessment
f. The student and patient meet in the patient’s home for aboutone hour to complete the pharmaceutical assessment. The student checks the contents of the medicine cabinet and thepatient’s pill box. They discuss the patient’s understanding ofeach prescription, when it should be taken, what it is for,special instructions, and potential adverse drug reactions.The patient is also encouraged to discuss any side effectsexperienced and to ask questions regarding medication regi-mens.
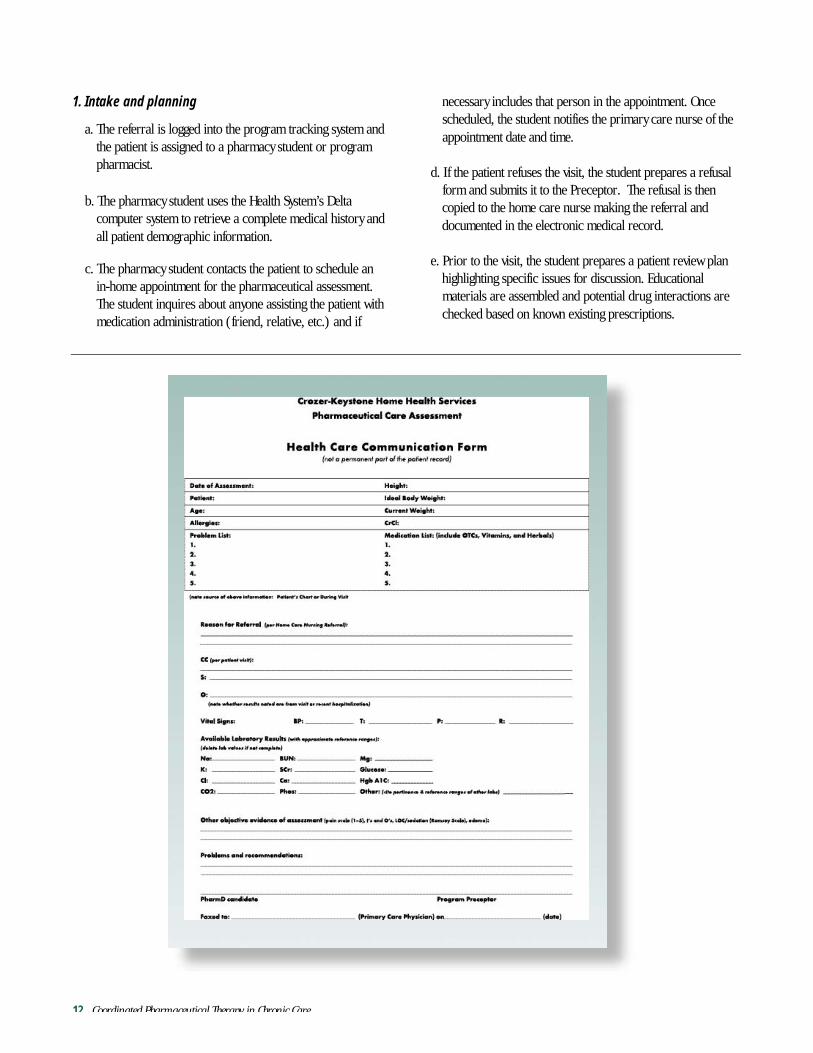
g. The home visit is documented using a standardizedPharmaceutical Care Assessment Form (see below). Thisform includes demographic information, medical history,medication lists, visit observations, and vital sign/lab reportresults. The form is completed with a succinct list of priori-tized problems and recommendations for regimen modifica-tion, additional patient education, patient assistance, andother pharmaceutical interventions.
h. The entire Program team meets weekly with the Preceptor toreview all assessment forms and recommendations. The assessment is modified to reflect team conclusions, and afinal copy is delivered to the Preceptor and the home carenurse.
A formalized tool, the Pharmaceutical Care Assessment Health CareCommunication Form supports the in-home assessment. Thisform (shown on page 12) documents key patient data, medicalproblems, all prescription and OTC medications, patient observa-tions, and recommendations. Upon completion of the form, it is
reviewed and approved by the Preceptor, and formal recommen-dations are made to the patient’s home care nurse and physician.
3. Recommendation documentation, communication,
and follow-up
i. The home care nurse is informed, in person or by voicemail, about the results of the visit, potential or existing prob-lems, and important recommendations. Critical issues foundwhile the pharmacist is still at the home are communicatedto the primary care nurse and Preceptor via pager, and cor-rective action is taken immediately.
j. The student records the patient visit and any recommenda-tions directly into the Health System’s Delta computer system,which communicates the results of the visit to all the patient’sproviders including his physician, nurses, etc. and becomespart of the patient’s permanent medical record.
k. A follow-up telephone visit is conducted to review anychanges in medications or altered regimens and to answeradditional questions. The follow-up call is documented in areport and submitted to the Preceptor and home care nurse.
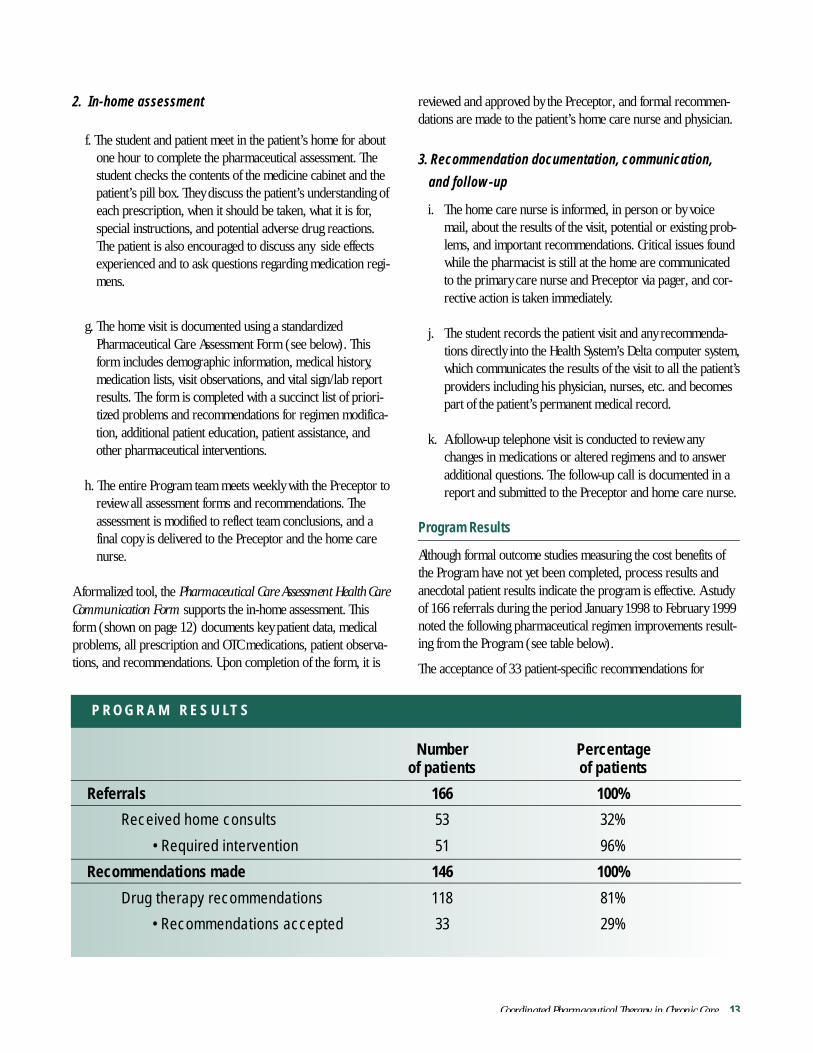
Program Results
Although formal outcome studies measuring the cost benefits ofthe Program have not yet been completed, process results and anecdotal patient results indicate the program is effective. A studyof 166 referrals during the period January 1998 to February 1999noted the following pharmaceutical regimen improvements result-ing from the Program (see table below).
The acceptance of 33 patient-specific recommendations for
Number Percentageof patients of patients
Referrals 166 100%
Received home consults 53 32%
• Required intervention 51 96%
Recommendations made 146 100%
Drug therapy recommendations 118 81%
• Recommendations accepted 33 29%
P R O G R A M R E S U LT S

14 Coordinated Pharmaceutical Therapy in Chronic Care
the 166 referrals indicates the intake assessment tool is working effectively to select appropriate patients for the Program, and the in-home pharmaceutical assessments are effectively identifying awide variety of therapy improvement opportunities.
During the three-month period from April 1, 1999 to June 30,1999 the Program received 420 referrals. Compared to the 166 referrals received from January 1998 to February 1999, thisrepresents an annual growth rate of over 1,000%. The Program’sdramatic growth during 1999 indicates an overwhelmingly positiveresponse from the home care nurses and primary care physicians.As the Program advances in the future, Crozer-Keystone plans tocomplete a comprehensive outcomes assessment and to constantlymonitor the effectiveness of the intake assessment tool and otherProgram features.
Three Case Examples Provide Evidence of the Program’sEffectiveness:
• Case 1. A 77-year-old woman was referred to the Programdue to her recent myocardial infarction and history of multi-ple medications. During the home visit, the student noted a duplication in therapy with clopidogrel plus aspirin –– a combination that resulted in an increase in bruising. Also,the patient was without a clinically indicated drug (ACEinhibitor) proven to decrease morbidity and mortality in postmyocardial infarction patients. Furthermore, the patient, whoalso has a history of asthma, was prescribed an antihyperten-sive agent but was suffering from bronchoconstriction anddifficulty in breathing. The antihypertensive has been shownto have bronchoconstrictive properties. The Program recom-mended the duplicate drugs be removed from the patient’sregimen and an ACE inhibitor added. The patient’s physicianagreed with the recommendations and implemented themimmediately, avoiding a potentially dangerous drug interac-tion. The patient has not been re-admitted to the home careprogram or hospital.
• Case 2. A 76-year-old woman, referred to the Program dueto “excruciating pain” from arthritis and spinal stenosis, wasnoted to be suffering from inadequate pain control andinsomnia. The student suggested an immediate-release narcotic for break-through pain control, combined with acontinuous-release narcotic for long-acting pain control. Achange in dosing schedule for the diuretic furosemide wasalso suggested – the dose was to be given earlier in the dayinstead of just prior to sleep to prevent frequent nocturia.The recommendations were approved by the patient’s physi-
cian and resulted in improved pain control and decreasednocturia, significantly improving the patient’s quality of life.
• Case 3. A 74-year-old woman with a history of chronic airway obstruction, heart failure, bronchitis, and arthritis wasreferred for an in-home pharmacy consult because her drugtherapy included multiple medications with possible drug-drug interactions. During the visit, the student notedseveral duplications of therapy such as for her pain control.The patient was also prescribed two corticosteriod inhalantswhile only one is clinically indicated for the treatment ofchronic airway obstructive disease. Furthermore, the patientwas prescribed guaifenesin/phenylpropanolamine andamitriptyline. Concurrent use of these medications may resultin hypertension, cardiac arrhythmias, and tachycardia. The Program recommended discontinuing four medications.The recommendations were implemented, drastically reducing the potential for adverse side effects (especiallyfalls) and potential drug interactions.
Lessons Learned and Keys to Success
Three essential lessons were learned as Crozer-Keystone imple-mented this program over the course of four years.
Physician and nurse manager acceptanceA critical factor leading to implementation of the Program was thesupport and acceptance of the health system’s physicians, and particularly the primary care nurses (case managers) at the homecare sites. Gaining support was accomplished by leveraging otherhealth system programs like the CHF disease management program. The leadership team of the CHF disease managementprogram helped identify the need for the Program; designed it tofit the needs of the physicians and primary care nurses; and builtinitial support for the implementation of pilots. The pilot programwas used to fine tune Program tools, demonstrate Program effectiveness, and broaden the support base.

Coordinated Pharmaceutical Therapy in Chronic Care 15
Anticipate growth and maintain flexibilityPharmaceutical coordination programs that are well designed,have physician and provider support, and target well-definedpatient needs are likely to experience phenomenal growth andcreate the potential for unmet demand. Maintaining initial successand momentum does not require anticipating every detail from theoutset, but rather a mindset that embraces flexibility and creativity.By effectively anticipating the potential growth of the Program,Crozer-Keystone was able to expand capacity through creative partnerships with pharmacy colleges, and through “controlledrelease” of the Program into the system’s two additional homecare agencies. By maintaining positive momentum throughout itsgrowth, Crozer-Keystone ensured the Program’s long-term success.
Assessment and data collection toolsThe importance of designing and utilizing consistent, effectivetools to perform home care intake and in-home pharmaceuticalassessments cannot be underestimated. Nurse case managers andany other health care professionals opening a case can use theintake tool as a guideline to make effective referral decisions.Similarly, the structured format of the assessment form maintainsconsistency of reporting, and guides inexperienced pharmacy students to make comprehensive assessments and recommenda-tions. Both tools can be used as a starting point for health systemsinterested in implementing a similar program, and they can be tailored to meet the specific needs of the health system, home care program, and patients.
In summary, the Program provides a rational approach to delivering coordinated pharmaceutical services to patients with complex medication regimens. In-home visits allow patients andpharmacists to work together in a comfortable, private setting toassess the patient’s pharmaceutical needs and to take appropriatecorrective action. Through an innovative arrangement with pharmacy schools, the Program can be implemented at little or no cost to the health system or its patients.
The Crozer-Keystone Health System
Crozer-Keystone Health System’s network of facilities and physicians provides residents of Delaware County, Pennsylvaniaand surrounding communities with easy access to primary careand specialty services. Crozer-Keystone consists of five hospitals with1,088 licensed inpatient beds and 649 sub-acute and skilled nurs-ing beds in its seven long-term care and transitional care unitsoperated by 1,128 medical staff. The health system includes 36 pri-mary care sites staffed by 147 physicians conducting over 200,000 office visits annually.
In addition, Crozer-Keystone operates three centers for occupational health, a sports club, and centers for family health ineach of its primary service areas.
Case 2
N e w Te c h n o l o g i e s i n B u r n C a r eR e q u i r e C o o r d i n a t i o n o fP h a r m a c e u t i c a l T h e r a p y
A l t a B a t e s H o s p i t a l B u r n C a r e C e n t e rS a n F r a n c i s c o B a y A r e a , C Aw w w. a l t a b a t e s . c o m

Coordinated Pharmaceutical Therapy in Chronic Care 17
Overview ............................................................................ 18
“Blended Medicine”........................................................... 18
Pharmaceutical Coordination in Burn Care........................ 18Effective Dosage Levels in Pain Control ........................ 18Effective Dosage Levels in Antibiosis............................. 19Dietary Concerns and Impact of Diet on
Pharmaceutical Effectiveness ...................................... 19Pharmaceutical Challenges in Discharge Planning........ 19
Coordinating Pharmaceutical Care..................................... 19The Burn Coordinator is the Hub of the
Coordination Wheel ................................................. 20Role of Pharmacists in Coordination............................ 20
Lessons Learned and Keys to Success................................. 20Unique patient circumstances heighten need for
pharmaceutical coordination .................................... 20
Nurse Coordinator role enables pharmaceutical coordination ......................... 21
Information and communication systems leverage hospital-wide resources............................. 21
The Alta Bates Hospital....................................................... 21
Appendix: Advances in Burn Care ...................................... 22
C O N T E N T S
18 Coordinated Pharmaceutical Therapy in Chronic Care
Overview
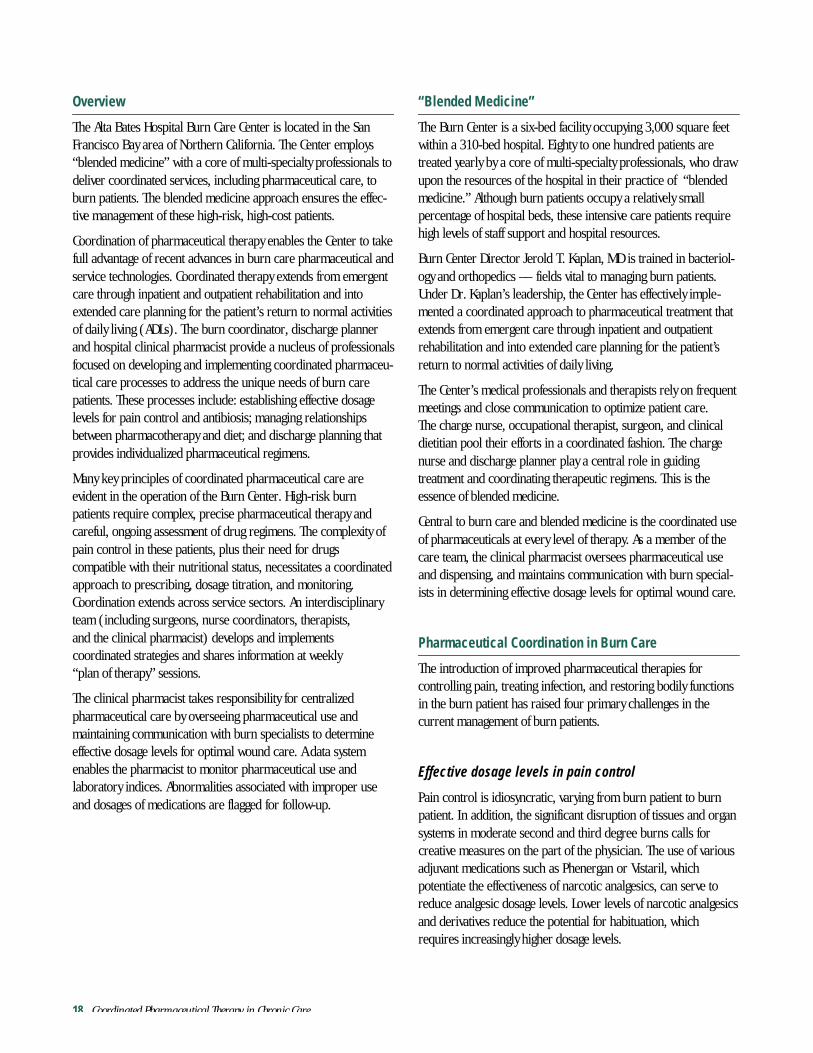
The Alta Bates Hospital Burn Care Center is located in the SanFrancisco Bay area of Northern California. The Center employs“blended medicine” with a core of multi-specialty professionals todeliver coordinated services, including pharmaceutical care, toburn patients. The blended medicine approach ensures the effec-tive management of these high-risk, high-cost patients.
Coordination of pharmaceutical therapy enables the Center to takefull advantage of recent advances in burn care pharmaceutical andservice technologies. Coordinated therapy extends from emergentcare through inpatient and outpatient rehabilitation and intoextended care planning for the patient’s return to normal activitiesof daily living (ADLs). The burn coordinator, discharge plannerand hospital clinical pharmacist provide a nucleus of professionalsfocused on developing and implementing coordinated pharmaceu-tical care processes to address the unique needs of burn carepatients. These processes include: establishing effective dosagelevels for pain control and antibiosis; managing relationshipsbetween pharmacotherapy and diet; and discharge planning thatprovides individualized pharmaceutical regimens.
Many key principles of coordinated pharmaceutical care are evident in the operation of the Burn Center. High-risk burnpatients require complex, precise pharmaceutical therapy andcareful, ongoing assessment of drug regimens. The complexity ofpain control in these patients, plus their need for drugs compatible with their nutritional status, necessitates a coordinatedapproach to prescribing, dosage titration, and monitoring.Coordination extends across service sectors. An interdisciplinaryteam (including surgeons, nurse coordinators, therapists, and the clinical pharmacist) develops and implements coordinated strategies and shares information at weekly “plan of therapy” sessions.
The clinical pharmacist takes responsibility for centralized pharmaceutical care by overseeing pharmaceutical use and maintaining communication with burn specialists to determineeffective dosage levels for optimal wound care. A data systemenables the pharmacist to monitor pharmaceutical use and laboratory indices. Abnormalities associated with improper useand dosages of medications are flagged for follow-up.
“Blended Medicine”
The Burn Center is a six-bed facility occupying 3,000 square feetwithin a 310-bed hospital. Eighty to one hundred patients aretreated yearly by a core of multi-specialty professionals, who drawupon the resources of the hospital in their practice of “blendedmedicine.” Although burn patients occupy a relatively small percentage of hospital beds, these intensive care patients requirehigh levels of staff support and hospital resources.
Burn Center Director Jerold T. Kaplan, MD is trained in bacteriol-ogy and orthopedics –– fields vital to managing burn patients.Under Dr. Kaplan’s leadership, the Center has effectively imple-mented a coordinated approach to pharmaceutical treatment thatextends from emergent care through inpatient and outpatientrehabilitation and into extended care planning for the patient’sreturn to normal activities of daily living.
The Center’s medical professionals and therapists rely on frequentmeetings and close communication to optimize patient care. The charge nurse, occupational therapist, surgeon, and clinicaldietitian pool their efforts in a coordinated fashion. The chargenurse and discharge planner play a central role in guiding treatment and coordinating therapeutic regimens. This is theessence of blended medicine.
Central to burn care and blended medicine is the coordinated useof pharmaceuticals at every level of therapy. As a member of thecare team, the clinical pharmacist oversees pharmaceutical useand dispensing, and maintains communication with burn special-ists in determining effective dosage levels for optimal wound care.
Pharmaceutical Coordination in Burn Care
The introduction of improved pharmaceutical therapies for controlling pain, treating infection, and restoring bodily functionsin the burn patient has raised four primary challenges in the current management of burn patients.
Effective dosage levels in pain control
Pain control is idiosyncratic, varying from burn patient to burnpatient. In addition, the significant disruption of tissues and organsystems in moderate second and third degree burns calls for creative measures on the part of the physician. The use of variousadjuvant medications such as Phenergan or Vistaril, which potentiate the effectiveness of narcotic analgesics, can serve toreduce analgesic dosage levels. Lower levels of narcotic analgesicsand derivatives reduce the potential for habituation, whichrequires increasingly higher dosage levels.
Coordinated Pharmaceutical Therapy in Chronic Care 19
Titration of analgesic dosage levels must take into account thepatient’s vital signs, respiratory rate, hematological and respiratorystatus, body language, idiosyncratic drug reactions, and neuromental and neurologic status. The complexity and interde-pendency of these issues requires a coordinated approach to pharmaceutical prescribing, dosage titration, and monitoring.
Effective dosage levels in antibiosis
To achieve effective levels of antibiosis to prevent infection, onemust rely upon clinical wound examination as well as such time-honored methods as antimicrobial susceptibility testing or discsensitivity testing. Proper wound culture methods are essential foreffective isolation and treatment of wound contaminants.Coordination of pharmaceutical prescribing with wound culturemethods ensures that patients receive optimal antibiotic treatmentwhile minimizing the risk of antibiotic drug resistance.
Dietary concerns and impact of diet on pharmaceutical effectiveness
Moderately to severely burned patients require more protein andcalories to compensate for what is sometimes the loss of ten percentof body weight or more at the time of injury. A delicate balanceexists between intravenous fluid intake and protein intake as well.
The registered clinical dietitian and medical staff should take electrolyte disturbances and fluid-volume disturbances intoaccount. Where intravenous nutrition is not effective, hyper-alimentation remains an option at all times. The clinicaldietitian must remain vigilant in adjusting dietary needs for burnvictims with preexistent diabetes, liver disease, or hypertension toensure the continued effectiveness of their existing therapeuticregimens during recovery from the acute burn trauma.
Pharmaceutical challenges in discharge planning
Oral medications may be used unless the patient has a venouscatheter in place for continuing intravenous home therapy. Suchpatients require daily home nursing care and periodic alterationof the intravenous site to avoid infection and skin maceration.Hence, patients lacking the means for home care nursing mustsometimes make do with oral medications exclusively. Moreover,the administration of topical wound medications and bandagingoften is beyond the scope of self-administered patient care.Appropriate discharge planning integrates the pharmaceuticalneeds of each patient with his or her individual self-care capacity,financial constraints, and caregiver circumstances.
Lastly, oral analgesics are often substituted for intramuscular analgesics at the time of discharge. The monitoring of analgesiceffectiveness and drug interactions is more problematic whenpatients must monitor their own responses to oral medicationswithout recourse to vital signs and other indices of therapeuticresponse.
Each of these issues heightens the need for coordinated pharma-ceutical care, which considers each patient’s circumstances whenselecting and administering pharmaceutical regimens across therapidly changing care continuum. As the patient moves from in-patient emergent care to outpatient rehabilitation and finally tohome care, the professional team must constantly assess a complex, interdependent array of medical, social, psychological,and financial considerations to ensure optimal pharmaceuticaltreatment.
To ensure the availability of resources required to support thiseffort, the Center Director insists that third party administratorsand reviewers provide these burn patients with all necessary ser-vices and adequate rehabilitation time to recover from theirinjuries. The Alta Bates Burn Care Foundation provides additionalsupport for medical care.
Coordinating Pharmaceutical Care
The Center fulfills the following therapeutic goals and commit-ments regarding pharmaceutical care of burn patients:
• The appropriate use of pharmaceuticals in wound care
• The selective and specific use of medications
• The selection of appropriate doses of analgesics early on toreduce drug dependency
• The reduction of antibiotic drug resistance through short-term, aggressive therapy
• The coordination of pharmaceutical therapies throughout thecare continuum
The Center maintains close adherence to these principles of therapy and provides for the specialized needs of its patients byintegration of pharmaceutical therapy through its well-coordinatedcare team. Although burn patients require relatively few basicmedications (e.g., opiates, Benadryl, silver sulfadiazine, furacin,and various antibiotics), drug interactions and iatrogenic complications are possible. These complications can result fromthe patient’s existing therapies for chronic conditions such as diabetes, liver disease, arthritis, and hypertension. The focus ofthe clinical pharmacist on the totality of drug therapy has minimized such adverse events.

20 Coordinated Pharmaceutical Therapy in Chronic Care
The Burn Coordinator is the hub of the coordination wheel
The Center is a model of multi-specialty or “blended care” medicine. Core team members, including surgeons, nurse coordi-nators, therapists, and the clinical pharmacist, meet weekly at“plan of therapy” sessions to discuss therapeutic options for theirpatients. These meetings also serve to keep all team membersabsorbed and involved in individual patient care.
While these meetings ensure that all members are involved indeveloping coordinated therapeutic plans for the patients, dailypharmaceutical coordination is the responsibility of the BurnCoordinator. At Alta Bates a specialized Nurse Coordinator (NC)performs the burn coordinator function. The NC is responsible fordressing changes, skin and wound care, tube feeding, and emer-gent care for respiratory crises, in addition to responsibility forcoordinating all pharmaceutical care. Specialized wound caretraining, and often ACL certification, enables the NC to maintaincontrol of these multiple tasks.
Along with the physician, the NC has the responsibility of titratingintravenous, intramuscular, and oral medications to achieve effec-tive pain control among patients with different pain thresholds.The Burn Coordinator must also adjust for age and health status inadministering pain medications at effective dosage levels. Burnseverity and organ and body functioning impacted by the burntrauma also influence drug dosing.
The NC assumes the role of discharge planner. The NC mustchoose the proper setting for continuing burn care and rehabilita-tion, whether at home, in a skilled nursing facility, or at a boardand care facility. The NC must wean the burn patients from hospital care while acclimatizing them to an adequate level of self-sufficiency in ADLs. This includes adequate self-care at home,psychosocial adjustment, and ability to use assistive aids such ascasts, splints, crutches, canes, or wheelchairs. The most difficultproblem the NC faces is the lack of sufficient community safetynets and resources available to the post-burn patient. Months ofpainstaking burn care and rehabilitation can be reversed by anabsence of transitional services and housing for burn patients withchronic and permanent after-effects of their injuries.
Role of pharmacists in coordination
The management of medications in burn therapy at the Center isthe province of the hospital’s clinical pharmacist. The pharmacistis assisted by a software program that monitors hospital patientsfor pharmaceutical use and laboratory indices, and that alsoserves as a pharmaceutical screening device.
When the computer notes systemic abnormalities associated withmedications, the pharmacist will “flag” the findings and send anotation to the burn physician and to the patient's chart. Thepharmacist will suggest that the physician consult with him todetermine what adjustments in dosage may be necessary or beneficial. Thus, the hospital’s coordinated information systemallows the pharmacist to effectively support the care team andNurse Coordinator in the Burn Center without being dedicated tothe Center on a full-time basis. The blended medicine model takesfull advantage of the spectrum of hospital resources without significant cost to the Burn Center.
The clinical pharmacist also closely monitors changes in bodychemistry, noting renal, hematologic, hepatic, and auditory statusconcurrent with antibiotic usage. The burn patient on aminoglyco-side therapy to combat gram-negative organisms will have frequent auditory testing. Changes in blood levels are noted and flagged for the physician's attention. In addition, the pharmacist monitors the concentration of the antiseptic furacinused in topical wound care.
Lessons Learned and Keys to Success
Over the past ten years, the Burn Center has constantly evolved itspractices to incorporate a blended medicine approach to all burncare. Through the efforts of the surgeons and nurse coordinators,this coordinated approach to patient care incorporates each of thecritical components of burn care therapy. Three keys to successenabled the effective coordination of pharmaceutical therapy intothe blended medicine approach.
Unique patient circumstances heighten need for pharmaceutical coordination
Burn victims present many immediate and long-term chal-lenges requiring a comprehensive approach to care coordina-tion from emergent care to a variety of home care settings.Many challenges were realized during the initial emergent carestage, such as the fact that wound debridement and re-hydra-tion take precedence over pharmaceutical issues. However,overall treatment success relies, in part, on effective use ofpharmaceutical therapies. Therefore, it is critical to recognizethe interdependent role of pharmaceutical therapies and theimpact other patient circumstances may have on their effec-tiveness. Explicitly recognizing these issues provides the basisfor developing a coordinated pharmaceutical therapyapproach and for complementing the blended medicine teamwith appropriate pharmaceutical support.

Coordinated Pharmaceutical Therapy in Chronic Care 21
Nurse Coordinator role enables pharmaceutical coordination
Recognizing the unique needs of burn care patients, a burncenter must centralize and clearly delineate responsibility forcoordinating all patient activities. Effective coordination ofpharmaceutical therapy relies on the coordinator being closeto the patient at all times and physically located on the BurnCenter ward. Although the Hospital’s clinical pharmacist pro-vides support and expert input to the pharmaceutical coordi-nation process, primary day-to-day responsibility is maintainedat the Burn Center and is coordinated by the NurseCoordinator. Clear delineation of the NC’s role as the coordi-nator of therapeutic interventions ensures the pharmaceuticaltherapies are monitored and adjusted in a coordinated fashionwith other patient-specific therapy and planning, such aswound debridement, dietary changes, and discharge planning.
Information and communication systems leveragehospital-wide resources
Information systems can extend the knowledge and expertiseof hospital personnel at low incremental costs. The systems atAlta Bates Hospital support the coordination of the burn teamby monitoring patients and providing feedback to team members. This is especially important for members who arenot full-time employees of the Burn Center. In particular, thesesystems allow the Center to leverage the Hospital’s clinicalpharmacist as an integral member of the team, and also convey his knowledge and support to others without his dailypresence at the Center.
In summary, Alta Bates Hospital and the Burn Center Director recognized the unique needs of burn care patients and forged acoordinated approach to treating these patients throughout theirrecovery and transition back to activities of daily living. TheH o s p i t a l ’s information systems and support departments facilitatedthis approach through creative leveraging of the Hospital’sresources. Through the efforts of the Burn Center Director and theNurse Coordinator, the Burn Center ensures these high-risk, high-cost patients receive the highest quality care.
The Alta Bates Hospital
Alta Bates Medical Center has a 90-year history of providing excellent medical care and services to the East Bay Area inNorthern California. Founded in 1905 by Nurse Alta Bates, the hos-pital is located on three major campuses in Berkeley and Oakland,and is the major referral center for the East Bay Medical Network.
Areas of excellence include :
• Burn Center
• Rehabilitation Services
• Occupational Health
• 24-hour Emergency Center
• Mental Health Services
• Bone Marrow and Kidney Transplant Programs
• Heart & Vascular Services
• Comprehensive Cancer Center
• Family Birth Center
• Perinatal Center
• Women and Infants Services
The 555-bed Medical Center has 2,700 employees and 900 physicians on staff. Its medical staff is distinguished by the fact thatmore than 90% of its active physicians are board certified.
The Medical Center supports many community programs includingthe East Bay AIDS Center, Adult Sickle Cell Anemia Program,Mentoring Program for Teens, Primary Care Access Clinic, BreastHealth Access for Women with Disabilities, Audio Health Library,and other free public health education classes.
Alta Bates Medical Center is part of the Alta Bates Health System, a non-profit organization dedicated to serving the East Bay.Its mission is to provide high-quality, accessible, affordable healthcare in a comfortable setting for families. It is affiliated with SutterHealth, which is comprised of 5,000 physicians and 25 hospitals inNorthern California.

22 Coordinated Pharmaceutical Therapy in Chronic Care
Appendix: Advances in Burn Care
Burn care medicine has advanced significantly from the field hos-pitals and “Medevac” teams who cared for burn victims in theKorean War. MASH team surgeons would debride burn sites,amputate when necessary, and skin graft when appropriate. At thattime a limited array of antibiotics was available to fight complicat-ed wound infections.
Gram-negative infection or wound sepsis were dreaded events.Patients were bathed frequently with full body immersion as a pre-lude to extensive debridement and topical care. Orthotists andprosthetists crafted bulky splints and braces in attempts to avoidjoint contractures and to restore joint mobility.
Morphine, Demerol, and Percodan were the mainstays of paincontrol. Introduction of the sulfonamides in wound care antisepsismarked a major stride in the treatment of partial and full thick-ness burns. Topical Sulfamylon cream proved quite effective inwound surface antisepsis by combating various gram-positive andgram-negative surface wound contaminants includingPseudomonas aeruginosa and some fungi.
Physiotherapists provided most of the post-burn rehabilitation,using overhead slings and pulleys to mobilize the burn victim assoon as possible. Strengthening and flexibility exercises were usedto preserve functional capacity and mobility.
Over the last 25 to 30 years, significant advances in burn carehave taken place. The sulfonamide derivative, silver sulfadiazine,has largely supplanted Sulfamylon among sulfonamide-basedcreams in topical wound care. This cream is well absorbed intothe tissues and facilitates wound decontamination so that effectiveskin grafting and wound granulation can take place. It is partiallyeffective against superinfection and wound contaminants, includ-ing many yeasts and fungi.
In addition, a powerful array of antibiotics, such as the aminogly-cosides gentamycin, and tobramycin along with the penicillinderivative Geopen (disodium carbenicillin), have been formulatedto combat the gram-negative wound contaminants such asPseudomonas and Bacteriodes. Extended spectrum antibiotics,along with heparin locks and central venous therapy, have furtherincreased antibiotic effectiveness.
New medications in respiratory medicine have contributed signifi-cantly to progress in dealing with burn after-effects or sequelaesuch as smoke inhalation, pulmonary edema, atelectasis, pul-monary obstruction, bronchospasm, and pneumonia.Bronchodilating medications such as albuterol and Atravent
expand airways and dry respiratory tissues. Steroid inhalants suchas sodium medrol are used extensively to offset bronchospasmand airway compromise.
The progression beyond disc sensitivity methods for establishingeffective Mean Inhibitory Concentrations (MICs) of antibiotics hasbeen startling. Today, modern laboratories can use an automatedsystem which examines tube-dilutions of wound bacteria grown onenriched media. Effective pharmaceutical dosage levels and identification of microorganisms is greatly accelerated. Hence,effective wound debridement and irrigation has progressed in lockstep with more effective pharmaceuticals.
Advances in orthopedics have been significant for total jointreplacement and reconstruction. Monoarthrodial and biarthrodialjoint surfaces can frequently be salvaged through plastic andmetallic implants, which restore joint mobility and function.Occupational therapists (OTs) have in many instances supplement-ed physiotherapists within burn centers. The OT tries to preserve,maintain, or restore lost functional capacity and also serves as amonitor for standards of patient autonomy and self-determination.

Coordinated Pharmaceutical Therapy in Chronic Care 23
Case 3
C o o r d i n a t i o n o f P h a r m a c e u t i c a lC a r e i n H i g h - r i s k P a t i e n t s w i t hC o a g u l a t i o n D i s o r d e r s
T h e J o h n s H o p k i n s B a y v i e w M e d i c a l C e n t e rB a l t i m o r e , M Dw w w. j h b m s . j h u . e d u
Prepared by: June M. Buckle1, ScD; Mary G. Myers2, RN, MS; Burt Finkelstein3, PharmD; Charles Twilley4, PD, MBA
1 Associate, Health Policy & Management, The Johns Hopkins University Department of Health Policy and Management, School of Hygiene and Public Health. At the time this programwas developed, Dr. Buckle was Senior Director, Care Management and Outcomes Evaluation, The Johns Hopkins Medical Center.
2 Director of Case Management. 3 Director of Pharmacy Services.4 Clinical Coordinator of Anticoagulation Service

Coordinated Pharmaceutical Therapy in Chronic Care 25
Overview............................................................................. 26
Forging a New Approach to Care........................................ 26
The Care Management Program: Framework and Governance .............................................. 26
The Care Management Executive Oversight Group........ 27The Executive Quality Management Council.................. 27
Advances in Anticoagulation Therapy Underlie the Need for Coordinated Care....................... 27
The Anticoagulation Service (ACS): An Example of Successful Pharmaceutical Coordination ...................... 28
Goals........................................................................ 28 Coordinated Pharmaceutical Care............................ 28Guidelines................................................................ 28Comorbidities .......................................................... 29New Patients............................................................. 29The Case Manager.................................................... 29Coordination of Anticoagulant Care Across Settings . 29Evaluation of the Program........................................ 30Impact of the Program............................................. 30
The Johns Hopkins Bayview Medical Center....................... 31
C O N T E N T S

26 Coordinated Pharmaceutical Therapy in Chronic Care
Overview
The Johns Hopkins Bayview Medical Center in Baltimore,Maryland has established an interdisciplinary care managementprogram that serves patients across the Center’s care delivery settings. The goal is to provide a coordinated array of services andcontinuity of care as patients move among services and providers.To accomplish this, interdisciplinary teams were organized as partof a general re-engineering of care processes and staff functions.This enabled improved management of care by linking the corefunctions of the various service entities.
As one of its initiatives, Hopkins Bayview initiated an anticoagula-tion service (ACS) for high-risk in-patients and outpatients whorequire close monitoring of medications and lifestyles. The ACSprovides continuity of pharmaceutical care, prevents sequellae,and manages overall costs for high-risk patients with various diagnoses, including atrial fibrillation, cardiomyopathy, congestiveheart failure, and other conditions requiring anticoagulation therapy and services.
After one year of operation the patients in the ACS were better ableto attain and maintain therapeutic prothrombin levels. Theyrequired fewer trips to the service and were regulated with lessfrequent testing of prothrombin levels. A reduction of 20% in totalcosts resulted from a decreased need for monitoring and bloodtests.
Several principles of coordinated pharmaceutical care are evidentin the operation of the anticoagulation service at Hopkins Bayview:
Top management was seriously committed to the coordination and continuity of pharmaceutical care for all patients, especiallyfor those moving among services and providers. Managementaggressively abolished old structures to enable the linking of corefunctions of the various services. Patients can now obtain therapywithout a trip to a distant, centralized department.
An interdisciplinary team of physicians, pharmacists and otherproviders oversees and assumes centralized responsibility andaccountability for pharmaceutical treatment of anticoagulationpatients. The service’s longitudinal database enables continuousmonitoring of drug regimens, medical history, and all currentlyprescribed medications. The service also provides education topatients, providers, and caregivers.
The service coordinates pharmaceutical care for anticoagulationpatients across the continuum of services and treatment sites. Forexample, the service works with Hopkins Home Care to enableswitches in anticoagulation therapy to be made at home that wouldnormally be performed in the hospital. Lastly, the service performsresearch to determine the effectiveness of its programs.
Forging a New Approach to Care
The Bayview staff now practices coordinated, patient-centeredcare, within a care delivery system that puts patients at the locus ofall activities. A new acute-care hospital, the Bayview Pavilion, wasdesigned with this model in mind. The hospital offers a compre-hensive, coordinated array of services on the patient care unitsranging from rehabilitation to X-ray to pharmaceutical services.This efficient system not only improves staff productivity but alsoallows patients to be treated without disruption or a trip to a distant, centralized department for testing or therapy.
In order to achieve this coordinated status, the Johns HopkinsBayview Medical Center needed to “reinvent” itself. In doing so, itwas often necessary for major service departments to abolish oldstructures and approaches. This was necessary to make room forthe development of new practice models made possible by linkingthe core functions of the various service sectors.
Rethinking and redesigning work processes was necessary toachieve dramatic improvements in critical measures of perfor-mance including quality, cost, service, and efficiency. Thisrequired managers to become change agents, and front-line staffto become empowered to redesign their work environments. Itnecessitated staff from various departments to form interdiscipli-nary teams to resolve common patient-focused problems.Redesign also included new approaches to coordinating caremanagement activities. For the pharmacy service this involved theredesign and coordination of high-quality pharmaceutical care,while selecting the most cost-effective approaches.
The new care management framework and its governance aredescribed below. An example is then provided of how an interdisciplinary team was able to coordinate pharmaceutical careto establish a successful service for anticoagulation patients, especially those with complex medical needs.
The Care Management Program: Framework and Governance
Care management at Bayview, and throughout Hopkins’ multi-organizational system, is an interdisciplinary program focused onwellness and health promotion and empowering patients throughself-care and education. The program reflects the belief that prevention and early intervention produce higher quality carewhile minimizing cost. Therefore, the program seeks to supportindividuals at the least intense level of service and in the mostappropriate setting. This is accomplished while striving for qualityoutcomes and assuring continuity of care across the continuum.

Coordinated Pharmaceutical Therapy in Chronic Care 27
The program is designed to be applied to groups of patients aswell as individuals in a variety of health care delivery settings andto create smooth transitions from one site of care to another.Therefore, new roles and new services have been created and provided, and mechanisms for evaluating quality- and value-basedcare have evolved.
The Care Management Executive Oversight Group
The Oversight Group oversees the care management program,which is an integral component of Bayview’s quality managementstructure. Group members include physicians, case managers,administrators, and representatives of all clinical departmentsincluding laboratory, radiology, and pharmaceutical services. TheGroup’s objectives include establishing strategic direction for caremanagement; integrating all clinical services into care processes;developing guidelines and extended care pathways; overseeing allclinical practice improvement initiatives; and evaluating outcomesof care. The Group oversees the development of regular guidelinereports that coordinate the clinical and financial outcomes of carefor each condition under study.
The Executive Quality Management Council
The Oversight Group reports to the Council, the committee at thehighest level of the organizational structure that evaluates the quality of clinical care. Council members include Bayview’s chiefexecutives (e.g., President, Chief Financial Officer, Vice Presidentfor Medical Affairs, physician chiefs, administrators, and clinicaldepartment directors). The Council oversees the coordination ofcare across the continuum, secures resources to advance clinicalpractice, and assures economies of scale across various commit-tees in the organization. The Council receives regular reports fromthe Oversight Group that reflect continuing progress towardsachieving improved clinical outcomes, patient satisfaction, andcoordination of new roles and services. Reports from the Councilare forwarded to the Board of Tr u s t e e s .
As a result of the commitment of these top executives to the caremanagement program, a greater emphasis was placed onadvanced, independent service roles for health care professionalsdesigned to meet the special needs of high-risk patients. T h e r e f o r e ,the activities of case managers (advanced practice nurses) andpharmacists were integrated into the care management program tomanage high-risk populations of patients with specific chronic conditions over time and care setting. The case managers focus onspecific conditions, such as congestive heart failure, and pulmonary and neurological problems. They also participate inguideline development, pharmaceutical care, and social services,and are integral to the anticoagulation program described below.
Advances in Anticoagulation Therapy Underlie the Needfor Coordinated Care
The development of new medications, and new clinical knowledgeregarding the mainstay agents aspirin and warfarin, has facilitatedtherapy for patients at risk for thromboembolism. Although warfarin has long been used to prevent thromboembolic disease,studies continue to discover and refine techniques to augment itssafety and effectiveness.
New drugs for acute-care therapy include the low molecular-weight heparin agents, an advance over unfractionated heparin,which requires intravenous administration. These agents, devel-oped in the 1990s, are smaller pieces of the heparin molecule andcan be given by subcutaneous injection. They can usually beadministered once daily, in a weight-based dose, without subse-quent monitoring or dose adjustment. Other advances includethrombolytic agents (t-PA, streptokinase, and others) for heartattacks, stroke, pulmonary embolism, and deep vein thrombosis;and agents for heparin-induced thrombocytopenia (danaparoidand recombinant hirudin).
However, therapeutic gains from these advances in acute-caretherapy can be offset by improper transition to oral, long-termanticoagulant agents, mainly warfarin. Although warfarin is aneffective anticoagulant, it has a complex dose-response relation-ship. Due to its narrow therapeutic index, significant changes inclotting time can result from as little as a 15% change in dose.Even slight underdosing can result in thrombosis, and too muchcan lead to serious bleeding. The reported combined rate ofmajor hemorrhage and thrombosis is between 10% to 20%.However, warfarin prevents 20 strokes for every bleeding episodethat occurs.
In addition, up to five days are required after any dose change (or diet change affecting vitamin K levels) to reach the newantithrombotic state. Elderly or debilitated patients often requirelower daily doses of medication; and drug interactions with warfarin are not always known or predictable.
For these reasons, blood clotting time for patients on long-termanticoagulation therapy must be closely monitored, and a varietyof tests have now become available for this purpose. One crucialadvance over the last decade is the standardization of prothrombintime testing from one laboratory to another. In addition, the abilityto test for prothrombin times at home, using whole blood fromcapillaries, now enables patient self-testing and self-managementof anticoagulant dose adjustments.
Despite the potential for improved therapy associated with thesenew medications and tests, anticoagulant therapy is often inade-quate – especially when care is not coordinated and prescribers

28 Coordinated Pharmaceutical Therapy in Chronic Care
and patients are not educated on best use of medications. Forexample, an American College of Cardiology study reported a 30%drop-off in compliance with anticoagulant therapy after one year.Often, anticoagulation therapy is not prescribed, or is under-dosed. Although warfarin is an effective anticoagulant in atrial fib-rillation, one study reported that only 38% of women with thiscondition were treated properly with warfarin. Since atrial fibrilla-tion is a leading cause of stroke, coordination of pharmaceuticaltreatment, involving both provider and patient participation, canhave a great influence on treatment outcomes and costs.
The Anticoagulation Service (ACS): An Example ofSuccessful Pharmaceutical Coordination
The ACS at Bayview was created in response to the need for coor-dinated anticoagulation therapy. The Service was designed by aninterdisciplinary team led by members of Bayview’s Departmentsof Medicine and Pharmacy. Phillip Zieve, MD and Burt Finkelstein,PharmD, collaborated to gain full support for the team from themedical staff and also gained the administration’s approval forfunding of a full-time pharmacist position.
Dr. Zieve is Physician Chief and Professor of Medicine at TheJohns Hopkins University, and a practicing clinical hematologist.Dr. Finkelstein is Director of Pharmacy Services at Bayview. Hisresponsibilities include helping to define how pharmaceutical ser-vices are managed across the System and overseeing the pharma-ceutical requirements for all in-patients and ambulatory patients. Dr. Finkelstein and the Clinical Coordinator of the ACS, senior staff pharmacist Charles Twilley, PD, MBA, are empowered to leadthe interdisciplinary team as ACS services become increasinglyintegral to the new practice model. The ACS is administered withthe philosophy that anticoagulation therapy is woven into patients’lives; and with education, knowledge, and understanding abouttheir conditions, the patients will be able to better manage theirtherapy.
Goals
The goal of the ACS is to serve high-risk anticoagulation patientswho require close monitoring of their medicines and lifestyles inorder to enhance quality of life and prevent sequellae. The ACS isdesigned to further coordinate pharmaceutical care through caremanagement processes, including monitoring and consultativeservices to physicians and health care providers. The Service oversees continuity of care for the Medical Center’s outpatients
and in-patients who require oral or parenteral anticoagulation.Emphasis is on achieving maximum benefit while minimizing cost,improving quality of life, and increasing patient and provider satisfaction.
Pharmaceutical care management for this patient population means:
• Providing monitoring and dose modifications for chronicanticoagulated patients;
• Assuring optimal anticoagulation while minimizing untoward effects;
• Assuring attainment of desired therapeutic outcomes, with minimal adverse effects and sequellae using evidence-based guidelines;
• Assisting in the transition from chronic oral to short-termparenteral anticoagulation when medically indicated;
• Providing education to patients, caregivers, and providers;
• Conducting ongoing outcomes-oriented research;
• Providing coordinated pharmaceutical care across the continuum of services.
Coordinated pharmaceutical care
Planning and designing the ACS program reflected Bayview’sthree-fold mission of patient care, education, and research.Planning included developing interdisciplinary performanceimprovement activities, contributing to the literature throughdevising and maintaining a database, and creating coordinated evidence-based practice guidelines. To further ensure coordina-tion of pharmaceuticals in the care management processes, aninterdisciplinary team developed standards for documentation,education, and accountability for pharmacotherapy.
Guidelines
Integrating pharmaceutical care necessitated that the ACS ClinicalCoordinator play a critical role in the development of evidence-based therapy management guidelines that optimize functional andmedical outcomes and minimize disability progression. The coor-dinator led the interdisciplinary guideline team, and worked withthe Medical Center’s Director of Guideline Development to ensurethat the guidelines were fully coordinated across care deliverysites. The current literature was reviewed for standards of care,and current medication practices were defined.

Coordinated Pharmaceutical Therapy in Chronic Care 29
The ACS longitudinal database contains patient, clinical, satisfac-tion, and financial information. Data are maintained on primaryand comorbid diagnoses, concomitant drug therapy, and recenthistory of anticoagulant dosing for the conditions seen in the clinic(e.g., atrial fibrillation, cardiomyopathy, congestive heart failure,and other coagulopathies). From the database, reports about drugusage practices and costs were presented to the interdisciplinaryteam to identify opportunities for performance improvement. Thebenefits of specific drugs were discussed (e.g., low molecular-weight heparin) and drug protocols were reviewed before determining the final evidence-based guideline.
Comorbidities
Among the elderly population with multiple comorbidities seen atthe clinic, coordinated pharmaceutical care plays an essential rolein identifying and managing issues of polypharmacy. Guidelinesaddress initiation and maintenance of therapy, assessment of inter-actions among multiple medications, dosing modifications, acutetransition from oral to parental anticoagulation, chronic monitor-ing of therapy, and treatment of supratherapeutic INR values. TheACS collaborates closely with physicians of patients with multiplecomorbidities, who are often the patients at greatest risk.
New patients
The intensity of anticoagulant therapy for all new patients is deter-mined by their primary care physician (PCP) or referring physi-cian. If the desired therapeutic range is not specified, it is deter-mined by the ACS physician consultant or the ACS pharmacist.Each new patient and his family or caregiver meets initially withACS staff. At this time, relevant education materials about therapyand initial laboratory values and their meanings are discussed. Fornon-English speaking patients, the service facilitates access to educational materials in the patient’s native language. Forproviders, the ACS subscribes to the newsletter AnticoagulationForum, which can be e-mailed to all on-line providers as an element of continuing education from the service.
Subsequent patient visits involve obtaining laboratory testing,adjusting dosages, and providing follow-up care. Changes in thera-py, in accordance with established guidelines, are conveyed to thepatient by telephone or in person when the patient is scheduledfor the next test. The ACS communicates with the patient frequentlyon issues such as information on drug therapy, diet, and dosechanges based on altered health status. In addition, to ensure con-tinuity of care, vacation planning is offered to patients who requiremonitoring and who are leaving the area for an extended period.
A letter is provided so that the testing can be performed at anyfacility.
The ACS also begins documentation for the medical records,which are always available for review by providers. On-line ele-ments of the electronic record give providers with security accessthe ability to gather information across the health system. In addi-tion to the ACS comprehensive database, documentation about theclinical needs and responses to therapy is maintained for thepatient’s in-patient or outpatient medical record. Also maintainedare copies of other correspondence to the patient (e.g., reminderletters, vacation letters) and correspondence to the PCP.
The case manager
When high-risk cardiac patients are admitted to the MedicalCenter, they are either screened for automatic referral or arereferred by another professional to the cardiology case manager.During the intake assessment, the case manager obtains a detailedmedication history and current usage calendar. If the patient hasbeen on outpatient anticoagulation therapy with complications inmanagement (i.e., unable to obtain a therapeutic prothrombintime), the care manager makes an additional assessment to con-sider current issues and lifestyle risk factors. For example, apatient may be noncompliant with the standard medication regi-men because it interferes with his or her work schedule. The casemanager also obtains information from the insurer about coverageissues.
All of this information is then presented to the ACS pharmacistwho determines if the patient should receive the services of theACS. Specifically, he assesses if quality of care could be enhancedand complications reduced if the patient were constantly moni-tored, had further education about self-care, and had stable thera-peutic values maintained. The case manager also presents herfindings to the patient’s PCP, orients him to the ACS service andfacilitates the PCP’s agreement to delegate anticoagulation manage-ment to the ACS.
Coordination of anticoagulant care across settings
The ACS provides services that integrate pharmaceutical careacross the continuum of services provided by the system. Forexample, the ACS works in concert with Hopkins Home Care whena transition from warfarin to heparin is needed for a patient whohas developed deep vein thrombosis. Such cases usually requirebrief hospitalization, but the ACS is able to perform this transitionin the patient’s home. The patient saves a minimum of $2,400 inout-of-pocket expenses for hospital room and board since theinsurer will likely deny the procedure as an in-patient charge.
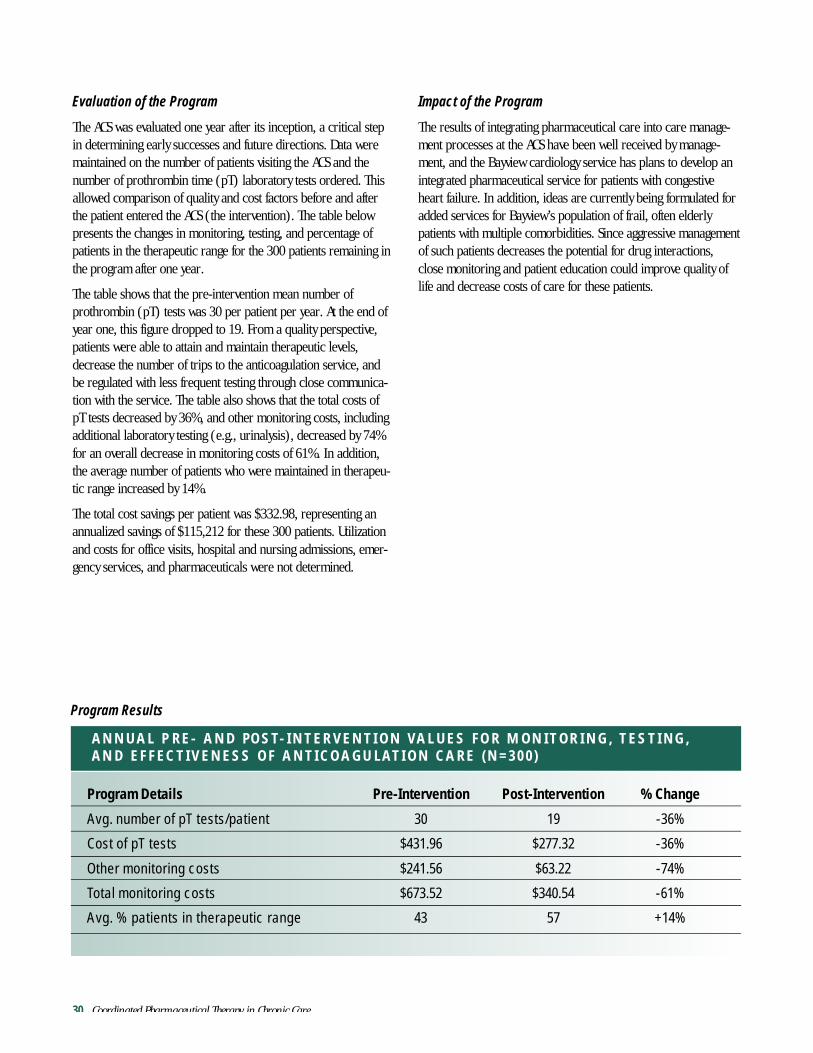
30 Coordinated Pharmaceutical Therapy in Chronic Care
Evaluation of the Program
The ACS was evaluated one year after its inception, a critical stepin determining early successes and future directions. Data weremaintained on the number of patients visiting the ACS and thenumber of prothrombin time (pT) laboratory tests ordered. Thisallowed comparison of quality and cost factors before and afterthe patient entered the ACS (the intervention). The table belowpresents the changes in monitoring, testing, and percentage ofpatients in the therapeutic range for the 300 patients remaining inthe program after one year.
The table shows that the pre-intervention mean number of prothrombin (pT) tests was 30 per patient per year. At the end ofyear one, this figure dropped to 19. From a quality perspective,patients were able to attain and maintain therapeutic levels,decrease the number of trips to the anticoagulation service, andbe regulated with less frequent testing through close communica-tion with the service. The table also shows that the total costs of pT tests decreased by 36%, and other monitoring costs, includingadditional laboratory testing (e.g., urinalysis), decreased by 74%for an overall decrease in monitoring costs of 61%. In addition,the average number of patients who were maintained in therapeu-tic range increased by 14%.
The total cost savings per patient was $332.98, representing anannualized savings of $115,212 for these 300 patients. Utilizationand costs for office visits, hospital and nursing admissions, emer-gency services, and pharmaceuticals were not determined.
Impact of the Program
The results of integrating pharmaceutical care into care manage-ment processes at the ACS have been well received by manage-ment, and the Bayview cardiology service has plans to develop anintegrated pharmaceutical service for patients with congestiveheart failure. In addition, ideas are currently being formulated foradded services for Bayview’s population of frail, often elderlypatients with multiple comorbidities. Since aggressive managementof such patients decreases the potential for drug interactions,close monitoring and patient education could improve quality oflife and decrease costs of care for these patients.
Program Details Pre-Intervention Post-Intervention % Change
Avg. number of pT tests/patient 30 19 -36%
Cost of pT tests $431.96 $277.32 -36%
Other monitoring costs $241.56 $63.22 -74%
Total monitoring costs $673.52 $340.54 -61%
Avg. % patients in therapeutic range 43 57 +14%
A N N U A L P R E - A N D P O S T- I N T E R V E N T I O N VA L U E S F O R M O N I T O R I N G , T E S T I N G , A N D E F F E C T I V E N E S S O F A N T I C O A G U L AT I O N C A R E ( N = 3 0 0 )
Program Results
Coordinated Pharmaceutical Therapy in Chronic Care 31
The Johns Hopkins Bayview Medical Center (JHBMC)
JHBMC has a long history of employing performance improvementapproaches when addressing systems issues, especially for chroniccare patients. The three-fold mission of JHBMC focuses on excellence in patient care, teaching, and research. A state-of-the-art, hospital-based outpatient facility was completed in1999, ensuring that patients have access to and receive quality care across the health care continuum.
The JHBMC offers a comprehensive array of clinical services for per-sons with chronic conditions, including hospital, primary care, pre-vention, and specialty care services to the Southeast Baltimore com-munity, the greater Baltimore metropolitan community, as well as an international population. JHBMC is a full-service, 700-bed community teaching hospital and long-term care facility housing Maryland’s only regional burn cen-ter, and an area-wide trauma center; as well as centers for renal dialysis, a neonatal intensive care, and a sleep disorders center.
Johns Hopkins Geriatrics Center is one of the national demonstration sites for the Program of All-Inclusive Care for the Elderly (PACE). The Center provides residential and outpatientday and respite care, home and office-based assessments, andhouse calls. The National Institute on Drug Abuse and the gerontology section of the National Institute of Aging are also located on the campus.
JHBMC staff works closely with Johns Hopkins Bayview Physicians,PA, a not-for-profit, multi-specialty practice whose physicians arefull-time faculty of Johns Hopkins School of Medicine. JHBMC is alsoa major teaching site for the School of Medicine, and has its own teaching programs in medicine andgeriatrics.
Case 4
C e n t r a l i z e d A c c o u n t a b i l i t y f o rC o o r d i n a t e d P h a r m a c e u t i c a lC a r e i n a M u l t i - S p e c i a l t y C l i n i c
P a l o A l t o M e d i c a l F o u n d a t i o n C l i n i cP a l o A l t o , C Aw w w. p a m f . o r g

Coordinated Pharmaceutical Therapy in Chronic Care 33
Overview................................................................................. 34
Coordinating Pharmaceutical Care.......................................... 34
Managed Care Fuels Need to Coordinate Pharmaceutical Care 35
The Path to Pharmaceutical Coordination............................... 35
An Innovative Funding Model Leads to Implementation .......... 36
Quality Improvement and Pharmaceutical Coordination......... 36Pharmaceutical Coordination through
Disease Management of Depression........................... 36Pain, Lipid-lowering, and Anticoagulation Clinics............. 37Frequent Visitor Program.................................................. 38
Benefits of Accountability for Pharmaceutical Coordination.... 38
Lessons Learned and Keys to Success...................................... 39Focus on Pharmaceutical Coordination
to Achieve Competitive Advantage................................ 39Link Pharmaceutical Utilization with Outcomes
to Enable Process Improvement................................. 39Centralize Responsibility for Pharmaceutical Coordination
to Facilitate Process Improvement.............................. 39
The Palo Alto Medical Foundation........................................... 39
C O N T E N T S

34 Coordinated Pharmaceutical Therapy in Chronic Care
Overview
This case study examines the driving forces that led to centralizedresponsibility for pharmaceutical coordination at the Palo AltoMedical Foundation Clinic, and how pharmaceutical coordinationis key to the effectiveness of various quality improvement projects.
Management’s assumption of responsibility for pharmaceuticalcoordination has enabled an increased focus on the role of phar-maceuticals in care improvement initiatives. Adding pharmaceuti-cal coordination to these ongoing initiatives has resulted in perfor-mance improvement throughout the Clinic’s patient population.
Many principles of coordinated pharmaceutical care are evident in this case study:
The Clinic has aligned its financial incentives and clinical goalsthrough its focus on coordination of drug therapy. The Clinicbelieves that although aspects of coordinated pharmaceutical care,such as education and improved compliance, may result inincreased prescription use and costs, overall costs are likely todecrease due to reduced use of services.
A key feature of this program is its emphasis on centralizedresponsibility for pharmaceutical coordination. Top managementassumed this responsibility and assigned cross-service account-ability for this function to a clinical pharmacist, who reports tosenior management.
Accurate pharmaceutical and clinical databases provide vital support to the Clinic’s quality improvement programs. A robustprescription database enables analysis of physician prescribing,identification of areas for improvement, and the targeting of follow-up education efforts. These databases remove the Clinic’sdependency on its HMO contracting partners for critical information.
The Frequent Visitor Program identifies high-risk patients whorequire additional attention and a high level of provider coordina-tion. Using the prescription database, a number of critical condi-tions were identified, including asthma, depression, diabetes, andother chronic diseases. The database also identifies patients whowould benefit from further pharmaceutical coordination efforts,including patient education, counseling, and compliance support.
High-risk, chronic care patients are also served by disease-focusedclinics that provide ongoing education, counseling, and conditionmonitoring. It is anticipated that these efforts will increase medication compliance, identify drug interactions, and supportlifestyle habits that complement drug therapies.
The disease-focused clinics are managed through a teamapproach involving a combination of providers and educators,including pharmacists, nurses, and physicians. Linking activities inthese clinics with each patient’s primary care physician ensuresmaximum coordination of pharmaceutical therapies.
Physician education is provided by the clinical pharmacist, whodevelops and delivers follow-up education to targeted physicians.The pharmacist also maintains Clinic-wide physician educationprograms. This education is essential to the success of the Clinic’sdisease management programs. Patient education is enhanced bythe Clinic’s web site, which provides answers to frequently askedquestions.
Coordinating Pharmaceutical Care
The Palo Alto Medical Foundation is a multi-specialty group practice that operates three primary clinics in the Silicon Valley.More than 186 physicians and 848 nurses and support staff deliver pediatric, family practice, internal medicine, and OB/GYNservices. Over 50% of the Clinic patients are managed careenrollees. The Foundation’s clinics (collectively referred to as “the Clinic”) have implemented many initiatives designed to coordinate and improve patient care. Coordinating pharmaceuticalcare is an essential element of these efforts.
Several key factors underlie the Clinic’s success in pharmaceuticalcoordination and resultant benefits. Top management has assumedresponsibility for pharmaceutical coordination, and has assignedcentralized, cross-service accountability for this function. This hasprovided a framework for successful implementation of manyquality improvement programs. In addition, the linkage of phar-maceutical utilization data with treatment outcomes data has facilitated treatment process improvement. This linkage and otherelements of pharmaceutical coordination have provided knowl-edge of drug utilization patterns and their relationships with treat-ment outcomes and costs. This information is especially importantin projecting costs for contracts based on global capitation.
The impetus for the program and key stages of its evolution areexamined in this case study which describes the implementation ofPalo Alto’s depression disease management, anticoagulation, andfrequent visitor initiatives. Multi-specialty clinics like the Palo AltoMedical Foundation are well-suited to leading the pharmaceuticalcoordination effort with the assistance of their health plan contracting partners and other health care industry participants.
The linchpin of the Clinic’s success in coordinating pharmaceuti-cal care has been the centralized accountability for pharmaceuti-cal coordination. This accountability rests with the Clinic’s clinical

Coordinated Pharmaceutical Therapy in Chronic Care 35
pharmacist who reports to the Assistant Director of Health Plans, amember of the senior management team. The clinical pharmacistis responsible for supporting all quality improvement initiativesthat have pharmaceutical aspects across all three clinics.
This case study examines the driving forces that led to centralizedresponsibility for pharmaceutical coordination, and how pharma-ceutical coordination is key to the effectiveness of various qualityimprovement projects.
The assumption of responsibility for pharmaceutical coordination,and assigning this responsibility to the clinical pharmacist, hasenabled an increased focus on the role of pharmaceuticals in careimprovement initiatives. In addition, the Clinic has assembled theprescription databases necessary for developing and monitoringquality improvement initiatives. These databases remove theClinic’s dependency on its HMO contracting partners for criticalinformation. Adding pharmaceutical coordination to its ongoingcare improvement initiatives, and supporting them with a clinicalpharmacist, has resulted in accelerated performance improvementthroughout the Clinic’s patient population.
Managed Care Fuels Need to CoordinatePharmaceutical Care
As managed care growth skyrocketed in Northern California in the1990s, the need to manage the quality and cost of medical carebecame increasingly important to the Clinic’s managed care customers. Most California health plans eventually included a prescription benefit, and these plans sought to control prescription spending through a host of benefit design featuressuch as generic switching, restrictive formularies, and prior authorization. The health plans also asked the Clinic for assistancein managing physician prescribing patterns. Thus, the Clinic wasdriven by its customers to analyze, monitor, and alter prescribing,believing that this would lower drug costs.
The Clinic does not directly benefit from any drug cost savings that have accrued from these efforts; the financial risk for thepharmaceutical benefit is currently borne by the health plan, andis managed by a PBM or the plan itself. Although global risk contracts are increasingly common, the Clinic receives fixed (capitated) payments only for professional services.
However, the Clinic realizes the value of taking responsibility formanaging the total cost and quality of care, including pharmaceu-ticals. Thus, the Clinic is coordinating and managing pharmaceuti-cal care despite its inability to benefit from any reductions in drugcosts. Such reductions may result from its programs targetinginappropriate use of resources (e.g., the Frequent Visitor Program
described below). Implementation of other coordinated care programs, including clinical guidelines, education, and improvedcompliance, may increase prescription use, although overall costsare likely to decrease due to reduced use of services. Increaseddrug costs accompanied by lower overall costs may result fromthe Clinic’s coordinated programs for depression, pain, lipid, andcoagulation disorders (see below). Underuse of medications,resulting in compromised outcomes, is common for all of theseconditions.
By focusing on pharmaceutical coordination, the Clinic believes itwill increase its knowledge of pharmaceutical utilization issues,create more coordinated health care service models, and increasethe overall effectiveness of care. The competitive advantage that isgained from this knowledge will help the Clinic estimate risk forthe drug budget component of global risk arrangements in thefuture.
The Path to Pharmaceutical Coordination
In 1990, Medical Director Sydney Hecker, MD, and Director ofPharmacy Robert Scheidtman, PharmD, began coordinating phar-maceutical care at the Clinic. They soon realized that the prescrib-ing patterns of its physicians were extremely diverse and could notbe easily analyzed due to a lack of valid, useful prescribing data.Although the Clinic received reports of physician prescribing pat-terns from the various HMOs, the reports came intermittently; indifferent formats; on small patient populations; and were based oncomparisons to each HMO’s unique formulary. Therefore thereports were inadequate for analyzing the true prescribing pat-terns of the Clinic’s physicians. Using the reports as a basis forcoordinating pharmaceutical care throughout the Clinic provedineffective and became the genesis for the Clinic’s current efforts.
Hecker and Scheidtman set out to coordinate pharmaceutical careusing a three-pronged approach:
• Develop useful physician prescribing profiles based on adatabase of reliable, complete, and timely prescribing datafor all patients served by the Clinic,
• Create a prescribing guideline designed to meet the objectiveof delivering cost-effective, high-quality medical care, and
• Increase focus and accountability for coordinating pharma-ceutical care by creating a clinical pharmacist role as aresource for professional teams.
Hecker previously chaired a pharmacy and therapeutics commit-tee for an association of physician groups, and the committee

36 Coordinated Pharmaceutical Therapy in Chronic Care
developed an objective pharmaceutical guideline as a tool. Heckerinitially used this guideline to assist the Clinic in developing andevaluating disease management programs. The guideline served asa standard against which all pharmaceutical performance couldbe measured, and effectively replaced the various formularies usedby the managed care plans to create physician-prescribing reports.The Clinic subsequently developed its own guideline, specifically toencourage and measure the quality of pharmaceutical prescribingby the Clinic’s physicians.
Simultaneously, Scheidtman began building broad-based supportfor creating a clinical position to coordinate pharmaceutical carethroughout the Clinic’s many quality improvement initiatives. Thisposition was ultimately filled with a clinical pharmacist, using aninnovative funding model that leveraged both public and privatefunds.
An Innovative Funding Model Leads to Implementation
Although there was a groundswell of support for the clinical pharmacist position and the need was clearly recognized, garnering management approval for creating the position waschallenging since it was difficult to quantify the hard-dollar returnon the investment.
Scheidtman proposed creating the position with primary fundingfrom nine pharmaceutical company partners. These firms con-tributed a total of $65,000 toward funding the clinical pharmacistposition. In addition, the Clinic struck a partnership arrangementwith the University of California San Francisco School of Pharmacy.Under the arrangement, UCSF would place a clinical pharmacist atthe Clinic and assume responsibility for 50% of the salary. Thisprovided real-life experience in a medical group setting as part ofthe UCSF curriculum. The combination of pharmaceutical compa-ny funding and the partnership with UCSF allowed the Clinic tocreate the position on a provisional basis. After the first year, thereturn on investment from the position was clear, and manage-ment approved the position on a permanent basis.
The clinical pharmacist has facilitated the coordination of pharmaceutical care within this large clinic, especially throughactivities associated with its disease management programs. Such activities include:
• Networking with pharmaceutical company representatives toidentify the most recent clinical studies in the disease area
• Identifying, researching, and analyzing the most relevant clinical and pharmacoeconomic studies in the disease area
• Analyzing practice patterns and interviewing physicians todevelop a primary care physician needs assessment
• Assisting process improvement teams to develop cost-effective, high-quality clinical guidelines tailored to theneeds of Clinic physicians
• Delivering follow-up education to targeted physicians
• Developing and delivering Clinic-wide physician educationprograms
• Developing and maintaining a prescription database that canbe used to monitor the program’s effectiveness
Quality Improvement and Pharmaceutical Coordination
Pharmaceutical coordination is evident in the operation of three ofthe Clinic’s quality improvement initiatives: disease managementprograms, lipid-lowering and anti-coagulation clinics, and theFrequent Visitor Program. These programs rely on the establish-ment and maintenance of accurate clinical databases, analysis of clinical patterns, management of care delivery teams, and education of providers on pharmaceutical care. These functionsare best carried out within a framework of centralized account-ability for pharmaceutical coordination.
Pharmaceutical coordination through disease management of depression
The Clinic is implementing a number of disease management(DM) programs as part of an overall effort to improve patientcare. These programs focus on complex patient populations thatrequire a high degree of service coordination to maximize thequality and cost-effectiveness of care. The depression initiativeclearly demonstrates the value of DM programs that coordinatepharmaceutical care.
The DM program for depression focuses on developing and imple-menting a depression treatment guideline for patients in primarycare. Bruce Bienenstock, MD, head of the Clinic’s psychiatry services, initiated the depression DM program by gaining approvalfrom the Quality Assurance and Clinical Improvement Board. The proposed program included four primary components: 1) documentation of current treatment patterns and primary carephysician needs; 2) development of a depression treatment guide-line; 3) education of primary care physicians on the guideline;and 4) monitoring results.
Documenting current disease treatment patterns and primary carephysician needs enabled the clinical pharmacist, Dr. Lori Reisner,to perform chart reviews and credibly discuss treatment alterna-tives and education needs with the primary care physicians. After numerous meetings with primary care physician groups,

Coordinated Pharmaceutical Therapy in Chronic Care 37
Drs. Bienenstock and Reisner had a clear understanding of physician needs related to identifying and treating patients withdepression in their practices.
This needs assessment assisted them in gathering information forguideline development. Such information included clinical studies,reviews, AHRQ and other guidelines, and DM programs. Thesewere used to build an evidence-based treatment guideline forhigh-quality care, tailored to the needs of the Clinic’s primary carephysicians.
Dr. Reisner played an important role in assembling and assessingthe information upon which the guideline was based. Dr. Bienenstock said, “Dr. Reisner brought unique skills to theteam and an ability to effectively interface with pharmaceuticalcompany representatives to gather clinical evidence.” In addition,her perspective added value to the analysis of various studies andalgorithm options. The final algorithm summarized the preferredtreatment regimen on one page, accompanied by a compendiumof supporting facts and studies.
Although algorithm development is critical, the most importantstep in the program was educating primary care physicians on thebenefits of SSRI antidepressant medications and other recom-mended treatment options. The clinical pharmacist delivered mostof the training on depression, as well as specific informationdelineating drug products, to the primary care physicians. Theclinical pharmacist’s role as an educator is essential to successfulimplementation of DM programs within the medical group setting.
Finally, no clinical performance improvement process is completewithout a thorough measurement and monitoring system in place.Dr. Reisner oversees this system using a robust prescription data-base developed by combining the numerous data feeds receivedfrom its managed care partners.
After initiating a process to collect the data on a regular basis, Dr.Reisner and a programmer designed an analysis tool to enable herto monitor the DM program, using the prescription database toanalyze physician prescribing, identify areas for improvement, andtarget follow-up education efforts. Using the physician prescribingprofiles from the database, together with the Clinic’s own pharma-ceutical guideline and its depression guideline, she conductedone-on-one education and training sessions with the primary carephysicians. In Phase II of the measurement program, the Clinicwill link guideline usage to clinical outcomes using its newlyimplemented electronic medical record system.
In addition to depression, the Clinic is currently implementing DMprograms for several other chronic conditions, including diabetes,asthma, and congestive heart failure. The clinical pharmacist playsa key role in each of these efforts and ensures that consistent
methods are applied in all disease areas to effectively coordinatepharmaceutical care for all Clinic patients. For example, the monitoring and measurement tools developed for the depressionprogram, particularly the prescription database, will be applieduniversally to all disease management programs.
Pain, lipid-lowering, and anticoagulation clinics
As part of the Clinic’s ongoing effort to coordinate care for high-risk, chronic conditions, disease-focused clinics are beingdeveloped to provide pain management, lipid-lowering, and anticoagulation services. The goal of these new clinics is to provide education, counseling, and condition monitoring topatients on an ongoing basis, relying heavily on proper pharma-ceutical care. Therefore, coordinating pharmaceutical care withinthese clinics is anticipated to increase compliance with drug regimens, to identify drug interactions, and to influence lifestylehabits that complement drug therapies, thereby improving overallquality of care and reducing total system costs.
Each clinic will be established by the clinical pharmacist and managed by a combination of providers and educators, includingpharmacists, nurses, and physicians. Linking activities in each ofthese clinics with each patient’s primary care physician will ensuremaximum coordination of the total care plan, including pharma-ceutical coordination.
38 Coordinated Pharmaceutical Therapy in Chronic Care
Frequent Visitor Program
In 1997, Kathy Korbholz, Senior Administrator, ordered a reportlisting a specific patient’s visits over a twelve-month period. Shewas alarmed to discover that the patient had made over 190appointments during the period. The patient had cancelled andrescheduled over 50 visits and had seen 24 different physicians in16 different departments. A chart review uncovered no chronicmedical problems, identified numerous tests, and provided no realanswers. Believing she had stumbled across the rare patient, Ms.Korbholz nevertheless ordered a report for all patients havingmore than 20 visits during each of the past two years. The result-ing report identified over 4,000 patients with more than 20 visits;the original patient was relegated to page 12. Clearly, manypatients were not having their medical needs met despite extensiveuse of Clinic services. Together with a care management team ofphysicians, administrators, nurses, and the clinical pharmacist,she set out to improve the coordination of care for these patientsby initiating the Frequent Visitor Program.
In 1997, over 4,200 patients, or 3.59% of all Clinic patients, wereidentified as frequent visitors. They consumed approximately 20%of the Clinic’s services. An analysis derived from the newly devel-oped prescription database identified a number of critical areasfor attention, including patients with chronic diseases such asasthma, depression, and diabetes. The analysis also identifiedthose patients who could benefit from further pharmaceuticalcoordination efforts, including patient education, counseling, andcompliance support.
The Clinic instituted a number of programs in 1998 to better man-age frequent visitors, including:
• Flagging patient charts to identify those requiring additionalattention, continuity of provider, and a high level of providercoordination,
• Creating a frequent visitor check list to be completed at each visit,
• Building social support groups through “group visits” forpatients with similar ailments, and
• Posting answers to frequently asked questions on the Clinic’sweb site to provide medical information without the need foran office visit.
The clinical pharmacist enabled the care process improvementteams to increase their performance by:
• Having better access to pharmaceutical prescribing data,
• Bringing an in-depth knowledge of pharmaceutical therapiesand their pitfalls to the team,
• Analyzing possible pharmaceutical-related causes for frequent visits, and
• Assisting the team to develop and deliver effective educationon pharmaceutical issues.
Benefits of Accountability for Pharmaceutical Coordination
Focusing on pharmaceutical coordination and creating a clinicalpharmacist role charged with overseeing pharmaceutical coordi-nation has brought many benefits to the Clinic, including:
• Developing a comprehensive prescription drug database that can be used to enable a variety of clinical improvementprograms,
• Facilitating and supporting the design, implementation, andmonitoring of disease management programs in diabetes,asthma, and depression,
• Providing valuable pharmaceutical knowledge to all clinicalprocess improvement teams,
• Developing expanded roles for pharmacists by planning andfounding pain, lipid-lowering, and anticoagulation clinics,and most importantly,
• Achieving more effective pharmaceutical utilization throughout the system.
The clinical pharmacist function and related pharmaceutical coordination efforts are still in their infancy at the Clinic. Theseefforts form the platform for the many clinical improvement programs that are now operational. These programs are successful in terms of process. Significant improvements in clinical outcomes and patient satisfaction are expected and will be assessed.
Coordinated Pharmaceutical Therapy in Chronic Care 39
Lessons Learned and Keys to Success
During the course of the past three years, as the Clinic implement-ed its pharmaceutical coordination program, three essentiallessons were learned:
Focus on pharmaceutical coordination to achieve competitive advantage
A provider organization should focus on pharmaceutical coordina-tion, even if it is currently not at risk for the drug budget. In doingso, the organization will increase its knowledge of pharmaceuticalutilization issues, create more coordinated health care servicemodels, and increase the overall effectiveness of care. Such organizations will be better prepared to understand and acceptfinancial risk for pharmaceutical care from HMO contracting partners who are increasingly preferring global risk contracts.
Link pharmaceutical utilization with outcomes to enableprocess improvement
Information is the key enabler in implementing almost any clinicalprocess improvement program. Analyzing and implementing phar-maceutical treatment often requires a comprehensive prescriptiondatabase linked to outcomes and other patient information.Although most clinics do not have timely access to such informa-tion, as electronic medical records become more common in theclinic setting, pharmacists and process improvement teams will bebetter able to assess and implement improvement initiatives, edu-cation efforts, guidelines development, and performance monitors.
The Clinic invested substantial time and resources to develop theprescription database they needed to move these processes forward. The Clinic will continue to improve utilization of informa-tion by linking pharmaceutical use and protocol compliance tooutcomes and other service use. By the continued use of an elec-tronic medical record, the Clinic will acquire additional knowl-edge to further improve the coordination of pharmaceutical care.
Centralize responsibility for pharmaceutical coordination to facilitate process improvement
Clearly identifying a person or department accountable for coordi-nating pharmaceutical care can facilitate many clinical processimprovement programs. Once the Clinic created the clinical phar-macist role and held the pharmacist accountable for pharmaceuti-cal coordination efforts, other members of the organization soughtout her support and knowledge to help them with pharmaceuticalaspects of their process improvement initiatives. This accountabili-
ty not only aided in the coordination of pharmaceutical care, butalso enabled overall service coordination at the Clinic. The key isnot necessarily who is responsible for pharmaceutical coordina-tion, but rather that responsibility is centralized and therefore recognized throughout the health care system.
In summary, clear accountability, accurate and comprehensiveprescription data, and recognition of the importance of outpatient pharmaceutical care can be achieved by creating a rolespecifically responsible for coordinating pharmaceutical care. At the Palo Alto Medical Foundation, this position was filled by aclinical pharmacist and resulted in effective implementation of a variety of innovative programs throughout the organization.
The Palo Alto Medical Foundation
The Palo Alto Medical Foundation for Health Care, Research &Education is a not-for-profit, tax-exempt public charity nationally rec-ognized for leadership in health care delivery. The Foundation pio-neered the multi-specialty group practice of medicine and outpatient services as ways to improve the quality and cost-effective-ness of health care. The Foundation was one of the first organizations in the country to embrace the concept of a coord i n a t e dhealth care delivery system in a managed care setting as a superiorapproach to improving health services.
In 1987, using community philanthropy, long-term financing, and amulti-million dollar gift from its physicians, the Foundation acquiredthe assets of the Palo Alto Clinic Partnership (founded in 1930).Together with the former Palo Alto Medical Research Foundation(founded in 1950) and a new education division, they created atruly coordinated health care delivery system.
The Foundation operates three primary clinics in the Silicon Va l l e ywith over 186 physicians and 848 nurses and support staff. In addi-tion to the 69 researchers and staff at the Research Institute and the 17educators in the education division, the Foundation employs over1,100 health care professionals.
In 1993, the Foundation became an affiliate of the Sutter HealthSystem based in Sacramento, California. This allied the Foundationwith a very strong health system. Like the Palo Alto MedicalFoundation, Sutter is a not-for-profit organization comprised of morethan 30 health-related entities, including hospitals, other medicalfoundations, an insurance company, and support organizations.Through Sutter, the Foundation recently joined with the California Health Care System to form a statewide health carenetwork, Sutter Health.
Case 5
E d u c a t i o n I m p r o v e s M e d i c a t i o nM a n a g e m e n t , R e g i m e nK n o w l e d g e , a n d O u t c o m e s i nH I V / A I D S P a t i e n t s
S a n F r a n c i s c o D e p a r t m e n t o f P u b l i c H e a l t hS a n F r a n c i s c o , C Aw w w. d p h . s f . c a . u s

Coordinated Pharmaceutical Therapy in Chronic Care 41
Overview of the HIV/AIDS Treatment Education Certification Program (TECP)........... 42
Complex Treatment Regimens for HIV/AIDS Patients............... 42
The Path to TECP Implementation........................................... 42
Elements of the Program......................................................... 43
Results and Benefits................................................................ 44Knowledge Base of Counselors Improved ............................ 44Improved Drug Therapy, Treatment Outcomes,
Quality of Life................................................................. 44
Expanding and Improving the Program................................... 45
Lessons Learned and Keys to Success...................................... 45
Additional Information on the Origins of TECP....................... 45
C O N T E N T S

42 Coordinated Pharmaceutical Therapy in Chronic Care
Overview
The Treatment Education Certification Program (TECP), sponsored by the San Francisco Department of Public Health,enhances basic knowledge regarding HIV/AIDS care and treatment. TECP is offered to non-medical service providers,including treatment advocates, case managers, peer advocates,mental health and substance abuse counselors, and others whowork directly with low-income HIV-positive clients. If necessary,the trainees interact directly with the medical professionals who provide care for these clients.
This training program enables these non-medical providers to better assist their clients in meeting the challenges posed by theircomplex therapeutic regimens. The program also helps theseproviders in identifying inappropriate or conflicting drug therapies.
The core of the program is a three-day course on HIV/AIDS, itsmany comorbidities, and the complex treatment regimens faced bythese patients. Once certified, trainees provide patients with thesupport and education necessary to ensure compliance with theirtreatment regimens and to maximize the value of their pharma-cotherapy. The trainees are not intended to replace the physician.Rather, they provide a baseline of information, together with emotional and practical support, for a complex patient populationwith multiple social and physical challenges. Case reports indicatethat the program has been successful in improving pharmaceuticaltherapy in HIV/AIDS patients. This innovative program demon-strates how public health officials and not-for-profit programs canbe essential forces in the coordination of pharmaceutical care.
Several principles of coordinated pharmaceutical care are exemplified in this program that serves clients who have multiplecoexisting diseases and who often receive prescriptions from several physicians. Effective communication and feedback amongcaregivers was an essential element of the program, and patientswere educated and involved in the treatment plan. Strong leader-ship by individuals within participating organizations promotedsuccess and rapid acceptance of the program. In addition, thepeer-to-peer training fostered a sense of teamwork that built astrong support network for the future.
Complex Treatment Regimens for HIV/AIDS Patients
Dramatic progress in our ability to suppress HIV replicationthrough powerful new medications has resulted in widespreadoptimism that HIV can become a long-term manageable disease.However, with a multitude of antiretroviral drugs now availableand in development, HIV treatment regimens have becomeincreasingly complex.
In addition to receiving treatments designed to suppress HIV replication, most patients are also treated for common clinicalmanifestations of HIV disease, such as AIDS wasting, HIV-associat-ed psychiatric disorders, pneumococcal infections, pneumocystiscarinii pneumonia, cytomegalovirus, and other bacterial infec-tions. Many patients also require therapy for other comorbidities,such as cardiac conditions, diabetes, and asthma. The combina-tion of these regimens confronts the AIDS patient with one of themost complex treatment regimens in medicine.
TECP was created in response to this challenge. Program partici-pants help guide patients through prescribed drug regimens. TECPalso provides participants with the knowledge necessary to helppatients effectively use available pharmaceutical treatments, andaddresses the need to integrate education, treatment advocacy, andsupport in the HIV/AIDS community. TECP ensures that patientshave qualified professionals to answer their questions regardingtreatment options, results, side effects, and appropriate usage.
The Path to TECP Implementation
TECP was made possible by federal funding provided to state andlocal public health agencies under the Ryan White ComprehensiveAIDS Resources Emergency (CARE) Act. The funds provided toSan Francisco’s Department of Public Health were used to createand support public health and wellness programs throughout thecity. The programs are administered through a complex array ofagencies. TECP is managed by two of these agencies, the Asian andPacific Islander Wellness Center (API) and Project Inform.
TECP was designed with three primary goals: 1) to initiate market-ing, public relations, and advocacy effort within CARE programmanagers and the general public; 2) to develop program management tools; and, 3) to develop training curriculum andresource materials.
API hired the program coordinator and master trainer and begandeveloping the marketing, outreach, and administrative materials.Project Inform took primary responsibility for developing the cur-riculum and training materials.
A three-fold approach was used to market the program to the

Coordinated Pharmaceutical Therapy in Chronic Care 43
local Ryan White CARE-funded programs. First, a programbrochure was posted at all Ryan White CARE-funded sites in SanFrancisco in order to attract interest from individual non-medicalproviders. Second, TECP Coordinator Mathew Sharp visited program managers of Ryan White CARE agencies to personallyintroduce them to TECP. This one-on-one outreach resulted in significant interest. Third, the program was marketed through themedia. For example, on December 1, 1998 the San FranciscoChronicle ran a story on TECP, which extended interest in the program beyond the local agencies. These efforts resulted in astrong demand for the training courses; training sessions wereoften over-enrolled. In addition, agencies outside the SanFrancisco Department of Public Health’s purview became aware of TECP and enrolled their providers through a tuition-based pro-gram that was added to respond to the strong market demand.
API also took the lead in developing tools necessary to effectivelymanage the overall program, including tools for intake, screening,scheduling and follow-up with training course participants. APIdesigned participant tracking systems, eligibility certification pro-cedures, and all data entry forms used to monitor the progress ofthe program and individual program participants.
Project Inform led all curriculum design efforts and,together with API, managed the overall design of thethree-day curriculum, including pre- and post-trainingcertification examinations, instructional materials, and anHIV Treatment Education Briefing Book for distribution toall participants.
During the program design phase, Project Inform and API conducted a focus group with a number of non-medical providersto establish a baseline for program planning, evaluation, and standards for certification, and to collect input for curriculumdesign. In addition, a panel of advisors and experts was asked tohelp guide overall program development, particularly the curriculum.
Elements of the Program
The training curriculum and accompanying HIV TreatmentEducation Briefing Book include sections on: HIV treatment training philosophy; HIV pathogenesis; standards of care; anti-HIV treatments and therapies; opportunistic infections;research, clinical trials and access issues; compliance issues andstrategies; strategies for working with multiply diagnosed clientsand underserved populations; and sources for updated treatmentinformation.
The three-day training course forms the centerpiece for TECP.Each three-hour course was attended by eighteen participants andwas led by Project Inform. The training course is augmented by an annual treatment education update, provider work group sessions and one-on-one consultations for participants who needadditional individualized training.
Five provider work group sessions, lasting three hours each, wereheld during the year. Each session focused on a topic of interestthat could not be covered in sufficient detail during the three-daytraining. Each session also featured a guest lecturer from the San Francisco HIV/AIDS research and treatment community.These work group sessions, together with the treatment educationupdates and the core training sessions, form a powerful year-round training program.
Individual tutoring was provided for participants having difficultywith the pace or volume of content covered in the training. Theseconsultations focused on areas such as treatment options, HIVpathogenesis, and other complex topics. These tutoring sessionsproved particularly valuable for participants who were having difficulty passing the certification exam.
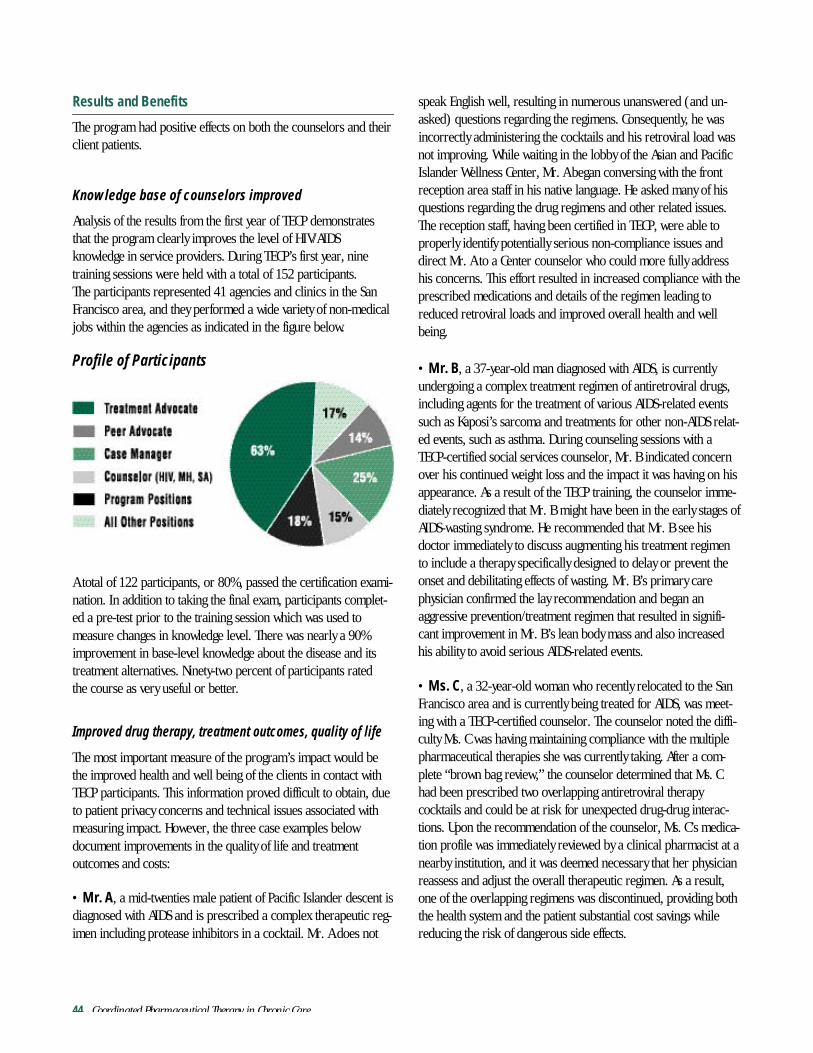
44 Coordinated Pharmaceutical Therapy in Chronic Care
Results and Benefits
The program had positive effects on both the counselors and theirclient patients.
Knowledge base of counselors improved
Analysis of the results from the first year of TECP demonstratesthat the program clearly improves the level of HIV/AIDS knowledge in service providers. During TECP’s first year, ninetraining sessions were held with a total of 152 participants. The participants represented 41 agencies and clinics in the SanFrancisco area, and they performed a wide variety of non-medicaljobs within the agencies as indicated in the figure below.
A total of 122 participants, or 80%, passed the certification exami-nation. In addition to taking the final exam, participants complet-ed a pre-test prior to the training session which was used to measure changes in knowledge level. There was nearly a 90%improvement in base-level knowledge about the disease and itstreatment alternatives. Ninety-two percent of participants rated the course as very useful or better.
Improved drug therapy, treatment outcomes, quality of life
The most important measure of the program’s impact would bethe improved health and well being of the clients in contact withTECP participants. This information proved difficult to obtain, dueto patient privacy concerns and technical issues associated withmeasuring impact. However, the three case examples below document improvements in the quality of life and treatment outcomes and costs:
• Mr. A, a mid-twenties male patient of Pacific Islander descent isdiagnosed with AIDS and is prescribed a complex therapeutic reg-imen including protease inhibitors in a cocktail. Mr. A does not
speak English well, resulting in numerous unanswered (and un-asked) questions regarding the regimens. Consequently, he wasincorrectly administering the cocktails and his retroviral load wasnot improving. While waiting in the lobby of the Asian and PacificIslander Wellness Center, Mr. A began conversing with the frontreception area staff in his native language. He asked many of hisquestions regarding the drug regimens and other related issues.The reception staff, having been certified in TECP, were able toproperly identify potentially serious non-compliance issues anddirect Mr. A to a Center counselor who could more fully addresshis concerns. This effort resulted in increased compliance with theprescribed medications and details of the regimen leading toreduced retroviral loads and improved overall health and wellbeing.
• Mr. B, a 37-year-old man diagnosed with AIDS, is currentlyundergoing a complex treatment regimen of antiretroviral drugs,including agents for the treatment of various AIDS-related eventssuch as Kaposi’s sarcoma and treatments for other non-AIDS relat-ed events, such as asthma. During counseling sessions with aTECP-certified social services counselor, Mr. B indicated concernover his continued weight loss and the impact it was having on hisappearance. As a result of the TECP training, the counselor imme-diately recognized that Mr. B might have been in the early stages ofAIDS-wasting syndrome. He recommended that Mr. B see his doctor immediately to discuss augmenting his treatment regimento include a therapy specifically designed to delay or prevent theonset and debilitating effects of wasting. Mr. B’s primary carephysician confirmed the lay recommendation and began anaggressive prevention/treatment regimen that resulted in signifi-cant improvement in Mr. B’s lean body mass and also increasedhis ability to avoid serious AIDS-related events.
• Ms. C, a 32-year-old woman who recently relocated to the SanFrancisco area and is currently being treated for AIDS, was meet-ing with a TECP-certified counselor. The counselor noted the diffi-culty Ms. C was having maintaining compliance with the multiplepharmaceutical therapies she was currently taking. After a com-plete “brown bag review,” the counselor determined that Ms. Chad been prescribed two overlapping antiretroviral therapy cocktails and could be at risk for unexpected drug-drug interac-tions. Upon the recommendation of the counselor, Ms. C’s medica-tion profile was immediately reviewed by a clinical pharmacist at anearby institution, and it was deemed necessary that her physicianreassess and adjust the overall therapeutic regimen. As a result,one of the overlapping regimens was discontinued, providing boththe health system and the patient substantial cost savings whilereducing the risk of dangerous side effects.
Profile of Participants

Coordinated Pharmaceutical Therapy in Chronic Care 45
Expanding and Improving the Program
TECP will build upon its core strengths and expand to includeadditional trainees. TECP’s success has spread to agencies andorganizations throughout the greater Bay Area and beyond; therefore, TECP has created a tuition-based enrollment option forproviders from outside San Francisco.
TECP is also working with the federal government’s HealthResearch and Services Administration (HRSA) to fund a nationalrollout of TECP to cities and agencies throughout the country.According to Mathew Sharp, TECP Project Coordinator,“The foundation is in place to build a powerful nationwide training program to teach non-medical providers to assistHIV/AIDS patients with their treatment regimens.”
Lessons Learned and Keys to Success
Development and implementation of TECP has yielded insight into many keys to success in building and integrating a training program for counselors of patients with a complex chronic medical condition.
First, chronic care patients with complex diseases, such asHIV/AIDS, need knowledgeable service providers at every point ofcontact within their sphere of influence. Often this advice is soughtin less formal venues than the physician’s office, including friends,fellow patients, case managers, treatment advocates and othersworking in the system. Providing potential contacts with the in-depth knowledge and resources to answer these questions andserve as a safety-net resource for HIV/AIDS patients improvespatient compliance with treatment regimens and quality of life.TECP trainees can now answer routine questions with confidenceand recognize issues that are best handled directly by the patient’sphysician. TECP has given non-medical providers important base-line information to help patients cope with the complex treatmentregimens resulting from their disease.
Second, successfully launching a training program like TECPrequires a focus on specific diseases and the challenges faced bychronic care patients. TECP benefited greatly from San Francisco’sstrong HIV/AIDS community and a well-established network ofRyan White CARE-funded organizations. Starting a similar programin other communities where the agency network is not as strongwould present additional marketing and organizational challenges.Similarly, other chronic conditions with less developed supportnetworks and patient communities would require additional marketing and grass roots activism.
Third, strong leadership from within the organizations receivingthe training can promote success among participating organiza-
tions. The leadership provided by API and Project Inform wasfrom within the Ryan White CARE-funded agency community andresulted in rapid acceptance of TECP. In addition, the peer-to-peertraining concept fostered a sense of teamwork that builds a strongsupport network for the future. Combining this informal sense ofcommunity with the formalized, ongoing training of the providerwork groups and treatment education updates builds a supportnetwork of HIV/AIDS non-medical providers who can embraceand lead continuous improvement throughout the non-profitagency system.
Additional Information on the Origins of TECP
In San Francisco, the Ryan White CARE Act funds programs thatare administered by the AIDS Office of the San FranciscoDepartment of Public Health (SFDPH). The SFDPH has tasked theSan Francisco Ryan White HIV Health Services Planning Council toassess community needs and prioritize services to be supportedwith federal HIV/AIDS dollars. The 1998 efforts of the PlanningCouncil recognized the need to assist its more than 15,000HIV/AIDS clients in gaining access to, interpreting, and evaluatingtheir treatment options so they can make informed choices. In addition, the Planning Council wanted to hold its nearly 300non-medical AIDS workers accountable for establishing and maintaining a high standard of competence in a rapidly evolvingfield. The Planning Council recommended funding a program like TECP, and called for proposals from the area’s Ryan Whitefunded agencies.
The Asian and Pacific Islander Wellness Center, the largest non-profit HIV/AIDS agency dedicated to Asians and PacificIslanders in the United States, together with Project Inform, thenation’s leading HIV/AIDS treatment information and advocacysource, developed a grant proposal for submission to theDepartment of Public Health. The collaboration of these two leading HIV/AIDS organizations fit the Planning Council vision perfectly, and the Treatment Education Certification Program wasfunded and launched in September of 1998. The collaborationbrought together Project Inform’s unique skills of treatment advocacy and training program design with the day-to-day opera-tional understanding of a large non-profit HIV/AIDS wellness center. The combined expertise of these two organizations waswell suited to implementing this complex program across all 68Ryan White agencies in the San Francisco Metropolitan Area.
46 Coordinated Pharmaceutical Therapy in Chronic Care
What the Case Studies Have Taught Us
The five programs profiled in this report provide insights on successful strategies and approaches for achieving coordinatedpharmaceutical treatment.
Leadership and Management
A commitment by top management characterized many of thesesuccessful programs. Management often acted on this commitmentby assigning accountability for the coordination function to anindividual or a team.
A “champion” with a vision of coordinated care, often the medicaldirector or staff pharmacist, is needed to spearhead the initiativeand, most importantly, to engage the interest and cooperation ofclinicians.
A pharmacist was often the key driver for the development andimplementation of the coordinated care process. The pharmacistoften worked in partnership with the “champion” (if he or shewas not the champion). Nurses often proved to be effective coor-dinators of the day-to-day operation of the program. These newroles for health care professionals provided added value for theorganization.
Partnerships
Successful partnerships between provider organizations and phar-macy schools have resulted in win-win situations for both parties.Pharmacy students or interns who assumed integral roles in pro-gram implementation received valuable experience; the providerorganization received low-cost professional assistance in operatingthe program.
Information Systems
Acquisitions of nursing homes, hospitals, and other sites of caredelivery by health systems have generally resulted in fragmentedinformation systems in which prescribing data are not linked totreatment outcomes data. Although integration of medical chartsacross sites and a fully computerized medical record are rare, thishas not prevented many of the case study sites from linkingenough information to implement an effective level of coordinatedpharmaceutical care.
Coordination Across Sites of Care
Specialty clinics within hospitals – e.g., for burn care or anticoag-ulation – can be a central focus for coordination of pharmaceuti-
cal care across care sites of the parent health system. These hospi-tal-based clinics have extended coordinated services into theambulatory care setting and home care.
Education
The pace of progress in pharmaceutical technology has height-ened the need for both provider and patient education. Educatingand providing feedback to physicians and patients is essential foroptimal use of advanced pharmaceutical technologies, such asthose for patients with HIV/AIDS.
Evaluation
Improvements in treatment outcomes and costs were noted inthose coordinated pharmaceutical programs that engaged in somemeasurement of program effects. However, since such programsoften evolve as resources permit, rigorous and comprehensivecost/benefit evaluations are rarely performed. In addition, recentcutbacks in operating budgets make such evaluations less likely.However, pharmacy professors or graduate students in search ofinteresting, relevant research projects could perform such analy-ses. Demonstration of a net economic gain to the organization willhelp maintain support for the program and justify funding forexpansion.
Some of the evaluations that were done indicated that drug expen-ditures may rise as a result of coordinated pharmaceutical care,especially in those programs focused on reducing undertreatmentor improving medication compliance. However, in some of theseprograms, increased drug costs were accompanied by lower over-all costs as well as improved quality of care. This is illustrated inthe coordinated programs for depression, pain, lipid, and coagu-lation disorders.
Competitive Advantage
Coordinated pharmaceutical care programs can be useful even tothose provider organizations not currently at risk for drug expen-ditures. In addition to increasing the overall effectiveness of care,improved pharmaceutical coordination will also help such organi-zations enhance their knowledge of pharmaceutical utilization patterns. Substantial competitive advantage may result from thisknowledge. In addition, improved knowledge of drug usage patterns will help provider organizations entering global capitationarrangements to better estimate drug budget risk.