Controversies: Lead in or no lead in ? PRO Controversies: Lead in or no lead in ? PRO Lawrence...
22
Controversies: Lead in or no lead in ? PRO Lawrence Serfaty Hôpital Saint-Antoine Paris 5th Paris Hepatitis Conference, January 30-31 2012
-
Upload
kerrie-martin -
Category
Documents
-
view
227 -
download
0
Transcript of Controversies: Lead in or no lead in ? PRO Controversies: Lead in or no lead in ? PRO Lawrence...

Controversies: Lead in or no lead in ?
PRO
Lawrence Serfaty
Hôpital Saint-Antoine
Paris
5th Paris Hepatitis Conference, January 30-31 2012

Lead-in phase
W0 W4
PI + Peg-IFN + RBV
Weeks of treatment
Peg-IFN + RBV
Triple therapyDual therapy

Lead-in phase
• Improvement of triple therapy effectiveness ?
• Prediction of triple therapy effectiveness ?

Lead-in phase
• Improvement of triple therapy effectiveness ?
• Prediction of triple therapy effectiveness ?

Impact of lead in phase on boceprevir effectiveness
(SPRINT-1: naïve patients)
% of patients with negative PCR
Kwo PY et al. Lancet 2010

But higher rate of RVR at W4 of triple therapy
Kwo PY et al. Lancet 2010
% RVR
P < 0,001
Higher percentage of patients eligible for shorter treatment duration

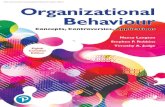
Impact of lead in phase on telaprevir effectiveness (REALIZE: tt-experienced patients)
Previous relapser Previous partial responder
Previous null responder
0
20
40
60
80
10088
54
33
83
59
29
Lead-inNo Lead-in
% SVR
Zeuzem S et al. J Hepatol 2011; 54: S3

Lead-in phase
• Improvement of triple therapy effectiveness ?
• Prediction of triple therapy effectiveness ?

New molecules: new challenges
• Improvement of SVR but :
- Resistant variants occurrence
- New or higher rate of side effects
- Cost of PIs (±EPO).
Need for predictors of response

BOC RGT%
SV
R
<0.5
Log10 viral load decrease after 4 wks of P/R lead-in
0.5 – <1.0
1.0 – <1.5
1.5 – <2.0
2.0 – <3.0
3.0 – <4.0≥4.0
Undetectable
Poordad F et al. NEJM 2011; 364: 1195-1206
Viral load decline after 4 wks of lead-in is predictive of boceprevir effectiveness
(SPRINT-2: naïve patients)

High rate of SVR in patients with negative HCV RNA at W4 of lead-in (SPRINT-2)
Vierling JM. et al. EASL 2011. J Hepatol 2011: 54: S197 (abstract 481)
SV
R (
%)
0
20
40
60
80
100 97
48 P/R
29/30
89
BOC TGR
17/19
90
BOC/PR48
18/20
Patients with RVR

IL28B genotyping for selection of RVR patients
Thompson AJ, Gastroenterology 2010

Place of PEG + RBV in G1 patients naïve of treatment ?
PEG + RBV
IL28B CC et F≤2
12 weeks triple therapy ?
AFEF guidelines
W4 Undetectable HCV RNA (30%) Detectable HCV RNA
Triple therapyPEG + RBV during 22/44 weeks according to viral
load at baseline

<1 log >1 log <1 log >1 log <1 log >1 log0
20
40
60
80
100
62
88
56 59
15
54
Relapsers Partial responders
Nul responders
%SVR
Treatment-experienced patients: SVR according to HCV viral load decline at W4 of lead-in (REALIZE)
Poordad F et al. J Hepatol 2011; 54: S6

Resistant variant occurrence and sensitivity to interferon
> 1 log < 1 log0
100
200
300
400
500
600
700
800
536
93
87
52
39
115
Patients with resistancePatients without resis-tanceND
n patients
41%
6%
* SPRINT-2 + RESPOND-2 pooled data

Proposal in prior nul responders
PEG + RBV
W4 VL decline< 1 log
Stop treatment (excepted rescue)
Triple therapy
VL decline> 1 log
AFEF guidelines

Relapsers Partial responders0
102030405060708090
18
60
82
40 < 1log> 1log
% of patients
Bacon F et al. NEJM 2011; 364: 1207-1217
Reclassement of treatment-experienced patients (RESPOND-2)
Viral load decline at W4 of lead in

Testing tolerance with PEG+Riba prior initiating triple therapy
• Dosage adjustment of PEG+Riba according to tolerance (hematological toxicity)
• Initiating growth factors prior to triple therapy

Conclusion
Lead in phase
Selection of patientseligible for PEG+RBV(naive RVR patients)
Shorter treatment duration
with boceprevir
Reclassement of tt-experienced patients
Highly predictive in nul responders(VL decline<1log)
Tolerance to PEG+RBV(dosage adjustment)


sensitive
resistant
DAA
resistant
sensitive
PEG+Riba
Mechanism of resistanceInterferon sensitivity and resistant variants occurence

sensitive
resistant
DAA
resistant
sensitive
PEG+Riba
Mechanism of resistanceInterferon sensitivity and resistant variants occurence