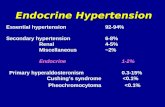
Controversies in Endocrine Hypertension: The Case of Primary ...
33
CONTROVERSIES IN MINERALOCORTICOID HYPERTENSION: THE CASE OF PRIMARY ALDOSTERONISM José A. Rodriguez-Portales, MD, FACP Division of Internal Medicine Department of Endocrinology Catholic University of Chile School of Medicine
-
Upload
roger961 -
Category
Health & Medicine
-
view
1.372 -
download
1
Transcript of Controversies in Endocrine Hypertension: The Case of Primary ...

CONTROVERSIES IN MINERALOCORTICOID
HYPERTENSION:THE CASE OF PRIMARY ALDOSTERONISM
José A. Rodriguez-Portales, MD, FACP
Division of Internal MedicineDepartment of Endocrinology
Catholic University of Chile School of Medicine

JW Conn
Primary aldosteronism,
a new clinical syndrome.
J Lab Clin Med 1955
• Aldosterone-producing adenoma• Hypertension
• Hipokalemia• Metabolic Alkalosis
CONN’S SYNDROME20% of pts. with hypertension
have it
OK,10%

Are we missing the diagnosis
in 10% of our hypertensive patients?

Diagnosis of Primary AldosteronismDiagnosis of Primary Aldosteronism
Case-finding strategies
Confirmatory tests
Subtype evaluation tests

CLASSICAL TRIAD OF PRIMARY CLASSICAL TRIAD OF PRIMARY HYPERALDOSTERONISMHYPERALDOSTERONISM
HypertensionHypokalemiaSuppressed PRA
< 1% ofhypertensive pts.
have it

PRIMARY HYPERALDOSTERONISM:increased diagnosis in normokalemic patients
0
10
20
30
40
50
60
70
1985 86 87 88 89 90 91 92 93
K+ normalK+ low
# pa
tien
ts /
year
YearGordon RD, Lancet 1994; 344: 240-243.

FREQUENCY OF HYPOKALEMIA IN PATIENTS WITH PRIMARY ALDOSTERONISM
Mulatero P, Stowasser M, Loh K, Fardella CE et al. J Clin Endocrinol Metab. 2004.Mulatero P, Stowasser M, Loh K, Fardella CE et al. J Clin Endocrinol Metab. 2004.
Hypokalemia in only 25%

CASES OF 1ary ALDOSTERONISM DIAGNOSED BEFORE AND AFTER USING THE PA/PRA RATIO
Mulatero P, Stowasser M, Loh K, Fardella CE et al. J Clin Endocrinol Metab 2004Mulatero P, Stowasser M, Loh K, Fardella CE et al. J Clin Endocrinol Metab 2004..
15-FOLD INCREASE

CONFIRMATORY TESTSCONFIRMATORY TESTS
Oral sodium loading testNa intake > 13 g/day UNa V > 200 mEq/dayThird day: 24-h urine collection for Na, aldo, creatUAldo > 12 μg/24 h Autonomous secretionSensitivity 96% Specificity 93%

CONFIRMATORY TESTSCONFIRMATORY TESTS
Saline infusion:Isotonic saline infusion, 500 ml/h for 4 hours. Positive result: serum aldosterone > 5 ng/dl.
Aldosterone suppression with fludrocortisone: Fludrocortisone 0.1 mg/6h for 4 days. Diet supplemented with NaCl 6 g/day Serum potassium must be monitored daily Positive result: serum aldosterone > 5 ng/dl

0
20
40
60
80
0 50 100 150 200 250
Time (min)
ZGH
APA
Normal
ALDOSTERONE RESPONSE TO SALINE LOAD
Holland OB, Hypertension 1984

SERUM ALDOSTERONE/PRA RATIO IN NORMOTENSIVE SUBJECTS
Fardella C.E., Mosso L., Montero J. et al Rev. Med. Chile 2000Fardella C.E., Mosso L., Montero J. et al Rev. Med. Chile 2000

305 HYPERTENSIVE PATIENTS305 HYPERTENSIVE PATIENTS
PA/PRA
44 PA/PRA ≥ 25 261 PA/PRA < 25
13 classic 1ary aldo
PA > 16ng/dl
PRA < 0,5 ng/ml/h
PA/PRA > 50
31 probable 1ary aldo
29 1ary aldo (9.5%) Essential hypertension
13 (+) 16 (+)
Fludrocortisone
Fardella C.E., Mosso L., Montero J. et al J Clin Endocrinol Metab. 2000Fardella C.E., Mosso L., Montero J. et al J Clin Endocrinol Metab. 2000

546 (10.7)4994Total
61(6.0)Captopril>201020Japan2004Omura M
54 (18.0)Fludrocortisone>30300Australia2003Stowasser M
66 (6.3)Captopril>351046Italy2003 Rossi E
37 (6.1)Fludrocortisone>25609Chile2003Mosso LM
18 (20.0)PRA and Aldo ur c>2088bUSA2002Calhoun DA
106 (21.0)NA>20505USA2002Schwartz GL
15 (17.0)CT-NMR-I131 scan>10090USA2001Gallay BJ
22 (10.1)NA>36216South Africa2000Rayner BL
16 (4.6)Saline infusion>20350Singapore2000Loh KC
43 (9.2)Fludrocortisone>27465UK2000Lim PO
Prevalencen (%)
Confirmatorytest
Author (Ref) Year Country Patients (n) ARR (ng/dL / ng/mL·h)
29 (9.5)Fludrocortisone>25305Chile2000Fardella, CE
PREVALENCE OF HYPERALDOSTERONISM IN DIFFERENT POPULATIONS

William F YOUNG JrMayo, Rochester MN
Celso GOMEZ-SANCHEZJackson, MS
Carlos FARDELLALorena MOSSOSantiago, Chile
Paolo MULATEROFranco VEGLIO
Torino, Italy
Keh-Chuan LOHSingapore
Michael STOWASSERRichard D GORDONBrisbane, Australia

SUBTYPES OF 1ary HYPERALDOSTERONISM
Aldosterone-producing adenoma (APA) 35%
Bilateral Adrenal Hyperplasia (BAH) 65%
Unilateral Adrenal Hyperplasia (PAH) < 1%
Aldosterone-producing carcinoma (APC) < 1%
Aldosterone-producing carcinoma < 1%
FAMILIAL FORMS
Glucocorticoid-Remediable Aldosteronism (GRA) < 2%
Familial HA Type II (FH-II) < 2%

FREQUENCY OF ALDOSTERONE-PRODUCING ADENOMA
Mulatero P, Stowasser M, Loh K, Fardella CE et al. J Clin Endocrinol Metab 2004.Mulatero P, Stowasser M, Loh K, Fardella CE et al. J Clin Endocrinol Metab 2004.
APA only in 30% of 1ary aldo cases

DIAGNOSING SUBTYPES OF DIAGNOSING SUBTYPES OF HYPERALDOSTERONISMHYPERALDOSTERONISM
Adrenal CT Scan or MRI.
Adrenal veins catheterization with simultaneous sampling for aldosterone and cortisol.
Other tests: postural test, post spironolactone urinary aldosterone measurement, dexamethasone suppression test, 18 OH B, 18 OH cortisol derivatives, genetic testing.

ADENOMA CORTICO SUPRARRENAL ADRENAL CT SCAN IN HYPERALDOSTERONISM
Helpful in diagnosing APA if > 5 mm.
Helpful in diagnosing BAH if area > 10 mm.
Suggests adrenal cancer if > 6 cm.
Micro-macronodular hyperplasias may suggest a false diagnosis of APA
Main disadvantage: incidentalomas

Right Adrenal Vein
Inferior Vena Cava
Left Adrenal Vein
ADRENAL VEIN SAMPLING
Best method to detect lateralization
Adrenal vein/inferior vena cava cortisol ratio must be >2
Lateralization exists if Aldo/cortisol ratio is 4-fold higher than in contralateral adrenal vein
Adrenal vein catheterization may help avoid unnecesary surgery and identify microadenomas not detected by CT scanning.

Concordance: APA 8/15, BAH 4/21

Young WF. Clinical Endocrinology 2007; 66:607-618

Why is Primary Aldosteronism Why is Primary Aldosteronism important ?important ?
Primary aldosteronism may be one of the most frequent causes of secondary hypertension.
Hypertension can be cured or successfully treated with mineralocorticoid antagonists.
Aldosterone can cause vascular and cardiac damage independent from hypertension.

End-Organ Damage of AldosteroneEnd-Organ Damage of Aldosterone
PA patients compared with hypertensive patients:PA patients compared with hypertensive patients:Higher prevalence of metabolic syndromeHigher urinary albumin excretionIncreased arterial wall stiffnessGreater left ventricular massHigher rate of cardiovascular events

1,99
8,02
13,2
20
0
5
10
15
20
25
Stage1
Stage2
Stage3
Resistant
Calhoun D, Hypertension 2002Mosso L, Fardella C . Hypertension 2003
PREVALENCE OF 1ary ALDO BY SEVERITY OF HT (JNC VI)

Milliez P et al. J Am Coll Cardiol 2005
0
5
10
15
20
25
30
35
40
1ary ALDO EH 1ary ALDO EH
LVH-US LVH-ECG
p=0.01 p=0.001
PREVALENCE OF LEFT VENTRICULAR HYPERTROPHY IN PATIENTS WITH 1ary ALDO vs. EH

1ary ALDO EH
0
10
20
30
40
50
60 ACLVF
Rossi GP Hypertension 2002
DIASTOLIC DYSFUNCTION IN PATIENTS WITH 1ary ALDO vs. EH

0
10
20
30
40
50
60
70
80
PREVALENCE OF MICROALBUMINURIA IN PATIENTS WITH 1ary ALDO
Halimi JM, J Hypertens 1995
1ary ALDO LR-EH NR-EH

HYPERTENSION AFTER SURGERY IN PATIENTS WITH PRIMARY HYPERALDOSTERONISM
Rochester
66% 33%
1%
65%
35%
TorinoBrisbane
55%45%
Singapore
55% 40%
5%
Cured
Improved
No change
Santiago
30%70%
Mulatero P, Stowasser M, Loh K, Fardella CE et al. J Clin Endocrinol Metab 2004Mulatero P, Stowasser M, Loh K, Fardella CE et al. J Clin Endocrinol Metab 2004..

If aldosterone is an “evil” hormone and primary hyperaldosteronismis worse than hypertension alone, should we undertake a thorough
search for this condition in all patients with hypertension?

Who should be screened for PA?Who should be screened for PA?
Hypertension and hypokalemiaResistant hypertensionAdrenal incidentaloma and hypertensionOnset of hypertension <20 years of ageSevere hypertension (>160/100 mm Hg)Whenever considering secondary hypertension
Young WF. Clinical Endocrinology 2007; 66:607-618

How to screen?How to screen?
Plasma aldosterone/plasma renin activity ratioCorrect hypokalemiaLiberalize sodium intakeWithdraw MCH receptor blockers, OC 4 weeksUse α blockers + verapamil if needed for HT

CONCLUSIONSCONCLUSIONS
Primary hyperaldosteronism is a more frequent cause of hypertension than previously thought.
Primary hyperaldosteronism can be diagnosed by the combination of a high PA/PRA ratio and failure to suppress aldosterone with volume-expanding maneuvers.
At present time, case detection can be recommended only for selected patient groups.
Primary hyperaldosteronism should be diagnosed not only to treat hypertension but also because aldosterone by itself may be harmful for the cardiovascular system and kidneys.