
Controversial Issues in the Management of Childhood Asthma: Insights...
46
Controversial Issues in the Management of Childhood Asthma: Insights from NIH Asthma Network Studies Stanley J. Szefler, MD Helen Wohlberg and Herman Lambert Chair in Pharmacokinetics, Head, Pediatric Clinic Pharmacology, National Jewish Health & Professor of Pediatrics and Pharmacology, University of Colorado School of Medicine
Transcript of Controversial Issues in the Management of Childhood Asthma: Insights...
Controversial Issues in the Management of Childhood Asthma:
Insights from NIH Asthma Network Studies
Stanley J. Szefler, MD
Helen Wohlberg and Herman Lambert Chair in Pharmacokinetics,Head, Pediatric Clinic Pharmacology,
National Jewish Health&
Professor of Pediatrics and Pharmacology,University of Colorado School of Medicine

Learning Objectives
• To review recent studies that impact the approach to asthma therapy.
• To summarize key findings that differentiate treatment by age in children.
• To indicate methods to select therapy to optimize effect and minimize adverse effects.

DisclosureConsultant for Boehringer Ingelheim, Genentech,
Glaxo Smith Kline, Merck, Novartis
Grant support:NHLBI Childhood Asthma Management
Program, Asthma Clinical Research Network,Childhood Asthma Research and Education Network and AsthmaNet
NIAID Inner City Asthma Consortium NIEHS/EPA Childhood and Environmental
Health Center Grant

Disclosure
Grant support (continued):CDPHE Colorado Cardiovascular, Cancer and
Pulmonary Disease ProgramCaring for Colorado Foundation, Glaxo Smith Kline Health Outcomes Program.

THE CHANGING FACES OF ASTHMA
Time Period Goal of Management Medications
1960’s1970’s1980’s
1990’s
2000’s2010’s
Relieve bronchospasmPrevent bronchospasmPrevent allergen induced
bronchospasm
Prevent and resolve inflammation
Achieve asthma controlPersonalized medicine;Early intervention
EpinephrineAlbuterol, theophyllineCromolyn
Inhaled glucocorticoidsLeukotriene modifiersLong acting ß-agonistsCombination therapyAnti-IgEBiomarkers/Genetics;Immunomodulators?

THE CHANGING FACES OF HEALTH CARE
Time Period Management Goals Contact
1950’s1960’s1970’s1990’s2000’s2010’s
Relief of symptomsSymptom managementSymptom preventionDisease managementDisease controlDisease prevention
Physician onlyPhysician/secretaryPhysician/office staffMultiple physiciansMultidisciplinary staffStrategic Partners

Primary Goal of Therapy: Achieving and Maintaining Asthma Control
• Primary goal of asthma therapy is to enable a patient to achieve and maintain control over their asthma- Eliminate impairments including
symptoms, functional limitations, poor quality of life, and other manifestations of asthma
- Reduce risk of exacerbations, ED visits, and hospitalizations
• Treatment goals are identical for all levels of asthma severityNHLBI. National Asthma Education and Prevention Program. Full report of the Expert Panel: Guidelines for the
Diagnosis and Management of Asthma (EPR-3). Available at: http://www.nhlbi.nih.gov/guidelines/asthma/asthgdln.htm. Accessed August 31, 2007.

Pediatric Population
• NAEPP defined three age groups- 12 years and above- 5 to 11 years of age- Less than 5 years of age
• Treatment goals are identical for all age groups
• Treatment steps vary by age due to available studies and disease presentation.
NHLBI. National Asthma Education and Prevention Program. Full report of the Expert Panel: Guidelines for the Diagnosis and Management of Asthma (EPR-3). Available at: http://www.nhlbi.nih.gov/guidelines/asthma/asthgdln.htm. Accessed August 31, 2007.

Assessing Asthma Control and Adjusting Therapy
in Youths 12 Years of Age and Adults

Stepwise Approach for Managing Asthma in Youths >12 Years of Age and Adults

Stepwise Approach for Managing Asthma in Children Aged 5–11 Years
RecommendedStep for Initiating
Treatment
Classification of Asthma SeverityIntermittent Persistent
Step 1Mild Moderate Severe
Step 2 Step 3 Step 3 or 4
Step up if needed
(first, check adherence,
environmental control, and
comorbid conditions)
Assess control
Step down, if possible
(and asthma is well controlled
for at least 3 months)
IntermittentAsthma
Persistent Asthma: Daily MedicationConsult with asthma specialist if step-4 care or higher is required.
Consider consultation at step 3.Step 1 Step 2 Step 3 Step 4 Step 5 Step 6
Preferred:SABA prn
Preferred:low-dose ICSAlternative:
cromolyn, LTRA,nedocromil, or theophylline
Preferred:EITHER:
low-dose ICS + LABA, LTRA, or
theophyllineOR
medium-dose ICS
Preferred:medium-dose ICS
+ LABAAlternative:
medium-dose ICS+ LTRA or
theophylline
Preferred:high-dose ICS
+ LABAAlternative:
high-dose ICS + either LTRA or
theophylline
Preferred:high-dose ICS +
LABA + oral systemic
corticosteroidAlternative:
high-dose ICS + LTRA or
theophylline + oral systemic
corticosteroid
Patient Education and Environmental Control at Each StepSteps 2–4: Consider subcutaneous allergen immunotherapy for patients who have allergic asthma.
Quick-Relief Medication for All Patients
NAEPP, NHLBI, NIH. Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma. August 2007.
Presenter
Presentation Notes
Stepwise Approach for Managing Asthma in Children Aged 5–11 Years For children aged 5 to 11 years, LTRAs are still a recommended alternative to ICSs.1 Additionally, an LTRA or a LABA may be added to low-dose ICSs rather than increasing the dose in patients with moderate persistent asthma.1 Please note that these National Institutes of Health treatment tables may contain information about certain products and uses that are not approved by the US Food and Drug Administration. For more details, please consult the individual product’s prescribing information. Reference: 1.National Asthma Education and Prevention Program, National Heart, Lung, and Blood Institute, National Institutes of Health. Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma; Full Report 2007. Bethesda, MD: US Dept of Health and Human Services: August 2007. �NIH publication 07-4051.
Approaches toPersonalizing Asthma Management• Early intervention strategies – Who?
What treatment? What outcomes?• Biomarkers – Which ones? What
application?• Combination therapy – How soon?
What type?• Genetics/epigenetics – Are we there
yet?• Immunomodulators – benefit-risk?
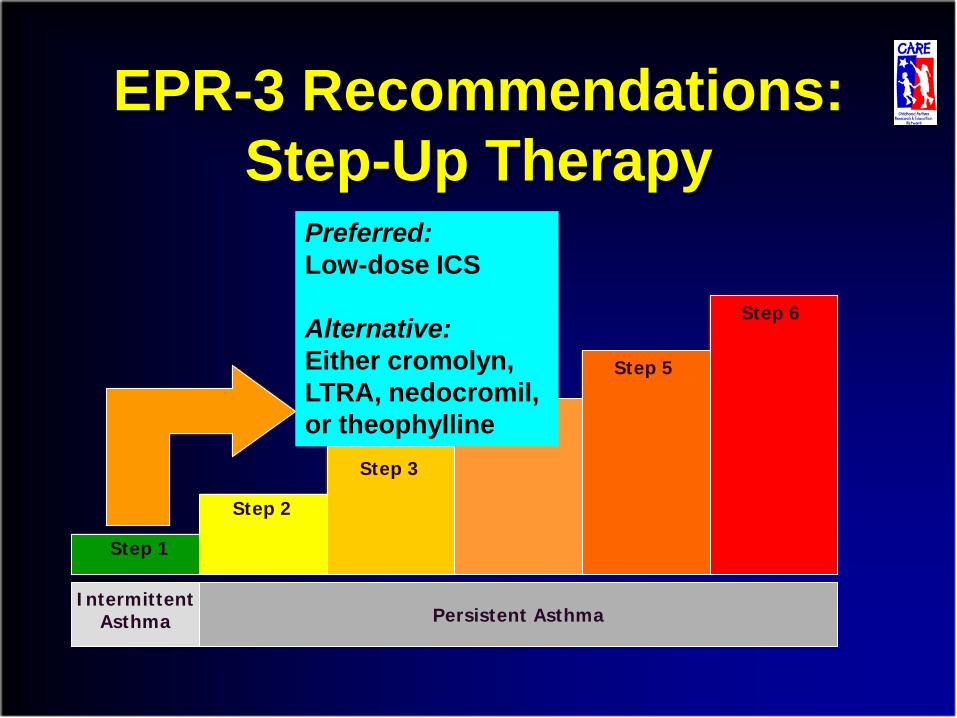
EPR-3 Recommendations:Step-Up Therapy
IntermittentAsthma Persistent Asthma
Step 1
Step 2
Step 3
Step 4
Step 5
Step 6
Preferred:Low-dose ICS
Alternative:Either cromolyn, LTRA, nedocromil, or theophylline
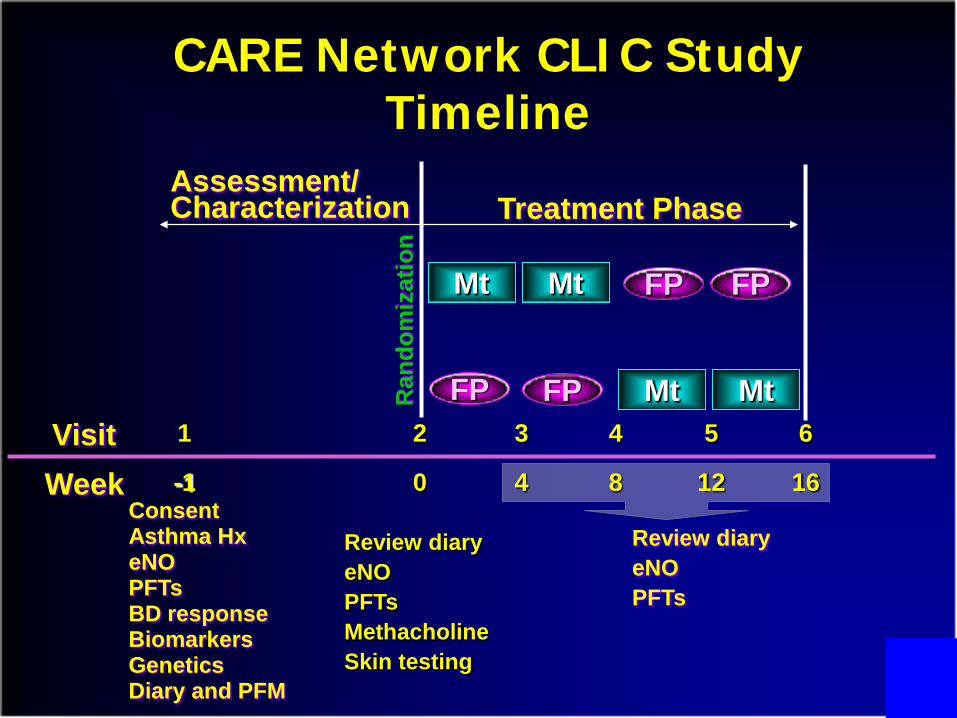
CARE Network CLIC Study Timeline
Assessment/Characterization
Mt
Treatment Phase
FP
Mt
FP
FP FP
Mt Mt
ConsentAsthma HxeNOPFTsBD responseBiomarkersGeneticsDiary and PFM
Review diaryeNOPFTsMethacholineSkin testing
Visit 1 2 3 4 5 6
Week -1 0 4 8 12 16
Review diaryeNOPFTs
Ran
dom
izat
ion
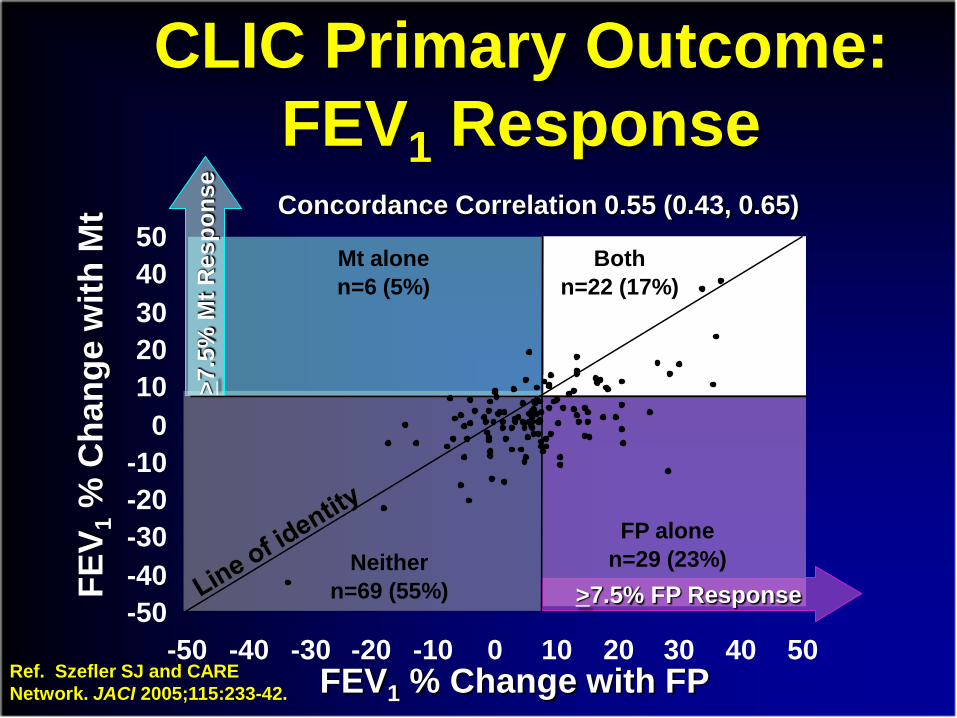
CLIC Primary Outcome: FEV1 Response
FEV1 % Change with FP
FEV 1
% C
hang
e w
ith M
t
Mt alonen=6 (5%)
Neithern=69 (55%)
FP alonen=29 (23%)
Bothn=22 (17%)
Concordance Correlation 0.55 (0.43, 0.65)>7
.5%
MtR
espo
nse
>7.5% FP Response
Ref. Szefler SJ and CARE Network. JACI 2005;115:233-42.
-50-40-30-20-10
01020304050
-50 -40 -30 -20 -10 0 10 20 30 40 50

Baseline Characteristic (Categorical) FP Mt
FEV1 < 90% predicted (pre-BD) 4.16** 1.78FEV1/FVC < 0.80 (pre-BD) 4.26** 2.40*Methacholine PC20 ≤ 1 mg/ml 2.62* 1.17eNO > 25 ppb 2.75* 2.03TEC > 350 cells/mm3 2.34* 1.62Serum ECP > 15 µg/L 2.78** 1.18IgE > 200 kU/L 2.86** 0.96uLTE4 > 100 pg/mg 2.03 3.22*Female 1.14 2.30Minority 0.84 1.98Age ≤ 10 years 0.64 2.50*
**p ≤ 0.01; *p ≤ 0.05
CLIC FEV1 Response ≥ 7.5%:Odds Ratio
Ref. Szefler SJ and the CARE Network. J Allergy Clin Immunol 2005;115:233-42.

CLIC Differential Response Analysis
• Higher bronchodilator use
• Greater response to bronchodilator
• Higher exhaled nitric oxide
• Higher serum eosinophilic cationic protein
• Lower pre-bronchodilator FEV1 percent predicted
• Lower FEV1/FVC
• Lower methacholine PC20
Greater response to fluticasone over montelukast for increased FEV1 was associated with:
Ref. Szefler SJ and the CARE Network. J Allergy Clin Immunol 2005;115:233-42.

CLIC Conclusions
• Children with lower pulmonary function or higher levels of markers associated with allergic inflammation should receive ICS therapy.
• Children without these indicators could receive a therapeutic trial of either ICS or LTRA.
How does the asthma-related phenotype influence the choice of medication selected to improve pulmonary function?
Ref. Szefler SJ and the CARE Network. J Allergy Clin Immunol 2005;115:233-42.
Follow-up Study
• LTE4/FENO ratios were associated with a greater response to montelukast than FP for FEV1 and for asthma control days.
• Children with high LTE4/FENO ratios were likely to be younger and female and exhibit lower levels of atopic markers and methacholine reactivity.
Can we predict who would have a better response to montelukast over ICS?
Ref. Rabinovitch N and the CARE Network. J Allergy Clin Immunol 2010;126:545-51 and 959-61.

EPR-3 Recommendations:Step-Up Therapy
IntermittentAsthma Persistent Asthma
Step 1
Step 2
Step 3
Step 4
Step 5
Step 6

BADGER Protocol: Overview
Period 1 Period 2 Period 3Run-in period on 1xICS to demonstrate
lack of control
16 weeks 16 weeks 16 weeks
Run-in Period 2-8 weeks
Randomization
Three Treatment Period, Double blind, 3 way cross-over
2.5 x ICS = fluticasone DPI 250 µg BID
1xICS+LABA = fluticasone/salmeterol DPI 100/50 BID
1xICS+LTRA = fluticasone DPI 100 µg BID + montelukast
1xICS = fluticasone DPI 100 µg BID
2.5 x ICS or
1x ICS + LABA or
1 x ICS + LTRA
2.5 x ICS or
1x ICS + LABA or
1 x ICS + LTRA
2.5 x ICS or
1x ICS + LABA or
1 x ICS + LTRA
Evaluation Period Evaluation Period Evaluation Period

LABA
ICS
Primary Outcome: Probability of BESTResponse Based on Composite Outcome*
LTRA
*Ref. Lemanske RF and CARE Network. NEJM 2010;362:975-985.
LABA step-up was more than 1.5 times as likely to produce the best response
(p = 0.002)
(p = 0.004)

BADGER Study: Conclusions
• Significant variability in treatment response was noted at the Step-3 level.
• LABA step-up therapy was more than 1.5 times as likely to produce the best response.
• Many children demonstrated a best response to either step-up ICS or LTRA.
• Several characteristics, such as baseline ACT®, eczema, and race could be useful in selecting medication treatment for best response.
Ref. Lemanske RF and CARE Network. NEJM 2010;362:975-985.

Summary Points• Inhaled corticosteroids are the preferred long-
term controller therapy at Step 2 level.• At Step 3 Level, LABA step-up therapy was
more than 1.5 times as likely to produce the best response.
• LTRA are alternative choices for Step 2 long-term controller and supplementary Step 3.
• Variable response can occur at either Step 2 or Step 3 therapy and alternative treatments may be selected within each Step before stepping up therapy.

Key Recommendations
• Diagnosis is often difficult.• Treatment has not been adequately studied.• Criteria for initiation of long-term control therapy:
- 3 wheezing episodes in past year and positive asthma risk profile.- those who require symptomatic treatment > 2 days per week - two or more severe exacerbations within 6 months
Managing asthma in children 0 - 4 years

NHLBI. National Asthma Education and Prevention Program. Full report of the Expert Panel: Guidelines for the Diagnosis and Management of Asthma (EPR-3). Available at: http://www.nhlbi.nih.gov/guidelines/asthma/asthgdln.htm. Accessed August 31, 2007.

• Randomized, multicenter, double-blind, parallelgroup, placebo-controlled trial
• 285 two and three year olds at high-risk for asthma• Fluticasone 44 µg/puff or placebo (2 puffs b.i.d.)
Year 3
Screening/Eligibility Run-in
Interim Efficacy Tests
PEAK: Study Design
Years 1 & 21 month
Randomize
Treatment Observation

0.75
0.80
0.85
0.90
0.95
1.00
6 12 18 24 30 36
† † †
†
ICSPlacebop<0.05p<0.01
Prop
ortio
n of
Epi
sode
-free
Day
s
Months
Episode-free Days During the Entire Study
Treatment Observation
Guilbert TW and CARE Network. NEJM 2006;354:1985-97. Copyright © [2006] Massachusetts Medical Society. All rights reserved.
Presenter
Presentation Notes
Episode-free days during the two-year treatment period. Fluticasone during the two-year treatment period, compared to placebo, significantly improved the proportion of episode-free days. Clear effect on treatment which disappeared off treatment. The proportion of episode days in the ICS group compared to the placebo group was 97% vs 96% at baseline, 96% vs. 89% at the end the treatment phase and 84% vs. 87% at the end of the observation year demonstrating increase in the frequency of asthma-like symptoms over time.
Outcomes During Observation Phase
• No differences between groups seen for:– Number of exacerbations requiring systemic
corticosteroid bursts– Unscheduled physician visits– Hospitalizations– Bronchodilator use– Montelukast use– Respiratory system impedance
• Average # of days of supplemental ICS use: 26% less in ICS group (p=0.007) during first 3 months
• There were no significant differences in adherence, completed visits, drop-outs, treatment failures or serious adverse events between study groups.
Presenter
Presentation Notes
During the observation year, no differences in the rates of systemic corticosteroid courses or montelukast use, rate of hospitalizations or lung function as measured by impulse oscillometry were seen between treatment groups; however, the active group had significantly less ICS use compared to the placebo group.
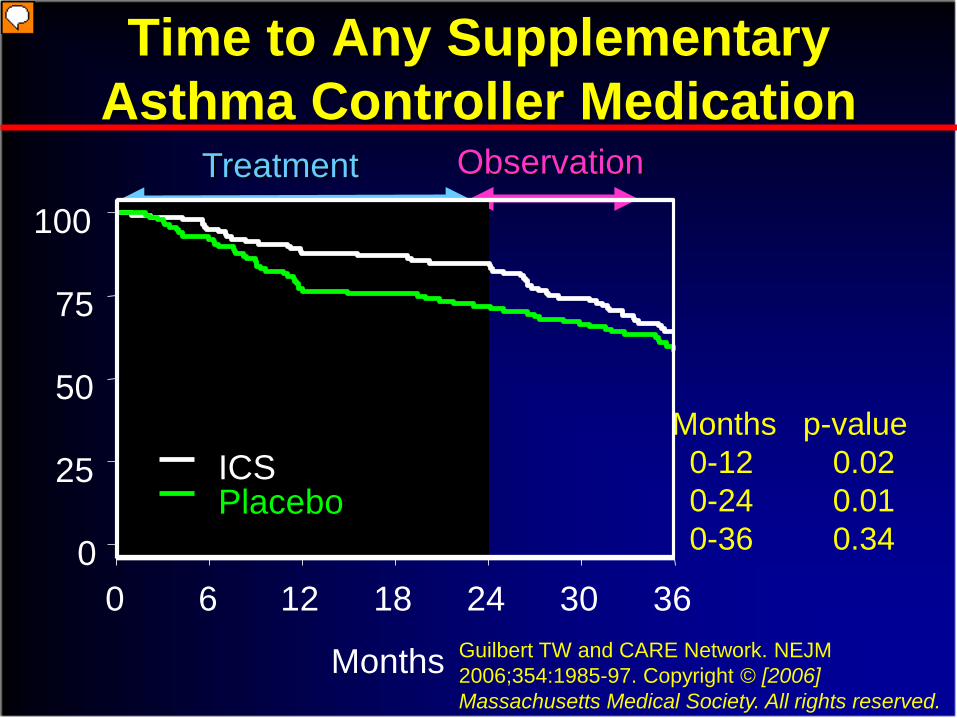
Time to Any Supplementary Asthma Controller Medication
Months p-value0-12 0.020-24 0.010-36 0.34
Treatment Observation
0 6 12 18 24 30 36
Months
0
25
50
75
100
ICSPlacebo
Guilbert TW and CARE Network. NEJM 2006;354:1985-97. Copyright © [2006] Massachusetts Medical Society. All rights reserved.
Presenter
Presentation Notes
Kaplan-Meier Estimates for Time to Initiation of Any Supplementary Asthma Controller Medication (Fluticasone, montelukast, or Other Nonassigned Asthma Medications). Time to initiation of any supplementary asthma controller medicine is significantly longer in the ICS group during the treatment period. Approximately 30% of the children in PEAK experienced a steroid exacerbation similar to the 40% of CAMP required steroids in placebo group.
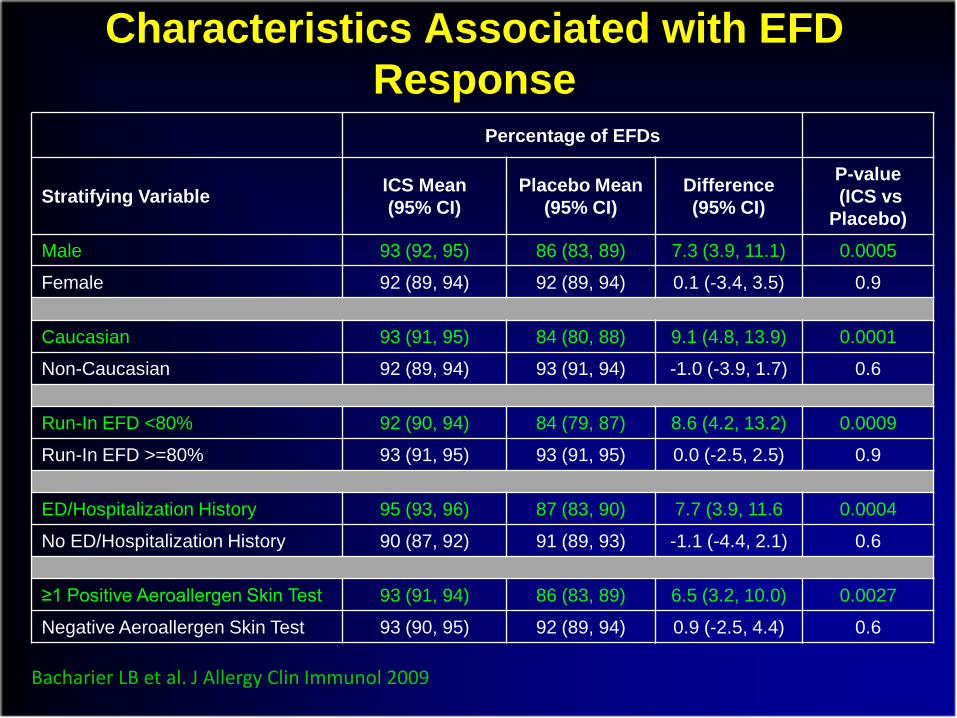
Characteristics Associated with EFD Response
Percentage of EFDs
Stratifying Variable ICS Mean (95% CI)
Placebo Mean (95% CI)
Difference(95% CI)
P-value(ICS vs
Placebo)Male 93 (92, 95) 86 (83, 89) 7.3 (3.9, 11.1) 0.0005
Female 92 (89, 94) 92 (89, 94) 0.1 (-3.4, 3.5) 0.9
Caucasian 93 (91, 95) 84 (80, 88) 9.1 (4.8, 13.9) 0.0001
Non-Caucasian 92 (89, 94) 93 (91, 94) -1.0 (-3.9, 1.7) 0.6
Run-In EFD <80% 92 (90, 94) 84 (79, 87) 8.6 (4.2, 13.2) 0.0009
Run-In EFD >=80% 93 (91, 95) 93 (91, 95) 0.0 (-2.5, 2.5) 0.9
ED/Hospitalization History 95 (93, 96) 87 (83, 90) 7.7 (3.9, 11.6 0.0004
No ED/Hospitalization History 90 (87, 92) 91 (89, 93) -1.1 (-4.4, 2.1) 0.6
≥1 Positive Aeroallergen Skin Test 93 (91, 94) 86 (83, 89) 6.5 (3.2, 10.0) 0.0027
Negative Aeroallergen Skin Test 93 (90, 95) 92 (89, 94) 0.9 (-2.5, 4.4) 0.6
Bacharier LB et al. J Allergy Clin Immunol 2009

Acute Intervention
Management Strategies
(AIMS)
A study evaluating the effects of episodic use of an inhaled corticosteroid or a leukotriene receptor
antagonist on the frequency and severity of acute wheezing episodes in young children
Presenter
Presentation Notes
I am delighted to have this opportunity to present the results of the CARE Network’s fourth clinical trial, AIMS....

Background• Population of interest
– Young children with intermittent wheezing and severe exacerbations
• Research questions– Does treatment with ICS or LTRA early in
the course of acute respiratory tract illnesses increase the proportion of episode free days over a 12 month period compared to conventional therapy*?
– Do these treatments modify the severity of the acute episodes?
*Conventional therapy - inhaled bronchodilator followed by the sequential addition of systemic corticosteroids
Presenter
Presentation Notes
In this population, we posed 2 research questions:...
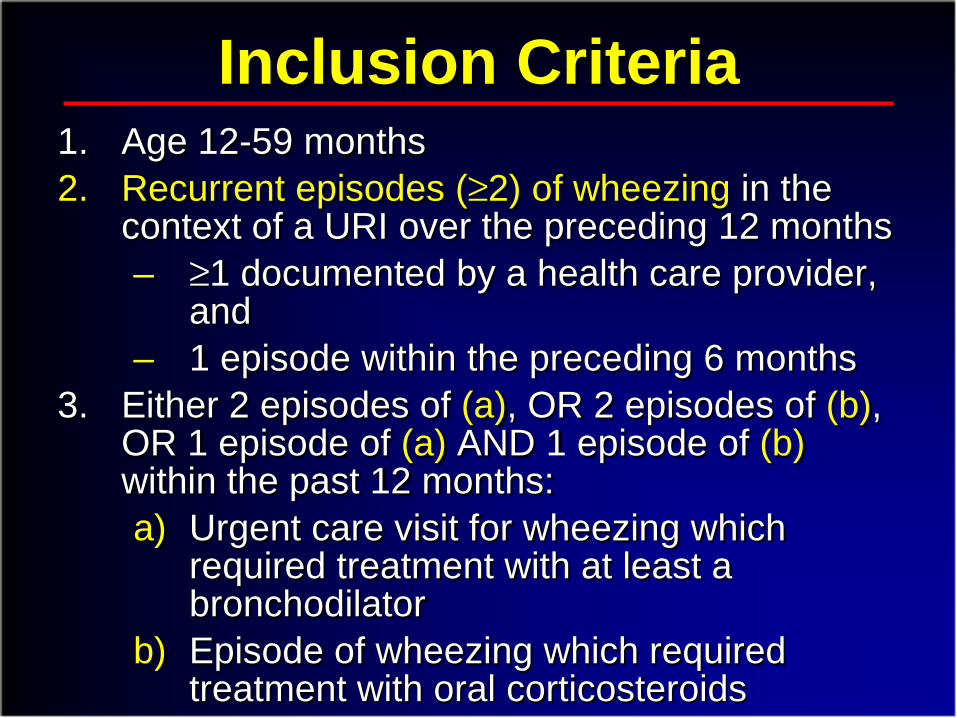
Inclusion Criteria1. Age 12-59 months 2. Recurrent episodes (≥2) of wheezing in the
context of a URI over the preceding 12 months– ≥1 documented by a health care provider,
and – 1 episode within the preceding 6 months
3. Either 2 episodes of (a), OR 2 episodes of (b), OR 1 episode of (a) AND 1 episode of (b) within the past 12 months:a) Urgent care visit for wheezing which
required treatment with at least a bronchodilator
b) Episode of wheezing which required treatment with oral corticosteroids

RandomizationRun-in
Study Overview
Drug Dosing DurationBudesonide (Pulmicort Respules® - AstraZeneca) 1.0 mg twice daily 7 days
Montelukast (Singulair® -Merck)
4mg granules (12-23 month)4 mg chewable tablets (24-59 months)
7 days
Albuterol - MDI or Nebulization Solution
(Proventil® – Schering)
4 times daily, thenas needed
2 days
2 weeks 52 weeks
At first sign of RTI –associated symptoms
ICS(Budesonide)
LTRA(Montelukast)
b2- agonist(Albuterol)
Active Placebo Active
Placebo Active Active
Placebo Placebo Active
Presenter
Presentation Notes
AIMS is a RANDOMIZED, DOUBLE BLIND, PLACEBO CONTROLLED DOUBLE DUMMY trial lasting 52 weeks examining the relative efficacies of 3 treatment strategies initiated at the 1st sign of RTI-associated symptoms. After a 2 week run in period to assure absence of persistent symptomatic asthma, children were randomized to 1 of 3 treatment arms. No daily therapy was prescribed. At the 1st sign of RTI-associated symptoms, parents were instructed to begin study medications. All participants received albuterol 4x daily for the 1st 2 days, followed by as needed use. 1 group received ICS in the form of budesonide 1mg twice daily for 7 days along with a placebo LTRA The 2nd group received LTRA in the form of montelukast 4mg once daily for 7 days along with placebo ICS. The conventional therapy group received placebos for both ICS and LTRA. Oral corticosteroids were available to all groups for rescue based upon protocol-defined criteria. Study medications and matching placebos were graciously donated by AstraZeneca, Merck and Schering.

Criteria for Starting Study Medications
• Identification by parental interview of the typical pattern of symptom progression from respiratory illness to chest symptoms for each child
• Development of an individualized action plan • Continual education to reinforce recognition
of this symptom pattern• Initiation of a 7-day study treatment course at
the onset of the identified symptom pattern
Presenter
Presentation Notes
This trial of episodic use of medications required establishing strict and individualized..... At all study contacts, there was continual..... Parents were instructed to initiate a 7-day....
-13 -7 1 7 14
0.0
0.2
0.4
0.6
0.8
1.0
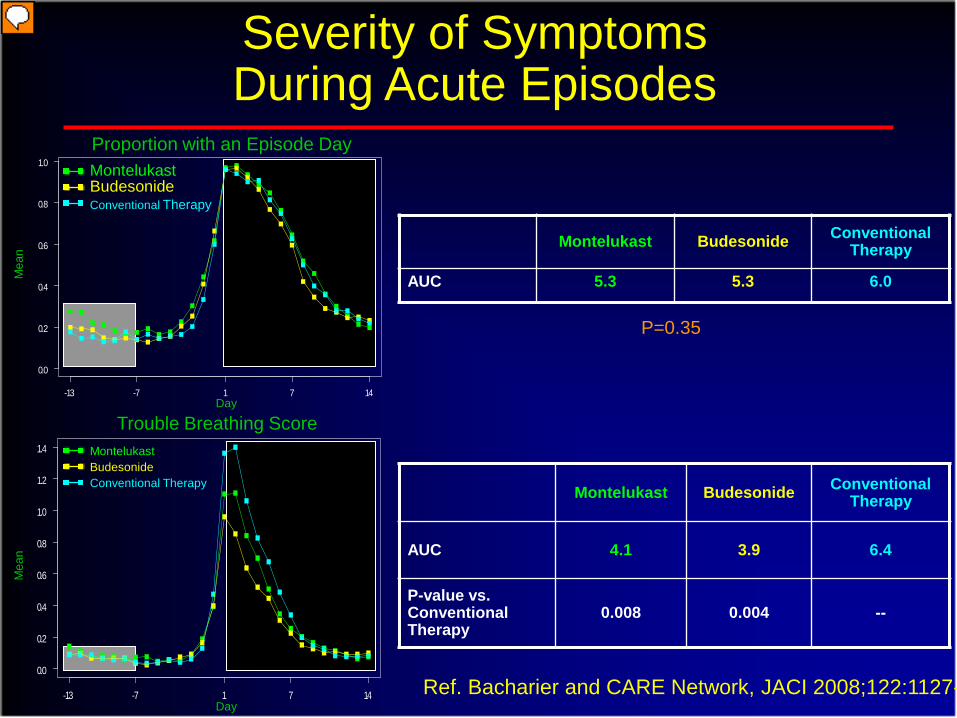
Severity of Symptoms During Acute Episodes
Montelukast Budesonide Conventional Therapy
AUC 5.3 5.3 6.0
Montelukast Budesonide Conventional Therapy
AUC 4.1 3.9 6.4
P-value vs. Conventional Therapy
0.008 0.004 --
P=0.35
MontelukastBudesonideConventional Therapy
MontelukastBudesonideConventional Therapy
Day
Day
Proportion with an Episode Day
Trouble Breathing Score
Mea
nM
ean
-13 -7 1 7 14
0.0
0.2
0.4
0.6
0.8
1.0
1.2
1.4
Ref. Bacharier and CARE Network, JACI 2008;122:1127-
Presenter
Presentation Notes
This slide depicts representative examples for 2 symptom components, episode days and trouble breathing score. The x-axis represents the day of illness, with day 1 defined as the day on which study medication was started, and the y-axis represents the symptom variable. In the upper panel, the y-axis represents the proportion of patients experiencing an episode day, with 100% having an episode day on day 1 of illness by definition. In the lower panel, the y-axis represents the mean trouble breathing score. The AUC for the baseline symptom level from 13 to 7 days prior to onset of illness is calculated in the area shaded in grey. This baseline level is then subtracted from the symptom AUC during the 14 days following initiation of study medication use, shown in black. The AUCs are then compared across treatment groups. In the upper panel, there is no significant difference between the 3 treatment groups in terms of episode days. In contrast, the lower panel demonstrates significantly lower AUCs for the montelukast and budesonide groups indicating lower trouble breathing scores over the illness period in these 2 groups.

Summary – Effect of Treatment Over 12 Months in the Entire Study Group
• The addition of montelukast or budesonide at the early signs of RTI-associated symptoms did not differ significantly from albuterol alone in:– The proportion of EFDs (primary outcome)– Oral corticosteroid use, urgent care visits,
hospitalizations (secondary outcomes)– Growth or adverse effects (thus, both
treatment approaches were safe)

Pediatric Asthma:Early Intervention
• Variability in asthma control should be anticipated• Reasons for variability should be identified and
addressed• Inhaled glucocorticoids are the preferred first line
long-term control therapy• Inhaled glucocorticoids are effective in alleviating
symptoms but do not alter the natural history of asthma.
• Alternative therapies merit investigation as potential interventions following early diagnosis of asthma.

Early Intervention
• Intermittent ICS therapy?• Prevent asthma exacerbations?• Montelukast as initial therapy?• Anti-IgE?• SLIT?• Other immunomodulator therapy?
Where do we go from here?

Maintenance vsIntermittent
Inhaled Steroids InWheezing Toddlers
(MIST) TrialA trial in preschool children with recurrent wheezing,
positive asthma predictive index and prior year severe wheezing exacerbation that compares the
effect of maintenance low-dose ICS versus intermittent high-dose ICS at the onset of respiratory tract illnesses on the rate of exacerbations requiring
systemic corticosteroids

Rationale for MIST
• Exacerbations & utilization major challenges in recurrent wheezing toddlers especially the high-risk.
• Two potential ICS regimens for control in toddlers– Maintenance low-dose ICS (PEAK)– Intermittent high-dose ICS during RTI (AIMS)
• More evidence-based data needed in the treatment of recurrent wheezing toddlers.
• A direct comparative trial is needed between maintenance low-dose ICS and intermittent high-dose ICS during RTI to reduce exacerbations.
• Such a study should be directed at the high-risk recurrent wheezing toddler

Interference With Stages of Asthma Progression
Established Disease
Post-NatalGenetics
Environment
Pre-NatalGenetics Exposure
Inception of Disease
Prevent
Cure
Treatment
Window
of Opportunity

Asthma Management
• Utilize asthma characteristics, biomarkers, and genetics to “profile” asthma severity and prognosis.
• Select medications based on driving factors of disease presentation and predictors of response.
• Monitor response and assess reasons for treatment failure.
• Develop proactive approach and adjust therapy accordingly.
Individualized or “Personalized” Approach

Where Do We Go From Here?
• Improve process of asthma management to apply step-care approach
• Identify alternative biomarker for Step 3• Assess “step-up” treatment strategies to
improve control and reduce exacerbations• Environment control measures• Reduce impact of viral infection• Immune-based therapy to reduce impact of
allergen-induced inflammation.
Possibilities to improve asthma control
Future Approaches toImproving Asthma Management
• Genetics• Early intervention• Immunomodulators• Biomarkers• Combination therapy


















