Control of Breathing
49
Control of Breathing
description
Control of Breathing . THE REGULATION OF ALVEOLARVENTILATION. The level of alveolar ventilation is driven mainly from the input of specific chemoreceptors to the central nervous system. Chemoreceptors monitor the chemical composition of body fluids. - PowerPoint PPT Presentation
Transcript of Control of Breathing

Control of Breathing



Objectives 1.Distinguish between the automatic and conscious/voluntary control of
breathing. Identify the key structures involved in generation of the resting quiet breathing rhythm of inspiration followed by expiration.
2.Specify the key sources of sensory input to the rhythm generator that modify its output to the respiratory muscles.
3.Identify the location of the central & peripheral chemoreceptors and describe their effect (if any) on ventilation in response to changes in arterial PCO2 , PO2 and pH.
4.Describe how a decrease in plasma pH regulates ventilation & partial pressures of oxygen and carbon dioxide in the blood. Provide examples of metabolic acids that have this effect in exercise and in diabetes.



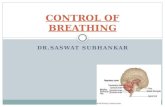
Brain stem area involved in respiratory control



Excites the inspiratory center in the medulla, prolonging the period of action potentials in the phrenic nerve, and thereby prolonging the contraction of the diaphragm.
The pneumotaxic center (location: upper pons) turns off inspiration, limiting the burst of action potentials in the phrenic nerve.Prolongs expiration

•The phrenic nerve is formed by rootlets exiting the cervical spine C3,C4,C5. Two bilateral phrenic nerves supply the hemidiaphragms. ”C3,4,5 keep the diaphragm alive”
• Intercostal nerves exiting thoracic & lumbar spine provide input to nerves supplying the intercostal & abdominal muscles










Central Chemoreceptors

1. Changing carbon dioxide levels:
Acute• Ventilation increases
linearly with any rise in PaCO2 above resting values, whereas ventilation decreases when PaCO2 falls below 40 mm Hg.
Chronic• Patients with chronic pulmonary
disease may not be able to ventilate at levels required to hold PaCO2 at 40 mm Hg.
• Ventilation increases initially when PaCO2 begins to rise because the pH of the CSF falls, but the choroid plexus responds by se-creting HCO3- into the CSF, which, over a period of 8–24 hours, largely offsets the effect of the higher PaCO2 on plasma pH.
• Thus, although PaCO2 may remain high, the medullary chemorecep-tors no longer register the change, and the respiratory control system adapts to a new, higher PaCO2.






Effect of Low Arterial PO2 to StimulateAlveolar Ventilation When Arterial CarbonDioxide and Hydrogen Ion ConcentrationsRemain Normal



Ventilatory responses to changes in arterial PCO2 (PaCO2) and PO2 (PaO2).



Composite Effects of PCO2, pH, andPO2 on Alveolar Ventilation

Acid–base Considerations
• When CO2 dissolves in water, it forms carbonic acid. Although a relatively weak acid, it is produced in such prodigious quantities (>20 moles/day) that it could seriously interfere with normal tissue function if its levels were not closely monitored and regulated.
• In practice, the central nervous system (CNS) maintains plasma pH within an extremely tight range (pH 7.35–7.45), in part by adjusting ventilation to hold Paco2 at around 40 mm Hg.


Causes of changes in extracellular fluid pH
• Changes in pH caused by the lungs are referred to as respiratory acidosis or respiratory alkalosis. Non respiratory changes are referred to as metabolic acidosis or metabolic alkalosis.– Respiratory acidosis: Increased Paco2 results from
hypoventilation, V̇A/ mismatches, or an increase in the Q̇diffusional distance between the alveolar sac and pulmonary blood supply (due to pulmonary fibrosis or edema, for example).
– Respiratory alkalosis: Paco2 decreases with hyperventilation, typically because of anxiety or other emotional state. It can also result from hypoxemia precipitated by ascent to high altitude.


Decreases in arterial pH
• Decreases in arterial pH cause an increase in ventilation, mediated by peripheral chemoreceptors for H+.
• This effect is independent of changes in the arterial PCO2 and is mediated only by chemoreceptors in the carotid bodies (not by those in the aortic bodies).

Decreases in arterial pH
• In metabolic acidosis, when there is decreased arterial pH, the peripheral chemoreceptors are stimulated directly to increase the ventilation rate (the respiratory compensation for metabolic acidosis)

Effect of Arterial pH on Respiration

H+ concentration(Metabolic alkalosis)

Primary pulmonary Hypoventilation

Primary Pulmonary hyperventilation

Abnormal Breathing Patterns
• Apneustic breathing• Biot’s breathing• Cheyne-Stokes breathing