Control and prevention of human plague
5
Indian J Pediatr 1994; 61 : 629-633 Control and Prevention of Human Plague Shashi Kant and L.M. Nath Department of Community Medicine, All India Institute of Medical Sciences, New Delhi Plague is essentially a disease of wild rodents. Sylvatic (wild) plague exists all over the world. In all some 200 or more species of rodents representing all the major families throughout the world can harbour plague naturally.' Natural foci of Sylvatic plague has been present in India all these years though no case of human plague was reported since 1967 until the present epidemic. Rodent plague activity continue to occur in most, if not all, existing world foci representing a major thrust of new outbreaks at any time in presently quiescent area. There are four players involved in initi- ating and maintaining plague among hu- man population viz. a flea, a rodent, a ba- cillus and man. Theoretically, the transmis- sion of the disease can be stopped if any one of these player is effectively managed. However, the ease with which any of these can be manipulated differs. An integrated approach, i.e. simultaneous action on all of them is far more rewarding because of synergy. Control of Fleas There are atleast 31 fleas which are proven vector of plague. 2 If fleas can be destroyed, Reprint requests: Dr. L.M. Nath, Professor & Head, Department of Community Medicine, All India Institute of Medical Sciences, Ansari Nagar, New Delhi-110 029. bubonic plague cannot be spread, so flea destruction by insecticide is the essential process in stopping spread. Control of flea should precede the destruction of rodents. There has been some suggestion that fleas have acquired resistance to commonly used insecticide e.g. DDT (dichloro-diphe- nyl-trichloroethane) and BHC (benzene hexachloride). If the fleas are sensitive then the powder of DDT (10%) or BHC (3%) can be used. If resistance is suspected to one or both of these insecticides then the dust of carbaryl (2%) or malathion (5%) should be used. Before commencing the spray, all food items and utensils should be removed from inside the house. The spray area should include the entire floor, walls upto three feet above the floor level, crevices in the wall, roofing of thatched houses, cloth- ing, bedding and pets like dogs, cats, etc. Burrows of the rodent should also be insuffiated with the insecticides. A flea index should be established and monitored. The total flea index is the average number of flea of all species per host, the specific flea index the average number of flea of each species per host and the burrow and nest flea index the average number of each species of flea per burrow or nest. Flea indices do not in themselves indicate an imminent plague epidemic. They serve as a warning that more stringent control measures are needed to protect human beings. During epidemic when insecticidal
-
Upload
shashi-kant -
Category
Documents
-
view
221 -
download
3
Transcript of Control and prevention of human plague

Indian J Pediatr 1994; 61 : 629-633
Control and Prevention of Human Plague
Shashi Kant and L.M. Nath
Department of Community Medicine, All India Institute of Medical Sciences, New Delhi
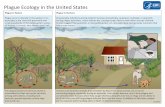
P l a g u e is essentially a disease of wild rodents. Sylvatic (wild) plague exists all over the world. In all some 200 or more species of rodents representing all the major families throughout the world can harbour plague naturally.' Natural foci of Sylvatic plague has been present in India all these years though no case of human plague was reported since 1967 until the present epidemic. Rodent plague activity continue to occur in most, if not all, existing world foci representing a major thrust of new outbreaks at any time in presently quiescent area.
There are four players involved in initi- ating and maintaining plague among hu- man population viz. a flea, a rodent, a ba- cillus and man. Theoretically, the transmis- sion of the disease can be s topped if any one of these player is effectively managed. However, the ease with which any of these can be manipulated differs. An integrated approach, i.e. simultaneous action on all of them is far more rewarding because of synergy.
Control of Fleas
There are atleast 31 fleas which are proven vector of plague. 2 If fleas can be destroyed,
Reprint requests: Dr. L.M. Nath, Professor & Head, Department of Community Medicine, All India Institute of Medical Sciences, Ansari Nagar, New Delhi-110 029.
bubonic plague cannot be spread, so flea destruction by insecticide is the essential process in stopping spread. Control of flea should precede the destruction of rodents. There has been some suggestion that fleas have acquired resistance to commonly used insecticide e.g. DDT (dichloro-diphe- nyl-trichloroethane) and BHC (benzene hexachloride). If the fleas are sensitive then the powder of DDT (10%) or BHC (3%) can be used. If resistance is suspected to one or both of these insecticides then the dust of carbaryl (2%) or malathion (5%) should be used. Before commencing the spray, all food items and utensils should be removed from inside the house. The spray area should include the entire floor, walls upto three feet above the floor level, crevices in the wall, roofing of thatched houses, cloth- ing, bedding and pets like dogs, cats, etc. Burrows of the rodent should also be insuffiated with the insecticides.
A flea index should be established and monitored. The total flea index is the average number of flea of all species per host, the specific flea index the average number of flea of each species per host and the burrow and nest flea index the average number of each species of flea per burrow or nest. Flea indices do not in themselves indicate an imminent plague epidemic. They serve as a warning that more stringent control measures are needed to protect human beings.
During epidemic when insecticidal

630 "It tE INDIAN JOURNAL OF PEDIATRICS 1994; Vol. 61. No. 6
spray is done, the flea index should drop to zero within 48 hrs of application.' Health personnel working in plague epidemic area should protect themselves against the insect bite by dusting their legs with insecticides or by application of insect repellant. Wearing of knee gum boots provides added protection against insect bite.
Control of Rodents
Plague is a disease of rodents which man can get due to this proximity to the rodents. Any measure which will keep them apart will reduce the risk of human plague. Attempt to destroy the rodents in the wild is doomed to fail because the nature restores the ecological balance fairly rapidly. Moreover, even if the concerned species is eliminated locally, its space will be occupied by others who may be hos t / vector for other diseases. In order to reduce the r o d e n t / m a n contact to the minimum possible, following measures are useful :
General Sanitation
Rodents get attracted to the house because of the availability of waste food material. Denial of food to the rodents by proper storage, collection and disposal of garbage will make the house less attractive to the rodents. Good quality housing which in- cludes rat proofing, will deny the rodents access to the house. Rat burrows should be blocked with concrete mixture. Sanitation is the long term solution of the problem and all other measures should be consid- ered supplementary to this effort. Destruc- tion of rodents should never be attempted unless a prior control of fleas has been
achieved., otherwise, depr ived of their natural host fleas would be forced to feed on humans.
Some places e.g. seaports, airports and container bases etc need to be kept free of rats. Trapping and subsequent killing of rats, and use of rodenticide will help to achieve this end. Trapping achieves tem- porary reduction of commensal rodents and rats being suspicious by nature quickly become "trap wise". It is impor- tant to kill the trapped rate by drawing it in the water.
Two types of rodenticide are available; single dose (acute) and multiple dose (cu- mulative). Single dose poison causes death of the rat within 3-48 hours. Barium car- bonate and zinc phosphide are the two commonly used single dose poison. The multiple dose rodenticide are anticoagu- lant and cause internal hemorrhage lead- ing to slow death 4-10 days.
Fumigation is an effective method for destroying both rat and its flea. Calcium cyanide powder, on contact with moisture produces hydrogen cyanide gas which is lethal to rat. This method is appropriate for eradication of rats from containers and ships. Apart from rodents a very large number of mammals may be infected with Yersinia pestis. Dogs may become infected without any sign of illness. 3 Cats suffers from plague and die. At least three cases are on record of plague in humans caught from domestic cats, and Y. pestis was iso- lated from the tissues of two of the cats. 4.-~
Control of Cases
The diagnosis of human plague in the ini- tial stages of the current epidemic, when no cases had been reported for the last 28 years, was difficult. However , during the

1994; Vol. 61. No. 6 THE tN DIAN JOURNAL OF I~c2)IATRICS 631
epidemic conditions the clinical diagnosis is fairly obvious. Efforts should be made to get the confirmatory lab. diagnosis, but un- der no circumstance the treatment be de- layed even to the suspected cases. Isolation of pneumonic plague patient is essential. Though the bubonic cases are not infec- tious, isolation is recommended even for these cases. Cases and dead bodies should be handled with universal precaution. The attendants on pneumonic cases should provide themselves with face masks, goggles and rubber gloves. Prompt notifi- cation of cases is a must. International Health Regulations requires that the na- tional governmental notifies WHO about the human plague cases within 24 hours. ~
PREVENTION OF PLAGUE
Prevention could be sought either by immunoprophylaxis or chemoprophylaxis.
Immunoprophylaxis
Over the years many workers have prepared anti-plague serum and claimed that it would reduce the morbidi ty and mortality. No unequivocal proof could be established about their utility and hence WHO in 1970 decided against recommending the use of anti-plague serum. 7
Many different types of vaccine preparations, including both live and killed vaccines, have been developed and used in the past. Currently available vaccines can be broadly divided into the following categories-
1. Killed Vaccines. a. Halffkine broth vaccine; b. Casein hydrolysate direct vac- cine; c. Agar grown vaccine.
2. Live Attenuated Plague Vaccine.
3. Chemically Extracted Specific Protein of Y. pestis.
Killed Vaccines
Haffkine browth vaccine is the most toxic among the killed vaccines. Agar grown vaccine which is currently available in United States is the least toxic. Agar grown vaccine is practically free from nonspecific proteins, least toxic, more potent and eco- nomical to produce.
The vaccine available in United States contains killed virulent strain of yersinia (Indian isolate 195P). The vaccine is an aqueous suspension of 2000 million bacilli per ml. The baccilli is killed by formalin and preserved by adding phenol. The primary series of vaccination consists of three doses given intra-muscularly. Adults and children over ten years receive lml as initial dose to be followed by 0.2 ml four weeks later. Third dose of 0.2 ml is given six months after the first dose. Reduced dosage are given to children below ten years. Booster doses need to be given every six months upto three times after which booster can be given once every 1-2 years.
Vaccine produced in India is casein hydrolysate direct vaccine. It contains 2000 million organism per ml. The pr imary series of vaccination consists of two doses. The dose, route of administration and is schedule are different from that applicable in US. Initial adult dose is 0.5 ml given subcutaneously. Second dose of 1 ml is given 7-14 days after the first dose. Reduced dosage are given to children as per the recommendat ion of the manufacturer. One suggest vaccination schedule for children is as follows. ~

632 THE INDIAN JOURNAL OF PEDIATRICS 1994; Vol. 61. No. 6
Age 1st dose 2nd Dose 6 Monthly (yrs) Booster Dose
1-4 0.2 ml 0.4 ml 0.2 ml
5-10 0.3 ml 0.6 ml 0.3 ml
11-16 0.4 ml 0.8 ml 0.4 ml
Yet another schedule of killed plague vaccine for children as suggested by Forfear and ArneiP is as follows:
Age 1st Dose 2nd Dose (yrs)
1-5 0.1 ml 0.2 ml
5-12 0.25 ml 0.5 ml > 12 0.5 ml 1.0 rnl
Infants should not be given plague vac- cine. Booster is recommended every six months.
Booster doses are recommended every six months. Immunity starts developing af- ter 5-7 days of vaccination and lasts for about six months. Side effect of vaccine in- cludes fever, headache, malaise, lymphadenopathy, erythema and indura- tion at the injection site. The severity of side effects tend to increase with repeated vaccination. Repeat vaccination is not rec- ommended for persons who developed se- vere local or systemic reaction. The vaccine should not be given to persons with known hypersensi t ivi ty to beef protein, soya, casein or phenol. The vaccine is contraindicated for pregnant women be- cause of its potential to induce abortion or fetal abnormalities.
Live Attenuated Plague Vaccine.
Most of the live attenuated vaccines use EV 76 strain of yersinia pestis. This viru-
lent strain is maintained in pure culture form at the Pasture Institute, Paris. The strain contains Fraction 1 (envelope sub- stance) antigen which evokes production of protective antibodies. The vaccine strains invade the tissue and multiply but cannot proliferate at a rate which can pro- duce the disease.
Introduction of live vaccine through oral rout in the form of lozenges has also been tried. The drawback in this instance was that 45% of recipient developed local tonsilar or pharyngal reaction.
The side effects of the live vaccine are same as the killed vaccine albeit more pro- nounced. Additional problems associated with live vaccine includes wide variation in their immunogenici ty and virulence. The most alarming feature of live vaccine, however, is its potential to revert to viru- lent form.
There have been conflicting report re- garding the superiority of live versus killed vaccine. However neither vaccine provides absolute and /o r long lasting im- munity. Usually there is a clamour for vac- cination during an epidemic. This tempta- tion must be resisted because mass vacci- nation has absolutely no role in containing the epidemic. Spread of plague is to fast for this purpose. Moreover, widespread and severe side effects of tile vaccination renders it unfit for mass vaccination usage.
Plague vaccination is recommended only for small selected group of people. The Advisory Committee of Immunization Practices in the United States in 1982 rec- ommended that plague vaccination be given to the following group of people-
1. Field workers-e.g, ecologist, archae- ologist, biologist, geologit etc planning to work in an area known to have rodent plague.

1994; Vol. 61. No. 6 THE INDIAN JOURNAL OF PEDIATPd(2S 633
2. Laboratory workers who handle plague culture or plague infected animals.
3. Medical workers and public health workers who are dealing plague patients or who investigate plague outbreaks.
Thus plague vaccine is to be given to small group of people who are exposed to higher risk of contracting disease due to their vocation. Routine immunization for travelers going to plague endemic area is not recommended. Similarly vaccination is not advised to the residents of plague en- demic area.
The vaccine is believed to provide protection against fleaborne plague and might not be effective against airborne infection. 7 Therefore, persons who have been exposed to pneumonic plague must be advised chemoprophylaxis irrespective of their immunization status. Because the immunity provided by the vaccine is partial, any person who has had a definitive exposure should be put on prophylactic antibiotics, irrespective of his/her immunization status.
C h e m o p r o p h y l a x i s .
Prophylactic use of tetracycline is recommended for persons who are at risk for a short period. This includes contacts of plague patient, persons visiting plague epidemic area for a short time etc. In selected population it may also be used as a short term major in small explosive
outbreak until other measures can be initiated. Tetracycline in dosage of 10-15 mg /kg body weight (adult dose : 500 mg) every six hours for five days is recommended. The protection will wane as soon as the blood level of the antibiotic falls.
REFERENCES
1. Bahmanyar M, Cavanaugh DC. Plague Manual. Geneva : World Health Organisation, 1976.
2. Bleding JL. Textbook of Parasitology, 3rd edition. New York : Appleton-Century- Fox, 1965.
3. Rust JH, Miller BE, Bahmanyar M et al. The role of domestic animals in epidemi- ology of Plague. II. Antibody to Yersinia pestis in sera of dogs and cats. J Infect Dis 1971; 5 : 527-531.
4. Morbidity Mortality Weekly Report {USA) 1977; 26 : 337. Plague, United States.
5. Morbidity Mortality Weekly Report (USA). 1977; 26 : 215. Plague-Arizona, Colorado, New Mexico.
6. World Health Organization. International Health Regulations (1969). Third annotated edition, WHO, Geneva.
7. World Health Organisation. Technical Re- port series. 1971, no 447. WHO, Geneva.
8. Banker, DD. As quoted in Park JE, Park E. Textbook of Preventive and Social Medicine. llt~ edition, Jabalpur : Publishers Banarasidas Bhanot, 1986.
9. Forfear JO, Arneil GC, eds. Textbook ~ Paediatrics. 2nd edition, New York : Churchill-Livingstone, 1987.