Contraceptive Technology - Advance Family...
46
Contraceptive Technology March 14, 2013 Anne Burke, MD, MPH Associate Professor, Gynecology and Obstetrics/ Population, Family, Reproductive Health Medical Advisor, Gates Institute Johns Hopkins University (with thanks to Jeff Spieler, USAID)
Transcript of Contraceptive Technology - Advance Family...
Contraceptive Technology March 14, 2013
Anne Burke, MD, MPH Associate Professor, Gynecology and Obstetrics/
Population, Family, Reproductive Health Medical Advisor, Gates Institute
Johns Hopkins University
(with thanks to Jeff Spieler, USAID)
Priorities in Contraceptive Technology
l Expand access to, and availability of, EXISTING contraceptive methods (public and private sectors)
l Make existing methods EASIER, CHEAPER, BETTER
l Develop TOTALLY NEW TECHNOLOGY that can address unmet needs
Long-Acting Reversible Contraception
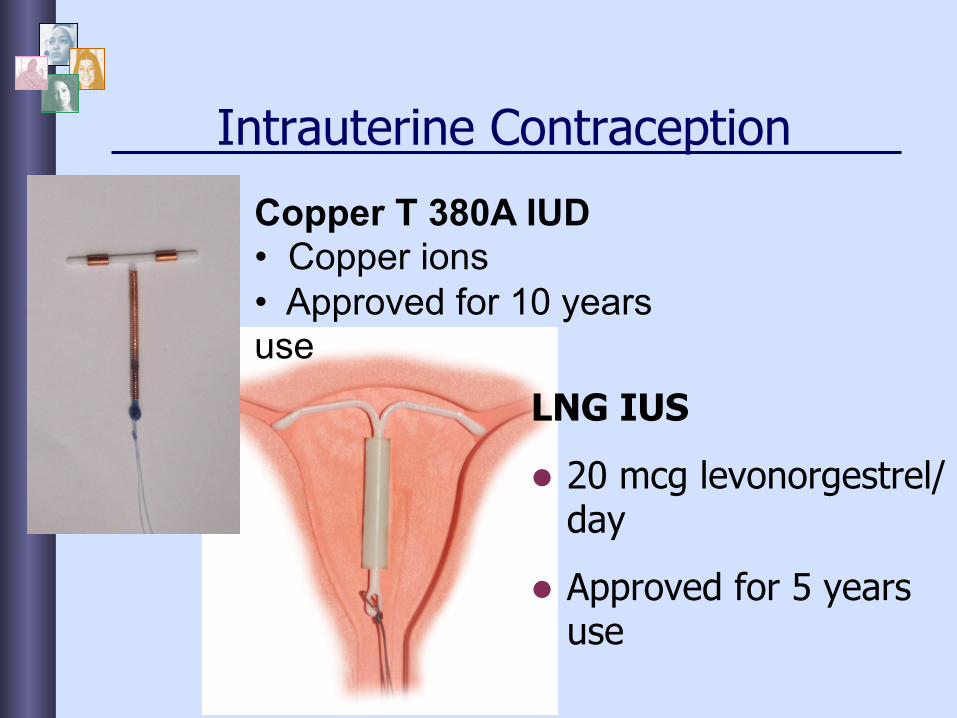
Intrauterine Contraception
LNG IUS
l 20 mcg levonorgestrel/day
l Approved for 5 years use
Copper T 380A IUD • Copper ions • Approved for 10 years use
IUDs: Mechanism
l Mechanism: primarily by preventing fertilization w Copper has direct effects on uterus, sperm and ova
w Levonorgestrel:
§ THICKENS cervical mucus
§ THINS endometrial lining
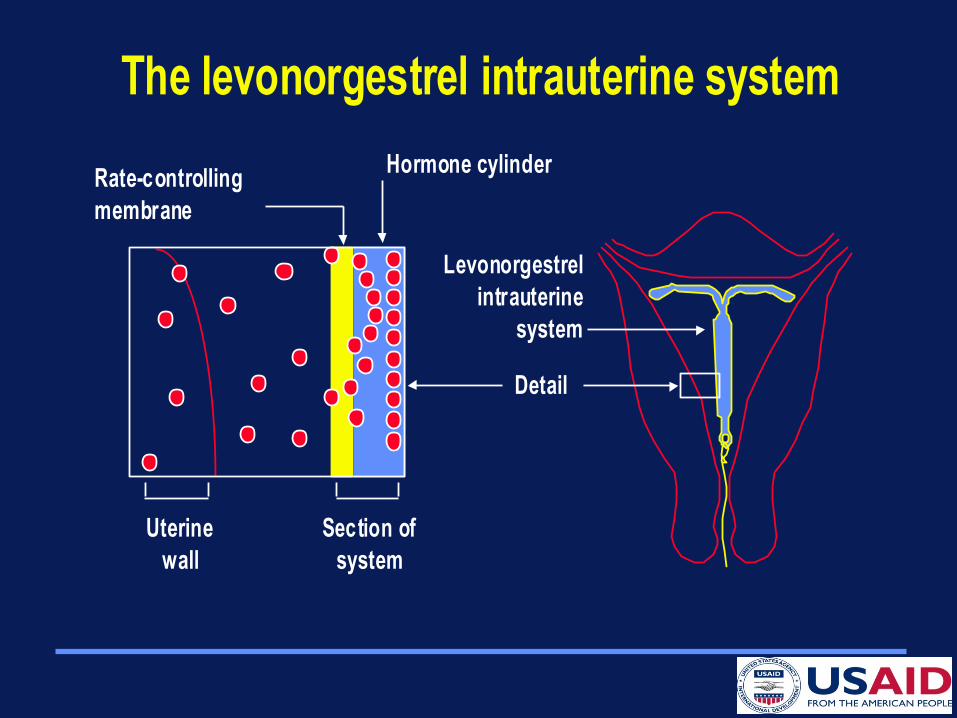
The levonorgestrel intrauterine system
Levonorgestrelintrauterine
system
Detail
Hormone cylinderRate-controllingmembrane
Uterinewall
Section ofsystem
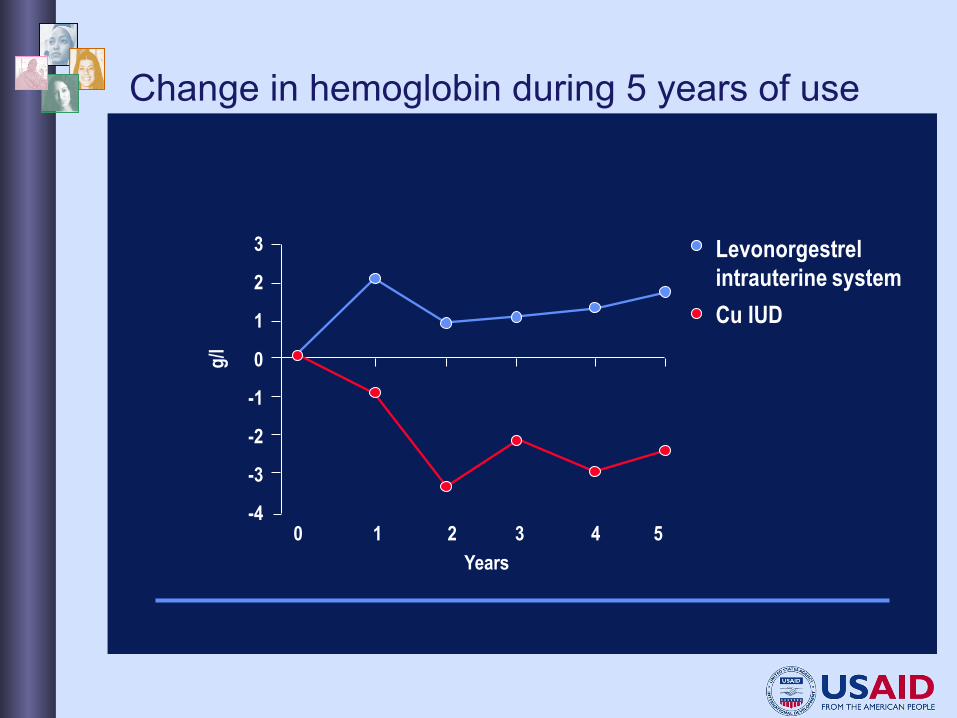
Years
Levonorgestrel intrauterine systemCu IUD
0 1 2 3 4 5
3
2
1
0
-1
-2
-3
-4
g/l
Change in hemoglobin during 5 years of use
Can IUD be used in:
l Adolescents?
l Nulliparous women?
l Women with previous pelvic infection?
l Women with HIV?
Can IUD be used in:
l Adolescents?
l Nulliparous women?
l Women with previous pelvic infection?
l Women with HIV?
YES!

Newly approved IUD
l “Skyla ®”
l A little smaller
l A little less hormone
l 3 years
Implanon/Nexplanon™ Etonogestrel Implants
l Progestin-only method
l 4 x 0.2cm
l Prevents ovulation
l Long-acting (3 years)
l Main side-effect is unpredictable menstrual cycles
l Fertility returns within a few days of removal
l Highly effective

Other implantable contraceptives
l Jadelle, Sinoplant
w 2-rod implant (levonorgestrel)
w Wide distribution in other countries
Zarin® (Sino-implant II)
l Subdermal Contraceptive Implant
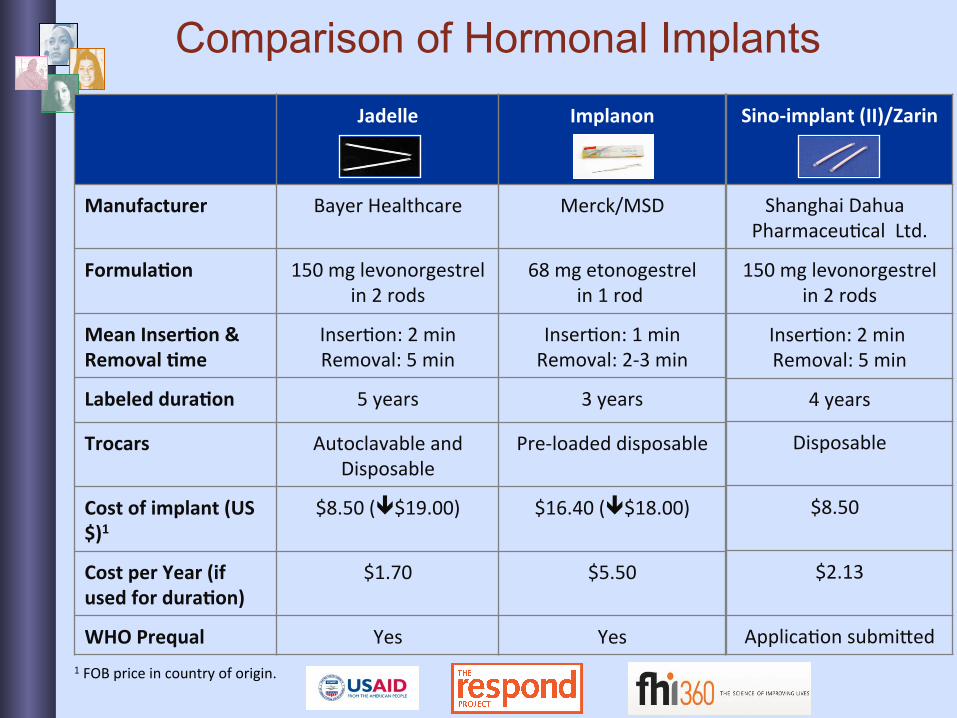
Sino-‐implant (II)/Zarin
Shanghai Dahua Pharmaceu/cal Ltd.
150 mg levonorgestrel in 2 rods
Inser/on: 2 min Removal: 5 min
4 years
Disposable
$8.50
$2.13
Applica/on submiGed
Comparison of Hormonal Implants Jadelle Implanon
Manufacturer Bayer Healthcare
Merck/MSD
Formula:on 150 mg levonorgestrel in 2 rods
68 mg etonogestrel in 1 rod
Mean Inser:on & Removal :me
Inser/on: 2 min Removal: 5 min
Inser/on: 1 min Removal: 2-‐3 min
Labeled dura:on 5 years 3 years
Trocars Autoclavable and Disposable
Pre-‐loaded disposable
Cost of implant (US$)1
$8.50 (ê$19.00) $16.40 (ê$18.00)
Cost per Year (if used for dura:on)
$1.70 $5.50
WHO Prequal Yes Yes 1 FOB price in country of origin.
Characteristics of LARC
l Immediately effective
l HIGHLY effective
l Safe
l Rapid return of fertility after removal
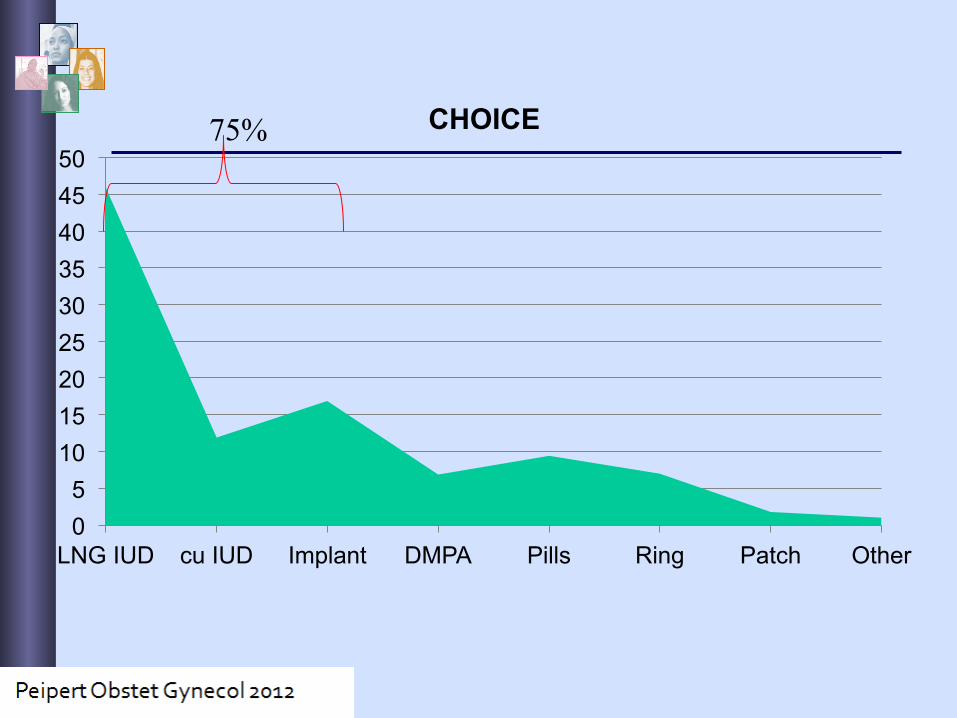
0 5
10 15 20 25 30 35 40 45 50
LNG IUD cu IUD Implant DMPA Pills Ring Patch Other
CHOICE 75%
Review of Safety of Postpartum IUD Cochrane database review, 2003
Main results l Immediate post-partum insertion of IUDs
appeared safe and effective. l Few contraindications to method l Expulsion rates appear to be higher
than with interval insertion. l Feasibility supported by PPIUD insertion
popularity in countries as diverse as China, Mexico, and Egypt.
l Early follow-up (6 weeks) may be important in identifying spontaneous IUD expulsions
Grimes D, Schulz K, van Vliet H, Stanwood N. Immediate post-partum insertion of intrauterine devices. The Cochrane Database of Systematic Reviews 2003, Issue 1
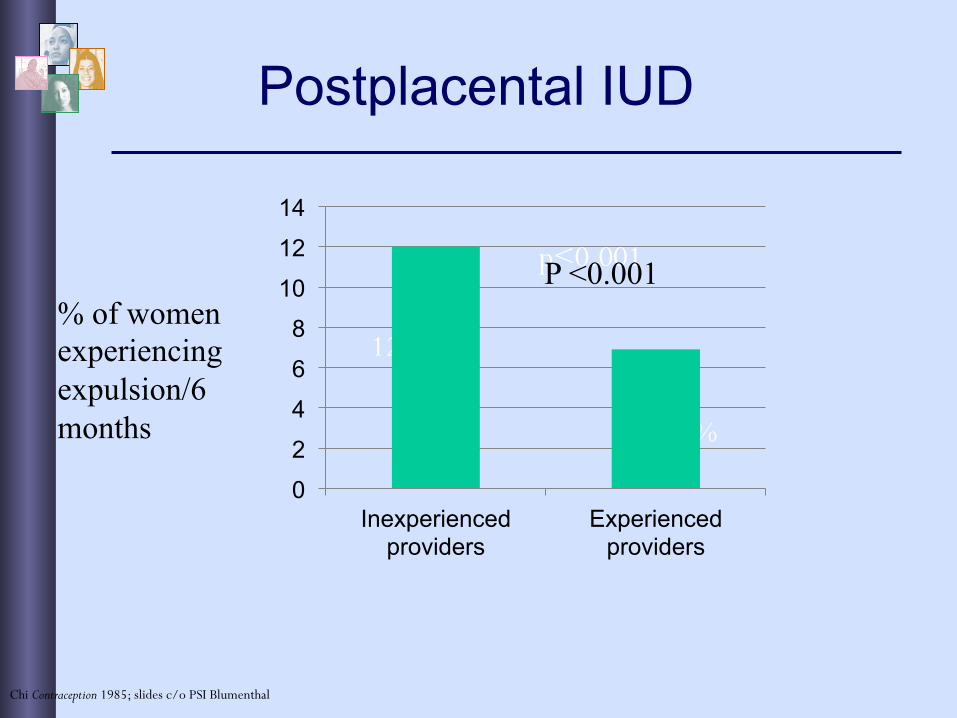
Postplacental IUD
6.9%
12.0%
p<0.001
Chi Contraception 1985; slides c/o PSI Blumenthal
0
2
4
6
8
10
12
14
Inexperienced providers
Experienced providers
% of women experiencing expulsion/6 months
P <0.001
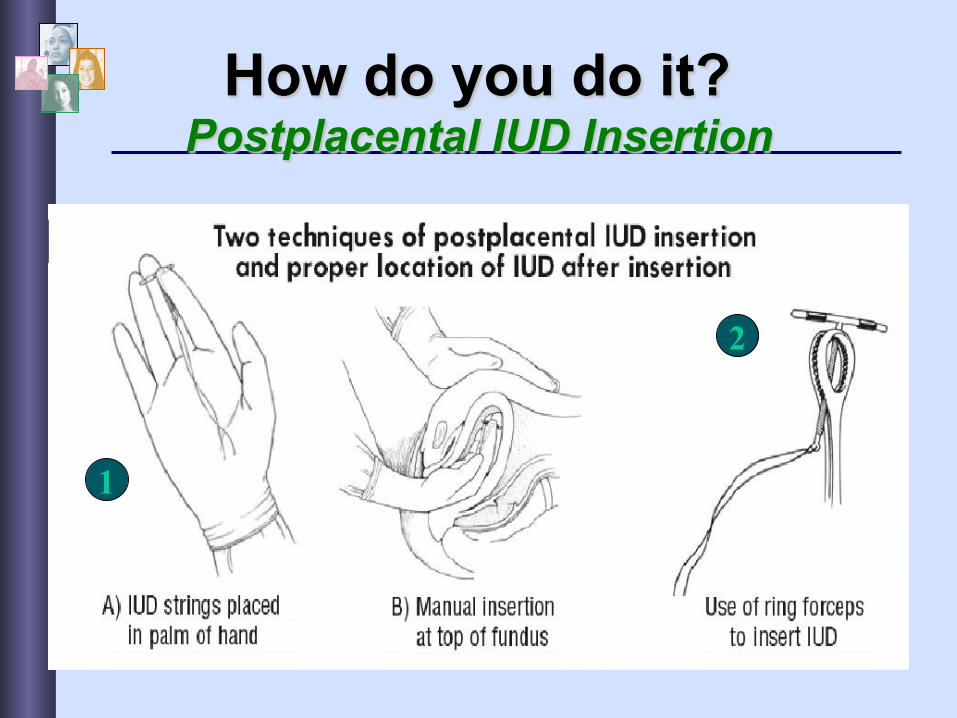
How do you do it? Postplacental IUD Insertion
2
1
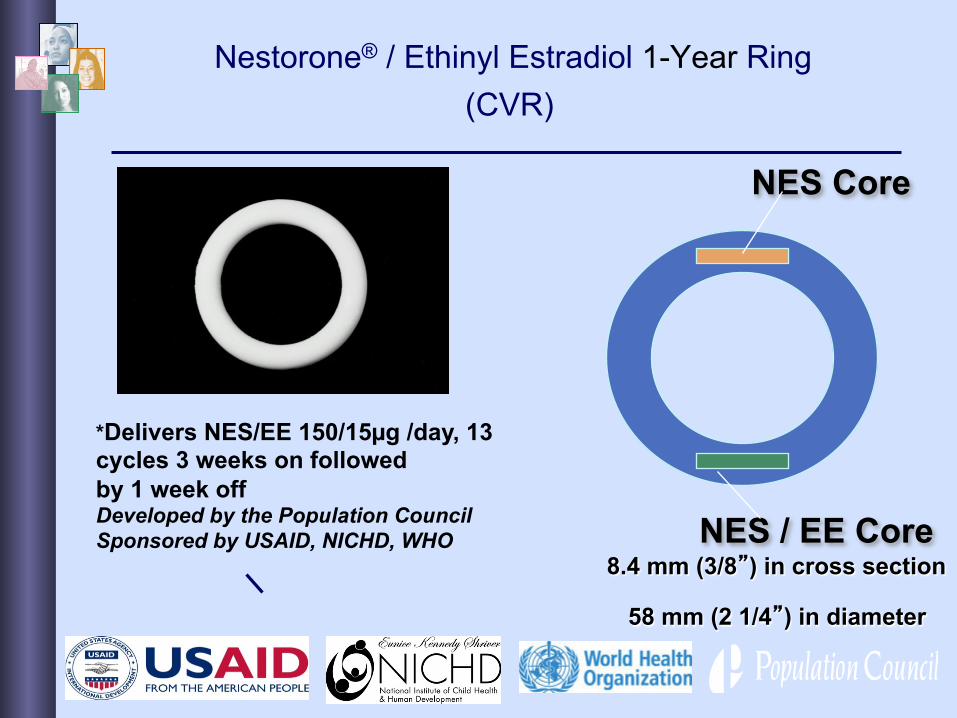
Nestorone® / Ethinyl Estradiol 1-Year Ring (CVR)
8.4 mm (3/8”) in cross section
58 mm (2 1/4”) in diameter
NES Core
NES / EE Core
*Delivers NES/EE 150/15µg /day, 13 cycles 3 weeks on followed by 1 week off Developed by the Population Council Sponsored by USAID, NICHD, WHO
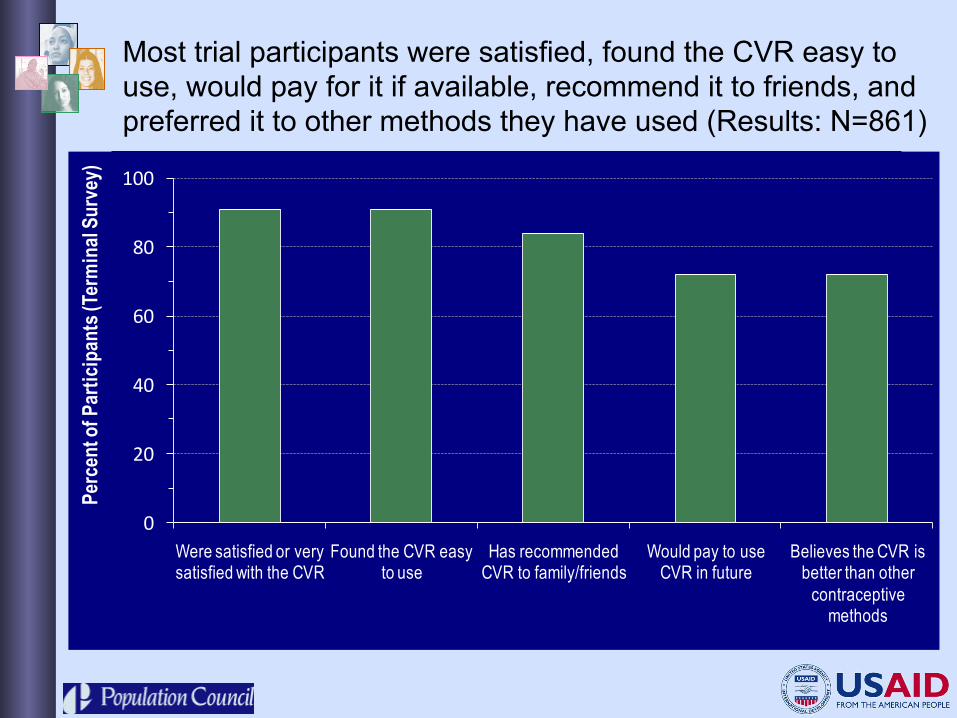
Most trial participants were satisfied, found the CVR easy to use, would pay for it if available, recommend it to friends, and preferred it to other methods they have used (Results: N=861)
0
20
40
60
80
100
Were satisfied or very satisfied with the CVR
Found the CVR easy to use
Has recommended CVR to family/friends
Would pay to use CVR in future
Believes the CVR is better than other
contraceptive methods
Perc
ent o
f Par
ticip
ants
(Ter
min
al Su
rvey
)
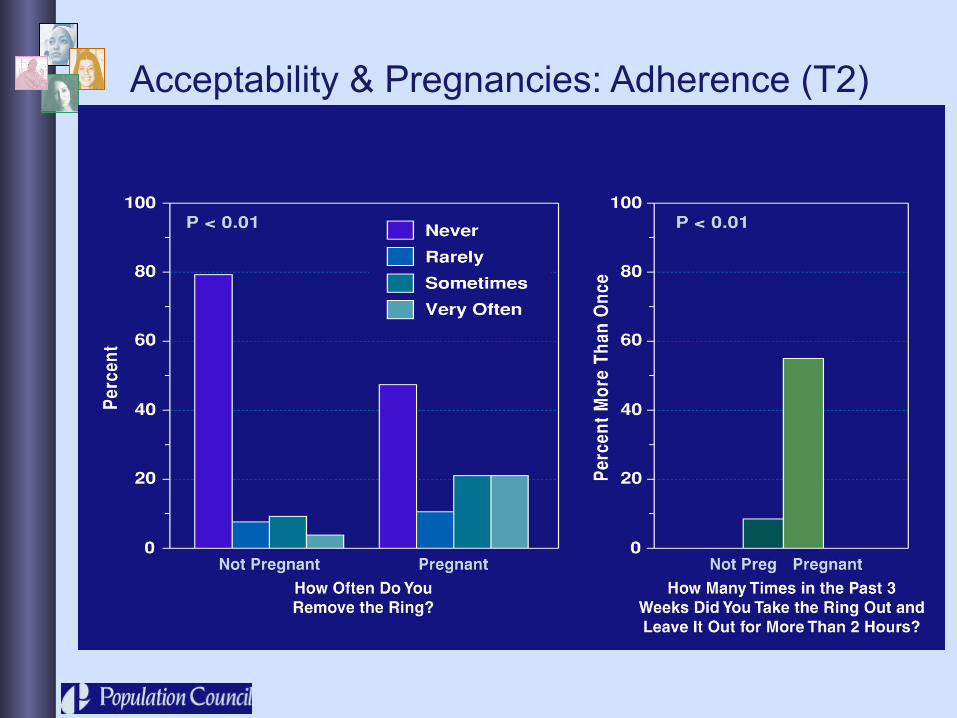
Acceptability & Pregnancies: Adherence (T2)
Injectables
l Advantages:
w Length of action
w Safety
w TASK-SHIFTING OPPORTUNITY
l Disadvantages:
w Continuation
w Side effects
DepoProvera®: Medroxyprogesterone acetate
l Given every 3 months
l Mechanism: w Suppresses ovulation
w Thickens cervical mucus
w Thins endometrium
l Intramuscular injection
New formulation of Depo-Provera: Depo-subQ Provera 104, for delivery with Uniject
Depo-subQ Provera 104: ▼ New formulation for subQ
injection ▼ 30% lower dose (104 mg vs.
150 mg) ▼ Rapid onset of action ▼ Same effectiveness, same
length of protection (>3 months)
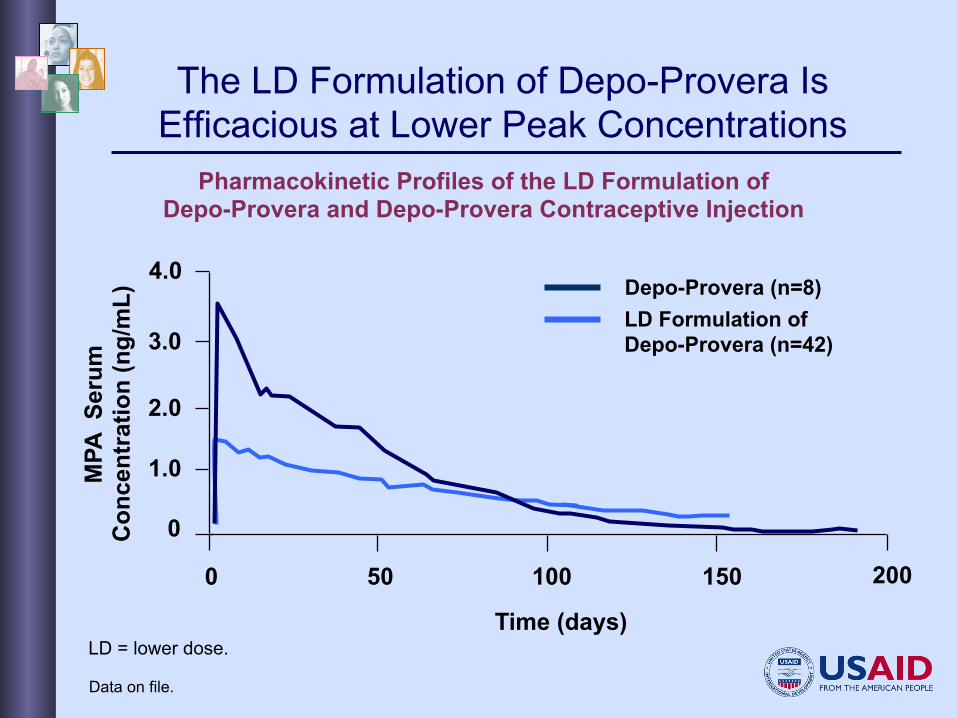
The LD Formulation of Depo-Provera Is Efficacious at Lower Peak Concentrations
Pharmacokinetic Profiles of the LD Formulation of Depo-Provera and Depo-Provera Contraceptive Injection
4.0
3.0
2.0
1.0
0
50 100 150 200 0
Depo-Provera (n=8) LD Formulation of Depo-Provera (n=42)
Time (days)
MPA
Ser
um
Con
cent
ratio
n (n
g/m
L)
Data on file.
LD = lower dose.
New formulation of Depo-Provera: Depo-subQ Provera 104, for delivery with Uniject
Uniject (Sayana Press): ▼ Single dose, single package ▼ Prefilled, sterile, non-reusable ▼ Short needles for subQ injection
(easier use by non-clinical personnel/CHWs)
▼ Compact; easy to use and store ▼ Potential for home- and self-
injection ▼ Approval by EMA and LDC
registration forthcoming
Emergency Contraceptive Pills
l SAFE l Mechanism: Primarily by delaying/ preventing ovulation
w Does not cause abortion
l Many brands available worldwide
l Repeated use is safe
l Less effective than “planned” BC
Trussell J, Jordan B. Contraception. 2006
l Pregnancy rates after levonorgestrel EC were 1.5 – 3%
l EC can be taken up to 72 (or 120) hours after intercourse, but effectiveness decreases with time. WHY? w Related to mechanism of action…
l Sperm can survive for several days
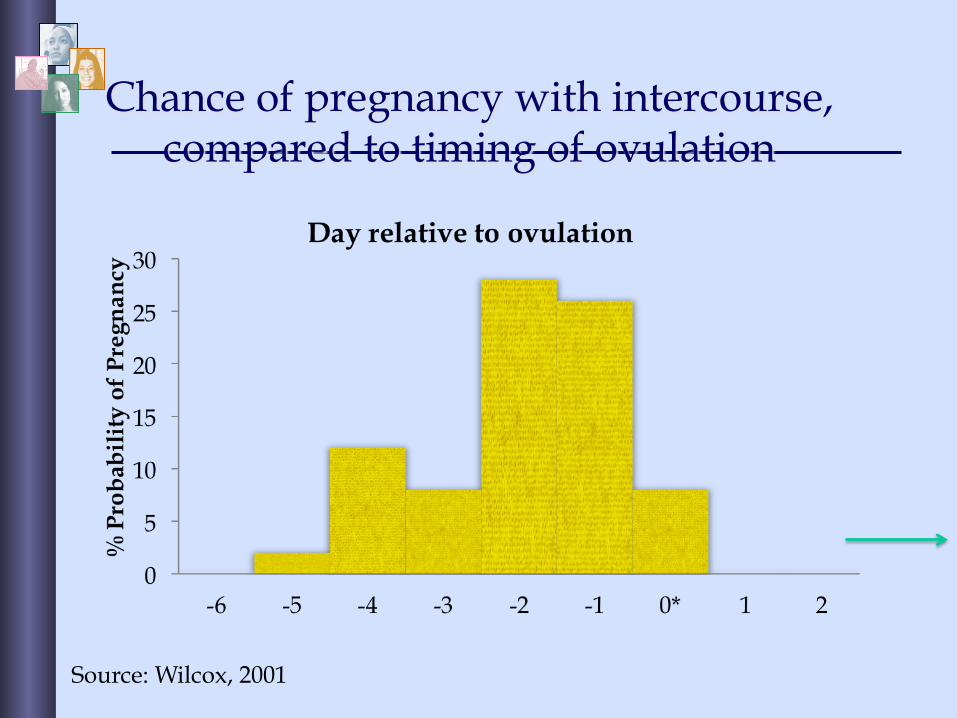
Chance of pregnancy with intercourse, compared to timing of ovulation
Source: Wilcox, 2001
l Antiprogestin, similar to mifepristone w Dose = 30mg
l Blocks ovulation
l May also have endometrial effects
l Does not cause abortion
l More effective than LNG for EC w Does not lose effectiveness with delay
w Lower pregnancy rates in the studies
Ulipristal for EC
page 32
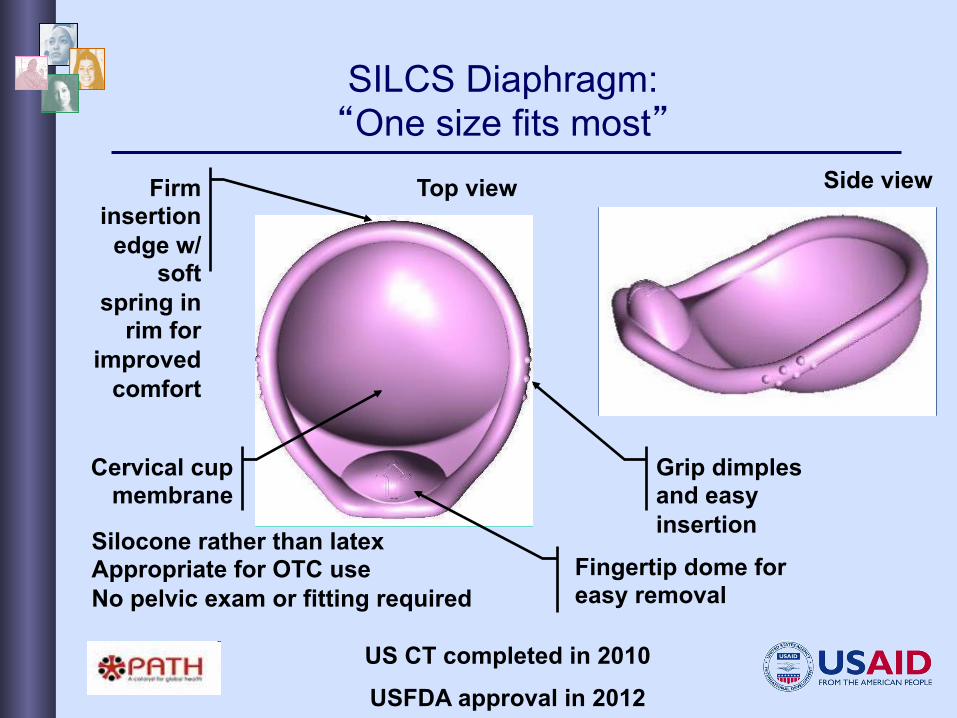
SILCS Diaphragm: “One size fits most”
Firm insertion edge w/
soft spring in
rim for improved
comfort
Grip dimples and easy insertion
Cervical cup membrane
Fingertip dome for easy removal
Side view Top view
Silocone rather than latex Appropriate for OTC use No pelvic exam or fitting required
US CT completed in 2010
USFDA approval in 2012
Woman’s Condom
• Easy to handle/use, insert and remove
• Stable during use • Comfortable for
both partners
• Less expensive than current options
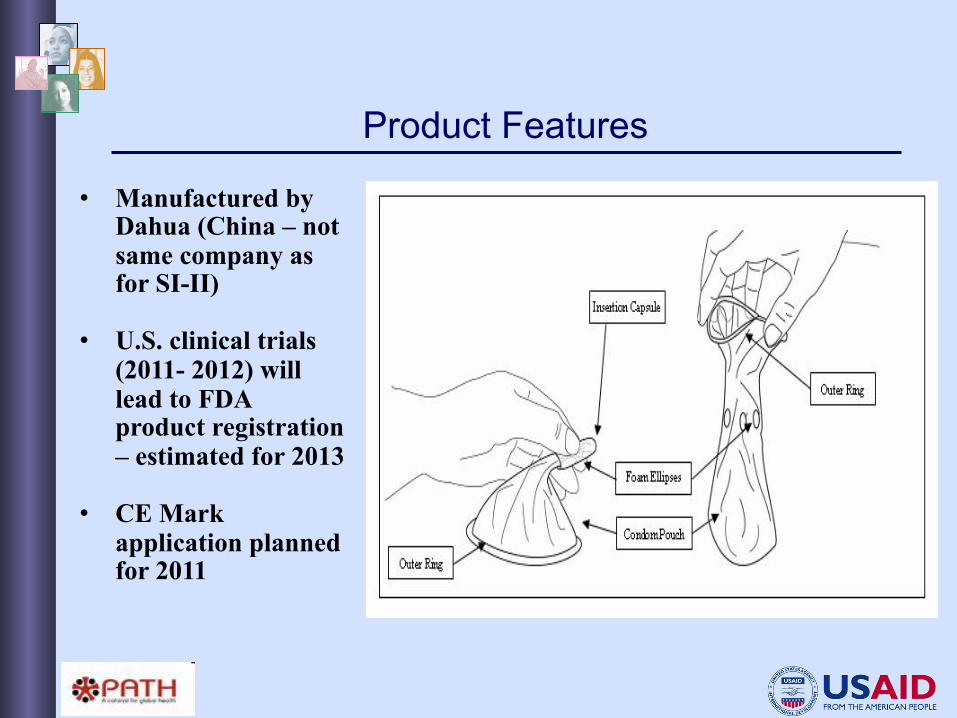
Product Features
• Manufactured by Dahua (China – not same company as for SI-II)
• U.S. clinical trials (2011- 2012) will lead to FDA product registration – estimated for 2013
• CE Mark application planned for 2011
New Contraceptive Methods Needed
1. Non-hormonal, non-steroidal or non-estrogen or novel progestin-only oral contraceptives
2. Biodegradable progestin-only implants (APS)
3. Non-surgical methods of male and female sterilization
4. Novel multi-purpose/dual protection methods (APS)
5. Peri-coital contraception
Spermicides – works in progress
l Highly effective?
l No vaginal irritation?
l Trials ongoing:
Amphora Gel (Evofem)
• Water-based gel • Acidiform • Hormone-free • Trials ongoing
2
“On demand” products: ü Used before/after intercourse ü Appropriate for women who have
infrequent sex, or who would like more direct control over their own protection
Priorities for product R&D:
Other MPT-related activities: Clarifying the Regulatory Approval of MPTs v Review existing guidance on combination products
from Regulatory Authorities (RAs)
v Convene technical meetings with RAs and WHO to discuss approval pathways for MPTs
Initiative for MPTs v Expand international awareness and support
for MPTs v Convene technical meetings to advance late-
stage product development and introduction
Sustained release devices: ü User-initiated, but do not require
daily action ü Should increase acceptability and
adherence, and therefore overall effectiveness
USAID support for MPTs:
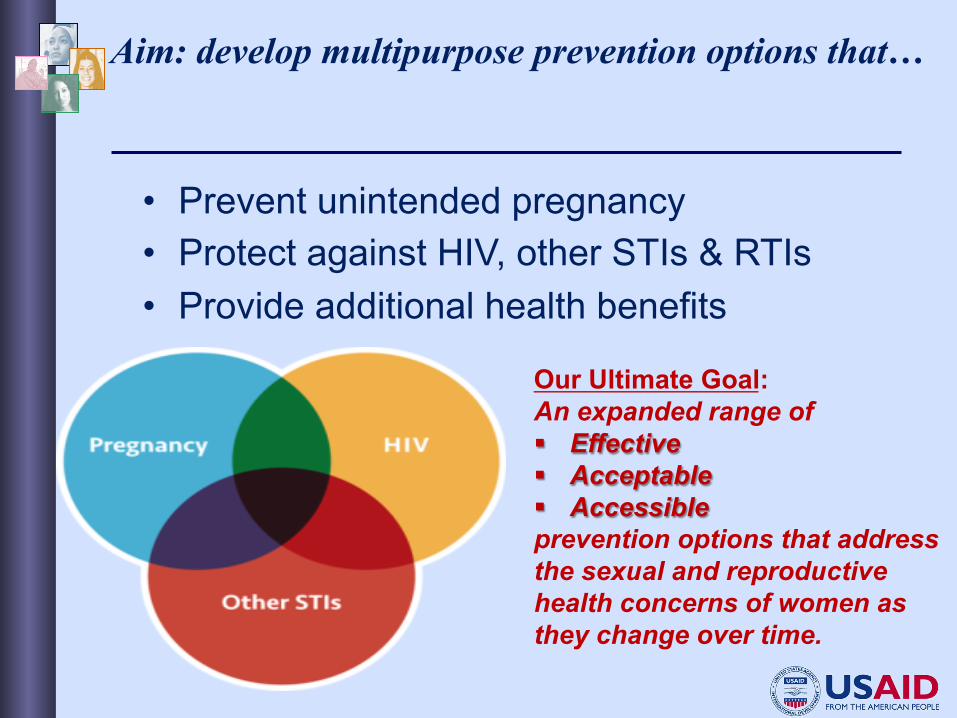
• Prevent unintended pregnancy • Protect against HIV, other STIs & RTIs • Provide additional health benefits
Our Ultimate Goal: An expanded range of § Effective § Acceptable § Accessible prevention options that address the sexual and reproductive health concerns of women as they change over time.
Aim: develop multipurpose prevention options that…
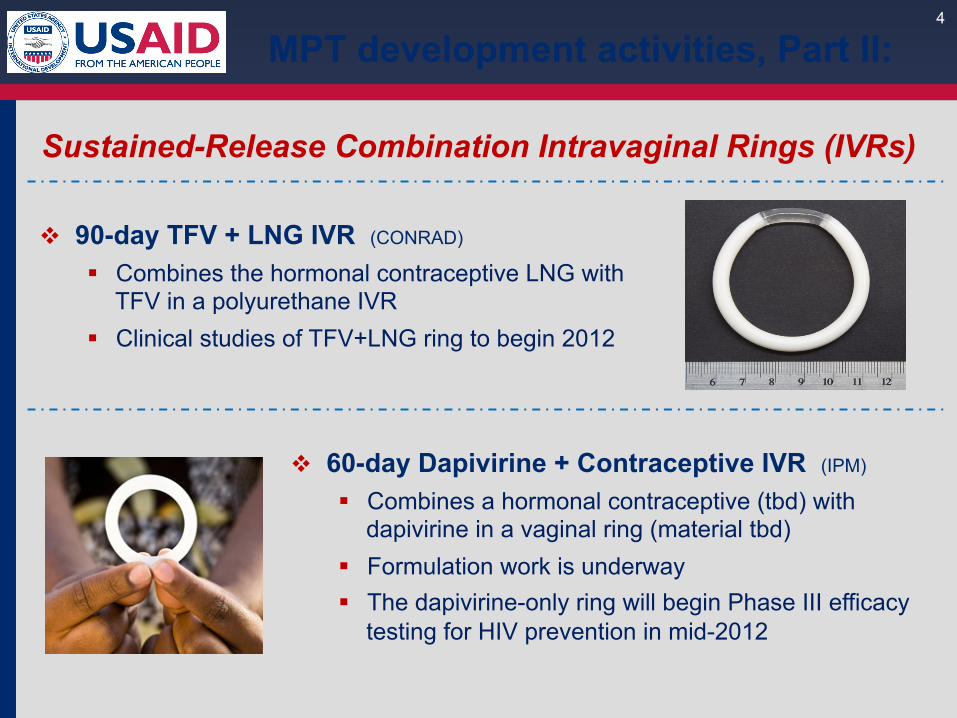
Sustained-Release Combination Intravaginal Rings (IVRs)
4
v 90-day TFV + LNG IVR (CONRAD)
§ Combines the hormonal contraceptive LNG with TFV in a polyurethane IVR
§ Clinical studies of TFV+LNG ring to begin 2012
v 60-day Dapivirine + Contraceptive IVR (IPM)
§ Combines a hormonal contraceptive (tbd) with dapivirine in a vaginal ring (material tbd)
§ Formulation work is underway § The dapivirine-only ring will begin Phase III efficacy
testing for HIV prevention in mid-2012
MPT development activities, Part II:
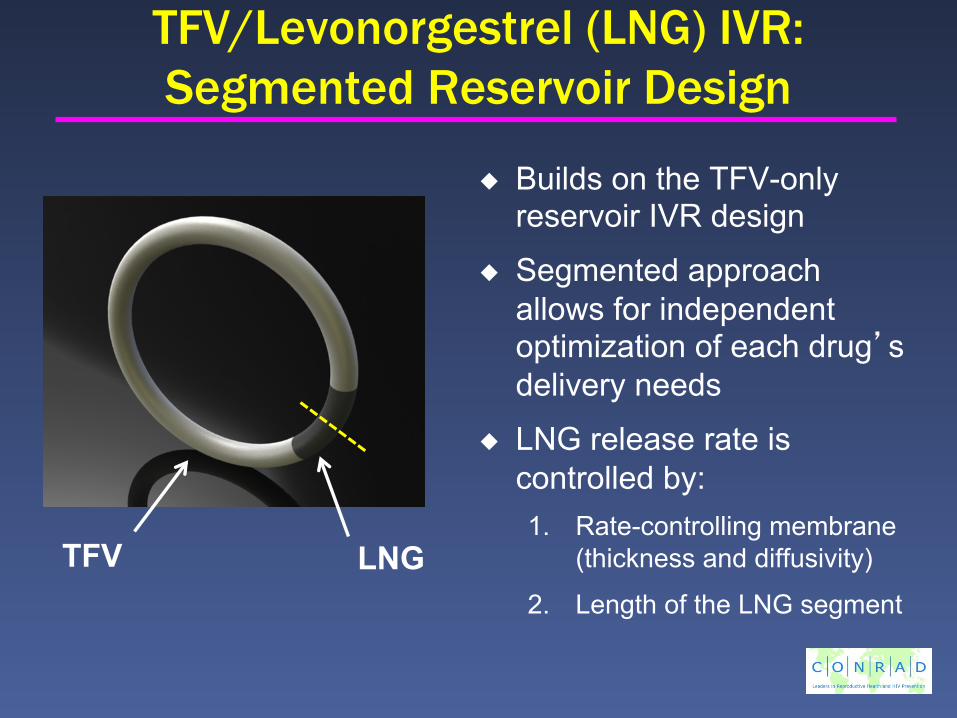
TFV/Levonorgestrel (LNG) IVR: Segmented Reservoir Design
Builds on the TFV-only reservoir IVR design
Segmented approach allows for independent optimization of each drug’s delivery needs
LNG release rate is controlled by: 1. Rate-controlling membrane
(thickness and diffusivity)
2. Length of the LNG segment
TFV LNG
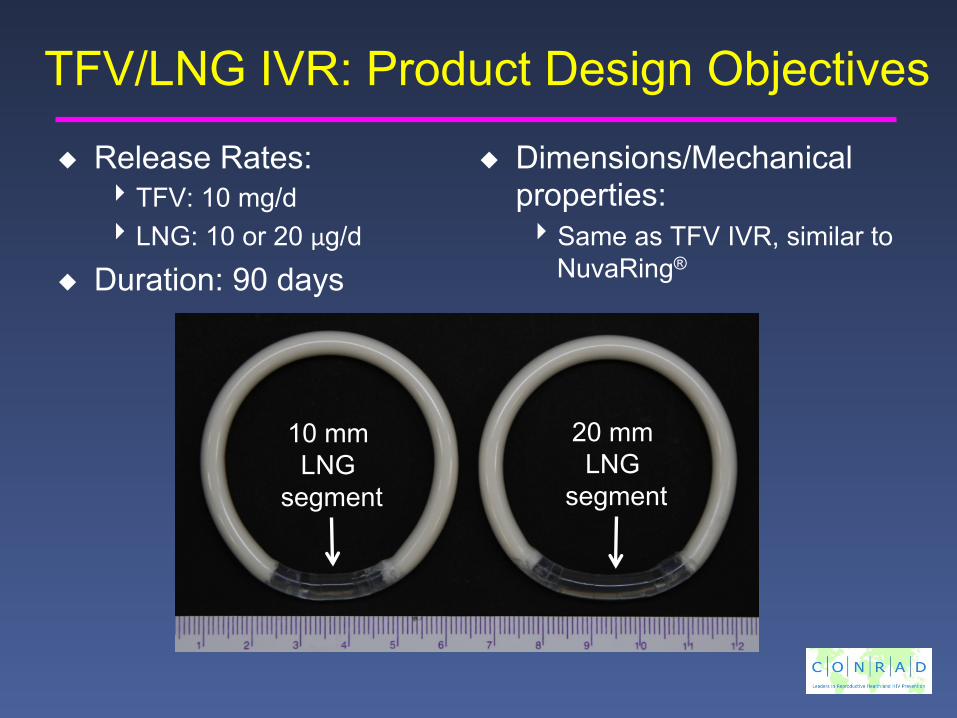
TFV/LNG IVR: Product Design Objectives
Release Rates: 4 TFV: 10 mg/d 4 LNG: 10 or 20 µg/d
Duration: 90 days
Dimensions/Mechanical properties: 4 Same as TFV IVR, similar to
NuvaRing®
20 mm LNG
segment
10 mm LNG
segment
3
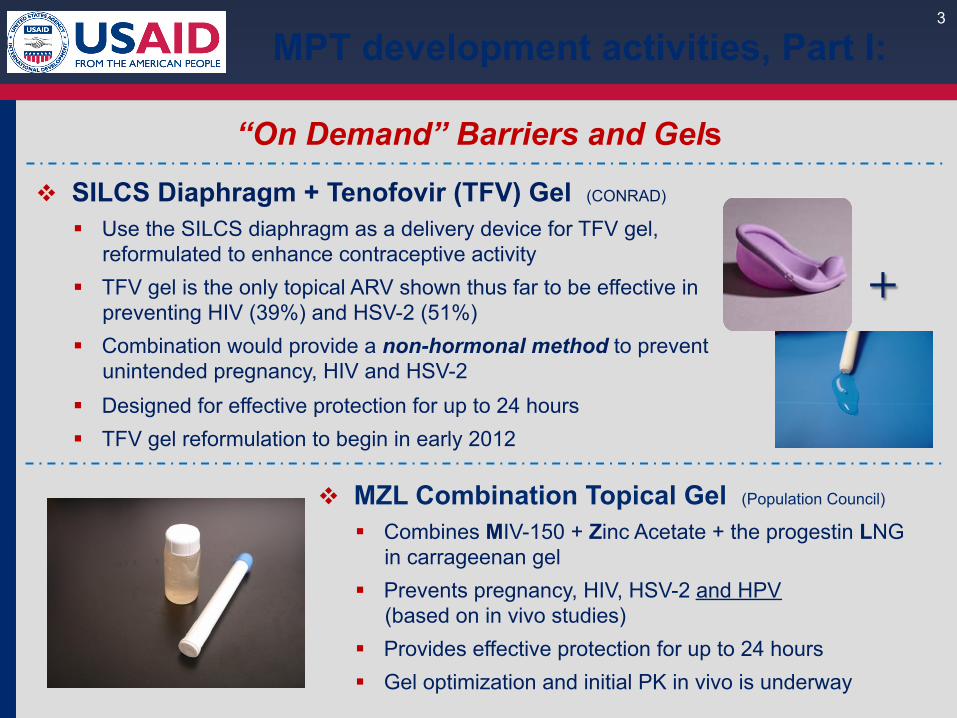
v MZL Combination Topical Gel (Population Council)
§ Combines MIV-150 + Zinc Acetate + the progestin LNG in carrageenan gel
§ Prevents pregnancy, HIV, HSV-2 and HPV (based on in vivo studies) § Provides effective protection for up to 24 hours § Gel optimization and initial PK in vivo is underway
v SILCS Diaphragm + Tenofovir (TFV) Gel (CONRAD)
§ Use the SILCS diaphragm as a delivery device for TFV gel, reformulated to enhance contraceptive activity
§ TFV gel is the only topical ARV shown thus far to be effective in preventing HIV (39%) and HSV-2 (51%)
§ Combination would provide a non-hormonal method to prevent unintended pregnancy, HIV and HSV-2
§ Designed for effective protection for up to 24 hours § TFV gel reformulation to begin in early 2012
“On Demand” Barriers and Gels
+
MPT development activities, Part I:
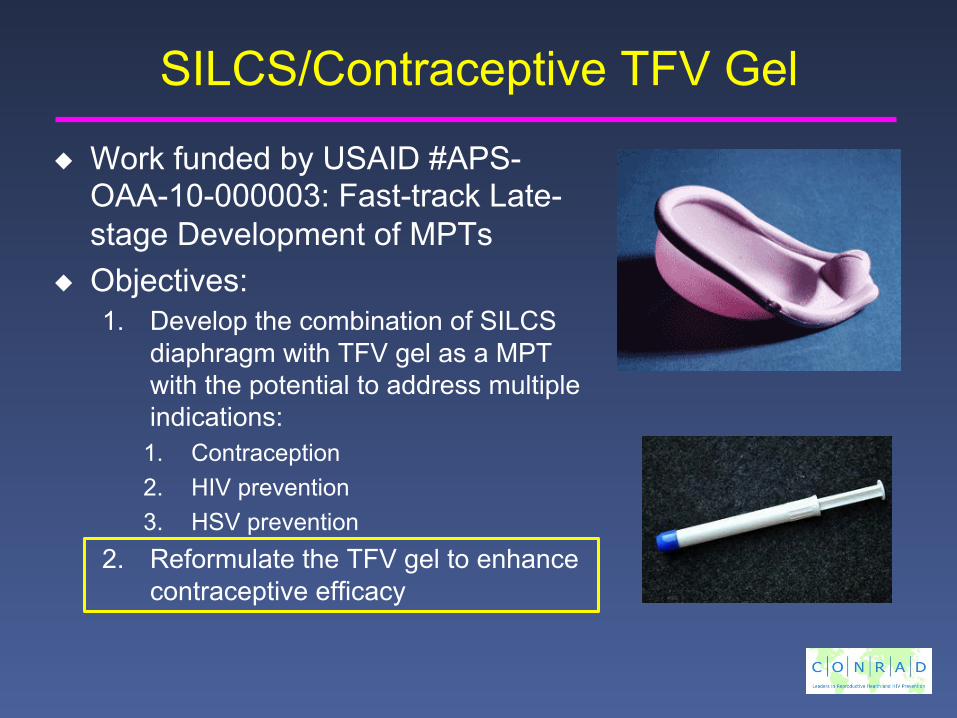
SILCS/Contraceptive TFV Gel
Work funded by USAID #APS-OAA-10-000003: Fast-track Late-stage Development of MPTs
Objectives: 1. Develop the combination of SILCS
diaphragm with TFV gel as a MPT with the potential to address multiple indications: 1. Contraception 2. HIV prevention 3. HSV prevention
2. Reformulate the TFV gel to enhance contraceptive efficacy
5
Conclusion: first-generation MPTs
Ø These MPT products in development could simultaneously prevent pregnancy, HIV, HSV-2, and HPV.
Ø Diversifying delivery & dosing options is KEY to meeting the different needs of women, and thereby expanding acceptability and use: § MZL gel: ideal method for women who would like a product they could
use “on demand”, and that lasts up to 24 hours
§ SILCS+TFV gel: ideal method for women who would like a non-hormonal contraceptive product that they control, especially for intermittent sex
§ Combination IVR (TFV+LNG or DAP+HC): ideal method for women who would like a highly effective product that requires minimal user involvement, and that provides continuous protection for 1-3 months
Our Aim: Expand the range of safe, effective and acceptable prevention options that meet different needs,
and are appropriate for delivery and use in low resource settings