Contents Appropriate Number of Definitive Drug Classes to ... · Appropriate Number of Definitive...
29
Appropriate Number of Definitive Drug Classes to Test in Outpatient Settings 3405 W Dr. Martin Luther King Jr. Blvd. Suite 200 Tampa, FL 33607 avalon-[email protected] https://www.avalonhcs.com/ Contents How many different definitive drug classes should be tested? Drug Use in the United States Trends in Prescriptions of Opioids in the U.S. Definitive Drug Testing What is the average number of drug classes prescribed per individual for which definitive testing would be indicated? What proportion of definitive urine drug tests rendered by providers consists of more than 7 drug classes? Guidelines References Appendices
Transcript of Contents Appropriate Number of Definitive Drug Classes to ... · Appropriate Number of Definitive...

Appropriate Number
of Definitive Drug
Classes to Test in
Outpatient Settings
3405 W Dr. Martin Luther King Jr. Blvd.
Suite 200 Tampa, FL 33607
[email protected] https://www.avalonhcs.com/
Contents
How many different definitive drug
classes should be tested?
Drug Use in the United States
Trends in Prescriptions of Opioids in the
U.S.
Definitive Drug Testing
What is the average number of drug
classes prescribed per individual for
which definitive testing would be
indicated?
What proportion of definitive urine
drug tests rendered by providers
consists of more than 7 drug classes?
Guidelines
References
Appendices

©2019 Copyright of Avalon Health Services, LLC. All rights reserved
Appropriate Number of Definitive Drug Classes to Test in Outpatient Settings Page 2 of 29
How many different drug classes should be tested definitively?
Urine drug testing (UDT) is an important patient monitoring tool designed to help with monitoring
prescription opioid therapy, screening for illicit drug use, and monitoring compliance with treatment
programs. Historically commonly abused drugs are known as SAMHSA-5, a group targeted in
federally regulated testing programs, including amphetamines, cannabinoids, cocaine, opiates, and
phencyclidine (PCP). Additional categories that may be screened for according to SAMHSA’s
(Substance Abuse and Mental Health Services Administration) website include benzodiazepines,
alcohol, opioids, and MDMA. Several national and state guidelines also exist to assist physicians with
prescribing and monitoring opioids. Often, such guidelines recommend that a presumptive urine
drug screen be performed first, and then, based on the results of the presumptive tests, additional
definitive urine drug testing should be performed to confirm the results of the screening results. Not
every presumptive urine drug test result needs to be confirmed since confirmation is needed only in
the face of unexpected screening results. In the specific case of chronic opioid therapy monitoring,
urine drug testing is just one of the available tools for patient management available to clinicians;
generally, urine drug testing results must be used in conjunction with professional judgement and
other opioid risk assessment tools (eg. Screener and Opioid Assessment for Patients in Pain, a 24-
item tool).
How large a panel of drugs to test for in
assessing a patient is a commonly asked
question. Use of too small a panel risks
missing clinically important exposures to
dangerous substances, yet too large a
panel leads to great unnecessary
expense, collection of information that is
not actionable, and other pitfalls
associated with over-testing, such as an
increasing risk of false-positive results.
Clearly, assessment of the more than one
thousand FDA-approved drugs or the
millions of known distinct chemical
entities is excessive, but less guidance
points one towards the correct number to
screen or confirm in any specific patient.
Basic clinical judgment, in combination with data from studies assessing patterns of abuse and
misuse, must therefore be employed in arriving at an answer to the question of the optimal size of
drug testing panels.
Use of too small a panel risks missing
clinically important exposures to
dangerous substances, yet too large a
panel leads to great unnecessary
expense, collection of information that is
not actionable, and other pitfalls
associated with over-testing, such as an
increasing risk of false-positive results.

©2019 Copyright of Avalon Health Services, LLC. All rights reserved
Appropriate Number of Definitive Drug Classes to Test in Outpatient Settings Page 3 of 29
Overall, in the clinical approach to assessing
potential misuse or abuse of substances,
barring specific medical/prescription
information about an individual patient, it is
highly unlikely that clinicians would need to
assess the presence or concentrations of more
than 7 different drug classes in their patients,
for three main reasons. First, very few patients
are prescribed more than 4 drug classes
simultaneously that require monitoring, such as
opioids. Second, patients tend to abuse or
misuse those drug classes with which they have
prior experience, addiction or dependence,
such as opiates or stimulants. Third and finally,
Bayesian interpretation of screening results
dictates that only those screening results that conflict with the initial clinical impression should be
confirmed with definitive testing. Thus, in a hypothetical patient who is being monitored during a
course of office-based opioid replacement therapy with buprenorphine, it would be most clinically
sound and efficient to screen for SAMHSA-5 drugs as well as relevant opioids, and only to confirm
with definitive testing those screening results that were unexpected; as the likely unexpected
findings would be opioids, benzodiazepines or
stimulants in these patients, definitive testing
confirmation of more than two or three drugs
would be rare, and certainly definitive testing
confirmation of more than 7 drug classes would be
difficult to support on clinical grounds. Very large
panels of definitive drug tests performed without
any prior screening tests are likewise lacking in a
clinical rationale, and there is a paucity of data
supporting such panels’ clinical superiority over
standard sequential screening-confirmation
strategies. Similar logic applies to testing for drugs
of abuse in the other clinical situations outlined
above, and it is for this reason that definitive
testing for over 7 drug classes in a single setting
does not meet criteria for medical necessity.
Drug Use in the United States
According to the 2016 National Survey on Drug Use and Health (NSDUH), as many as 28.6 million
Americans 12 or older used an illicit drug in the last 30 days, which corresponds to 10.6% of
Americans overall and 25% for young adults from 18 to 25. The 2016 NSDUH also states that 11.8
million misused opioids in the previous year, with 11.5 million misusing prescription pain relievers.
Approximately 8.2 million adults had a concurrent mental illness and substance abuse disorder in
the previous year (SAMHSA, 2017). A drug of abuse (DOA) may be defined as “a drug, chemical, or
plant product that is known to be misused for recreational purposes”, which can include drugs, such
It is highly unlikely that clinicians
would need to assess the
presence or concentrations of
more than 7 different drug
classes in their patients.
Large drug panel screening lacks
clinical superiority over standard
sequential screening-
confirmation strategies.

©2019 Copyright of Avalon Health Services, LLC. All rights reserved
Appropriate Number of Definitive Drug Classes to Test in Outpatient Settings Page 4 of 29
as pain relievers, that have legitimate prescriptions.
Drug testing may be performed for several reasons.
For example, patients in certain areas, including
pain management, substance abuse treatment, and
psychiatric treatment, have a higher propensity for
substance abuse and must be monitored as such
(Hoffman, 2018).
According to the CDC, in 2016, a 21.5% increase in
the number of age-adjusted rate of drug overdose
deaths occurred, and 66.4% of all drug overdose
deaths involved the use of opioids (CDC, 2017a).
The CDC monitors the number of deaths and
nonfatal overdoses of opioids in four categories
(CDC, 2017b):
Natural/semi-synthetic opioids, such as
morphine and oxycodone, respectively
Methadone
Synthetic opioids other than methadone
Heroin
Trends in Prescriptions of Opioids in the U.S.
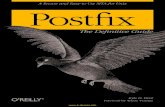
The overall trend in annual opioid prescribing rates have been falling from the peak in 2012 of 81.3
prescriptions per 100 persons to 58.5 in the most recently reported year (2017) (CDC, 2017c).
Appendix A contains the map showing the relative rate of prescriptions of opioids by state in 2017
with the highest rate (107.2 per 100
persons) reported in Alabama and the
lowest rate in the District of Columbia
(28.5 per 100 persons) (CDC, 2017e). The
rate of prescriptions, however, does not
reflect the relative rate of reported deaths;
for example, Alabama reported an age-
adjusted rate of 16.2 deaths per 100,000
whereas the District of Columbia had a
significantly higher rate of 38.8 deaths per
100,000 (CDC, 2017a). Appendix B
contains the map of the U.S. with the age-
adjusted rate of drug overdose by state in
2017 as reported by the CDC (CDC, 2017a,
2018).
DOA screening varies in composition
between countries. In the U.S., the typical
DOA screening tests for amphetamine,
cocaine, marijuana/tetrahydrocannabinol
2016 NSDUH
25% of Americans 18-25
years old used an illicit substance
within the past 30 days
50
55
60
65
70
75
80
85
2006 2008 2010 2012 2014 2016
Opioid Prescriptions in the United StatesData from the 2018 CDC Annual Surveillance Report
of Drug-Related Risks and Outcomes
Year

©2019 Copyright of Avalon Health Services, LLC. All rights reserved
Appropriate Number of Definitive Drug Classes to Test in Outpatient Settings Page 5 of 29
(THC), opioids, and phencyclidine (PCP) as included in the United States’ Drug-Free Workplace Act of
1988; these DOA are often referred as the SAMHSA 5, named after the Substance Abuse and Mental
Health Services Administration (Hoffman, 2018; Phan, Yoshizuka, Murry, & Perry, 2012). Although
drug use trends have changed dramatically since 1988, these five have remained on the basic drug
screen used across the U.S. The U.S. Department of Defense (DOD) removed PCP from its routine
screening but added benzodiazepines, amphetamine derivatives, common barbiturates, synthetic
and semisynthetic opioids, lysergic acid diethylamide (LSD), and synthetic cannabinoids. Other
countries or regions, such as Australia and the European Union, also include testing for
benzodiazepines and a wider range of opioids (Hoffman, 2018).
Definitive Drug Testing
Drug testing can be described as qualitative, semi-quantitative or quantitative, and can also be
described as presumptive or definitive. Qualitative refers to testing for the presence of a given
analyte, semi-quantitative reports if the analyte is present above or below a certain threshold or set
of thresholds, and quantitative testing reports the concentration of an analyte (drug) numerically.
Presumptive drug testing is used to identify use or non-use of a drug or a drug class, but this type of
testing cannot distinguish between closely related chemicals or structural isomers, and as it is
usually based on immunoassay, it is subject to the normal interferences that affect immunoassays.
Definitive drug testing usually refers to a more definitive methodology, such as mass spectrometry
or chromatography, and most often the combination of chromatography and mass spectrometry,
because these methods can identify use or non-use of a specific drug and/or its associated
metabolites. Both types of drug testing can be either quantitative or qualitative (Jannetto &
Langman, 2018). The frequency of testing is ultimately up to the ordering provider; testing may be
random or scheduled depending on the provider’s objectives (Becker & Starrels, 2018).
Urine is the most common specimen type used in drug testing for several reasons. Unlike blood or
saliva, the window of detection of most drugs is longer in urine; moreover, urine tests are generally
inexpensive, noninvasive, and convenient to use while still maintaining acceptable statistical validity.
Salivary testing can provide a higher rate of false-negative results, especially for individuals who
smoke. Urine may provide more objective assessment of drug levels compared to purely clinical
evaluation or a patient self-report (Becker & Starrels, 2018). One disadvantage of urine testing is a
“risk of adulteration of the sample by the patient to avoid detection of non-compliance with the
therapeutic regimen (AACC, 2017),” but there are analytical strategies that can be employed to
detect such adulteration.
Even though single-site studies have shown the potential positive impact of direct-to-definitive drug
testing for monitoring compliance in pain management by decreasing the number of false-positive
results (Gencheva et al., 2018), the current standard of care approach in most circumstances is to
initially perform a presumptive drug screen followed by a definitive drug test of any positive results
(Hadland & Levy, 2016). Mandatory guidelines for federal workplace drug testing using urine
samples also establishes initial screening for the SAMHSA drugs, and in 2017 they removed MDEA
from the authorized drugs and added MDA as an initial test analyte. In section 3.4 of the mandate,
they list the following as initial analytes (with the initial test cutoff values given in parentheses):
marijuana metabolites (50 ng/mL)
cocaine (150 ng/mL)
codeine/morphine (2,000 ng/mL)

©2019 Copyright of Avalon Health Services, LLC. All rights reserved
Appropriate Number of Definitive Drug Classes to Test in Outpatient Settings Page 6 of 29
hydrocodone/hydromorphone (300 ng/mL)
oxycodone/oxymorphone (100 ng/mL)
6-acetylmorphine (10 ng/mL)
phencyclidine (25 ng/mL)
amphetamine/methamphetamine (500 ng/mL)
MDMA/MDA (500 ng/mL)
Again, positive initial screens are to be followed by definitive drug testing (HHS, 2017). However,
higher cutoff values may not truly indicate compliance in patients. One study shows “wide variation
in the false-negative rate, ranging from 1.5% to 94.3% across a range of prescribed and illicit drugs
(Krock et al., 2017).”
The Centers for Medicare & Medicaid Services (CMS) in 2018 issued a statement reminding
laboratories and other providers to use correct coding for drug testing and screening. For
presumptive drug testing, codes 80305, 80306, and 80307 must be used; however, as part of the
National Correct Coding Initiative (effective January 1, 2016), HCPCS codes G0480-G0483 must be
used for definitive drug testing with only one code being allowed per date of service. G0480 is
defined as:
“Drug test(s), definitive, utilizing (1) drug identification methods able to identify
individual drugs and distinguish between structural isomers (but not necessarily
stereoisomers), including, but not limited to GC/MS (any type, single or tandem) and
LC/MS (any type, single or tandem and excluding immunoassays (e.g., IA, EIA, ELISA,
EMIT, FPIA) and enzymatic methods (e.g., alcohol dehydrogenase)), (2) stable isotope or
other universally recognized internal standards in all samples (e.g., to control for matrix
effects, interferences and variations in signal strength), and (3) method or drug-specific
calibration and matrix-matched quality control material (e.g., to control for instrument
variations and mass spectral drift); qualitative or quantitative, all sources, includes
specimen validity testing, per day; 1-7 drug class(es), including metabolite(s) if
performed (CMS, 2018)”.
The CMS definitive drug testing codes G0480 – G0483 are summarized below in Table 1:
Table 1: CMS Definitive Drug Test Codes
CMS definitive drug testing code Number of drug classes tested
G0480 1 - 7
G0481 8 - 14
G0482 15 - 21
G0483 22 or more

©2019 Copyright of Avalon Health Services, LLC. All rights reserved
Appropriate Number of Definitive Drug Classes to Test in Outpatient Settings Page 7 of 29
CMS also requires that the billing codes used are based on medical necessity. They state that
medical necessity documents “may include clinical evaluations, physician evaluations, consultations,
progress notes, physician’s office records, hospital records, nursing home records, home health
agency records, records from other healthcare professionals and test reports. It is maintained by the
physician and/or provider (CMS, 2012).” CMS also reiterates the importance of medical necessity
and notes that reimbursement documentation can often be inadequate in justifying necessity.
“Physician/LCMPs [licensed/certified medical professional] should be aware that
templates designed to gather selected information focused primarily for reimbursement
purposes are often insufficient to demonstrate that all coverage and coding
requirements are met. This is often because these documents generally do not provide
sufficient information to adequately show that the medical necessity criteria for the
item/service are met… Certificates of Medical Necessity (CMN), DME Information Forms
(DIF), supplier prepared statements and physician attestations by themselves do NOT
provide sufficient documentation of medical necessity, even if signed by the signed by
the ordering physician (CMS, 2019).”
The CMS also states that the physician/LCMP, when ordering a service from an outside entity, is
required to provide “adequate documentation supporting medical necessity” to the outside facility
at the time the item or service is ordered. Failure to do so can result in a review of the physician or
LCMP (CMS, 2019).
A report by Kaiser Health News (KHN) and Mayo Clinic reviewing the billing data from 2011 to 2014
shows that the federal government “paid providers more to conduct urine drug tests in 2014 than it
spent on the four most recommended cancer screenings combined.” The researchers estimated the
yearly cost to private insurers and Medicare Advantage to be approximately $8.5 billion from 2011
to 2014—more than the annual budget of the Environmental Protection Agency—based on data
from Medicare’s fee-for-service program, the CMS’ Beneficiary Public Use File, and the Current
Population Survey of the U.S. Census (Schulte & Lucas, 2017).
What is the average number of drug classes prescribed per
individual for which definitive testing would be indicated?
To address this question, the records of individuals (n = 101137) within the 2015 calendar year from
a private insurance company were reviewed. The average number of drug classes (for which
definitive drug testing is applicable) prescribed per month per individual was calculated. These
definitive drug classes include drugs associated with a potential of abuse and/or associated with
definitive toxicology screening, such as amphetamines and opioids. For a list of the definitive drug
classes as defined by the AMA that are included in the calculation, please see Appendix C. The
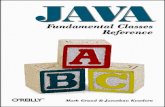
overall average number of drug classes per month per individual was 1.26, and the highest average
number of drug classes per month calculated for any single individual was 8.83. The graph in Figure
1 shows the distribution of the average number of drug classes per month for 2015 (note
logarithmic y-axis). The red bar in Figure 1 indicates 7 drug classes, the limit of drug testing as
covered by code G0480. Only 44 individuals (out of the more than 100,000 total) have monthly
averages greater than 7.0. The overall median number of drug classes prescribed monthly per
individual was 1. Table 2 lists the numerical values in greater detail. More than 50% of individuals

©2019 Copyright of Avalon Health Services, LLC. All rights reserved
Appropriate Number of Definitive Drug Classes to Test in Outpatient Settings Page 8 of 29
are prescribed no more than 1 drug
class per month on average of the
definitive drug classes as listed in
Appendix C. Please note that this
does not include prescription drugs
not regarded as a drug of abuse or
associated with a toxicology screen,
i.e. statins. Although there is no
direct correlation between the
number of drug classes prescribed
and the number of definitive drug
classes required to be tested per
patient, these data suggest that the
number of definitive drug classes
that needs to be tested is probably
not large. Even if an individual was
only prescribed suboxone
(buprenorphine), one single drug
class, they would still need
additional drug classes tested, but
the number of definitive drug classes
needed to be tested definitively
would be unlikely to exceed seven.
Table 2: Monthly Average Number of Definitive Drug
Classes per Individual
Average Monthly
Number of Drug
Classes
Number of Individuals Percent of Total
Number of
Individuals
0 – 1 55022 54.4%
1.1 – 2 26181 25.9%
2.1 – 3 11894 11.8%
3.1 – 4 5098 5.0%
4.1 – 5 2001 2.0%
5.1 – 6 708 0.7%
6.1 – 7 189 0.2%
7.1 – 8 37 0.04%
8.1 – 9 7 0.007%

©2019 Copyright of Avalon Health Services, LLC. All rights reserved
Appropriate Number of Definitive Drug Classes to Test in Outpatient Settings Page 9 of 29
What proportion of definitive urine drug tests rendered by
providers consists of more than 7 drug classes?
The data from two private insurers for the calendar year 2018 was examined to determine the total
number of units of G0480, G0481, G0482, and G0483 ordered. These data consist of all units of
service, including those that were denied coverage. So as to not skew the results, a rendering
provider must have provided a minimum number of 30 units of service to be included in the data
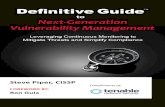
analysis. Figure 2 displays the usage of definitive drug testing for more than 7 drug classes on a
single order (i.e. panel testing) for each
rendering provider. The percent of
screens with more than 7 drug classes was
calculated by adding the number of units
of G0481, G0482, G0483 and dividing by
the total number of units for each
provider. The individual values ranged
from 0% (i.e. 100% G0480 only) to 98.6%
(or 1.4% of claims contained 7 or fewer
drug classes). The identities of the
individual laboratories have been withheld
and assigned a letter (A – T) based on
ascending order of noncompliance.
To determine if the usage of codes G0481
– G0483 is related to the total number of
tests performed by any particular
laboratory (i.e. is it possible that a
laboratory with minimal number of tests
has a higher proportion of panels with
more than 7 drug classes tested as
compared to a laboratory that renders a
large quantity of tests), the total number of units provided by each lab is provided for comparison in
Figure 3. Here, the lab providing the highest number of definitive drug screening tests (32607 units),
lab B within the figure, has the second-highest degree of usage of G0480 (only 0.5% of units
submitted were G0481 – G0483); however, the next highest lab provider, lab R (with 29943 units)
has the third highest percentage of panel screens with greater than 7 drug classes (69%). In fact,
this single lab comprised 68.7% of all units of G0481 – G0483 submitted by all labs combined (20531
units by lab R out of 29902 total units of G0481 – G0483). The next highest use of non-G0480 codes
ordered was by lab T with only 9.44%. All other labs with at least a minimum of 30 units of G0480 –
G0483 combined accounted for 21.9% as depicted in Figure 4. In summary, no correlation exists
between the number of units ordered and the rate of appropriately using the correct code for
definitive drug testing.

©2019 Copyright of Avalon Health Services, LLC. All rights reserved
Appropriate Number of Definitive Drug Classes to Test in Outpatient Settings Page 10 of 29
Conclusion
Urine drug testing is an important tool in monitoring
prescription opioid therapy, illicit drug use, and drug
abuse treatment compliance. In definitive drug
testing, the size of the toxicology panel is important
since a panel with too few analytes tested may
result in drugs missed and a panel with too many
analytes tested can result in over-testing and
possible false-positives. The CMS lists the G0480 –
G0483 coding series for definitive drug testing based
on the number of drug classes being tested rather

©2019 Copyright of Avalon Health Services, LLC. All rights reserved
Appropriate Number of Definitive Drug Classes to Test in Outpatient Settings Page 11 of 29
than by the testing methodology (i.e. immunoassays, spectroscopic assays, and so on). By reviewing
the records of more than 100,000 individuals over the course of a year, we determined the average
number of drug classes prescribed per individual per month. 99.96% of individuals were prescribed
7 drug classes or less on average (Figure 1), and the overall median number of drug classes
prescribed monthly is 1. These individuals fall within the scope of the G0480 code. These findings
do not preclude a two-tiered, sequential screening-confirmation strategy. The bulk (68.7%) of panel
tests containing more than 7 drug classes were rendered by a single laboratory (Figure 4). It appears
that large panels of definitive drug tests, using codes other than G0480, performed without any
prior screening tests are lacking in clinical rationale and that standard sequential screening-
confirmation strategies can be used to effectively monitor the patients in these populations.
Contact
The website for Avalon Healthcare Solutions is located at https://www.avalonhcs.com/. For
additional information, please contact Barry Davis, Avalon Chief Growth Officer, at
Guidelines
1. Centers for Disease Control and Prevention (CDC)
In the 2016 CDC guidelines, they recommend an evaluation of the benefits and harms of
continuing opioid-based therapy with the patient every three months or more
frequently; moreover, “for patients with opioid use disorder, clinicians should offer or
arrange evidence-based treatment, such as medication-assisted treatment with
buprenorphine or methadone (Dowell et al., 2016).”
Within the guidelines, the CDC recommends that clinicians should consider urine drug
testing prior to discontinuing opioids to determine possibility of withdrawal. The CDC
also recommends that “when prescribing opioids for chronic pain, clinicians should use
urine drug testing before starting opioid therapy and consider urine drug testing at least
annually to assess for prescribed medications as well as other controlled prescription
drugs and illicit drugs (recommendation category: B, evidence type: 4).” The CDC states
that “urine drug tests can provide information about drug use that is not reported by
the patient. In addition, urine drug tests can assist clinicians in identifying when patients
are not taking opioids prescribed for them, which might in some cases indicate diversion
or other clinically important issues such as difficulties with adverse effects (Dowell,
Haegerich, & Chou, 2016).”
Concerning the frequency of urine drug testing, they state, “While experts agreed that
clinicians should use urine drug testing before initiating opioid therapy for chronic pain,
they disagreed on how frequently urine drug testing should be conducted during long-
term opioid therapy. Most experts agreed that urine drug testing at least annually for all

©2019 Copyright of Avalon Health Services, LLC. All rights reserved
Appropriate Number of Definitive Drug Classes to Test in Outpatient Settings Page 12 of 29
patients was reasonable. Some experts noted that this interval might be too long in
some cases and too short in others, and that the follow-up interval should be left to the
discretion of the clinician. Previous guidelines have recommended more frequent urine
drug testing in patients thought to be at higher risk for substance use disorder.
However, experts thought that predicting risk prior to urine drug testing is challenging
and that currently available tools do not allow clinicians to reliably identify patients who
are at low risk for substance use disorder (Dowell et al., 2016).”
2. American Association in Clinical Chemistry (AACC)
AACC have published Laboratory Practice Guidelines: Using Clinical Laboratory Tests to
Monitor Drug Therapy in Pain Management in 2017. The main goal of their guidelines
was to provide evidence-based recommendations for the use of laboratory and point-of-
care (POC) urine drug tests for detection of drugs. AACC’s guidelines include 26
recommendations and 7 expert opinions.
AACC lists no recommendations for the frequency of testing but states that “more
frequent laboratory testing is recommended for patients with a personal or family
history of substance abuse, mental illness, evidence of aberrant behavior, or other high-
risk characteristics.” (Evidence A, II). Authors recommend using other tools available to
physicians in addition to urine drug screening for monitoring compliance. Urine drug
testing is recommended for detection of drugs in pain management patients (Evidence
B, II). POC qualitative presumptive tests offer similar performance characteristics to
laboratory-based immunoassays and therefore AACC recommends that physicians use
package inserts or consult laboratory personnel to accurately interpret lab results
(Evidence B, II). They recommend the use of qualitative immunoassays before
prescribing controlled substances to identify illicit drug use in pain management
patients (Evidence B, II). They also recommend confirming with definitive testing any
immunoassays that are not consistent with clinical presentation of the patient (A, III).
Although quantitative definitive urine testing is not more useful than qualitative
definitive testing, according to AACC there are advantages to use quantitative definitive
testing in certain situations such as: “…quantitative urine definitive testing is
recommended to identify variant drug metabolism, detect pharmaceutical impurities, or
metabolism through minor routes. Quantitative results may also be useful in complex
cases to determine the use of multiple opioids, confirm spiked samples, and/or rule out
other sources of exposure (e.g. morphine from poppy seeds) (AACC, 2017)” (Evidence A,
II).
AACC experts recommend ordering amphetamines, barbiturates, benzodiazepines,
cannabinoids, cocaine, opiates/opioids for a routine pain patient monitoring. They
suggest that additional substances could be tested for patients considered “high-risk
with known history of abuse for this medication prevalence of drug use is endemic to
local region, risky polypharmacy, multiple providers, or if prescribed and patient shows
lack of efficacy or toxicity”. Substances listed in this category include alcohol,
anticonvulsants, antidepressants, synthetic cathinones, antitussive, dissociative

©2019 Copyright of Avalon Health Services, LLC. All rights reserved
Appropriate Number of Definitive Drug Classes to Test in Outpatient Settings Page 13 of 29
anesthetic, hallucinogens and muscle relaxants (AACC, 2017).
3. Federation of State Medical Boards (FSMB)
Federation of State Medical Boards (FSMB) indicates in their Guidelines for Chronic Use
of Opioid Analgesics policy that for patients being prescribed opioids for chronic pain
management that “… the initial work-up should include a system review and relevant
physical examination, as well as laboratory investigations as indicated”(FSMB, 2017).
They also note the utility of periodic testing for monitoring adherence to the patient’s
treatment plan and to detect non-prescribed drugs. Regarding frequency of testing,
“Patients being treated for addiction should be tested as frequently as necessary to
ensure therapeutic adherence, but for patients being treated for pain, clinical judgment
trumps recommendations for frequency of testing (FSMB, 2017).”
Additionally, relative to how testing should be performed, the Federation of State
Medical Boards notes that POC tests have significant limitations in both sensitivity and
specificity, and therefore “the use of point of care testing for the making of more long
term and permanent changes in management of people with the disease of addiction
and other clinical situations may not be justified until the results of confirmatory testing
with more accurate methods … are obtained.” They also note that initial testing could
be done using immunoassays and followed up by a more specific technique such as
GC/MS or other chromatography-based technique. They highlight the importance of
knowing specific drug and metabolites, “not just the class of drug” for the pain
management.
4. American Society of Interventional Pain Physicians (ASIPP)
“Despite limited evidence for reliability and accuracy, screening for opioid use is
recommended, as it will identify opioid abusers and reduce opioid abuse. (Evidence:
limited)… UDT [urine drug testing] must be implemented from initiation along with
subsequent adherence monitoring, in an in-office setting with immunoassay and
confirmation for accuracy with chromatography in select cases, to identify patients who
are non-compliant or abusing prescription drugs or illicit drugs, and UDT may decrease
prescription drug abuse or illicit drug use when patients are in chronic pain
management therapy (Evidence: good) (Manchikanti et al., 2012a)”. In Part 1 of their
recommendations, ASIPP states that, “in a systematic review of treatment agreements
and UDT to reduce opioid misuse in patients with chronic pain, the evidence was
relatively weak in supporting the effectiveness of opioid treatment agreements and UDT
in reducing opioid misuse by patients with chronic pain (Manchikanti et al., 2012b).”
They note that a large percentage of testing requires follow-up confirmatory testing; in
fact, one study reports that approximately 36% of specimens required confirmation
testing, but that reference testing improves the accuracy of UDT for benzodiazepines to
83.2% (Manchikanti, Malla, Wargo, & Fellows, 2011). ASIPP also notes the limitations of
confirmation testing and POC testing. “UDT has become the standard of care for
patients on controlled substances; however, the relative value of in-office screening and

©2019 Copyright of Avalon Health Services, LLC. All rights reserved
Appropriate Number of Definitive Drug Classes to Test in Outpatient Settings Page 14 of 29
laboratory confirmation of those tests is sometimes unclear or controversial for
physicians. The POC manufacturers recommend that their test needs to be confirmed;
however, advantages and cost benefits have not been independently evaluated and
confirmed (Manchikanti et al., 2012b).”
5. Texas Pain Society
The Texas Pain Society released detailed guidelines concerning urine drug testing (UDT)
and its use in the practice of pain management. They do not recommend a prescribed
regimen of UDT but rather leave it to the discretion of the physician. They do
recommend random UDT over scheduled UDT. Concerning what should be included in a
UDT, “Elements of UDT may include specific gravity, temperature at the time of sample
collection, pH, creatinine concentration, and mass spectroscopic confirmatory testing
for the following agents: opioids (fentanyl, oxycodone, oxymorphone, tramadol,
methadone, hydrocodone, hydromorphone, morphine, codeine, propoxyphene,
meperidine, buprenorphine, tapentadol, 6-mono-acetyl morphine [6-MAM])…”(Owen,
Burton, Schade, & Passik, 2012). For the extensive list of possible drugs, in addition to
opioids, please review the attached table in Appendix D.
6. Annals of Internal Medicine Review
In 2014 Nuckols and colleagues released an extensive review of guidelines on
prescribing and monitoring opioids from more than ten different societies and
organizations in the Annals of Internal Medicine. No consensus concerning urine drug
monitoring or testing was noted across all guidelines; in fact, the APS-AAPM noted to
use UDT only “if risk is high; consider otherwise”. The NOUGG recommends that, if UDT
is used, to consider pros and cons (expert consensus). The Colorado Division of Workers
Compensation requires mandatory UDT. The VA/DoD and ASIPP uses UDT to establish a
baseline followed by random testing during treatment whereas the ACOEM and UMHS
uses UDT to establish a baseline followed by either a minimum of quarterly testing or
annual testing, respectively (Nuckols et al., 2014). The detailed table is included in
Appendix E.
7. American Society of Addictive Medicine (ASAM)
Concerning what drugs should be included in a UDT, ASAM states, “Drug testing panels
identify the use of only the specific drugs, drug classes, or drug metabolites built into
the particular test panel. However, clinicians should have the choice of what drugs to
test for each patient based on their assessment of that patient and risk history. Unlike
forensic testing, clinical testing should be individualized to each patient situation and
not determined by a forced panel of drugs. The most common immunoassay drug test
panel includes the SAMHSA-5: amphetamines (various stimulant drugs as a drug class),
marijuana metabolites (THC), cocaine metabolites, opiates (natural opiates such as
codeine and morphine, a metabolite of heroin but not other opioids such as oxycodone,
hydrocodone, buprenorphine and methadone), and phencyclidine (PCP) (ASAM, 2013).”

©2019 Copyright of Avalon Health Services, LLC. All rights reserved
Appropriate Number of Definitive Drug Classes to Test in Outpatient Settings Page 15 of 29
8. American Academy of Family Physicians (AAFP)
The AAFP published in 2019 recommendations concerning ordering and interpreting
urine drug tests. They state, “Several federal and state regulations have been enacted
that recommend or require urine drug testing in patients receiving long-term opioid
therapy. Similar guidance may apply to patients receiving long-term benzodiazepine or
stimulant therapy. (Kale, 2019).” They state that the frequency of urine drug testing
depends on individual risk factors and is ultimately left to the attending physician;
however, they do state a recommended frequency for urine drug testing given in the
Table 3 below:
Table 3: Recommended Frequency for Urine Drug Testing (Kale, 2019)
Level of misuse risk Frequency of testing
Low (no risk factors) Every 6 to 12 months
Moderate Every 3 to 6 months
High (mental health disorder, substance
use disorder, prior opioid misuse, aberrant
behavior*) or opioid dosage >120
morphine milligram equivalents
Every 1 to 3 months
*Aberrant behavior includes, but is not limited to, lost prescriptions, multiple requests for
early refills, opioid prescriptions from multiple physicians, unauthorized dose escalation, and
apparent intoxication.
They state the following clinical recommendation: “Urine drug testing can be used to
monitor compliance with prescribed therapy and detect the use of nonprescribed and
illicit substances, especially opioids, benzodiazepines, and heroin (Kale, 2019).”
9. American Pain Society/American Academy of Pain Medicine
The American Pain Society and American Academy of Pain Medicine joint guidelines
panel released their opioid treatment guidelines titled Clinical Guidelines for the Use of
Chronic Opioid Therapy in Chronic Non-cancer Pain in 2009. They addressed the
monitoring of controlled substances use via UDT as part of a chronic opioid treatment
(COT) program. The authors recommend periodic urine drug screening and suggest that
random urine drug screens may be more informative than scheduled or routine testing.
The guideline section on monitoring (Section 5) states:
“5.1: Clinicians should reassess patients on COT periodically and as warranted by
changing circumstances. Monitoring should include documentation of pain
intensity and level of functioning, assessments of progress toward achieving
therapeutic goals, presence of adverse events, and adherence to prescribed
therapies (strong recommendation, low-quality evidence).
5.2: In patients on COT who are at high risk or who have engaged in aberrant
drug-related behaviors, clinicians should periodically obtain urine drug screens

©2019 Copyright of Avalon Health Services, LLC. All rights reserved
Appropriate Number of Definitive Drug Classes to Test in Outpatient Settings Page 16 of 29
or other information to confirm adherence to the COT plan of care (strong
recommendation, low-quality evidence).
5.3: In patients on COT not at high risk and not known to have engaged in
aberrant drug-related behaviors, clinicians should consider periodically obtaining
urine drug screens or other information to confirm adherence to the COT plan of
care (weak recommendation, low-quality evidence). Clinicians should
periodically reassess all patients on COT. Regular monitoring of patients once
COT is initiated is critical because therapeutic risks and benefits do not remain
static” (Chou et al., 2009).
The American Pain Society guidelines state that for individuals at low-risk for adverse
outcomes, quarterly or semi-annual monitoring is sufficient. The risk for abuse may be
measured using standard tools, such as the Screener and Opioid Assessment for Patients
with Pain (SOAPP) and the Opioid Risk Tool. These types of tools may help clinicians
assess the suitability of long-term opioid therapy for chronic pain patients and may help
differentiate those patients who require more clinician monitoring while on long-term
opioid therapy. Both tools may be self-administered at or prior to an office visit, or
completed as part of an interview with a nurse, physician or psychologist (Chou et al.,
2009).
10. Washington State Agency Medical Directors’ Group (AMDG)
The AMDG published an Interagency Guideline on opioid dosing for chronic non-cancer
pain. This guideline and related expert commentary support low-risk individuals having
UDT up to once per year, moderate risk up to 2 per year, high risk individuals up to 3-4
tests per year, and individuals exhibiting aberrant behaviors should be tested at the
time of the office visit. They list the following as examples of aberrant behavior: “lost
prescriptions, multiple requests for early refills, opioids from multiple providers,
unauthorized dose escalation, apparent intoxication, etc. (AMDG, 2015).”
11. South Carolina Pain Management Guidelines
South Carolina’s guidelines have several statements and recommendations for clinicians
to help them with prescription and monitoring of controlled substances.
Recommendation #10 on page 23 states:
“When prescribing opioids for chronic pain, clinicians should use urine drug
testing before starting opioid therapy and consider urine drug testing at least
annually to assess for prescribed medications as well as other controlled
prescription drugs and illicit drugs”. In the discussion on pages 23 through 24,
this guideline explains to physicians on how to use urine drug testing during
patient monitoring. They explain that opioid pain medication used in
combination with other nonprescribed opioid pain medications,
benzodiazepines or heroin has potential to cause overdose, and, therefore,

©2019 Copyright of Avalon Health Services, LLC. All rights reserved
Appropriate Number of Definitive Drug Classes to Test in Outpatient Settings Page 17 of 29
patients must be assessed for those drugs during urine drug testing. There was
no consensus on the frequency of urine drug testing among experts. Experts
suggested that initial urine drug testing can be performed with an
immunoassay panel for commonly prescribed opioids and illicit drugs. For
those patients on less commonly used opioids, a more specific test was
recommended. In addition, they specified that confirmatory testing “should be
based on the need to detect specific opioids that cannot be identified on
standard immunoassays or on the presence of unexpected urine drug test
results”. This guideline explicitly states that clinicians must be familiar with
drugs included in urine drug testing panels and must know how to interpret
results. They encourage clinicians to consult a toxicologist or clinical pathologist
to help them with results interpretation and to directly confront patients about
unexpected results. This guideline discourages clinicians testing for substances
for which there will either be no patient management needed or it is unclear.
And, confirmatory testing must be restricted “to situations and substances for
which results can reasonably be expected to affect patient management
(SCBME, 2017).”
12. Wisconsin Worker’s Compensation Patient Care
Wisconsin’s Worker’s Compensation program recommends for any worker’s
compensation patient who will need opioid treatment for a period of more than 90
days, that the treating physician should follow these guidelines and or consider referral
to a Pain Management specialist. In their document, they state that “urine drug
screening before starting chronic opioid therapy is imperative” to verify that patient is
not using illegal substances. In addition, according to their guidelines, compliance
monitoring is mandatory for all patients on chronic opioid therapy with several tools
including urine drug screen for the first visit and with aberrant behavior and
unannounced urine drug screens thereafter (DWD, 2013).
13. American Society of Addictive Medicine (ASAM)
ASAM states quantification (assessing specific concentration of a drug) should not be
used to determine adherence with a specific dosage or formulation regimen. There are,
however, specific reasons for obtaining quantitative data. For example, quantification
can help a clinician decide why the other opioids are present. Serial creatinine-corrected
quantitative values can help the clinician distinguish cessation of drug use from
continued drug excretion from ongoing drug use. Finally, the guidelines note that state
laws may also guide testing decisions (ASAM, 2013).
14. Substance Abuse and Mental Health Services Administration (SAMHSA)
These guidelines are for certification for opioid treatment programs (OTPs). OTPs
require certification before they can dispense opioids to treat opioid addiction. SAMHSA
recommends benzodiazepines and amphetamines at a minimum be tested before

©2019 Copyright of Avalon Health Services, LLC. All rights reserved
Appropriate Number of Definitive Drug Classes to Test in Outpatient Settings Page 18 of 29
admission to any opioid treatment program. Barbiturates are also strongly
recommended to be tested at regular intervals during the program. Testing is not
limited to these classes of drugs and may vary from individual to individual (SAMHSA,
2007).
15. Institute for Clinical Systems Improvement (ICSI)
The ICSI in their guidelines concerning pain management released in 2017 recommend
that “routine random urine drug screens (UDS) for all patients on chronic opioid therapy
for pain should be done at least once per year. UDS should be done if there is concern of
aberrant behavior based on a prescriber’s assessments and clinical judgment (Hooten et
al., 2017).”
16. American Association for the Treatment of Opioid Dependence Inc. (AATOD)
The AATOD recommends cessation of benzodiazepines before admission to an opioid
treatment program (OTP). Gradually tapering off to a lower dose is also acceptable, but
benzodiazepine use must be addressed prior to an OTP admission. The AATOD
recommends toxicology screening for benzodiazepines, as well as routine checks of each
state’s Prescription Monitoring Drug Program. Confirmatory testing may also be used
(AATOD, 2017).
17. American Academy of Child and Adolescent Psychiatry (AACAP)
AACAP notes, “Toxicology screens are indicated for acute onset or exacerbations of
psychosis when exposure to drugs of abuse cannot otherwise be ruled out. Genetic
testing is indicated if there are associated dysmorphic or syndromic features (McClellan
& Stock, 2013).”
18. World Federation of Societies of Biological Psychiatry (WFSBP)
The WFSBP states that drug screening (urine and blood) should be sought for
schizophrenia patients as “presence of substance abuse or dependence is often not
recognized and systematically assessed, especially if such a patient is seen during an
acute psychotic episode” (WFSBP, 2015).
19. American Academy of Neurology (AAN)
The AAN states that “toxicology testing may be considered in children with status
epilepticus, when no apparent etiology is immediately identified” (AAN, 2018).
20. Department of Veterans Affairs/Department of Defense (VA/DOD)
These joint guidelines state “We recommend screening for use of tobacco, alcohol, illicit
drugs, and unauthorized use of prescription medication because their use is common
and can result in adverse outcomes” (strong recommendation) (DOD, 2018).

©2019 Copyright of Avalon Health Services, LLC. All rights reserved
Appropriate Number of Definitive Drug Classes to Test in Outpatient Settings Page 19 of 29
21. World Health Organization (WHO)
The WHO released an intervention guideline for mental, neurological, and substance use
disorder in non-specialized health settings. The WHO states that urine testing may be
considered to confirm abstinence and to “consider occasional urine testing to confirm
non-use”. Under the section concerning the investigation of chronic drug use, they state
to consider using urine drug screens “for emergency cases, a urine drug screen should
be conducted whenever intoxication, withdrawal, or overdose is suspected, especially in
cases when the person is unable to convey what they have ingested (WHO, 2016).” The
WHO lists the following substances as psychoactive substances: alcohol,
benzodiazepines, opioids, tobacco, cocaine, methamphetamines, amphetamine-type
stimulants, khat, cannabis, tramadol, “volatile” solvents, MDMA, and hallucinogens.
22. American College of Obstetricians and Gynecologists (ACOG)
ACOG states that additional research is needed to better understand the effects of
universal urine screening on clinical outcomes and recommend validated verbal
screening tools instead. ACOG acknowledges that urine drug testing has been used to
identify substance abuse and should only be performed in compliance with state’s laws
and with patient consent. ACOG also lists the following recommendations:
“Screening for substance use should be part of comprehensive obstetric care and
should be done at the first prenatal visit in partnership with pregnant woman.
Screening based only on factors, such as poor adherence to prenatal care or
prior adverse pregnancy outcome, can lead to missed cases and may add to
stereotyping and stigma. Therefore, it is essential that screening be universal.”
“Routine screening should rely on validated screening tools, such as
questionnaires, including 4Ps, NIDA, Quick Screen, and CRAFFT (for women 26
years or younger) (ACOG, 2017).
ACOG explicitly states, “Routine urine drug screening is controversial for several
reasons. A positive drug test result is not in itself diagnostic of opioid use disorder or its
severity. Urine drug testing only assesses for current or recent substance use; therefore,
a negative test does not rule out sporadic substance use… Health care providers should
be aware of their laboratory’s test characteristics and request that confirmatory testing
with mass spectrometry and liquid or gas chromatography be performed as appropriate
(ACOG, 2017).”
23. Society of Obstetricians and Gynaecologists of Canada (SOGC)
The SOGC recommends periodic drug screening for all pregnant women and all women
of childbearing age (III-A). The recommended method of drug screening is a urine
toxicology screen (II-2A); however, they state that prior to maternal drug toxicology
testing is ordered that informed consent be obtained (III-B) (Wong, Ordean, & Kahan,
2011).

©2019 Copyright of Avalon Health Services, LLC. All rights reserved
Appropriate Number of Definitive Drug Classes to Test in Outpatient Settings Page 20 of 29
24. American Psychiatric Association (APA)
The APA released their third edition of the Practice Guidelines for the Psychiatric
Evaluation of Adults in 2016. Within it, they acknowledge that urine toxicology may
provide clues to substance abuse during an initial psychiatric evaluation (APA, 2016).
25. Anxiety Disorders Association of Canada (ADAC)
The ADAC recommends urine toxicology as part of the patient’s baseline investigations if
warranted. This urine toxicology assessment applies to anxiety and other related
disorders, which include “panic disorder, agoraphobia, GAD, selective mutism,
separation anxiety disorder, SAD (social phobia), specific phobia, substance/medication-
induced anxiety disorder, as well as anxiety disorder due to another medical condition
or not elsewhere classified” (Katzman et al., 2014).
Evidence-based Scientific References
AACC. (2017). Using Clinical Laboratory Tests to Monitor Drug Therapy in Pain Management Patients.
Retrieved from https://www.aacc.org/science-and-practice/practice-guidelines/using-clinical-
laboratory-tests-to-monitor-drug-therapy-in-pain-management-patients
AAN. (2018). DIAGNOSTIC ASSESSMENT OF THE CHILD WITH STATUS EPILEPTICUS. Retrieved from
http://tools.aan.com/professionals/practice/guidelines/Status_Epilepticus_clinician.pdf
AATOD. (2017). Guidelines for Addressing Benzodiazepine Use in Opioid Treatment Programs (OTPs).
Retrieved from http://www.aatod.org/guidelines-for-addressing-benzodiazepine-use-in-opioid-
treatment-programs-otps/
ACOG. (2017). Opioid Use and Opioid Use Disorder in Pregnancy. Retrieved from
https://www.acog.org/-/media/Committee-Opinions/Committee-on-Obstetric-
Practice/co711.pdf
AMDG. (2015). Interagency Guideline on Prescribing Opioids for Pain. Retrieved from
http://www.agencymeddirectors.wa.gov/Files/2015AMDGOpioidGuideline.pdf
APA. (2016). THE AMERICAN PSYCHIATRIC ASSOCIATION PRACTICE GUIDELINES FOR THE PSYCHIATRIC
EVALUATION OF ADULTS. Retrieved from
https://psychiatryonline.org/doi/pdf/10.1176/appi.books.9780890426760
ASAM. (2013, 10/26/2013). Drug Testing: A White Paper of the American Society of Addiction Medicine
(ASAM). Retrieved from https://www.asam.org/docs/default-source/public-policy-
statements/drug-testing-a-white-paper-by-asam.pdf
Becker, W., & Starrels, J. (2018, 07/05/2018). Prescription drug misuse: Epidemiology, prevention,
identification, and management. Uptodate.com. Retrieved from
https://www.uptodate.com/contents/prescription-drug-misuse-epidemiology-prevention-
identification-and-management
CDC. (2017a, 12/19/2017). Drug Overdose Death Data. Retrieved from
https://www.cdc.gov/drugoverdose/data/statedeaths.html
CDC. (2017b, 02/09/2017). Opioid Data Analysis and Resources. Retrieved from

©2019 Copyright of Avalon Health Services, LLC. All rights reserved
Appropriate Number of Definitive Drug Classes to Test in Outpatient Settings Page 21 of 29
https://www.cdc.gov/drugoverdose/data/analysis.html
CDC. (2017c, 08/30/2017). Prescription Opioid Data. Retrieved from
https://www.cdc.gov/drugoverdose/data/prescribing.html
CDC. (2017d). U.S. Opioid Prescribing Rate Maps. Retrieved from
https://www.cdc.gov/drugoverdose/maps/rxrate-maps.html
CDC. (2017e, 07/31/2017). U.S. State Prescribing Rates, 2016. Retrieved from
https://www.cdc.gov/drugoverdose/maps/rxstate2016.html
CDC. (2018, 08/31/2018). 2018 Annual Surveillance Report of Drug-Related Risks and Outcomes —
United States. Retrieved from https://www.cdc.gov/drugoverdose/pdf/pubs/2018-cdc-drug-
surveillance-report.pdf
Chou, R., Fanciullo, G. J., Fine, P. G., Adler, J. A., Ballantyne, J. C., Davies, P., . . . Miaskowski, C. (2009).
Clinical Guidelines for the Use of Chronic Opioid Therapy in Chronic Noncancer Pain. The Journal
of Pain, 10(2), 113-130.e122. Retrieved from https://doi.org/10.1016/j.jpain.2008.10.008.
doi:10.1016/j.jpain.2008.10.008
CMS. (2012, 02/01/2012). Medical Necessity Documentation. Retrieved from
https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-
MLN/MLNProducts/Fast-Facts/Medical-Necessity-Documentation.html
CMS. (2018). Proper Coding for Specimen Validity Testing Billed in Combination with Drug Testing. MLN
Matters, SE18007, 1-4. Retrieved from https://www.cms.gov/Outreach-and-
Education/Medicare-Learning-Network-MLN/MLNMattersArticles/Downloads/SE18001.pdf.
CMS. (2019). Chapter 3 - Verifying Potential Errors and Taking Corrective Actions. In Medicare Program
Integrity Manual (Vol. Rev. 853). Retrieved from https://www.cms.gov/Regulations-and-
Guidance/Guidance/Manuals/Downloads/pim83c03.pdf
DOD, V. (2018). VA/DOD CLINICAL PRACTICE GUIDELINE FOR THE MANAGEMENT OF PREGNANCY.
Retrieved from
https://www.healthquality.va.gov/guidelines/WH/up/VADoDPregnancyCPG4102018.pdf
Dowell, D., Haegerich, T. M., & Chou, R. (2016). CDC Guideline for Prescribing Opioids for Chronic Pain -
United States, 2016. MMWR Recomm Rep, 65(1), 1-49. doi:10.15585/mmwr.rr6501e1
DWD. (2013). Chronic Opioid Clinical Management Guidelines for Wisconsin Worker’s Compensation
Patient Care. Retrieved from
https://dwd.wisconsin.gov/wc/medical/pdf/CHRONIC%20OPIOID%20CLINICAL%20MANAGEME
NT%20GUIDELINES%20.pdf
FSMB. (2017). Guidelines for the Chronic Use of Opioid Analgesics. Retrieved from
https://www.fsmb.org/globalassets/advocacy/policies/opioid_guidelines_as_adopted_april-
2017_final.pdf
Gencheva, R., Petrides, A., Kantartjis, M., Tanasijevic, M., Dahlin, J. L., & Melanson, S. (2018). Clinical
Benefits of Direct-to-Definitive Testing for Monitoring Compliance in Pain Management. Pain
Physician, 21(6), E583-e592.
Hadland, S. E., & Levy, S. (2016). Objective Testing: Urine and Other Drug Tests. Child and adolescent
psychiatric clinics of North America, 25(3), 549-565. Retrieved from
https://www.ncbi.nlm.nih.gov/pubmed/27338974
https://www.ncbi.nlm.nih.gov/pmc/PMC4920965/. doi:10.1016/j.chc.2016.02.005
HHS. (2017). Mandatory Guidelines for Federal Workplace Drug Testing Programs. Federal Register,
82(13), 7920-7970. Retrieved from
https://www.samhsa.gov/sites/default/files/workplace/frn_vol_82_7920_.pdf.
Hoffman, R. (2018, 10/16/2018). Testing for drugs of abuse (DOA). Uptodate.com. Retrieved from
https://www.uptodate.com/contents/testing-for-drugs-of-abuse-doa

©2019 Copyright of Avalon Health Services, LLC. All rights reserved
Appropriate Number of Definitive Drug Classes to Test in Outpatient Settings Page 22 of 29
Hooten, M., Thorson, D., Bianco, J., Bonte, B., Clavel Jr, A., Hora, J., . . . Walker, N. (2017, August 2017).
Pain: Assessment, Non-Opioid Treatment Approaches and Opioid Management. Retrieved from
https://www.icsi.org/_asset/f8rj09/Pain.pdf
Jannetto, P. J., & Langman, L. J. (2018). Using Clinical Laboratory Tests to Monitor Drug Therapy in Pain
Management Patients. The Journal of Applied Laboratory Medicine: An AACC Publication, 2(4),
471-472. Retrieved from http://jalm.aaccjnls.org/content/jalm/2/4/471.full.pdf.
doi:10.1373/jalm.2017.025304
Kale, N. (2019). Urine Drug Tests: Ordering and Interpreting Results. Am Fam Physician, 99(1), 33-39.
Retrieved from https://www.aafp.org/afp/2019/0101/p33.pdf.
Katzman, M. A., Bleau, P., Blier, P., Chokka, P., Kjernisted, K., Van Ameringen, M., . . . Walker, J. R.
(2014). Canadian clinical practice guidelines for the management of anxiety, posttraumatic
stress and obsessive-compulsive disorders. BMC psychiatry, 14 Suppl 1(Suppl 1), S1-S1.
Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/25081580
https://www.ncbi.nlm.nih.gov/pmc/PMC4120194/. doi:10.1186/1471-244X-14-S1-S1
Krock, K., Pesce, A., Ritz, D., Thomas, R., Cua, A., Rogers, R., . . . Kilbourn, K. (2017). Lower Cutoffs for LC-
MS/MS Urine Drug Testing Indicates Better Patient Compliance. Pain Physician, 20(7), E1107-
e1113. Retrieved from
https://www.painphysicianjournal.com/current/pdf?article=NDcxNw%3D%3D&journal=108.
Manchikanti, L., Abdi, S., Atluri, S., Balog, C. C., Benyamin, R. M., Boswell, M. V., . . . Wargo, B. W.
(2012a). American Society of Interventional Pain Physicians (ASIPP) guidelines for responsible
opioid prescribing in chronic non-cancer pain: Part 2--guidance. Pain Physician, 15(3 Suppl), S67-
116.
Manchikanti, L., Abdi, S., Atluri, S., Balog, C. C., Benyamin, R. M., Boswell, M. V., . . . Wargo, B. W.
(2012b). American Society of Interventional Pain Physicians (ASIPP) guidelines for responsible
opioid prescribing in chronic non-cancer pain: Part I--evidence assessment. Pain Physician, 15(3
Suppl), S1-65. Retrieved from
https://www.painphysicianjournal.com/current/pdf?article=MTcwMg%3D%3D&journal=68.
Manchikanti, L., Malla, Y., Wargo, B. W., & Fellows, B. (2011). Comparative evaluation of the accuracy of
benzodiazepine testing in chronic pain patients utilizing immunoassay with liquid
chromatography tandem mass spectrometry (LC/MS/MS) of urine drug testing. Pain Physician,
14(3), 259-270.
McClellan, J., & Stock, S. (2013). Practice Parameter for the Assessment and Treatment of Children and
Adolescents With Schizophrenia. Journal of the American Academy of Child & Adolescent
Psychiatry, 52(9), 976-990. Retrieved from https://doi.org/10.1016/j.jaac.2013.02.008.
doi:10.1016/j.jaac.2013.02.008
Nuckols, T. K., Anderson, L., Popescu, I., Diamant, A. L., Doyle, B., Di Capua, P., & Chou, R. (2014). Opioid
prescribing: a systematic review and critical appraisal of guidelines for chronic pain. Ann Intern
Med, 160(1), 38-47. doi:10.7326/0003-4819-160-1-201401070-00732
Owen, G. T., Burton, A. W., Schade, C. M., & Passik, S. (2012). Urine drug testing: current
recommendations and best practices. Pain Physician, 15(3 Suppl), Es119-133.
Phan, H. M., Yoshizuka, K., Murry, D. J., & Perry, P. J. (2012). Drug testing in the workplace.
Pharmacotherapy, 32(7), 649-656. Retrieved from
https://accpjournals.onlinelibrary.wiley.com/doi/abs/10.1002/j.1875-9114.2011.01089.x.
doi:10.1002/j.1875-9114.2011.01089.x
SAMHSA. (2007). Guidelines for the Accreditation of Opioid Treatment Programs Retrieved from
https://www.samhsa.gov/sites/default/files/programs_campaigns/medication_assisted/2007-
otp-accreditation-guidelines.pdf

©2019 Copyright of Avalon Health Services, LLC. All rights reserved
Appropriate Number of Definitive Drug Classes to Test in Outpatient Settings Page 23 of 29
SAMHSA. (2017). Key Substance Use and Mental Health Indicators in the United States: Results from the
2016 National Survey on Drug Use and Health. Retrieved from
https://www.samhsa.gov/data/sites/default/files/NSDUH-FFR1-2016/NSDUH-FFR1-2016.pdf
SCBME. (2017). Revised Joint Pain Management Guidelines South Carolina State Boards of Dentistry,
Medical Examiners, Nursing and Pharmacy. Retrieved from
https://www.llr.sc.gov/pol/Medical/pdf/FINAL%20Joint%20Revised%20Pain%20Management%
20Guidelines%20August%202017.pdf
Schulte, F., & Lucas, E. (2017). Liquid Gold: Pain Doctors Soak Up Profits By Screening Urine For Drugs.
Kaiser Health News. Retrieved from https://khn.org/news/liquid-gold-pain-doctors-soak-up-
profits-by-screening-urine-for-drugs/
WFSBP. (2015). World Federation of Societies of Biological Psychiatry (WFSBP) Guidelines for Biological
Treatment of Schizophrenia Part 3: Update 2015 Management of special circumstances:
Depression, Suicidality, substance use disorders and pregnancy and lactation Retrieved from
http://www.wfsbp.org/fileadmin/user_upload/Treatment_Guidelines/Hasan_et_al__2015_.pdf
WHO. (2016). mhGAP Intervention Guide. Retrieved from
https://apps.who.int/iris/bitstream/handle/10665/250239/9789241549790-
eng.pdf?sequence=1
Wong, S., Ordean, A., & Kahan, M. (2011). Substance use in pregnancy. J Obstet Gynaecol Can, 33(4),
367-384. doi:10.1016/s1701-2163(16)34855-1

©2019 Copyright of Avalon Health Services, LLC. All rights reserved
Appropriate Number of Definitive Drug Classes to Test in Outpatient Settings Page 24 of 29
Appendix A: 2017 U.S. Prescribing Rate Map (CDC, 2017d)
This map depicts the 2017 rate per 100 persons for retail opioid prescriptions dispensed in the U.S. at a
state level. Alabama had the highest rate (107.2) whereas the District of Columbia had the lowest rate
28.5). The CDC reports that the national average prescribing rate in 2017 was 58.7, the lowest rate in
more than ten years (CDC, 2017d).

©2019 Copyright of Avalon Health Services, LLC. All rights reserved
Appropriate Number of Definitive Drug Classes to Test in Outpatient Settings Page 25 of 29
Appendix B: 2017 U.S. Rate of Drug Overdose Deaths (CDC,
2017a)
This map depicts the number of age-adjusted rates of drug overdose deaths (per 100,000) in the U.S. by
state in 2017 as reported by the CDC. The lowest rate reported is in Nebraska (8.1) with the highest rate
reported in West Virginia (57.8) (CDC, 2017a).

©2019 Copyright of Avalon Health Services, LLC. All rights reserved
Appropriate Number of Definitive Drug Classes to Test in Outpatient Settings Page 26 of 29
Appendix C: Drug Classes Used in Determining the Average
Number of Prescribed Drug Classes per Month per Individual
The following drug classes were used in determining the average number of prescribed drug classes
per month per individual:
NULLǂ
Alcohol(s)
Alkaloids, not otherwise specified (NOS)
Amphetamines
Analgesics, non-opioid
Antidepressants, NOS
Antidepressants, serotonergic
Antidepressants, tricyclic
Antiepileptics, NOS
Antipsychotics, NOS
Barbiturates
Benzodiazepines
Buprenorphine
Cocaine
Fentanyls
Gabapentin
Hypnotics, sedative (non-benzodiazepines)
Methadone
Methylphenidate
Opiates
Opioids and opiate analogs
Oxycodone
Pregabalin
Skeletal muscle relaxants
Tapentadol
Tramadol
ǂNULL indicates a drug not included in the cross walk (i.e. a drug, such as prednisone, that
is typically not associated with a toxicology screen).

©2019 Copyright of Avalon Health Services, LLC. All rights reserved
Appropriate Number of Definitive Drug Classes to Test in Outpatient Settings Page 27 of 29
Appendix D: Agents in UDT (Owen et al., 2012) with assigned
2018 CPT Definitive Drug Class Code
2018 CPT Definitive Drug Class Code
Opioids
buprenorphine 80348 buprenorphine
fentanyl 80354 fentanyls
6-mono-acetyl morphine (6-
MAM) 80356 heroin metabolite
methadone 80358 methadone
hydrocodone 80361 opiates
hydromorphone 80361 opiates
morphine 80361 opiates
codeine 80361 opiates
oxycodone 80365 oxycodone
oxymorphone 80365 oxycodone
propoxyphene 80367 propoxyphene
tapentadol 80372 tapentadol
tramadol 80373 tramadol
meperidine 80362-80364 opioids & opiates analogs
benzodiazepines
nordiazepam 80346, 80347 benzodiazepines
oxazepam 80346, 80347 benzodiazepines
temazepam 80346, 80347 benzodiazepines
barbiturates
phenobarbital 80345 barbiturates
secobarbital 80345 barbiturates
miscellaneous
ethanol or ethyl glucuronide 80320-80322 alcohol(s) (or alcohol biomarker)
amphetamine 80324-80326 amphetamines
methamphetamine 80324-80326 amphetamines
methylphenidate 80360 methylphenidate
cocaine 80353 cocaine
MDMA 80359 methylenedioxyamphetamines
phencyclidine 83992 phencyclidine
tetrahydrocannabinol (THC) 80349 cannabinoids, natural
carisoprodol and/or
meprobamate 80369, 80370 skeletal muscle relaxants

©2019 Copyright of Avalon Health Services, LLC. All rights reserved
Appropriate Number of Definitive Drug Classes to Test in Outpatient Settings Page 28 of 29
Appendix E Selected Guideline Recommendations from
(Nuckols et al., 2014)

©2019 Copyright of Avalon Health Services, LLC. All rights reserved
Appropriate Number of Definitive Drug Classes to Test in Outpatient Settings Page 29 of 29