Claudio Moretti, MD – University of Turin, Turin, Italy – [email protected].

Polyunsaturated Fatty Acids andCytokines: Their Relationship in AcuteLung Injury
69
Paolo Cotogni, Antonella Trombetta, Giuliana Muzio,Maria Felice Brizzi, and Rosa Angela Canuto
Contents
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 930Lung and Cytokines . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 930Lipids, PUFAs, and Lung Injury . . . . . . . . . . . . . . . . . . . . 932PUFAs and Lung Injury: Nutrients or Drugs? . . . . . . 934In Vitro Studies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 934Animal Studies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 937Clinical Studies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 938
Applications to Critical or Intensive Care . . . . . . . . 939
Applications to Other Conditions . . . . . . . . . . . . . . . . . 940
Guidelines and Protocols . . . . . . . . . . . . . . . . . . . . . . . . . . . 940
Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 941
Summary Points . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 941
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 941
AbstractAcute lung injury (ALI) and acute respiratorydistress syndrome (ARDS) are inflammatorydiseases whose clinical severity depends onthe grade of inflammatory response. Inflamma-tory cytokines are key elements in the patho-genesis of ALI/ARDS, and the occurrence ofan imbalance between pro- and anti-inflammatory cytokines leads to additionalnon-pulmonary organ dysfunction which con-tributes to excess mortality rates.
Treatment of these patients includes nutri-tion support with lipids, usually soybeanoil-based lipid emulsions, which are rich inomega (n)-6 polyunsaturated fatty acids(PUFAs) and deficient in n-3 PUFAs; however,too much n-6 PUFAs are detrimental due totheir pro-inflammatory effects. Conversely, alarge amount of experimental studies and somerandomized clinical trials showed the benefitsof the n-3 PUFA administration in the contextof ALI because of their anti-inflammatoryproperties. Based on these data, several scien-tific societies recommended in their guidelines,with an A or B grade of recommendation, theuse of n-3 PUFAs in ALI/ARDS patients.However, at present, the issue of lipid therapyin ALI/ARDS is still controversial due, at leastin part, to inconclusive or contradicting resultsin several recent clinical trials using n-3PUFAs.
P. Cotogni (*)Department of Medicine, Anesthesiology and IntensiveCare, S. Giovanni Battista Hospital, University of Turin,Turin, Italye-mail: [email protected]
A. Trombetta • M.F. BrizziDepartment of Medical Sciences, University of Turin,Turin, Italye-mail: [email protected];[email protected]
G. Muzio • R.A. CanutoDepartment of Experimental Medicine and Oncology,University of Turin, Turin, Italye-mail: [email protected];[email protected]
# Springer Science+Business Media New York 2015R. Rajendram et al. (eds.), Diet and Nutrition in Critical Care,DOI 10.1007/978-1-4614-7836-2_112
929

List of AbbreviationsAA Arachidonic acidALI Acute lung injuryARDS Acute respiratory distress syndromeBAL Bronchoalveolar lavageDHA Docosahexaenoic acidEN Enteral nutritionEPA Eicosapentaenoic acidFA Fatty acidFiO2 Fractional inspired oxygenICU Intensive care unitIL InterleukinLOS Length of stayLPS LipopolysaccharideLT Leukotrienen OmegaPaO2 Arterial oxygen partial pressurePG ProstaglandinPN Parenteral nutritionPUFA Polyunsaturated fatty acidRCT Randomized controlled trialTNF Tumor necrosis factorTX Thromboxane
Introduction
Acute respiratory distress syndrome (ARDS) isconsidered a form of acute diffuse lung injury(ALI). According to the Berlin definition (Fergusonet al. 2012), each subcategory of ARDS (mild,moderate, and severe) is defined by mutually exclu-sive ranges of the ratio between arterial oxygenpartial pressure (PaO2) and fractional inspired oxy-gen (FiO2) (200mmHg<PaO2/FIO2�300mmHg,100 mm Hg<PaO2/FIO2�200 mm Hg, and PaO2/FIO2�100 mm Hg, respectively).
The acute phase of this syndrome is manifestedby the early onset of respiratory failure (character-ized by hypoxemia refractory to oxygen supplywithin 1 week of a known clinical insult ornew/worsening respiratory symptoms) related toseveral triggers and clinical disorders generally dis-tinguished in pulmonary [pneumonia (bacteria orvirus), microbial products (e.g., endotoxins),pulmonary aspiration of gastric contents] andextrapulmonary (trauma/hemorrhagic shock,
extensive burns, ischemia/reperfusion injury, acutepancreatitis, cardiopulmonary bypass, transfusionsof blood products) (Leaver and Evans 2007).
ARDS is frequently progressive and it is char-acterized by distinct phases with different clinical,radiographic, and histopathological findings.Radiographicfindings are similar to those observedin the case of cardiogenic pulmonary edema,mainly bilateral infiltrates (irregular and asymmet-ric) and sometimes pleural effusions (Fig. 1).
Histopathological findings of ALI include diffusealveolar epithelium damage (principally, denudationof the basementmembrane of the alveolus and necro-sis of type I cells) with activated neutrophils, alveolarmacrophages, hyaline membranes, and protein-richedema fluid in the alveolar spaces (Fig. 2).
The pathophysiology of ALI is complex andmultifaceted. The lung inflammatory responseinvolves various interactions among many celltypes, and it is characterized by the production andrelease of several chemical mediators. Figure 3 is asimplified graphic description of how the anatomyand physiology of alveolar space, the main site ofinflammatory reactions occurring in ALI, change.
Lung and Cytokines
The lung is a complex organ with many differentcell types, i.e., pneumocytes (alveolar type I and II),
Fig. 1 Anteroposterior chest radiograph from a patientwith the acute respiratory distress syndrome who wasreceiving mechanical ventilation. Irregular and asymmetricinfiltrates are present throughout both lung fields
930 P. Cotogni et al.

pulmonary capillary endothelial cells, alveolarmacrophages, and fibroblasts. Several studiessuggest that the lung itself can be an importantcytokine-producing organ.
Cytokines are a diverse group of inflammatorymediators, produced by a wide variety of celltypes, which initiate and orchestrate the hostresponse to different injuries. Intercellular commu-nication through cytokine networking playsa key role for homeostasis. Cytokines seem tohave concentration-dependent effects. At lowerconcentrations, they modulate tissue response toinjuries; at higher concentrations, they induceproportionally more severe local and systemicinflammatory responses. If this cytokine over-production is not regulated, it may remarkablyamplify the release of further pro-inflammatorymediators and, at least, the overall inflammatoryresponse.
Both ALI and ARDS are characterized byan intense inflammatory response. In ARDSearly phase, the alveolar space is the site ofsignificant inflammatory reactions (Pugin et al.1999). ALI/ARDS are characterized by alveolarinfiltration with neutrophils and macrophages,both able to release inflammatory cytokines.However, recent theories suggest that it is notthe neutrophil and macrophage number but their
alveolarair space
protein-richoedema fluid
type I cell
capillary
alveolar macrophage
type II cell
necrotictype I celldamaged
type I cell
intacttype II cell
hyalinemembrane
migratingneutrophil
IL-10IL-8IL-6IL-1β
type
hme
IL-10IL-8IL-6IL-6IL-1β
activatedneutrophil
cell damage
activation
Normal alveolus Alveolus in acute lung injury
alveolar macrophage
TNF-α
Fig. 3 The normal alveolus and the alveolus in acute lunginjury. Neutrophil is shown migrating through a gap in thecapillary endothelium into the alveolar space (activatedneutrophil). In the alveolar space, an alveolar macrophageis secreting cytokines: tumor necrosis factor (TNF)-α,interleukin (IL)-1β, IL-6, IL-8, and IL-10. The alveolar
type I cells are damaged or necrotic, while alveolar typeII cells are intact and release cytokines. The tissue archi-tecture is disrupted with the formation of hyaline mem-branes on the denuded basement membrane. The alveolarspace is filled by protein-rich edema fluid
Fig. 2 Alveolar damage in acute lung injury/acute respira-tory distress syndrome. The tissue architecture is disrupted,alveoli are collapsed, alveolar type II (ATII) cells are hyper-plastic, and alveolar type I cells are necrotic. Alveoli containprotein-rich edema fluid and macrophages. Collagen deposi-tion in the interstitium has begun. Hematoxylin and eosinstaining, 200� magnification. The picture was kindly givenby Luisa Delsedime, MD, Anatomia Patologica, AOU Cittàdella Scienza e della Salute, Turin, Italy
69 Polyunsaturated Fatty Acids and Cytokines: Their Relationship in Acute Lung Injury 931

pro-inflammatory cytokine release that produceslung injury. In this setting, cytokines have a cen-tral position as signaling mediators that initiate,increase, and maintain inflammatory responses ona local basis. Indeed, in ALI/ARDS, an accumu-lation of both pro- and anti-inflammatory cyto-kines within the alveolar spaces is demonstrated.
Many cytokines were detected at elevatedlevels in bronchoalveolar lavage (BAL) fluid inpatients with ARDS, i.e., tumor necrosis factor(TNF)-α, interleukin (IL)-1β, IL-6, IL-8, andIL-10. TNF-α is the main pro-inflammatory cyto-kine and it is important in driving the initial lunginflammatory response, principally indirect by thestimulation of other cytokines (i.e., IL-6 andIL-8). IL-6 occupies a crucial place in the ARDSinflammatory response. Chemokine IL-8 is themajor neutrophil chemotactic factor into thealveolar space, and it is an early marker forthe development of ARDS. Finally, IL-10, whichhas anti-inflammatory effects, plays a pivotal rolein closing down the inflammatory response once itachieves its primary purpose.
The pivotal role of a hyper-inflammatoryresponse, characterized by overproduction ofTNF-α, IL-6, and IL-8, in the evolution of thedisease from ALI to ARDS is documented.Indeed, many studies report a higher mortality inpatients who have increased pro-inflammatorycytokine concentrations (TNF-α, IL-6, and IL-8)in the BAL at the onset of ARDS or persistentincreased concentrations in days 3–10.
Physiologically, the critical dependency on thepresence of the inflammatory ligand (e.g.,platelet-activating factor) and free arachidonicacid (AA) may help to confine the outbreak oflipid-mediator production to sites of initial inflam-matory process. Conversely, compartmentaliza-tion of alveolar cytokines can be lost in the caseof a damaged alveolar barrier. Cytokines gener-ated in the alveoli may go into the systemic circu-lation leading to the beginning of a systemicinflammatory response syndrome.
The reason why a patient with ALI developsARDS while another recovers is still notcompletely clear. In ARDS-developing patients,it is hypothesized that, at some level, regulation ofthe inflammatory response must be inadequate,
but why or when this regulation is insufficient isa matter of debate. The study of the balancebetween pro- and anti-inflammatory cytokines isof greater importance to understand the patho-physiology of ALI than a single cytokine concen-tration, because the degree of cytokine imbalanceis a contributing element to disease severity (Parket al. 2001).
Persistently high levels of pro-inflammatorycytokines, as well as a reduced production ofanti-inflammatory cytokines, have been demon-strated to be correlated with the severity of lunginjury. The degree of this cytokine imbalance hasa pivotal role in inducing other non-pulmonaryorgan dysfunctions and increasing mortality ratesin ARDS patients. In particular, thepro-inflammatory activity depends on the balancebetween the cytokine and its inhibitor(s). InARDS early phase, the finding of low levels ofanti-inflammatory cytokines (i.e., IL-10 and IL-1receptor antagonist) in the BAL is associated withan increase in patient mortality. The ratio TNF-αto IL-10 in the BAL fluid was significantly higher(3.52 vs. 0.85) in patients with ARDS than inthose at risk of developing ARDS.
Lipids, PUFAs, and Lung Injury
Among ALI ventilated patients, malnutrition hasbeen associated with adverse outcomes due toincreased infection risk, prolonged mechanicalventilation dependency, prolonged intensive careunit (ICU) length of stay (LOS), and highermortality.
In general, critically ill patients receive nutri-tion support including lipids. Administration oflipid emulsions offers many advantages inpatients with acute respiratory failure, becausecompared with glucose they provide a richersource of calories in a small volume with a lowercarbon dioxide load and less hyperglycemia.Moreover, lipid supply is mandatory to avoidessential fatty acid (FA) deficiency.
Accepted guidelines recommend providing30–35 % of nonprotein calories as lipids inpatients with ALI/ARDS (Mizock 2001). Lipidswere introduced into parenteral nutrition (PN)
932 P. Cotogni et al.

formulations in the 1960s. However, there is alack of consensus about the optimal source andcomposition of lipids (long- vs. medium-chaintriglycerides, soybean oil vs. olive oil and fishoil) both in parenteral and enteral formulas forthe patient with ALI/ARDS.
Commonly used parenteral lipid emulsions(i.e., soybean oil-based fat emulsions) containlarge amounts of n-6 polyunsaturated fatty acids(PUFAs) (i.e., more than 50 % of linoleic acid)that form AA [omega (n)-6 PUFA], while only7 % α-linolenic acid can be metabolicallyconverted to eicosapentaenoic acid (EPA, n-3PUFA) and docosahexaenoic acid (DHA, n-3PUFA). Therefore, intravenous fat emulsionshave a very low n-3/n-6 PUFA ratio, rangingbetween 1:5 and 1:7. Likewise, the n-3/n-6 ratioin enteral products may be as low as 1:50. Thus,ALI/ARDS patients – either on standard enteralnutrition (EN) or PN – are generally exposed to alarge quantity of linoleic acid. However, adminis-tration of high quantities of linoleic acid is notdesirable in ALI/ARDS patients because it causesa production of high amounts of AA, whose mainfunctional role is to be a substrate for the synthesisof bioactive pro-inflammatory mediators knownas eicosanoids [above all, prostaglandin (PG)-E2,thromboxane (TX)-A2, and leukotriene (LT)-B4]and platelet-activating factor, which modulatesseverity and duration of inflammatory responses.
The impact of parenteral lipid supply on thelung function of patients with acute respiratoryfailure has been contradicting. Potential harmfuleffects have been related to type and/or adminis-tration rate of lipid emulsions. In particular, someauthors thought that these negative effects mightcorrelate to the infusion of soybean oil-based lipidemulsions – because they are rich in linoleic acid –and suggested that linoleic acid-derived synthesisof eicosanoids may worsen gas exchange andpulmonary hemodynamics in critically illpatients. Eicosanoids are major pathogenetic fac-tors of ARDS, and their negative effects on pul-monary function (e.g., increased permeability,edema formation, polymorphonuclear activation,thrombocyte aggregation, vasoconstriction, andbronchoconstriction) have been widelyinvestigated.
As early as 1942, the immunomodulatoryproperties of lipids were displayed. Over the pastyears, there has been an improved understandingof PUFA pathophysiology, and several mecha-nisms for the interaction between PUFAs andinflammation or immune response have beendemonstrated. Indeed, after PUFA supply (diet,as well as EN or PN), many cell properties andrelated functions are modified, mainly the inflam-matory and immunity responses (Calder 2006).
Briefly, n-3 PUFAs are more regarded asanti-inflammatory, whereas n-6 PUFAs as pro-inflammatory. More recent studies suggested thatn-3 PUFAs may be involved in the resolution ofinflammation (Calder 2013a).
Since a network of factors regulates the rela-tionship between n-3 and inflammation, the mech-anisms underlying the effects of n-3 PUFAs oncell event modulation are complex. To summarizethe mechanisms of n-3 PUFA modulation of theinflammatory response, it can be said that themain and well-demonstrated anti-inflammatoryactions of n-3 PUFAs include the following:
(a) A decreased production of AA-derived medi-ators such as 2-series PG and LTB4 as a resultof a reduction in AA content of cell mem-branes and of inhibition of AA metabolism.
(b) An increased production of eicosanoid medi-ators from EPA (e.g., 3-series PG and LTB5),since these mediators have weak biologicalpotency compared with those produced fromAA; for example, LTB5 is 10- to 100-fold lesspotent as a neutrophil chemotactic agent thanLTB4, or PGE3 is a less potent inducer ofcyclooxygenase-2 gene expression in fibro-blasts and of IL-6 production by macrophagescompared with PGE2.
(c) A decreased T-cell proliferation and produc-tion of IL-2 induced by EPA and DHAproviding.
(d) A decreased expression of some adhesionmolecules on the surface of monocytes, mac-rophages, lymphocytes, and endothelial cellsinduced by EPA and DHA providing.
(e) A decreased production of pro-inflammatorycytokines, due to decreased activation ofpro-inflammatory transcription factors such
69 Polyunsaturated Fatty Acids and Cytokines: Their Relationship in Acute Lung Injury 933

as nuclear factor κ-B and increased activationof anti-inflammatory transcription factorssuch as peroxisome proliferator-activatedreceptor-γ.
(f) An increased production of resolvins (E-seriesfrom EPA and D-series from DHA) andprotectins (from DHA) having potent anti-inflammatory or inflammation-resolvingproperties.
PUFAs and Lung Injury: Nutrientsor Drugs?
Over the last 25 years, the discovered ability ofn-3 PUFAs to downregulate many differentresponses of the inflammatory process hassuggested to several researchers that these FAsmight have a key role in determining the gradeof severity of some inflammatory diseases. Con-sequently, n-3 PUFAs have been widely used notonly as nutrients but mainly as pharmacologicalagents.
Briefly, the rationale of the therapeutic use ofn-3 PUFAs was based on several well-establishedissues: (1) PUFAs are key structural and func-tional elements of the phospholipids in cell mem-branes; (2) cells involved in the immunity andinflammation (neutrophils, monocytes, macro-phages, dendritic cells, and endothelial cells) arericher in n-6 PUFAs than n-3, but the contents ofAA, EPA, and DHA can bemodified by n-3 PUFA(i.e., EPA and DHA) administration (oral, enteral,and parenteral); (3) PUFA challenge, as well asthe FA composition of cell membrane of humaninflammatory cells, influences the functions ofthose cells; and, last but more important, (4) n-3PUFAs and n-6 PUFAs have opposing influenceson inflammation.
ALI/ARDS are inflammatory diseases too;therefore, numerous studies have been carriedout to evaluate strategies (drugs or interventionalprocedures) to reduce the severity of lung inflam-matory processes by lowering the production ofpro-inflammatory mediators (eicosanoids andcytokines). Nonetheless, few studies have founda significant improvement on mortality in thosepatients.
Since 1997, many editorials have stressed thepossibility to manipulate the inflammatoryresponse in ALI/ARDS patients using n-3PUFAs as drugs (the so-called pharmaconutrition)(Mayer and Seeger 2008). The research on theinfluence of FAs on immunity started in the1970s. Subsequently, a great number of workswith cell or animal models have been carried outwith the aim to demonstrate efficacy in modifyingthe inflammatory responses of fish oil or theirmain active components (i.e., EPA and DHA).Likewise, there have been some clinical trials ofenteral or parenteral administration of fishoil-enriched nutrition formulas in critically illpatients with ALI/ARDS.
In Vitro Studies
The experimental models used were animal iso-lated lungs or, mainly, cell line models. Fre-quently, a human lung carcinoma cell line (A549cells) was used. A549 are alveolar epithelial cellswith type II pneumocyte properties that retainmany of the characteristics of normal humantype II epithelial cells and could synthesize leci-thin and phosphatidylcholine with a high percent-age of desaturated FAs. Several authors usedalveolar type II cells because it was shown tohave a central position in the pathophysiology ofthe alveolar space.
After in vitro administration, FAs were rapidlyincorporated in the phospholipid spectrum ofalveolar cell membranes; in fact, as pulmonarysurfactant (the surface-active phospholipoproteincomplex) producers, alveolar type II cells have ahigher lipid metabolism, e.g., a significantincrease in DHA concentration in the lung phos-pholipid fraction was observed 1 h after DHAinfusion.
Several experimental studies with isolatedlungs and culture of different pulmonary cellsclearly showed a pivotal role of AA and its metab-olites as mediators of injury. In contrast, supple-mentation of n-3 PUFAs demonstrated toreduce alveolar release of pro-inflammatory medi-ators and to reduce organ failure in animal lungmodels.
934 P. Cotogni et al.

Rapid changes in cell membrane phospholipidFA composition and lipid-derived inflammatorymediator generation were observed both aftershort cell exposure to n-3 PUFAs and short-termintravenous administration of n-3 PUFAs. It wasobserved that PG3 was produced within 5 min ofA549 cell exposure to EPA – with a peak at 4 h –and this rapid increase of PG3 was correlated withthe metabolism of EPA by cyclooxygenases in theA549 cells. Experimental data suggested that EPAand DHA are both able to inhibit PGE2
production.A short-term n-3 PUFA supplementation
induced a significant increase in the n-3 PUFAcomposition of perfusate (after 5 min) and lungtissue (after 3 h). After as little as 3 h of lungperfusion with an n-3 PUFA-enriched emulsion,significant alterations in the spectrum of eicosa-noid generation were found in the isolatedlung model. Likewise, after 10 min in a model ofseptic lung injury, it was found that the vascularleakage provoked by bacterial exotoxin in rabbitlungs was differentially influenced by AA versusEPA, related to the generation of 4- versus5-series LTs.
Early studies demonstrated that EPA andDHA inhibited endotoxin-stimulated productionof IL-6 and IL-8 by cultured human endothelialcells and n-3 PUFAs inhibited endotoxin-inducedTNF-α production by cultured monocytes. Thedifferential impact of manipulation of cell mem-brane phospholipid composition due to n-3 PUFAversus n-6 PUFA administration on cytokine pro-duction provoked by pro-inflammatory mediatorswas demonstrated in A549 cells.
Although DHA is not able to give rise to LTs, ithas a pivotal role since it can be incorporatedunchanged into membrane lipids or retroconvertedinto EPA. Evidence suggests that the anti-inflammatory and immunosuppressive effects ofn-3 PUFA supply may be attributed mainly, oreven exclusively, to DHA supplementation.
In the past two decades, many authors havehighlighted that the n-3/n-6 PUFA ratio in nutri-tion support may influence inflammation sinceoptimal n-3 administration was not only doserelated but was also independently affected bythe n-3/n-6 PUFA ratio. Different n-3/n-6 PUFA
ratios from 1:1 to 1:4 have been proposed, but thequestion of the most favorable n-3/n-6 PUFA ratioin ALI/ARDS patients is still to be defined.
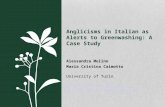
The impact of the n-3/n-6 PUFA ratio on cyto-kine release by A549 cells exposed to an endo-toxin (i.e., lipopolysaccharide – LPS) challengewas investigated in a recent experimental study(Cotogni et al. 2011). As in many studies, theinflammatory process was elicited by administra-tion of LPS – a component of Gram-negativebacteria cell wall – because LPS is an importantmediator in the pathogenesis of ARDS and A549cells are able to produce the acute phase proteinLPS-binding protein. In particular, it was deter-mined the time- and dose-dependent effect of LPSon the TNF-α response in A549 cells (Fig. 4). TheFA composition in phospholipids of A549 cellmembranes was also analyzed, and the n-3/n-6PUFA ratio was reported to be 1:5, with AA asthe most prevalent PUFA (Table 1).
The administration of different ratios of AAand DHA on the LPS-induced cytokine responsefrom A549 cells showed that the supply of 1:1 and
3 7 240
100
200
300
baseline
LPS 100
LPS 200
LPS 400
TN
F-α
(pg
/106
cells
)
hours
Fig. 4 TNF-α release from LPS-stimulated A549 cells.TNF-α concentrations were measured in cell culture mediaby ELISA assay at the time points indicated. The resultswere expressed as picograms of released cytokines per 106
adherent cells (pg/106 cells) and as mean � SD (n = 9experiments). LPS lipopolysaccharide, TNF-α tumornecrosis factor-α. *P < 0.05 LPS 100 and 200 versus base-line, at 7 and 24 h; **P < 0.01 LPS 400 versus baseline, at24 h; ***P < 0.005 LPS 400 versus baseline, at 7 h;#P < 0.01 LPS 400 7 h versus LPS 400 24 h
69 Polyunsaturated Fatty Acids and Cytokines: Their Relationship in Acute Lung Injury 935

1:2 DHA/AA ratios reversed the baseline predom-inance of n-6 over n-3 in the n-3/n-6 PUFA ratioof cell membranes. Particularly, the release ofpro-inflammatory cytokines (TNF-α, IL-6, andIL-8) was reduced by 1:1 and 1:2 DHA/AA ratios;on the contrary, it was further increased by 1:4 and1:7 DHA/AA ratios if compared to LPS challengealone (Fig. 5). Moreover, the 1:1 and 1:2DHA/AA ratios were effective in increasing anti-inflammatory IL-10 release and in modifying thebalance between pro- and anti-inflammatory cyto-kines (Fig. 6). This finding confirmed previousstudies showing that IL-10 protects against thelethal effects of LPS by significantly reducingthe production of pro-inflammatory cytokines in
Table 1 Percentage content of fatty acids in phospho-lipids of A549 cell membranes
Fatty acid
C14:0 (saturated) 3.7
C16:0 (saturated) 31.9
C16:1 (monounsaturated) 9.6
C18:0 (saturated) 16.8
C18:1 (monounsaturated) 27.3
C18:2 (linoleic acid, n-6) 2.8
C20:4 (arachidonic acid, AA, n-6) 6.2
C22:6 (docosahexaenoic acid, DHA, n-3) 1.7
n-3/n-6 PUFA ratio 1:5
Data were expressed as the percentage of fatty acids and aremeans of four experiments. Percentage content of fattyacids less than 0.5 % was not reported. n omega, PUFApolyunsaturated fatty acid
0
100
200
300
400
500
0
1000
2000
3000
4000
5000
0
10000
20000
30000
40000
50000
0
20
40
60
80
100
TNF-α IL-6
IL-8 IL-10
DHA/AA
DHA/AA
bl C 1:1 1:2 1:4 1:7
DHA/AA
pg/1
06 c
ells
pg/1
06 c
ells
pg/1
06 c
ells
pg/1
06 c
ells
# #
# #
DHA/AA
bl C 1:1 1:2 1:4 1:7
bl C 1:1 1:2 1:4 1:7 bl C 1:1 1:2 1:4 1:7
Fig. 5 Lipopolysaccharide-stimulated TNF-α, IL-6, IL-8,and IL-10 release from A549 cells treated with differentDHA/AA ratios. Interleukin concentrations were measuredin cell culture media by ELISA assay at 7 h. The resultswere expressed as picograms (pg) of released cytokines per
106 adherent cells and as mean � SD (n = 4 experi-ments). AA arachidonic acid, bl baseline, C control, DHAdocosahexaenoic acid, IL interleukin, TNF-α tumor necro-sis factor-α. *P < 0.01 versus control; **P < 0.001 versusall; #P < 0.001 versus control and 1:2
936 P. Cotogni et al.

human monocytes and murine peritoneal macro-phages. These data suggested that inflammatorycytokine release was dependent on the proportionof n-3 in the n-3/n-6 PUFA ratio of alveolar cell
membranes, being reduced with the supply ofDHA and increased with a high proportion ofAA. According to several other data, shiftingthe PUFA supply from n-6 to n-3 with a ratioof 1:2 may be a good means to dampenpro-inflammatory responses in ALI.
Animal Studies
Experimental studies with animal models demon-strated that production of AA-derived eicosanoidsand cytokines decreases with a diet containing fishoil in ALI and septic murine models.
Macrophages isolated from mice fed with adiet containing fish oil produced less PGE2 andIL-6 in response to LPS stimulation than thoseisolated from mice fed with other lipid-enricheddiets.
Feeding rats with an n-3 PUFA-enricheddiet, as compared with an n-6 PUFA-enrichedone, was associated to: (1) a reduced severity oflung microvascular protein permeabilityand hypotension in a model of endotoxin-inducedALI, (2) a reduced synthesis of pro-inflammatoryeicosanoid (LTB4, PGE2, and TXB2)released from stimulated alveolar macrophages,and (3) a decrease in AA and an increase inEPA and DHA in cell membrane phospholipidsof alveolar macrophages. After intraperitonealinjection of LPS, peak plasma TNF-α, IL-1β,and IL-6 levels were more reduced inmice fed with a fish oil diet than in those fedwith a safflower oil diet (i.e., a diet rich in n-6PUFAs).
Using either a model of ALI, in which LPS wasinstilled in the trachea, or a model of intraperito-neal inflammation, in which LPS was injectedintraperitoneally, it was demonstrated that a3-day course of intravenous lipid emulsion infu-sions was sufficient to modify inflammatoryresponses. Fish oil-based lipid emulsions reducedalveolar leukocyte transmigration, proteinleakage, and cytokine production, as well ascytokine concentrations in the intravascular com-partment. Conversely, soybean oil-based lipidslead to a further increase in the inflammatoryresponse.
–0.5 0.0 0.5 1.0 1.5 2.0
C
DHA/AA1:1
DHA/AA1:2
DHA/AA1:4
DHA/AA1:7
0 1 2 3
C
DHA/AA1:1
DHA/AA1:2
DHA/AA1:4
DHA/AA1:7
0 1 2 3 4
C
DHA/AA1:1
DHA/AA1:2
DHA/AA1:4
DHA/AA1:7
TNF-α /IL-10 (log10 pg/106 cells)
IL-6/IL-10 (log10 pg/106 cells)
IL-8/IL-10 (log10 pg/106 cells)
Fig. 6 Ratios between pro-inflammatory (TNF-α, IL-6,and IL-8) and anti-inflammatory (IL-10) cytokines releasedfrom lipopolysaccharide-stimulated A549 cells treatedwith different DHA/AA ratios. Interleukin concentrationswere measured in cell culture media by ELISA assay at7 h. The results were expressed as log10 picograms (pg) ofreleased cytokines per 106 adherent cells and as mean �SD (n = 4 experiments). AA arachidonic acid, bl baseline,C control, DHA docosahexaenoic acid, IL interleukin,TNF-α tumor necrosis factor-α. *P < 0.001 versus control;**P < 0.001 versus all
69 Polyunsaturated Fatty Acids and Cytokines: Their Relationship in Acute Lung Injury 937

Clinical Studies
N-3 PUFA Administration via EnteralRouteClinical data showing benefits associated with theadministration of nutrition formulas enriched withn-3 PUFAs in ALI/ARDS patients came initiallyfrom three randomized controlled trials (RCTs)using the enteral route. These RCTs showed thatEN with a study formula containing EPA,γ-linolenic acid, and antioxidants (vitamins Cand E, β-carotene, and taurine), as comparedwith high-fat formula (control formula), reducedalveolar inflammatory mediators and improvedclinical outcomes in patients with ALI, ARDS,or sepsis.
The first RCT showed the ability of an enteralformula with a high n-3/n-6 PUFA ratio (1:1) toreduce pulmonary inflammation and improveclinical outcomes, i.e., better oxygenation, shorterrequirement for mechanical ventilation, shorterICU-LOS, and less incidence of new organ fail-ure; however, no difference in mortality wasobserved in ARDS patients (Gadek et al. 1999).Similarly, an RCT in ALI/ARDS mechanicallyventilated patients showed that an n-3 PUFA-enriched enteral diet may be more beneficial forgas exchange, respiratory dynamics, and length ofmechanical ventilation if compared with a controlformula, but no difference both in ICU or hospitalLOS and mortality was found between the twoformulas (Singer et al. 2006). Another RCT wasable to demonstrate that the administration of thesame enteral diet contributed to guarantee animproved oxygenation and an independencefrom mechanical ventilation, less incidence ofnew organ dysfunction, and more ICU-free daysand, mainly, was associated with lower mortalityrates in ARDS mechanically ventilated patientswith severe sepsis and septic shock (Pontes-Arruda et al. 2006). In 2008, a meta-analysis ofthe pooled outcomes from these three RCTs con-cluded that the n-3 PUFA-enriched enteral for-mula could reduce mortality, rate of new organfailure, ICU-LOS, and length of ventilation inALI/ARDS patients (Pontes-Arruda et al. 2008).
Nevertheless, in 2011, three further RCTs werepublished that addressed the issue of the potential
positive effects of an enteral n-3 PUFA-enrichednutrition in ALI/ARDS patients showing mixingresults. The first RCT analyzed the effect of anenteral n-3 PUFA-enriched diet in septic patientswith ALI or ARDS showing that the administra-tion of the study formula, compared to a controlformula with less lipids than in the previous threestudies, was associated to a shorter ICU-LOS butnot to an improvement in gas exchange or in alower incidence of novel organ failures (Grau-Carmona et al. 2011). A phase 2 placebo-controlled RCT in ALI patients investigating anenteral administration of fish oil for up to 14 daysdid not demonstrate a decrease in cytokine orother inflammatory marker concentrations bothin BAL fluid from baseline to day 4 or 8 and inplasma, as well as a decrease in ventilator-freedays, ICU-free days, organ failure score, or60-day mortality (Stapleton et al. 2011). The lastRCT tested the effects of enteral feeding with n-3PUFAs, γ-linolenic acid, and antioxidants on clin-ical outcomes in ALI patients in a phase 3 trial(OMEGA trial) using a twice-daily bolus admin-istration (Rice et al. 2011). Contrary to all otherRCTs, the authors reported that enteral adminis-tration of this formula was associated to signifi-cantly fewer ventilator-free days, ICU-free days,and non-pulmonary organ failure-free days, aswell as more days with diarrhea. The trial wasstopped early for futility at the first interim analy-sis. The interpretation of the OMEGA trial pre-sents some difficulties (Lev and Singer 2013).Firstly, it was used a different approach of twice-daily bolus administration of enteral formulasinstead of continuous enteral infusion. Secondly,the enteral diets administered to the study group(i.e., megadoses of n-3 PUFAs and lower proteincontent) and to the control group (i.e., higherprotein and carbohydrate content) are notably dif-ferent from those used in the first three RCTs.
N-3 PUFA Administration via ParenteralRouteEnteral administration of n-3 PUFAs mightrequire more time before effectively influencingthe cellular FA composition and the lipid-mediated inflammatory response. Moreover, thedaily volume of enteral formula prescribed is
938 P. Cotogni et al.

calculated such as to meet patients’ requirement ofcalories rather than a scheduled “pharmacologi-cal” dosage of n-3 PUFAs. It is well known thatICU patients exhibit different degrees of toleranceto EN, as it is well documented that the morepatients are critically ill, the less they tolerateEN. Thus, an unpredictable number of criticalpatients might not receive the “pharmacological”dosage of n-3 PUFAs.
An alternative approach to provide n-3 PUFAsto ICU patients unable to meet their nutritionrequirements by oral or enteral route is to admin-ister a parenteral formula prepared from fish oil.Differently to oral/enteral feeding, parenteraladministration of PUFAs can induce more rapidchanges in lipid-derived responses. Indeed, inALI, there is the need of promptly active treat-ments to early modulate the net inflammatoryresponse in the alveolar spaces.
In septic patients, intravenous infusion ofn-3 PUFAs modified lipid mediator synthesisand reduced endotoxin-stimulated monocyte pro-inflammatory cytokine production, while cyto-kine production was markedly amplified by n-6PUFA administration (Mayer et al. 2003). Con-versely, PN administered for 7 days with a 1:1mixture of medium-chain triglycerides and long-chain triglycerides, with the n-3/n-6 PUFA ratio of1:2 compared with a same mixture supplementedwith fish oil with the n-3/n-6 PUFA ratio of 1:7,did not affect inflammatory marker production ormeasures of clinical outcomes in an RCT in unse-lected critically ill medical patients (Frieseckeet al. 2008).
In the last 5 years, three RCTs have investi-gated the effects of parenteral administration ofn-3 PUFA-enriched lipid emulsions inALI/ARDS patients. The first RCT investigatedthe effects of an n-3 PUFA-enriched lipid emul-sion in ARDS patients with EN intolerance show-ing no significant changes in hemodynamic andgas exchange parameters (Sabater et al. 2008).Previously, the same authors had showed thatparenteral administration of an n-3-enriched lipidemulsion was accompanied by the synthesis of asmaller amount of pro-inflammatory lipid media-tors compared to long-chain triglyceride 100 %emulsion in ARDS patients. In a second trial,
patients with systemic inflammatory responsesyndrome or sepsis were randomized into twogroups to receive an intravenous lipid emulsionenriched or not in fish oil (Barbosa et al. 2010).The authors reported that the PaO2:FiO2 ratio atday 6 was significantly higher and plasma IL-6concentration significantly decreased in the grouptreated with fish oil; however, fish oil administra-tion did not improve the length of ventilation orICU-LOS and mortality. The last RCT investi-gated the effects of an intravenous administrationof n-3 PUFAs with the n-3/n-6 PUFA ratio of 1:2as supplementation of EN for 14 days in ARDSpatients finding that fish oil administration alonedid not improve ventilation, ICU-LOS, or survival(Gupta et al. 2011).
Applications to Critical orIntensive Care
ARDS is the most severe life-threatening mani-festation of ALI. Both remain a significant healthburden for intensivists and critical care physiciansbecause of their considerable morbidity and mor-tality. In 2005, in the USA, the crude incidence ofALI was 78.9 per 100,000 person-years; eachyear, there are 190,600 cases of ALI associatedwith 74,500 deaths and 3.6 million hospital days.In 2004, in 78 ICUs of ten European countries,ALI occurred in 463 (7 %) out of 6,522 admis-sions, and in the 16 % of the whole mechanicallyventilated patients, 65 % cases occurred on ICUadmission.
Pathologically, ALI and ARDS are inflamma-tory diseases; clinically, their severity depends onthe grade of inflammatory response. Thus, numer-ous studies have been carried out investigatingnew strategies to reduce the grade of this inflam-matory response, mainly by reducing the releaseof pro-inflammatory mediators. However, phar-macological therapies such as corticosteroids,ketoconazole, antioxidants, nitric oxide, prostacy-clins, exogenous surfactants, and β2 agonistsfailed to show positive results in human studies.
Supplementation with n-3 PUFAs was demon-strated to exert beneficial effects in a number ofinflammatory diseases. The rationale for their use
69 Polyunsaturated Fatty Acids and Cytokines: Their Relationship in Acute Lung Injury 939

in ALI/ARDS patients is consistent and based onseveral issues. Firstly, a large amount of experi-mental studies in lung models supports the anti-inflammatory properties of n-3 PUFAs. Secondly,patients at risk for ARDS and with establishedARDS have plasma EPA concentrations about25 % and 7 %, respectively, as compared withnormal, hypothesizing a potential benefit for n-3PUFA administration in those patients. Finally, inthree level I studies involving patients with ALI,ARDS, and sepsis, the use of an enteral dietenriched with n-3 PUFAs (in the form of EPA),γ-linolenic acid, and antioxidants was shown tosignificantly reduce ICU-LOS, mechanical venti-lation length, organ failure incidence, and mortal-ity if compared to the use of a standard enteralformula.
Based on these data, the European Society forClinical Nutrition and Metabolism, AmericanSociety of Parenteral and Enteral Nutrition, Soci-ety of Critical Care Medicine, and Canadianguidelines recommended, with an A or B gradeof recommendation, in their guidelines publishedbetween 2003 and 2009, the use of n-3 PUFAs inALI/ARDS patients. However, nowadays, theclinical application of these recommendationshas been lagging behind in critical or intensivecare, which is due, at least in part, to inconclusiveor contradicting results in several recent clinicaltrials using n-3 PUFAs.
Applications to Other Conditions
Over the last 25 years, the data coming out from agreat number of studies have left us an improvedknowledge of how n-3 PUFAs and their derivatemediators modulate inflammation/resolution andimmunity. Evidence that supports both the anti-inflammatory and antitumor effects of n-3 PUFAshas been gathered; moreover, the molecular path-ways underlying these effects have been clarifiedboth in vitro and in vivo. In particular, there is nowa better understanding of various mechanismsgenerating the production of inflammatory cyto-kines in several inflammatory, metabolic, andneurodegenerative diseases, as well as ininflammation-related cancers.
The capacity of n-3 PUFAs to determine a shiftfrom a strongly pro-inflammatory environment toone of reduced inflammation supports the hypoth-esis that these FAs might be useful as a componentof the therapy in various inflammatory diseases.Thus, EPA and/or DHA have been evaluated insome inflammatory conditions.
For the potential or in-use applications of n-3PUFAs to clinical conditions different from ALI,see a recent review (Calder 2013b). Briefly, fishoil or its derived EPA and DHA have demon-strated the efficacy in animal models of rheuma-toid arthritis, inflammatory bowel diseases, andasthma. There have been a number of clinicaltrials evaluating the effects of administration ofn-3 PUFAs in those diseases with contradictingresults. For example, there is some pretty goodevidence of the efficacy of n-3 PUFAs in rheuma-toid arthritis. Conversely, despite positive resultsin some studies, there is only weak evidence thatn-3 PUFAs have clinical benefits in inflammatorybowel diseases. Finally, clinical studies on fish oilin adult patients with asthma do not show benefit.
Guidelines and Protocols
The “European Society for Clinical Nutrition andMetabolism Guidelines on Enteral Nutrition:Intensive Care” (Kreymann et al. 2006) statedthat “Patients with ARDS should receive ENenriched with n-3 fatty acids and antioxidants”as a B grade recommendation. However, this rec-ommendation was not evaluated in the “ESPENGuidelines on Parenteral Nutrition: IntensiveCare” (Singer et al. 2009), although the authorsstated that “Addition of EPA and DHA to lipidemulsions has demonstrable effects on cell mem-branes and inflammatory processes; fishoil-enriched lipid emulsions probably decreaselength of stay in critically ill patients” both as Bgrade recommendations.
The American Society for Parenteral andEnteral Nutrition “Guidelines for the Provisionand Assessment of Nutrition Support Therapy inthe Adult Critically Ill Patient” (McClaveet al. 2009), also being co-published by the Soci-ety of Critical Care Medicine, stated that “Patients
940 P. Cotogni et al.

with ARDS and severe ALI should be placed onan enteral formulation characterized by an anti-inflammatory lipid profile (i.e., n-3 fish oil, borageoil) and antioxidants” (A grade recommendation).This recommendation was based on the three pos-itive trials published at that time.
The Canadian guidelines (updated June 2013)stated that “Based on 2 level 1 studies and 5 level2 studies, the use of an enteral formula with fishoils, borage oils and antioxidants in patients withALI and ARDS should be considered. When PNwith intravenous lipids is indicated, lipids thatreduce the load of n-6 FA/soybean oil emulsionsshould be considered. However, there are insuffi-cient data to make a recommendation on the typeof lipids to be used that reduce the n-6 FA/soybeanoil load in critically ill patients receiving PN.”
Conclusions
ALI/ARDS patients are at high risk of malnutrition;therefore, they need nutrition support, includinglipids. Soybean oil-based lipid emulsions, rich inn-6 PUFAs and commonly used for these patients,may aggravate the inflammatory response. In con-trast, fish oil-based lipid emulsions, rich in n-3PUFAs, may exert an anti-inflammatory effect.These data suggest that shifting the PUFA supplyfrom n-6 to n-3 could be an important elementaffecting the alveolar cytokine and eicosanoidrelease and consequently ameliorates the clinicaloutcome in ALI/ARDS patients.
In summary, there are good experimental evi-dence and convincing rationale according to then-3 PUFAs used in ALI/ARDS patients. However,recent RCTs using n-3 PUFAs in these patients didnot confirm these positive effects. Further studies arenecessary to offer more precise indications, timing,and modalities for n-3 PUFA administration.
Summary Points
• Acute lung injury (ALI) and acute respiratorydistress syndrome (ARDS) are inflammatorydiseases whose clinical severity depends onthe grade of inflammation.
• Cytokines are key elements in the pathogenesisof ALI/ARDS.
• Soybean oil-based lipid emulsions, rich inomega (n)-6 polyunsaturated fatty acids(PUFAs), may aggravate the inflammatoryresponse. In contrast, fish oil-based lipid emul-sions, rich in n-3 PUFAs, may exert an anti-inflammatory effect.
• Experimental and clinical data suggested thatshifting the PUFA supply from n-6 to n-3decreases the alveolar cytokine and eicosanoidrelease and consequently ameliorates the clin-ical outcome in ALI/ARDS patients.
• Based on these data, several scientific societiesrecommended in their guidelines the use of n-3PUFAs in ALI/ARDS patients.
References
Barbosa VM, Miles EA, Calhau C, et al. Effects of fish oilcontaining lipid emulsion on plasma phospholipid fattyacids, inflammatory markers, and clinical outcomes inseptic patients: a randomized, controlled clinical trial.Crit Care. 2010;14:R5.
Calder PC. n-3 polyunsaturated fatty acids, inflammation,and inflammatory diseases. Am J Clin Nutr. 2006;83Suppl 6:1505S–19S.
Calder PC. n-3 fatty acids, inflammation and immunity:new mechanisms to explain old actions. Proc Nutr Soc.2013a;72:326–36.
Calder PC. Omega-3 polyunsaturated fatty acids andinflammatory processes: nutrition or pharmacology?Br J Clin Pharmacol. 2013b;75:645–62.
Canadian clinical practice guidelines for nutrition supportin mechanically ventilated, critically ill adult patients.http://www.criticalcarenutrition.com. Accessed 1 Nov2013.
Cotogni P, Muzio G, Trombetta A, et al. Impact of the ω-3to ω-6 polyunsaturated fatty acid ratio on cytokinerelease in human alveolar cells. J Parenter EnteralNutr. 2011;35:114–21.
Ferguson ND, Fan E, Camporota L, et al. The Berlindefinition of ARDS: an expanded rationale, justifica-tion, and supplementary material. Intensive Care Med.2012;38:1573–82.
Friesecke S, Lotze C, Köhler J, et al. Fish oil supplemen-tation in the parenteral nutrition of critically ill medicalpatients: a randomised controlled trial. Intensive CareMed. 2008;34:1411–20.
Gadek JE, DeMichele SJ, Karlstad MD, et al. Effect ofenteral feeding with eicosapentaenoic acid, gamma-linolenic acid, and antioxidants in patients with acuterespiratory distress syndrome. Enteral Nutrition inARDS Study Group. Crit CareMed. 1999;27:1409–20.
69 Polyunsaturated Fatty Acids and Cytokines: Their Relationship in Acute Lung Injury 941

Grau-Carmona T, Morán-García V, García-de-Lorenzo A,et al. Effect of an enteral diet enriched witheicosapentaenoic acid, gamma-linolenic acid and anti-oxidants on the outcome of mechanically ventilated,critically ill, septic patients. Clin Nutr.2011;30:578–84.
Gupta A, Govil D, Bhatnagar S, et al. Efficacy and safety ofparenteral omega-3 fatty acids in ventilated patientswith acute lung injury. Indian J Crit Care Med.2011;15:108–13.
Kreymann KG, Berger MM, Deutz NDP, et al. ESPENguidelines on enteral nutrition: intensive care. ClinNutr. 2006;25:210–23.
Leaver SK, Evans TW. Acute respiratory distress syn-drome. BMJ. 2007;335:389–94.
Lev S, Singer P. n-3 fatty acids and γ-linolenic acid sup-plementation in the nutritional support of ventilatedpatients with acute lung injury or acute respiratorydistress syndrome. World Rev Nutr Diet.2013;105:136–43.
Mayer K, Seeger W. Fish oil in critical illness. Curr OpinClin Nutr Metab Care. 2008;11:121–7.
Mayer K, Gokorsch S, Fegbeutel C, et al. Parenteral nutri-tion with fish oil modulates cytokine response inpatients with sepsis. Am J Respir Crit Care Med.2003;167:1321–8.
McClave SA, Martindale RG, Vanek VW, et al. Guidelinesfor the provision and assessment of nutrition supporttherapy in the adult critically ill patient: Society ofCritical Care Medicine (SCCM) and American Societyfor Parenteral and Enteral Nutrition (A.S.P.E.N.).J Parenter Enteral Nutr. 2009;33:277–316.
Mizock BA. Nutritional support in acute lung injury andacute respiratory distress syndrome. Nutr Clin Pract.2001;16:319–28.
Park WY, Goodman RB, Steinberg KP, et al. Cytokinebalance in the lungs of patients with acute respiratory
distress syndrome. Am J Respir Crit Care Med.2001;164:1896–903.
Pontes-Arruda A, Aragão AM, Albuquerque JD. Effects ofenteral feeding with eicosapentaenoic acid, gamma-linolenic acid, and antioxidants in mechanically venti-lated patients with severe sepsis and septic shock. CritCare Med. 2006;34:2325–33.
Pontes-Arruda A, Demichele S, Seth A, et al. The use of aninflammation-modulating diet in patients with acutelung injury or acute respiratory distress syndrome: ameta-analysis of outcome data. J Parenter Enteral Nutr.2008;32:596–605.
Pugin J, Verghese G,Widmer MC, et al. The alveolar spaceis the site of intense inflammatory and profibrotic reac-tions in the early phase of acute respiratory distresssyndrome. Crit Care Med. 1999;27:304–12.
Rice TW,Wheeler AP, Thompson BT, et al. Enteral omega-3 fatty acid, γ-linolenic acid, and antioxidant supple-mentation in acute lung injury. JAMA.2011;306:1574–81.
Sabater J, Masclans JP, Sacanell J, et al. Effects on hemo-dynamics and gas exchange of omega-3 fatty acid-enriched lipid emulsion in acute respiratory distresssyndrome (ARDS): a prospective, randomized,double-blind, parallel group study. Lipids Health Dis.2008;7:39.
Singer P, Theilla M, Fisher H, et al. Benefit of an enteraldiet enriched with eicosapentaenoic acid and gamma-linolenic acid in ventilated patients with acute lunginjury. Crit Care Med. 2006;34:1033–8.
Singer P, Berger MM, Van den Berghe G, et al. ESPENguidelines on parenteral nutrition: intensive care. ClinNutr. 2009;28:387–400.
Stapleton RD, Martin TR, Weiss NS, et al. A phase IIrandomized placebo-controlled trial of omega-3 fattyacids for the treatment of acute lung injury. Crit CareMed. 2011;39:1655–62.
942 P. Cotogni et al.