high dose insulin in beta blocker and calcium channel blocker

Contemporary heart failure management
Dr Joris Mekel
GP meeting
26 March 2015

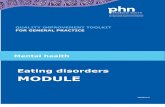
Case 1
• Mr T. McI. – 49 years
• Viral illness June 2014
• Progressive dyspnoea to NYHA FC III
• 6-8 mid-strength beers/day
• Unremarkable blood tests

Case 1
I
II
III
aVR
aVL
aVF
V1
V2
V3
V4
V5
V6
II
PID: 45948 08/22/2014 08:25:00 MCINNERNEY, TROY05/20/1965 DOB 49 years Male Dept
RoomTech NIK
Rx:Dx:
Req MD:Ref MD: DR CHEEMA
Rate 104PR 182QRSD 108QT 342QTc 449
--AXIS--P 77QRS -4T 79
Sinus tachycardia, rate 104 bpm.Normal PR intervalPossible Left atrial enlargementSeptal infarct , age undetermined
tj
CC: Dr. A. Cheema
- ABNORMAL ECG - Confirmed By: Tony Jackson 08/26/2014 15:58:44
GE MAC35 25 mm/sec 10 mm/mV F 60~ 0.5 - 150 Hz

Case 1

Case 1
• Angiogram normal
• Management:
– Admitted to hospital
– Diuretics, ACE inhibitor, β-blocker, Spironolactone, thiamine

Definition
• An inability for the heart to maintain sufficient blood flow to meet the metabolic requirements of the body, or to do so only at a raised filling pressure.

An inability for the heart to maintain sufficient blood flow to meet the metabolic requirements of the body

…or to do so only at a raised filling pressure.

Definition
• Clinical syndrome characterised by diminished effort capacity and dyspnoea due to cardiac dysfunction.

Compensatory Mechanisms
Frank-Starling Mechanism
a. At rest, no HF
b. HF due to LV systolic dysfunction
c. Advanced HF

Compensatory Neurohormonal Stimulation
Decreased Cardiac Output
Sympathetic nervous system
Renin-angiotensin system
Antidiuretic hormone (vasopressin)
Heart rate
Contractility Vasoconstriction Circulating volume
Anteriolar
Maintain blood
pressure
Cardiac output
Stroke volume
+
- +
Venous
Venous return to heart
( preload)
Peripheral edema and pulmonary
congestion

Compensatory Mechanisms
Frank-Starling Mechanism
a. At rest, no HF
b. HF due to LV systolic dysfunction
c. Advanced HF

Diagnosis
• History & clinical examination
• Blood tests (esp TFT, ferritin)
• ECG
• CXR
• Echocardiogram
• Angiography, cardiac catheterisation
• MRI

Diagnosis
• History & clinical examination
• Blood tests (esp TFT, ferritin)
• ECG
• CXR
• Echocardiogram
• Angiography, cardiac catheterisation
• MRI

Management
• Address underlying cause
– Correct ischaemia, repair/replace valves etc
• Non-pharmacological
– Avoid toxins
– Sodium & fluid restrict
– Exercise

Aetiology
• Ischaemia • Post-viral myocarditis • Hypertension • Valvular • Idiopathic - incl genetic • Nutritional eg Beri-beri • Toxins esp alcohol • Metabolic – haemochromatosis, Gaucher’s • Peripartum • Tachycardiomyopathy • Thyrotoxicosis • HOCM • Restrictive • Constrictive pericarditis • Rare eg non-compaction

Management
Lifestyle Modifications:
• Weight reduction
• Discontinue smoking
• Avoid alcohol and other cardiotoxic substances
• Exercise
Medical Considerations:
• Treat HTN, hyperlipidemia, diabetes, arrhythmias
• Coronary revascularization
• Anticoagulation
• Immunization
• Sodium restriction
• Daily weights
• Close outpatient monitoring

Management
• Pharmacological
– Diuretics
– ACE inhibitors
• ARB’s
– β-blockers
– Spironolactone
– Digoxin
– Ivabradine

Preload reduction
• Diuretics
• Nitrates

Compensatory Mechanisms
Frank-Starling Mechanism
a. At rest, no HF
b. HF due to LV systolic dysfunction
c. Advanced HF


Case 1
– β-blocker uptitration limited by hypotension
– Ivabradine started


Case 2
• Mr B.J. – 76 years
• Presents with progressive dyspnoea for a few months
• No angina, no history of hypertension, no recent infective illness, little alcohol
• Admitted to hospital with heart failure.
• Oedema, JVP elevated, heart rate 100 bpm, regular, BP normal.
• No murmurs

Case 2 - investigations
• Blood tests unremarkable
• TSH, ferritin

Case 2 - investigations

Case 2 - investigations
• ECG

Case 3 - investigations

Case 4 - investigations



Case 2 - management
• Diuretics
• ACE inhibitor
• Spironolactone
• β - blocker
• Aspirin
• Statin
• ACE-I & β – blocker uptitration limited by hypotension
• Symptomatic improvement but LVEF remained at 24%, NYHA FC II

Afterload reduction
• Concept evolved in 1970’s
• Sodium nitroprusside
• Phentolamine
• Nitrates
• Hydralazine

642 men with heart failure Randomised to Isosorbide mononitrate & Hydralazine vs Prazosin vs placebo 36% relative mortality risk reduction at 3 years (36% vs 47%)


• 253 patients, NYHA FC IV • Placebo vs Enalapril • Mortality risk reduction at 6 months showed a
40% relative risk reduction (26% vs 44%)

• 7601 patients with heart failure • Candesartan vs placebo (patients who tolerated ACE-I
were taking them • 10% relative risk reduction at 38 months

3023 patients, NYHA II – IV, EF >40% No effect on mortality, reduced hospital admissions

• 2548 patients, NYHA II – IV, EF <40% • 15% relative risk reduction in composite outcome of death or
hospital admission for heart failure.

• 2028 patients, ACE intolerant
• 23% relative risk reduction in death/hospital admission for heart failure

β-blockers
• MERIT-HF
• CIBIS
• Carvedilol
• SENIORS

Carvedilol
1094 patients, LVEF <35% Assigned 2:1 to Carvedilol or placebo 65% relative risk reduction (3.2% vs 7.8%) in death at 6 to 12 months

Bisoprolol
2647 patients, LVEF <35%, NYHA III or IV Bisoprolol or placebo 34% relative risk reduction (11.8% vs 17.3%) in mortality at 1.3 years

Metoprolol
3991 patients, LVEF <40%, NYHA II to IV 34% relative risk reduction (7.2 vs 11%) in mortality at 1 year

Nebivolol
2128 patients, >70 years, admission in 12 months prior or LVEF<35% Nebivolol vs placebo 14% relative risk reduction (31.1 vs 35.3%) in death/HF hospitalisation at 21 months

Aldosterone antagonists
• Spironolactone
• Eplerenone

Spironolactone
1663 patients, severe heart failure, LVEF <35% Spironolactone 25 mg vs placebo 30% relative risk reduction (35 vs 46%) in death at 24 months

Eplerenone
2737 patients, NYHA II, LVEF <35% Eplerenone (up to 50 mg) vs placebo 37% RR reduction (18 vs 26%) in death/HF hosp at 21 months

Digoxin
6800 patients, LVEF < 45% Digoxin 250 μg daily vs placebo No effect on mortailty (OR 0.99), 6% fewer hospitalisations at 37 months

Inotropes
• Increase mortality but sometimes needed for decongestion and symptom relief.

Case 2 - management
• CRT

Cardiac resynchronisation therapy

Cardiac resynchronisation therapy

Case 2 - management
ECG’s pre & post

Case 2 - management

Case 2 - management
BP improved
Beta-blocker uptitrated to target
ACE-I increased to ½ target
Asymptomatic

Case 3
• Mrs J.H. – 86 years
• IHD – PCI’s to RCA & left main
• Develops heart failure with persistent atrial fibrillation
• Cardioversion & Sotalol, later Amiodarone

Case 3
• Syncope with pauses
• Pacemaker

Case 3

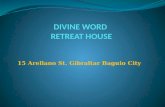
Case 4
• Mrs M.J. – 85 years
• Admitted with heart failure – NYHA FC III
• No angina
• Hypertension, hyperlipidaemia
• Long-term steroid therapy for PMR

Case 4
I
II
III
aVR
aVL
aVF
V1
V2
V3
V4
V5
V6
II
PID: 38311 06/14/2013 08:14:10 JONES, MIRIAM08/15/1927 DOB 85 years Female Dept
RoomTech SE
Rx:Dx:
Req MD:Ref MD: MEKEL, HARRIS
Rate 70PR 152QRSD 130QT 432QTc 466
--AXIS--P 62QRS -28T 93
Normal sinus rhythm with sinus arrhythmia, rate 70 bpmRight bundle branch blockMinimal voltage criteria for LVH, may be normal variantSeptal infarct , age undetermined
TJ
- ABNORMAL ECG - Unconfirmed Study 00// 00:0:
GE MAC35 25 mm/sec 10 mm/mV F 60~ 0.5 - 150 Hz


Case 4
• Medications:
– Candesartan, Rosuvastatin, Aspirin, Frusemide, ISMN, Carvedilol.

Coronary angiogram

Coronary angiogram

Case 4
• PCI to LAD, complicated by VF arrest, successfully resuscitated.





1 World Health Statistics, World Health Organization, 1995.
2 American Heart Association, 2002 Heart and Stroke Statistical Update.
HF Incidence and Prevalence
• Prevalence
– Worldwide, 22 million1
– United States, 5 million2
• Incidence
– Worldwide, 2 million new cases annually1
– United States, 500,000 new cases annually2
• HF afflicts 10 out of every 1,000 over age 65 in the U.S.2
• Extrapolating to regional Victoria
– 22,000

Prevalence of HF by Age and Gender
United States: 1988-94
0
2
4
6
8
10
Percent of
Population
20-24 25-34 35-44 45-54 55-64 65-74 75+
Males
Females
Source: NHANES III (1988-94), CDC/NCHS and the American Heart Association

Projections of prevalence of cardiovascular disease in 2010-2030 (USA)
Year
CAD
crude prevalence, %
HF crude prevalence, %
All CVD* crude prevalence, %
2010 8.0 2.8 36.9
2015 8.3 3.0 37.8
2020 8.6 3.1 38.7
2025 8.9 3.3 39.7
2030 9.3 3.5 40.5
% Change 16.6 25.0 9.9
*Includes hypertension, CAD, HF, stroke Heidenreich PA. Circulation 2011;123:933-944

30%
70%
Diastolic Dysfunction
Systolic Dysfunction
(EF < 40%) (EF > 40 %)
Left Ventricular Dysfunction • Systolic: Impaired contractility/ejection
– Approximately two-thirds of heart failure patients have systolic dysfunction1
• Diastolic: Impaired filling/relaxation
1 Lilly, L. Pathophysiology of Heart Disease. Second Edition p 200

Economic burden of
Chronic Heart Failure
Hospitalisation accounts for most CHF-associated costs
Stewart S, et al. Eur J Heart Fail 2002;4:361–71.
Primary Care
Outpatient referral
Drug treatment
Post-discharge outpatient visits
Hospital admissions
NHS data, United Kingdom
5% 6% 2%

Ivabradine

Logeart D, et al. Eur Heart J 2012;33 - Abstract Supplement 485
Elevated HR at discharge is a predictor of one-year mortality in HF patients (OFICA)
N=1658 (170 hospitals); median HR at discharge 71 bpm; 1 year mortality: 33%
41%

Audit of 100 CHF consecutive patients*, >50% had heart rate >70bpm
53.4% HR > 70 bpm 20.3% HR > 80 bpm
(N=20)
(N=54)
Cowie MR and Davidson L. Int J Clin Pract 2012; 66: 728 – 730
Pati
ents
Heart rate Reproduced with permission from M. Cowie,
Royal Brompton Hospital, UK
*sinus rhythm, EF < 40%, completed β-blocker uptitration [n=54] or intolerant of a β-blocker [n=20]

Analysis restricted to patients for whom the specialty of the first BB supply was known Source: Data from PBS 10% sample, Department of Human Services (CO8526)

Systolic Heart Failure treatment with
the If Inhibitor Ivabradine Trial
Swedberg K, et al. Lancet. 2010;376:875-85

Background
Elevated heart rate is associated with poor outcome in a number of
cardiovascular conditions including heart failure
Heart rate remains elevated in many heart failure patients despite
treatment by beta-blockers
Ivabradine is a novel heart rate-lowering agent acting by inhibiting the
If current in the sino-atrial node

Primary objective
To evaluate whether the If inhibitor ivabradine improves
cardiovascular outcomes in patients with
1.Moderate to severe chronic heart failure
2.Left ventricular ejection fraction ≤35%
3.Heart rate ≥70 bpm and
4.Optimised background therapy
Swedberg K, et al. Lancet. 2010;376:875-85

Patients and follow-up
Median study duration: 22.9 months; maximum: 41.7 months
6558 randomized
3268 to ivabradine 3290 to placebo
3264 analysed
1 lost to follow-up
3241 analysed
2 lost to follow-up
7411 screened
Excluded: 27 Excluded: 26
Swedberg K, et al. Lancet. 2010;376:875-85

Study endpoints
Primary composite endpoint
Cardiovascular death
Hospitalisation for worsening heart failure
Other endpoints
All-cause, CV and HF death
All-cause, CV and HF hospitalisation
Composite of CV death, hospitalisation for HF or non fatal MI
NYHA class / Patient & Physician Global Assessment
Swedberg K, et al. Lancet. 2010;376:875-85

Chronic HF background treatment
89 91
84
61
22
3
90 91
83
59
22
4
0
10
20
30
40
50
60
70
80
90
100
Beta-blockers ACEIs and/or ARBs
Diuretics Aldosterone antagonists
Digitalis ICD/CRT
Patients
(%)
Swedberg K, et al. Lancet. 2010;376:875-85
Ivabradine
Placebo
n= 3241
n=3264

Antialdost
antag, %
Diuretics,
%
BB,
%
ACEI/ARB, or
total, %
Baseline HR,
bpm
Study
61 84 89 91 80 SHIFT, 2010 (n=6505)
29 86 ST 82 79 SENIORS, 2005 (n=2128)
17 90 55 ACE+ ST 73 CHARM Added, 2003 (n=2548)
38 77 72 ST 71 HEAAL, 2009 (n=3846)
NA 85 7 ST 80 SOLVD 1991 (n=2569)
55 98 2 ST 80 CONSENSUS 1987 (n=253)
20 99 ST 96 83 COPERNICUS, 2001 (n=2289)
NA 99 ST 96 80 CIBIS II, 1999 (n=2647)
NA 91 ST 95 83 MERIT HF, 1999 (n=3991)
ST 100 10 94 81 RALES 1987 (n=253)
References supplied upon request.

Swedberg K, et al. Lancet. 2010;376:875-85
Mean heart rate reduction of 8 bpm
with ivabradine
0 2 weeks 1 4 8 12 16 20 24 28 32
90
80
70
60
50
67
75 75
80
64
Heart rate (bpm)
Ivabradine
Placebo
Months

Ivabradine reduced composite of CV death
and hospitalisation for worsening HF
Swedberg K, et al. Lancet. 2010;376:875-85
0 6 12 18 24 30
40
30
20
10
0
18% RRR
p<0.0001
Event Rate (%)
Lines
separate by 3
months
Ivabradine
Placebo
NNT = 26
Months
n=6505

Effect of ivabradine in pre-specified subgroups
Age <65 years ≥65 years
Sex Male Female
Beta-blockers No Yes
Aetiology of heart failure Non-ischaemic Ischaemic
NYHA class NYHA class II NYHA class III or IV
Diabetes No Yes
Hypertension No Yes
Baseline heart rate <77 bpm ≥77 bpm
Test for interaction
P = 0.029
1.5 1.0 0.5 Hazard ratio
Favours ivabradine Favours placebo
Swedberg K, et al. Lancet. 2010;376:875-85
NS
NS
NS
NS
NS
NS
NS
n=6505

Ivabradine reduced the composite of CV death
and hospitalisation for worsening HF in patients with a
heart rate >77bpm
Coralan Approved Product Information
n=3357

Treatment effect on the primary composite endpoint, its components
and secondary endpoints in patients with a heart rate >77bpm
Coralan Approved Product Information

Ekman et al EHJ 2011: 32; 2395

<72
72 to <75
75 to <80
80 to <87
≥87
No BB BB<25% BB ≥100%
Beta-blocker category
Baseline
HR category (bpm)
HR reduction according to B-blocker dose and HR category
HR reduction from
baseline to 28 days
with ivabradine*
(bpm)
BB 25-50% BB 50-100%
*Placebo corrected
No impact of BB dose
on HR reduction with ivabradine
Impact of baseline
HR on HR reduction
with ivabradine
Swedberg K, et al. J Am Coll Cardiol. 2012. n=6398

Recommended in Australian Heart Failure guidelines
TGA indication stipulates HR >77bpm

Adapted from reference 1 & 2. 1. Thollon C, et al. Br J Pharmacol. 2007;150:37-46. 2. DiFrancesco A, et al. Drugs. 2004;64:1757-1765.
3. Coralan Approved Product Information *Please refer to Coralan Approved Product Information before prescribing.
In the sinus node, the If current determines the slope of diastolic
depolarisation, the frequency of action potentials & thus heart rate1,2
Ivabradine - The first selective heart rate lowering agent 1,2,3

Surgery
• STITCH
• CABG
• Valve surgery

Management
• Device therapy
– ICD for poor LV function
– Cardiac resynchronisation therapy + ICD
• LV assist devices
• Cardiac transplantation



Cardiac resynchronisation therapy


Treatment Approach for the Patient with Heart Failure
Stage A
At high risk, no structural disease
Stage B
Structural heart disease,
asymptomatic
Stage D
Refractory HF requiring
specialized interventions
Therapy
• Treat Hypertension
• Treat lipid
disorders
• Encourage regular
exercise
• Discourage alcohol
intake
• ACE inhibition
Therapy
• All measures under
stage A
• ACE inhibitors in
appropriate
patients
• Beta-blockers in
appropriate
patients
Therapy
• All measures under
stage A
Drugs:
• Diuretics
• ACE inhibitors
• Beta-blockers
• Digitalis
• Dietary salt
restriction
Therapy
• All measures under
stages A,B, and C
• Mechanical assist
devices
• Heart
transplantation
• Continuous (not
intermittent) IV
inotropic infusions
for palliation
• Hospice care
Stage C
Structural heart disease with prior/current
symptoms of HF
Hunt, SA, et al ACC/AHA Guidelines for the Evaluation and Management of Chronic Heart Failure in the Adult, 2001

AF rate control

Effect of stopping
alcohol excess

The Vicious Cycle of Heart Failure Management
Chronic HF
MD’s Office
Emergency Room
Hospitalization
SOB
Weight
PO Lasix IV Lasix or
Admit
Diurese & Home

HFpEF
• Common – + 50%
• Increases with age,
• Commoner in women
• Commoner with history of hypertension
• Prognosis as poor as HFrEF
• Mainstay of treatment is diuretics and BP control

HFpEF

Remote monitoring

OSA & heart failure
• Commonly co-exist.
• Up to 30% of patients with heart failure have OSA

Refractory heart failure
• Sequential nephron blockade

Specific challenges
• Managing complications – AF, renal dysfunction
• Anticoagulation – Warfarin vs NOAC’s
• End-of-life care



Summary
• Heart failure is common and a large burden on healthcare
• Don’t forget the echocardiogram
• Look for reversible causes
• Fine-tune the medications
• Consider device therapy
• Involve the patient