

Consultancy Smith & Nephew Medtronic Research Support Smith & Nephew Hatton Research Institute GSH...
42
ZERO TOLERANCE: Transfusion Free Total Joint Replacement Mark A Snyder, MD Kathryn Eten RN, CCM Katy Loos, RN Orthopaedic Center of Excellence Good Samaritan Hospital Cincinnati, Ohio EPT 22, 2012 SABM 2012
-
Upload
mckenzie-milnes -
Category
Documents
-
view
217 -
download
4
Transcript of Consultancy Smith & Nephew Medtronic Research Support Smith & Nephew Hatton Research Institute GSH...

ZERO TOLERANCE: Transfusion Free Total Joint Replacement
Mark A Snyder, MDKathryn Eten RN, CCM
Katy Loos, RNOrthopaedic Center of Excellence
Good Samaritan Hospital Cincinnati, Ohio
SEPT 22, 2012 SABM 2012

Consultancy▪ Smith & Nephew▪ Medtronic
Research Support▪ Smith & Nephew▪ Hatton Research Institute GSH▪ IDEs
Bayer Boehringer Cadence
Co-management Arrangements▪ Good Samaritan Hospital
Consultancy▪ Smith & Nephew▪ Medtronic
Research Support▪ Smith & Nephew▪ Hatton Research Institute GSH▪ IDEs
Bayer Boehringer Cadence
Co-management Arrangements▪ Good Samaritan Hospital
DISCLOSUREDISCLOSURE

Good Samaritan HospitalTriHealth System

Centralization
Obamacare
Standardization
The Solution:Consumer (patient)-
Driven Care
Consumer-driven insurers
Consumer-friendly hospitals
Consumer-friendly employers
Consumer-supportive laws
Consumer-driven market
TRANSPARENCY!“Americans Favor Transparency in Medicare, Physician Changes,” May 2, 2006, www.zogby.com

“How physicians can change the
future of health care.”Porter ME, Teisberg EO. JAMA
2007;297(10):1103.
PRINCIPLES:*Goal is value for
patients*Organization around
conditions and cycles of care
*Measuring of results, risk-adjusted outcomes, and costs
Returning medicine to its proper focus:Enabling health and providing effective care. “ZERO”, TJA, REGISTRY* * *

A powerful approach to cost reduction in health care!
“Adverse events are associated with significantly increased hospitalization costs and appropriate evidence-based interventions are justified to minimize AEs.”
Kondalsamy-Chennakesavan S, et al. Gynecol Oncol. 2011;121(1):70 “Risk-adjusted total, Medicare, and beneficiary healthcare
costs were significantly higher for both THR and TKR patients with VTE.”
Boser O, et al. Curr Med Res Opin. 2011;27(2):423
Radically reduce adverse events! Invest in initiatives to apply best evidence
literature to care processes. Believe that real change can happen and
that it is good for all stakeholders! PATIENT SAFETY!

Top 10 Most Costly, Frequent Medical Complications In the US
http://www.soa.org/files/pdf/research-econ-measurement.pdf
Error type
% of injuries that are errors
Count of injuries (2008)
Count of Errors (2008)
Medical cost per Error
In Hospital Mortality Cost per Error
STD Cost Error
Total Cost per Error
Total Cost of Error Millions
Pressure Ulcer (Medicare Never Event)
>90%394,66
9374,96
4$8,730 $1,133 $425
$10,288
$3858
Postoperative infection
>90% 265,995
252,695
$13,312
$-$1,23
6$14,54
8$3,676
Mechanical complication of device, implant or graft
10-35%268,35
360,380
$17,709
$426 $636$18,77
1$1,133
Postlaminectomy syndrome 10-35%
505,881
113,823
$8,739 $-$1,12
4$9,863 1,123
Hemorrhage complicating a procedure
35-65%156,43
378,216 $8,665 $2,838 $778
$12,272
$960
Infection following infusion, injection, transfusion, vacc
>90%9,321 8,855
$63,911
$14,172 $-$78,08
3$691
Pneumothorax 35-65%51,119 25,256
$22,256
$-$1,87
6$24,13
2$617
Infection due to central venous catheter
>90% 7,434 7,062$83,36
5$- $-
$83,365
$589
Other complications of internal biological, synthetic
<10%535,66
626,783
$14,851
$1,768 $614$17,23
3$462
Ventral hernia w/o mention of obstruction or gangrene
10-35%239,15
653,810 $6,359 $260
$1,559
$8,178 $440

Why Zero Tolerance?
It is the right thing to do!

A New Day Is Coming!
CMS in cooperation with the AAOS Dry-run September 2012 National transparency 2013 via
compare.gov RSCR and RARR What are the targets?
▪ Mechanical complication readmission 90 days▪ PJI 90 days▪ SSI 90 days▪ Surgical site bleeding, PE, death 30 days▪ AMI, pneumonia, sepsis/septicemia 7 days

The Truth Hurts!
RARR 5.7% nationalRSCR 3.6%GSH 5.0% and 3.6% respectively
Years 2008 to 2010

Zero in on ZeroClinical Focus
30 day readmission
Patient FallsDissatisfaction
Poor Discharge Handoff
Catheter Assoc UTI
Infected THA/TKADeath from VTE
Ineffective Pain Management Transfusions
Strive For 0%
Dislocation
Two Things!
No “silver bullet”
Mountain climbing

Using The Evidence
Causal analysis Heget JR, et al. Jt Comm J Qual Improv 2002;28(12):660 Nicolini D, et al. J Health Serv Res Policy 2011;16 Suppl 1:34
BEFORE…DURING…AFTER Randomized clinical trials Meta-analyses Cochrane reviews Available clinical practice guidelines
(CPG) BEST PRACTICE PROPOSALS (BPP)
Barbieri A, et al. BMC Med 2009;7:32 Rotter T, et al. Cochrane Database Syst Rev 2010;
(3):CD006632

For ExampleReducing Blood Transfusions
BEFORE: uncorrected pre-op anemia
DURING: unfettered bleeding and no inhibition of fibrinolysis
AFTER: mandated strong VTE chemoprophylaxis
Evidence: STRONG, MODERATE, WEAK, INCONCLUSIVE

BPPReducing Blood Transfusions
BEFORE DURING AFTERRecognition of anemia with CBC more than 4 weeks prior to surgery (S)
Regional anesthesia (M)
Avoidance of strong VTE chemoprophylaxis in low risk TKA patients (S)
Correction of HgB <13 in males and <12 in females with erythropoietin and iron supplements (S)
Hypotensive anesthesia for those requiring GA
Lovenox 40 mg daily in TKA. INR targets near 1.5 for coumadinized patients (M)
Referral to hematology if HgB < 10
Pre-op TXA given 15 mg/kg 15 minutes before incision (S)
Transfusion triggers 7/21 unless cardiac symptoms unstable (S)
Avoidance of autologous donation (M)
Decreased tourniquet time, bipolar cautery (I)
IV fluid correction of hypotension and mild postural changes (I)
Drain avoidance (M)

Teamwork is required to enable Zero in on Zero
SurgeonsStaffAdministra
tionPatients
and family

Eisenhower Strategy
Get broad buy-inCollegially help everyone move in the
same direction to achieve a solution!Hospital credentialing:
▪ Docs must participate in the Registry▪ Docs may use the OCE marketing plan IF they
follow established CPGs and new BPP protocols where CPGs do not yet exist
▪ While docs must decide what is best for their individual patients, disagreements with CPGs and BPP protocols must be in writing

Salida JA, et al. Preoperative hemoglobin levels and the need for transfusion after prosthetic hip and knee surgery: predictive factors. JBJS 2002 84:216
Bong MR, et al. Risks associated with blood transfusion after total knee arthroplasty. J Arthroplasty 2004;19:281
REMEMBER THAT THE TWO LEADING CAUSES OF BLEEDING SUFFICIENT TO REQUIRE TRANSFUSION ARE 1) PRE-OP ANEMIA AND 2) POTENT ANTICOAGULANTS

Despite a low transfusion rate, 20% TKA/THA patients exhibited
preoperative anemia
< 13 gm/L for men and < 12 gm/L for women
Patients unaware of anemia since fatigue is the predominant symptom.
PCP acceptance of anemia since surgical options not in their usual treatment algorithms.
Patients with severe OA of the hip and/or knee are more likely to undergo TJA if this option is discussed with their PCP, but few patients experience this conversation!
Schonberg MA, et al. J Am Geriatr Soc 2009;57(1):82

Total Blood Transfusions
Zero BPP designed and trialed

2009
AVG
2010
AVG
Jan
11Fe
b 11
Mar
11
Apr 1
1M
ay 1
1Ju
n 11
Jul-1
1Aug
-11
Sep-1
1O
ct-1
1Nov
-11
Dec-1
1Ja
n-12
Feb-
12M
ar-1
2
0.00%
2.00%
4.00%
6.00%
8.00%
10.00%
12.00%
14.00%
16.00%
18.00%
20.00%
Elective Hip and Knee Arthroplasty RBC % Trans-
fused
% Transfused
Linear (% Transfused)

In 2010, transfusion cost for 321
allogenic and autologous units was $321,000.
In 2011 and 2012, we have already
saved over$500,000!
Shander A, et al. Transfusion 2010;50(4):753

Orthopaedics was an area of practice ready for change!
Collaborative group with strong leadership
Supportive multidisciplinary teamZero in on Zero initiative with
strong body of evidence to support best practice initiatives
High usage of blood productsWide variation in blood
management practices

ORTHOPAEDICS
Example of physician blinding for elective total hip arthroplasties
A B C D E F G H I J K L M N O P Q R S0.00%
20.00%
40.00%
60.00%
80.00%
100.00%
120.00%
Hip Cases With Transfusions
% Hip Cases With Transfu-sions By Doctor

ORTHOPAEDICS
Blinded physician-specific transfusion data Presented at Section meeting
Extensive literature review for evidence based best practice New practice initiatives for pre, intra, and post-
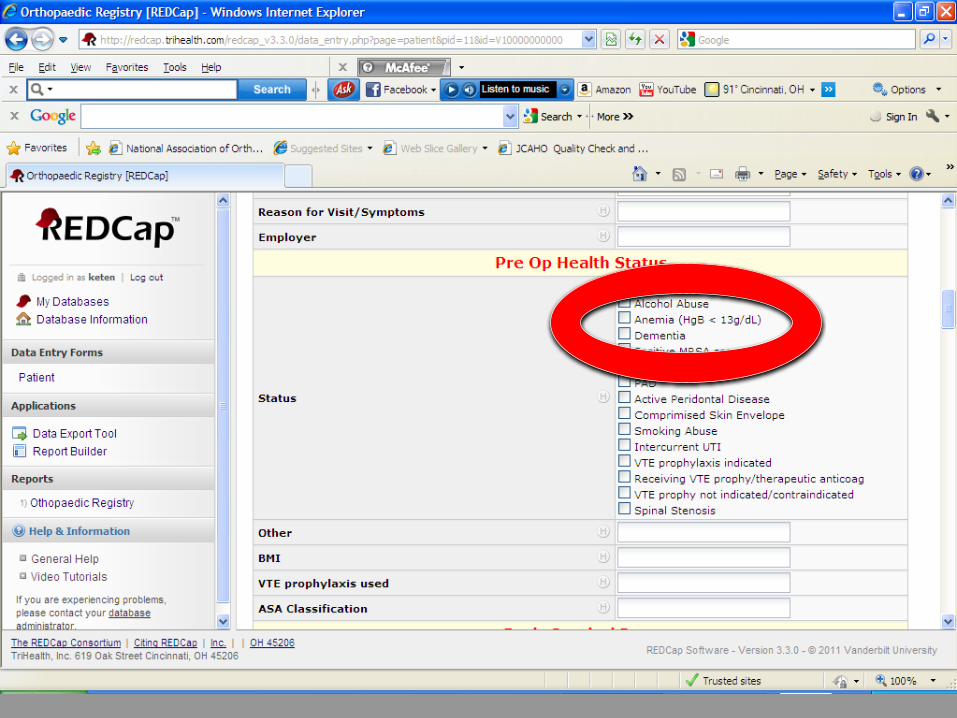
operative conservation Amended order sets to reflect changes Established Anemia Clinic
Orthopedic Center of Excellence (OCE) Quality measure: Preoperative anemia
Established metrics Posted on OCE dashboard

Pre-Surgical Anemia Protocol

Anemia Prevention
Anemia Clinic with automatic treatment of patients by hematologist
Education of residents, and individual services Go to each section meeting and deliver the
message that is pertinent to their practice Let other services know about the
successes gained by others Empower staff nurses as your advocates

Challenges: The Patient
Lack of knowledge about anemia
Overwhelmed when notified of anemic status
Feared surgery cancelation
Did not want to travel for additional doctor visits
Challenges: Physicians
Orthopedic surgeons tried to treat patients on a case by case basis only to meet resistance from PCP and third party payers.
PCP’s feared loss of control over patient care if patients were referred to a hematologist for mild anemia.
Speculation that the new process would delay surgery.
Communication gaps

Challenges: Hospital Process
Ownership of clinic process
Clinical exam space Departments wanted
new business but sometimes resisted implementation
Multi dept involvement
Verbal and electronic communication gaps between departments

How can a total joint registry enable blood conservation success?
Prospective, consecutive tracking of all total hip and knee arthroplasties enables physicians to see their own results in comparison with blood conservation best practices, and then choose to change their own practices.
The registry has “before/during/after” data that enables problem solving.

Patient ConsentIRB Approved

1)Early warning2)Influence MD behavior3)Decrease AE cost, M&M,
revTJA volume
REGISTRY BENEFITS!



August 1, 2011 to Sept 21, 2012405TJATotal AE 1.73%Transfusion 0%SSI 0%RSCR 0.49%RARR 0.49%
1/10 THE RAT
E
MAS DATA

BEFORE▪ Anemia detection▪ Anemia correction
DURING▪ Novel blood loss prevention▪ TXA administration▪ Avoidance of surgical drains
AFTER▪ TXA effect▪ Transfusion criteria 7/21▪ IV saline for minor postural hypotension and
lack if vigor
HOW WAS THIS ACCOMPLISHED?
TAKEHOME
MESSAGES
Part of a regional solution for an upcoming patient access crisis
Stellar safety and quality are win-wins for patients, providers, hospitals and society.
Physician leadership is critical to creating and sustaining patient-centered solutions for adverse event challenges in hip and knee replacement.
THE PATH
Center of Excellence
Zero in on Zero safety and quality initiative
Initiative deployment
Physician credentialing agreement
Registry
ZERO IN ON ZERO
Sir Winston Churchill Sir Winston Churchill
“SUCCESS IS NOT FINAL,FAILURE IS NOT FATAL: IT ISTHE COURAGE TO CONTINUE
THAT COUNTS.”


















