Constant Volume of the Human Lens and Decrease in...
9
Constant Volume of the Human Lens and Decrease in Surface Area of the Capsular Bag during Accommodation: An MRI and Scheimpflug Study Erik A. Hermans, Petra J. W. Pouwels, Michiel Dubbelman, Joost P. A. Kuijer, Rob G. L. van der Heijde, and Rob M. Heethaar PURPOSE. A change in surface area of the capsular bag and a change in volume of the lens can indicate whether a change in the shape of the lens during accommodation is due to the compressibility or the elasticity of the lens material. METHODS. 3D magnetic resonance imaging (MRI) was used to image the complete shape of the lens in a group of five healthy subjects between 18 and 35 years of age. A parametric repre- sentation of the cross-sectional shape was fitted to the edges of the lens, which were determined with a Canny edge filter. Based on a partition of the lens into eight parts, the parametric shape makes it possible to calculate the mean cross-sectional area, the volume, and the surface area as a function of accom- modation. Corrected Scheimpflug imaging was used to validate the results obtained with MRI. RESULTS. No significant difference in central anterior and pos- terior radius of curvature and thickness was found between the MRI and Scheimpflug measurements. In accordance with the Helmholtz accommodation theory, a decrease in the anterior and posterior radius of curvature and equatorial diameter and an increase in lens thickness occurred with accommodation. During accommodation, the mean cross-sectional area in- creased and the surface area decreased. However, no signifi- cant change in lens volume was found. CONCLUSIONS. The preservation of lens volume implies that the internal human lens material can be assumed to be incompress- ible and is undergoing elastic deformation. Furthermore, the change in surface area indicates that the capsular bag also undergoes elastic deformation. (Invest Ophthalmol Vis Sci. 2009;50:281–289) DOI:10.1167/iovs.08-2124 D uring accommodation, the thickness of the lens increases and the radius of curvature of the anterior and posterior central area decreases, resulting in an increase in optical power. According to the Helmholtz accommodation theory, 1 this deformation is caused by the ciliary muscle release of zonular tension. It is not exactly known whether the deforma- tion of the lens is due to the elasticity or the compressibility of lens material. A change in surface area (SA) of the capsular bag could indicate that the elasticity of the capsular bag plays an impor- tant role in accommodation. On the other hand, a change in lens volume (VOL) could indicate that decompression of the internal lens material is responsible for the accommodative changes. The objective of the present study was to determine the VOL of the lens and SA of the capsular bag and to investi- gate whether there is a change in these quantities with accom- modation. Therefore, the 3D geometry of the human lens was measured in vivo in a group of five healthy subjects. Further- more, knowledge about human lens VOL and strain in the capsular bag could be used for refilling the capsular bag with a viscoelastic material to restore accommodation. 2 Different methods have been applied to determine in vitro the VOL as a function of age. 3–5 In vivo, Strenk, et al. 6 used 2D magnetic resonance imaging (MRI) to measure the cross-sec- tional lens geometry. In one axial MRI slice the changes in thickness and equatorial diameter of the lens as a function of two different accommodation stimuli were measured in 25 healthy subjects. Furthermore, in another study, Strenk et al. 7 observed an increase in the cross-sectional area (CSA) of 25 human lenses, and they suggested that the lens may be com- pressed in the unaccommodated state. However, a change in the CSA does not necessarily imply a change in lens VOL. 8 In vitro, Gerometta et al. 9 placed bovine lenses in a stretching device, and based on lateral photographs of the CSA, the center of mass and VOL were determined during stretching. With accommodation, they measured an increase of 8% in bovine lens VOL. Based on data from the literature, they simulated a human lens during accommodation and expected that the human lens would undergo an increase of approximately 3% in lens VOL. It was suggested that compression of the lens mate- rial could play an important role in accommodation. However, the change in VOL of the human lens has not yet been mea- sured in vivo as a function of accommodation. In vitro, Fisher 10 developed a method with which to esti- mate the energy released by the anterior part of the lens capsule during accommodation. He concluded that the elastic- ity of the surface of the capsule plays a major role in the loss of accommodation. In studies conducted in vitro, Krag et al. 11 Krag and Andreassen, 12 and Heistand et al. 13 also determined the mechanical properties of the human capsule, but no in vivo measurement of strain during accommodation has ever been performed. Chien et al. 14 used various analytical functions to describe the cross-sectional shape of the human crystalline lens. Using polar coordinates, they found that a parameterization with cosines appeared to result in the best fit for the surface of the human lens. Kasprzak 15 proposed an analytical function that describes the complete axisymmetric lens profile in an accom- modated and a disaccommodated state. However, both de- scriptions contain many parameters with no physical meaning that have to be fit simultaneously. To compare Scheimpflug measurements of the central part of the lens with MRI mea- surements of the central and peripheral part of the lens, it is necessary to have a parametric geometry that can describe both parts separately. From the Department of Physics and Medical Technology, VU University Medical Center, Amsterdam, The Netherlands. Supported by SenterNovem Grant IS 043081. Submitted for publication April 4, 2008; revised May 7, 2008; accepted October 27, 2008. Disclosure: E.A. Hermans, None; P.J.W. Pouwels, None; M. Dubbelman, None; J.P.A. Kuijer, None; R.G.L. van der Heijde, None; R.M. Heethaar, None The publication costs of this article were defrayed in part by page charge payment. This article must therefore be marked “advertise- ment” in accordance with 18 U.S.C. §1734 solely to indicate this fact. Corresponding author: Erik A. Hermans, Department of Physics and Medical Technology, VU University Medical Center, Postbus 7057, 1007 MB Amsterdam, The Netherlands; [email protected]. Investigative Ophthalmology & Visual Science, January 2009, Vol. 50, No. 1 Copyright © Association for Research in Vision and Ophthalmology 281 Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/932956/ on 05/03/2018
Transcript of Constant Volume of the Human Lens and Decrease in...

Constant Volume of the Human Lens and Decrease inSurface Area of the Capsular Bag duringAccommodation: An MRI and Scheimpflug Study
Erik A. Hermans, Petra J. W. Pouwels, Michiel Dubbelman, Joost P. A. Kuijer,Rob G. L. van der Heijde, and Rob M. Heethaar
PURPOSE. A change in surface area of the capsular bag and achange in volume of the lens can indicate whether a change inthe shape of the lens during accommodation is due to thecompressibility or the elasticity of the lens material.
METHODS. 3D magnetic resonance imaging (MRI) was used toimage the complete shape of the lens in a group of five healthysubjects between 18 and 35 years of age. A parametric repre-sentation of the cross-sectional shape was fitted to the edges ofthe lens, which were determined with a Canny edge filter.Based on a partition of the lens into eight parts, the parametricshape makes it possible to calculate the mean cross-sectionalarea, the volume, and the surface area as a function of accom-modation. Corrected Scheimpflug imaging was used to validatethe results obtained with MRI.
RESULTS. No significant difference in central anterior and pos-terior radius of curvature and thickness was found between theMRI and Scheimpflug measurements. In accordance with theHelmholtz accommodation theory, a decrease in the anteriorand posterior radius of curvature and equatorial diameter andan increase in lens thickness occurred with accommodation.During accommodation, the mean cross-sectional area in-creased and the surface area decreased. However, no signifi-cant change in lens volume was found.
CONCLUSIONS. The preservation of lens volume implies that theinternal human lens material can be assumed to be incompress-ible and is undergoing elastic deformation. Furthermore, thechange in surface area indicates that the capsular bag alsoundergoes elastic deformation. (Invest Ophthalmol Vis Sci.2009;50:281–289) DOI:10.1167/iovs.08-2124
During accommodation, the thickness of the lens increasesand the radius of curvature of the anterior and posterior
central area decreases, resulting in an increase in opticalpower. According to the Helmholtz accommodation theory,1
this deformation is caused by the ciliary muscle release ofzonular tension. It is not exactly known whether the deforma-tion of the lens is due to the elasticity or the compressibility oflens material.
A change in surface area (SA) of the capsular bag couldindicate that the elasticity of the capsular bag plays an impor-
tant role in accommodation. On the other hand, a change inlens volume (VOL) could indicate that decompression of theinternal lens material is responsible for the accommodativechanges. The objective of the present study was to determinethe VOL of the lens and SA of the capsular bag and to investi-gate whether there is a change in these quantities with accom-modation. Therefore, the 3D geometry of the human lens wasmeasured in vivo in a group of five healthy subjects. Further-more, knowledge about human lens VOL and strain in thecapsular bag could be used for refilling the capsular bag with aviscoelastic material to restore accommodation.2
Different methods have been applied to determine in vitrothe VOL as a function of age.3–5 In vivo, Strenk, et al.6 used 2Dmagnetic resonance imaging (MRI) to measure the cross-sec-tional lens geometry. In one axial MRI slice the changes inthickness and equatorial diameter of the lens as a function oftwo different accommodation stimuli were measured in 25healthy subjects. Furthermore, in another study, Strenk et al.7
observed an increase in the cross-sectional area (CSA) of 25human lenses, and they suggested that the lens may be com-pressed in the unaccommodated state. However, a change inthe CSA does not necessarily imply a change in lens VOL.8 Invitro, Gerometta et al.9 placed bovine lenses in a stretchingdevice, and based on lateral photographs of the CSA, the centerof mass and VOL were determined during stretching. Withaccommodation, they measured an increase of 8% in bovinelens VOL. Based on data from the literature, they simulated ahuman lens during accommodation and expected that thehuman lens would undergo an increase of approximately 3% inlens VOL. It was suggested that compression of the lens mate-rial could play an important role in accommodation. However,the change in VOL of the human lens has not yet been mea-sured in vivo as a function of accommodation.
In vitro, Fisher10 developed a method with which to esti-mate the energy released by the anterior part of the lenscapsule during accommodation. He concluded that the elastic-ity of the surface of the capsule plays a major role in the loss ofaccommodation. In studies conducted in vitro, Krag et al.11
Krag and Andreassen,12 and Heistand et al.13 also determinedthe mechanical properties of the human capsule, but no in vivomeasurement of strain during accommodation has ever beenperformed.
Chien et al.14 used various analytical functions to describethe cross-sectional shape of the human crystalline lens. Usingpolar coordinates, they found that a parameterization withcosines appeared to result in the best fit for the surface of thehuman lens. Kasprzak15 proposed an analytical function thatdescribes the complete axisymmetric lens profile in an accom-modated and a disaccommodated state. However, both de-scriptions contain many parameters with no physical meaningthat have to be fit simultaneously. To compare Scheimpflugmeasurements of the central part of the lens with MRI mea-surements of the central and peripheral part of the lens, it isnecessary to have a parametric geometry that can describeboth parts separately.
From the Department of Physics and Medical Technology, VUUniversity Medical Center, Amsterdam, The Netherlands.
Supported by SenterNovem Grant IS 043081.Submitted for publication April 4, 2008; revised May 7, 2008;
accepted October 27, 2008.Disclosure: E.A. Hermans, None; P.J.W. Pouwels, None; M.
Dubbelman, None; J.P.A. Kuijer, None; R.G.L. van der Heijde,None; R.M. Heethaar, None
The publication costs of this article were defrayed in part by pagecharge payment. This article must therefore be marked “advertise-ment” in accordance with 18 U.S.C. §1734 solely to indicate this fact.
Corresponding author: Erik A. Hermans, Department of Physicsand Medical Technology, VU University Medical Center, Postbus 7057,1007 MB Amsterdam, The Netherlands; [email protected].
Investigative Ophthalmology & Visual Science, January 2009, Vol. 50, No. 1Copyright © Association for Research in Vision and Ophthalmology 281
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/932956/ on 05/03/2018
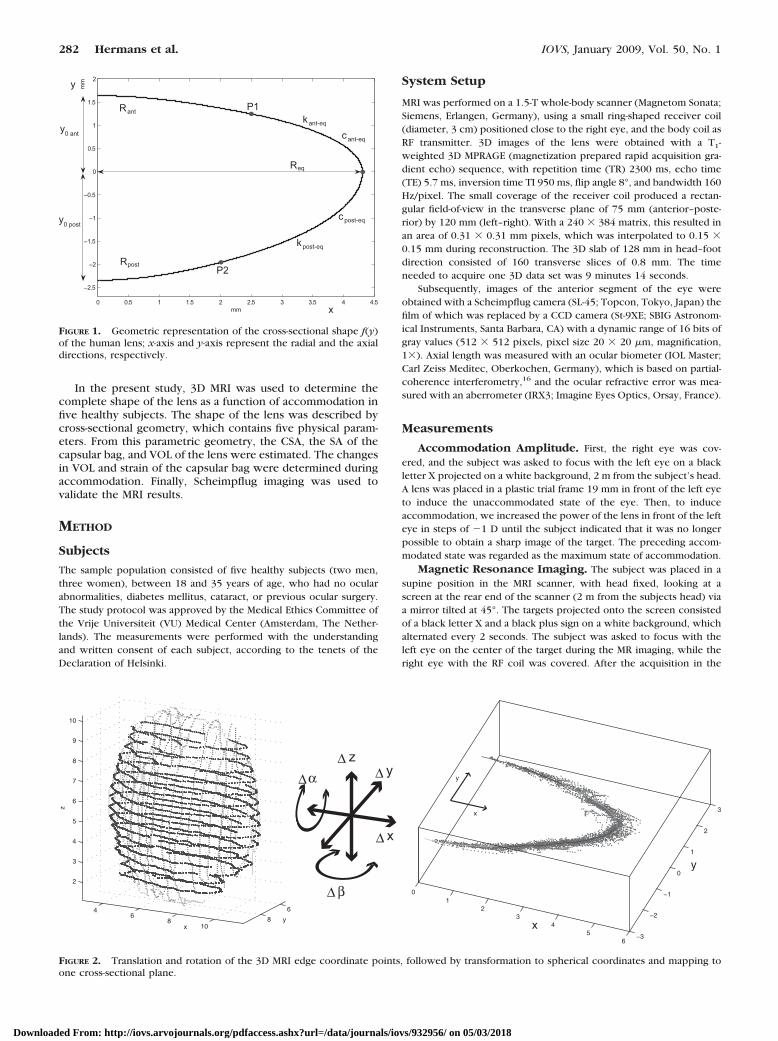
In the present study, 3D MRI was used to determine thecomplete shape of the lens as a function of accommodation infive healthy subjects. The shape of the lens was described bycross-sectional geometry, which contains five physical param-eters. From this parametric geometry, the CSA, the SA of thecapsular bag, and VOL of the lens were estimated. The changesin VOL and strain of the capsular bag were determined duringaccommodation. Finally, Scheimpflug imaging was used tovalidate the MRI results.
METHOD
Subjects
The sample population consisted of five healthy subjects (two men,three women), between 18 and 35 years of age, who had no ocularabnormalities, diabetes mellitus, cataract, or previous ocular surgery.The study protocol was approved by the Medical Ethics Committee ofthe Vrije Universiteit (VU) Medical Center (Amsterdam, The Nether-lands). The measurements were performed with the understandingand written consent of each subject, according to the tenets of theDeclaration of Helsinki.
System Setup
MRI was performed on a 1.5-T whole-body scanner (Magnetom Sonata;Siemens, Erlangen, Germany), using a small ring-shaped receiver coil(diameter, 3 cm) positioned close to the right eye, and the body coil asRF transmitter. 3D images of the lens were obtained with a T1-weighted 3D MPRAGE (magnetization prepared rapid acquisition gra-dient echo) sequence, with repetition time (TR) 2300 ms, echo time(TE) 5.7 ms, inversion time TI 950 ms, flip angle 8°, and bandwidth 160Hz/pixel. The small coverage of the receiver coil produced a rectan-gular field-of-view in the transverse plane of 75 mm (anterior–poste-rior) by 120 mm (left–right). With a 240 � 384 matrix, this resulted inan area of 0.31 � 0.31 mm pixels, which was interpolated to 0.15 �0.15 mm during reconstruction. The 3D slab of 128 mm in head–footdirection consisted of 160 transverse slices of 0.8 mm. The timeneeded to acquire one 3D data set was 9 minutes 14 seconds.
Subsequently, images of the anterior segment of the eye wereobtained with a Scheimpflug camera (SL-45; Topcon, Tokyo, Japan) thefilm of which was replaced by a CCD camera (St-9XE; SBIG Astronom-ical Instruments, Santa Barbara, CA) with a dynamic range of 16 bits ofgray values (512 � 512 pixels, pixel size 20 � 20 �m, magnification,1�). Axial length was measured with an ocular biometer (IOL Master;Carl Zeiss Meditec, Oberkochen, Germany), which is based on partial-coherence interferometry,16 and the ocular refractive error was mea-sured with an aberrometer (IRX3; Imagine Eyes Optics, Orsay, France).
Measurements
Accommodation Amplitude. First, the right eye was cov-ered, and the subject was asked to focus with the left eye on a blackletter X projected on a white background, 2 m from the subject’s head.A lens was placed in a plastic trial frame 19 mm in front of the left eyeto induce the unaccommodated state of the eye. Then, to induceaccommodation, we increased the power of the lens in front of the lefteye in steps of �1 D until the subject indicated that it was no longerpossible to obtain a sharp image of the target. The preceding accom-modated state was regarded as the maximum state of accommodation.
Magnetic Resonance Imaging. The subject was placed in asupine position in the MRI scanner, with head fixed, looking at ascreen at the rear end of the scanner (2 m from the subjects head) viaa mirror tilted at 45°. The targets projected onto the screen consistedof a black letter X and a black plus sign on a white background, whichalternated every 2 seconds. The subject was asked to focus with theleft eye on the center of the target during the MR imaging, while theright eye with the RF coil was covered. After the acquisition in the
0 0.5 1 1.5 2 2.5 3 3.5 4 4.5
–2.5
–2
–1.5
–1
–0.5
0
0.5
1
1.5
2
mm
mm
y
antR
postR
Req
P1
P2
post-eqc
ant-eqcant-eqk
post-eqk
y
x
0 ant
y0 post
FIGURE 1. Geometric representation of the cross-sectional shape f(y)of the human lens; x-axis and y-axis represent the radial and the axialdirections, respectively.
46
810
6
8
2
3
4
5
6
7
8
9
10
yx
z
12
34
56
−3
−2
−1
0
1
2
3
0
x
y
x
y∆
x
y
α
β
z
∆
∆
∆∆
FIGURE 2. Translation and rotation of the 3D MRI edge coordinate points, followed by transformation to spherical coordinates and mapping toone cross-sectional plane.
282 Hermans et al. IOVS, January 2009, Vol. 50, No. 1
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/932956/ on 05/03/2018

unaccommodated state, the lens positioned in the plastic trial frame infront of the left eye was changed to induce accommodation. A 3D MRIacquisition of the right eye was obtained in the unaccommodated andthe maximum accommodated states.
Scheimpflug Imaging. The Scheimpflug image of the lens wascaptured by dilating the pupil of the right eye of each subject with twodrops of 5% phenylephrine HCl. The same two accommodative statesas for the MRI examination were again created, using a trial frame andlenses in front of the left eye. The subject was instructed to fixate ona fixation light in the Scheimpflug camera, whereas the slit of thecamera was aligned along the optical axis of the right eye. The subjectwas then asked to fixate with the left eye on a Maltese star, the positionof which could be adjusted horizontally and vertically by remotecontrol until the subject reported that the fixation light of the Sche-impflug camera was superimposed on the center of the Maltese star. At
this point, the internal fixation light of the camera was turned off, andthe subject was asked to focus on the Maltese star while three imageswere obtained per accommodative state.
Aberrometry. To determine the accommodative response, wemeasured the refractive error of the right eye of each subject with theaberrometer. The same accommodative states were created as for theMRI and Scheimpflug measurements, with different lenses used infront of the left eye and a Maltese star as the fixation target. Afteralignment of the internal fixation light in the aberrometer with theMaltese star, the internal fixation light was turned off and the refractiveerror of the right eye was measured. Using a fixed 3-mm pupil, wetransferred the effective refractive error in both accommodative statesto accommodative response at the spectacle plane.
Postprocessing
The shape of the lens was described as a parametric curve with aminimal set of parameters that had a physical meaning. It was assumedthat the curve describing the cross-sectional shape of the lens and itsderivative are continuous and that the derivative in axial direction is 0at the equator and the radial derivative is 0 at the poles. Figure 1illustrates the geometric model that consists of anterior and posteriorparabolas representing the central area of the lens
x � �2�y � y0ant�
cantif x � 2.5 mm and y � 0 mm with cant �
1
Rant
(1)
x � �2�y � y0post�
cpostif x � 2.0 mm and y � 0 mm with cpost �
1
Rpost
(2)
with R as the central radius of curvature and (0, y0) as the apexposition (all units in millimeters).
With Scheimpflug imaging, the posterior central area of the lens isless visible than the anterior central area. Therefore, it is possible to fitthe anterior parabola at an aperture of 5 mm and the posterior parabolaat an aperture of only 4 mm.
The ratio between anterior and posterior thicknesses, with respectto the equatorial plane and the total thickness (TT), was defined as
−4 −3 −2 −1 0 1 2 3 4 −2−10 1
−4
−3
−2
−1
0
1
2
3
4
yx
z
FIGURE 3. Canny edge data points of the 20-year-old subject dividedinto eight parts.
MRI measurement
R R TT ratio R
^ ^ ^ ^ ^ant post eq
∆x ∆y ∆z ∆α ∆β ^ ^ ^ ^ ^
I
I
R R TT ^ ^ ^
ant post
III
III Scheimpflug measurement
estimation of axisymmetric shape parameters
estimation of orientation estimation of central parameters
estimation of shape parameters with fixed
TT and ratio
II
eq ^ ^ ^
ant post R R R
divide the MRI data intoeight parts
CSA SA VOL
^ ^ ^ II calculation of total
(calculated per part and summed)
R R TT ^ ^ ^
ant post
III validation ofcentral parameters
8 LENS PARTS
ASSUMING AXISYMMETRY
FIGURE 4. Estimation scheme forthe MRI and Scheimpflug measure-ments.
IOVS, January 2009, Vol. 50, No. 1 Constant Volume of the Human Lens during Accommodation 283
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/932956/ on 05/03/2018
ratio � � y0ant
y0post� (3)
TT � �y0ant� � �y0post�. (4)
The two curves in the periphery that closed the lens were formedby conics, which can be described by the following formulas
x � Req �cant�eq y2
1 � �1 � kant�eqcant�eq y2if x � 2.5 mm and y � 0 mm
(5)
x � Req �cpost�eqy
2
1 � �1 � kpost�eqcpost�eq y2if x � 2.0 mm and y � 0 mm
(6)
with Req as the equatorial radius, c as the curvature, and k as theasphericity of the conic.
To guarantee a continuous function, as well as a continuous deriv-ative, we constrained the four parameters of the conics to the follow-ing expressions:
cant�eq �Req � x1
y1�cant�Req � x1�x1 � y1�(7)
kant�eq �y1�2cant�Req � x1�x1 � y1�
�Req � x1�2 (8)
cpost�eq �Req � x2
y2�cpost�Req � x2�x2 � y2�(9)
kpost�eq �y2�2cpost�Req � x2�x2 � y2�
�Req � x2�2 (10)
with P1 (x1 � 2.5 mm, y1) and P2 (x2 � 2.0 mm, y2) as the position ofthe interception points between the anterior and posterior centralparabolic and the conic curves in the periphery.
CSA, SA, and VOL Calculation. With f(y) as the axisymmetriccross-sectional curve as a function of the axial position (y) with respectto the axis of rotation, it is possible to compute the CSA, the SA of thecapsular bag, and the VOL of the lens17
CSA � 2�y0post
y0ant
f�y�dy (11)
SA � 2��y0post
y0ant
f�y�� f ��y�2 � 1dy (12)
VOL � ��y0post
y0ant
f�y�2dy. (13)
The integrals in equations 11 and 13 were computed analytically, butthe integral in equation 12 had to be approximated numerically.
Step I: Parameter Estimation from MR Images Assum-ing Axisymmetry. The MR images were linearly interpolated to aspatial resolution of 0.1 � 0.1 � 0.1 mm, to determine the edge of thelens with subpixel accuracy. To determine the lens edges, a Cannyedge filter18 with automatic thresholding was applied to the interpo-lated MRI slices every 0.5 mm in the three principal directions. In everyCanny edge–filtered slice, chains of edge points were selected manu-
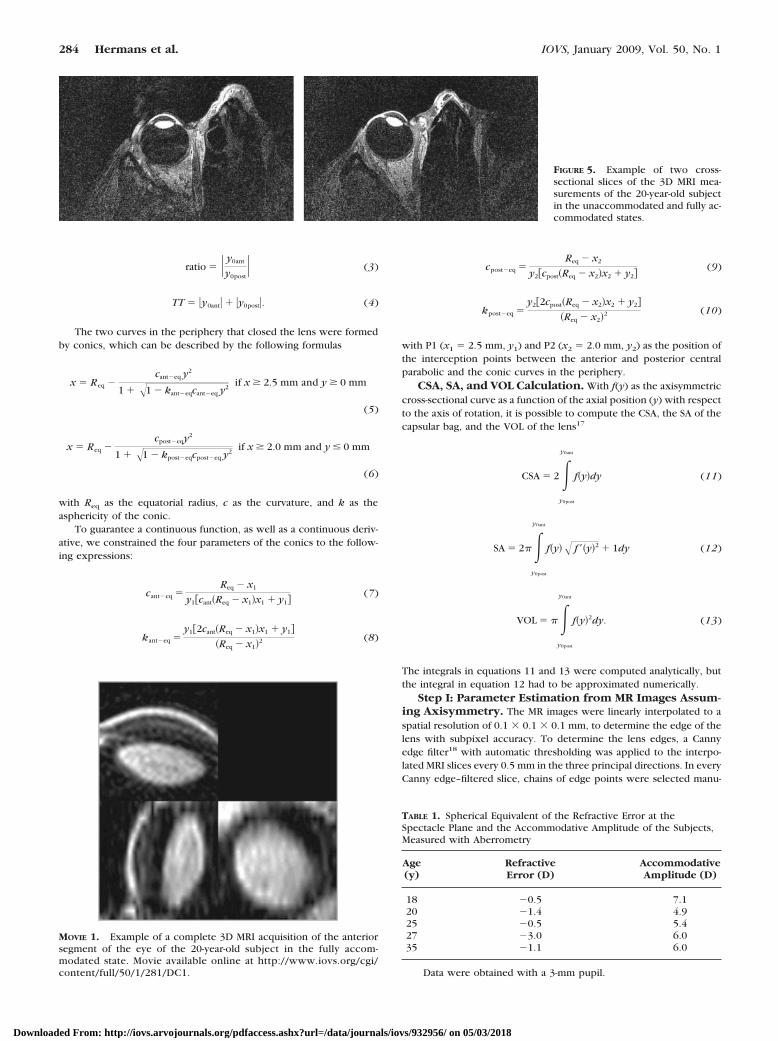
FIGURE 5. Example of two cross-sectional slices of the 3D MRI mea-surements of the 20-year-old subjectin the unaccommodated and fully ac-commodated states.
MOVIE 1. Example of a complete 3D MRI acquisition of the anteriorsegment of the eye of the 20-year-old subject in the fully accom-modated state. Movie available online at http://www.iovs.org/cgi/content/full/50/1/281/DC1.
TABLE 1. Spherical Equivalent of the Refractive Error at theSpectacle Plane and the Accommodative Amplitude of the Subjects,Measured with Aberrometry
Age(y)
RefractiveError (D)
AccommodativeAmplitude (D)
18 �0.5 7.120 �1.4 4.925 �0.5 5.427 �3.0 6.035 �1.1 6.0
Data were obtained with a 3-mm pupil.
284 Hermans et al. IOVS, January 2009, Vol. 50, No. 1
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/932956/ on 05/03/2018
ally by mouse to obtain the coordinates of the lens edge. Subsequently,these coordinates were translated (x, y, z), rotated (�, ), andtransformed to spherical coordinates. Under the assumption of anaxisymmetric lens, the cross-sectional shape is independent of thecircular direction. Therefore, all coordinate points were mapped toone cross-sectional plane (x, y) as can be seen in Figure 2.
Nonlinear least-squares curve-fitting with the reflective Newtonmethod (available in the MatLab Optimization toolbox; The MathworksInc., Natick, MA), was performed to estimate the orientation (x, y,z, �, and ) and shape parameters of the lens (Rant, Rpost, ratio, TT,and Req). The orientation and geometry in which the lens showed mostaxisymmetry was determined.
Step II: Parameter Estimation from MR Images Takinginto Account Lens Nonaxisymmetry. Because the lens is notcompletely axisymmetric, a better description of the geometry couldperhaps be obtained by dividing the lens into eight parts (Fig. 3). Thechoice of eight parts was a tradeoff between the number of data pointsper part and asymmetry. To obtain an accurate estimate of the SA andthe VOL of the lens, the cross-sectional geometry, as proposed inFigure 1, was fitted to each of the eight parts. The CSA, the SA, and theVOL were calculated for each part, and the mean of the CSAs of all
parts was calculated for each subject. Finally, the SA and the VOL of theparts were summed to obtain an estimate of the total SA and VOL ineach accommodative state.
Step III: Parameter Estimation from Scheimpflug Im-ages. The inclined position of the CCD camera, according to the
Scheimpflug principle, causes geometric distortion (type I). The lightrays that form the image of the lens are also refracted by the cornea andthe anterior side of the lens, causing refractive distortion (type II). Thecorrection for both types of distortion was performed with custom-developed software written in C.19 The index of refraction of thelens is needed to determine the path of the light rays that originatefrom inside the lens and are refracted on the anterior lens surface. Anequivalent index of refraction of the lens was estimated, using addi-tional information on axial length and refractive error. After correction,the anterior and posterior central parabolics and total thickness werefitted at an aperture of 4 and 5 mm, respectively, with the Levenberg-Marquardt method. Because of the 2D Scheimpflug imaging technique,it has to be assumed that the lens is axisymmetric. The position of theaxis of symmetry of the cross-sectional geometry inside the Scheimp-flug object plane was also estimated.
b
0 1 2 3 4 5 6 77
8
9
10
11
12
13
14
15
accommodation (D)
ante
rior
radi
us R
ant (
mm
)
0 1 2 3 4 5 6 7
4
5
6
7
8
9
accommodation (D)
post
erio
r ra
dius
Rpo
st (
mm
)
0 1 2 3 4 5 6 73.4
3.5
3.6
3.7
3.8
3.9
4
4.1
4.2
accommodation (D)
tota
l thi
ckne
ss T
T (
mm
)
a c
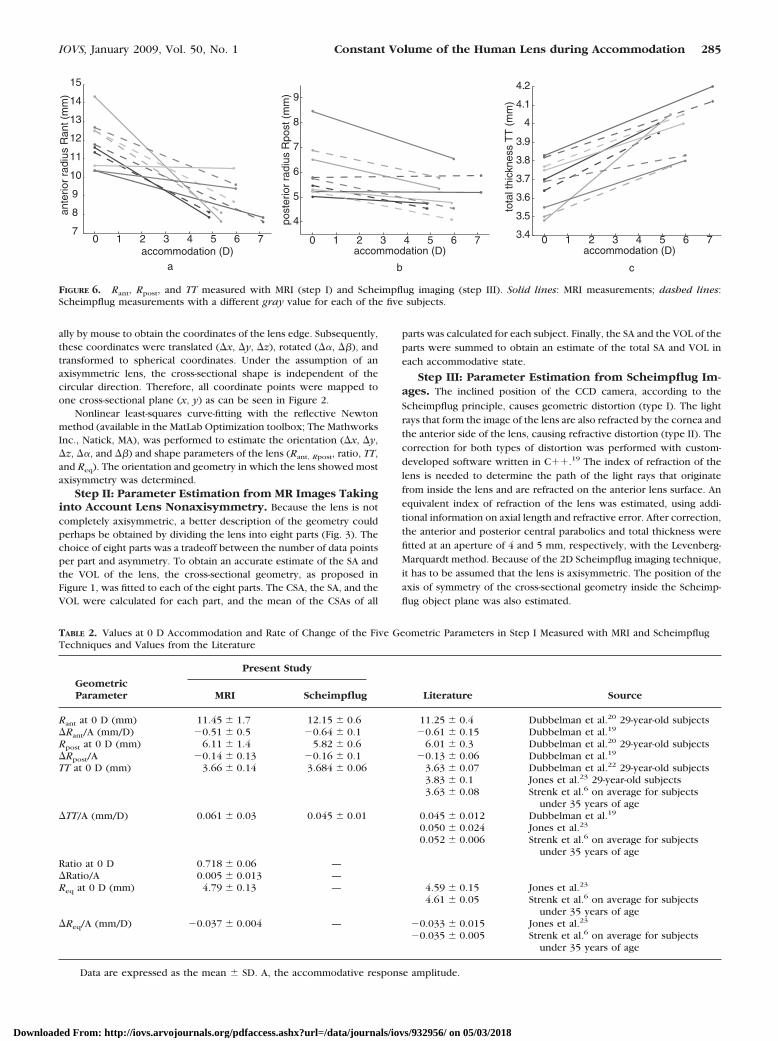
FIGURE 6. Rant, Rpost, and TT measured with MRI (step I) and Scheimpflug imaging (step III). Solid lines: MRI measurements; dashed lines:Scheimpflug measurements with a different gray value for each of the five subjects.
TABLE 2. Values at 0 D Accommodation and Rate of Change of the Five Geometric Parameters in Step I Measured with MRI and ScheimpflugTechniques and Values from the Literature
GeometricParameter
Present Study
Literature SourceMRI Scheimpflug
Rant at 0 D (mm) 11.45 � 1.7 12.15 � 0.6 11.25 � 0.4 Dubbelman et al.20 29-year-old subjectsRant/A (mm/D) �0.51 � 0.5 �0.64 � 0.1 �0.61 � 0.15 Dubbelman et al.19
Rpost at 0 D (mm) 6.11 � 1.4 5.82 � 0.6 6.01 � 0.3 Dubbelman et al.20 29-year-old subjectsRpost/A �0.14 � 0.13 �0.16 � 0.1 �0.13 � 0.06 Dubbelman et al.19
TT at 0 D (mm) 3.66 � 0.14 3.684 � 0.06 3.63 � 0.07 Dubbelman et al.22 29-year-old subjects3.83 � 0.1 Jones et al.23 29-year-old subjects3.63 � 0.08 Strenk et al.6 on average for subjects
under 35 years of ageTT/A (mm/D) 0.061 � 0.03 0.045 � 0.01 0.045 � 0.012 Dubbelman et al.19
0.050 � 0.024 Jones et al.23
0.052 � 0.006 Strenk et al.6 on average for subjectsunder 35 years of age
Ratio at 0 D 0.718 � 0.06 —Ratio/A 0.005 � 0.013 —Req at 0 D (mm) 4.79 � 0.13 — 4.59 � 0.15 Jones et al.23
4.61 � 0.05 Strenk et al.6 on average for subjectsunder 35 years of age
Req/A (mm/D) �0.037 � 0.004 — �0.033 � 0.015 Jones et al.23
�0.035 � 0.005 Strenk et al.6 on average for subjectsunder 35 years of age
Data are expressed as the mean � SD. A, the accommodative response amplitude.
IOVS, January 2009, Vol. 50, No. 1 Constant Volume of the Human Lens during Accommodation 285
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/932956/ on 05/03/2018
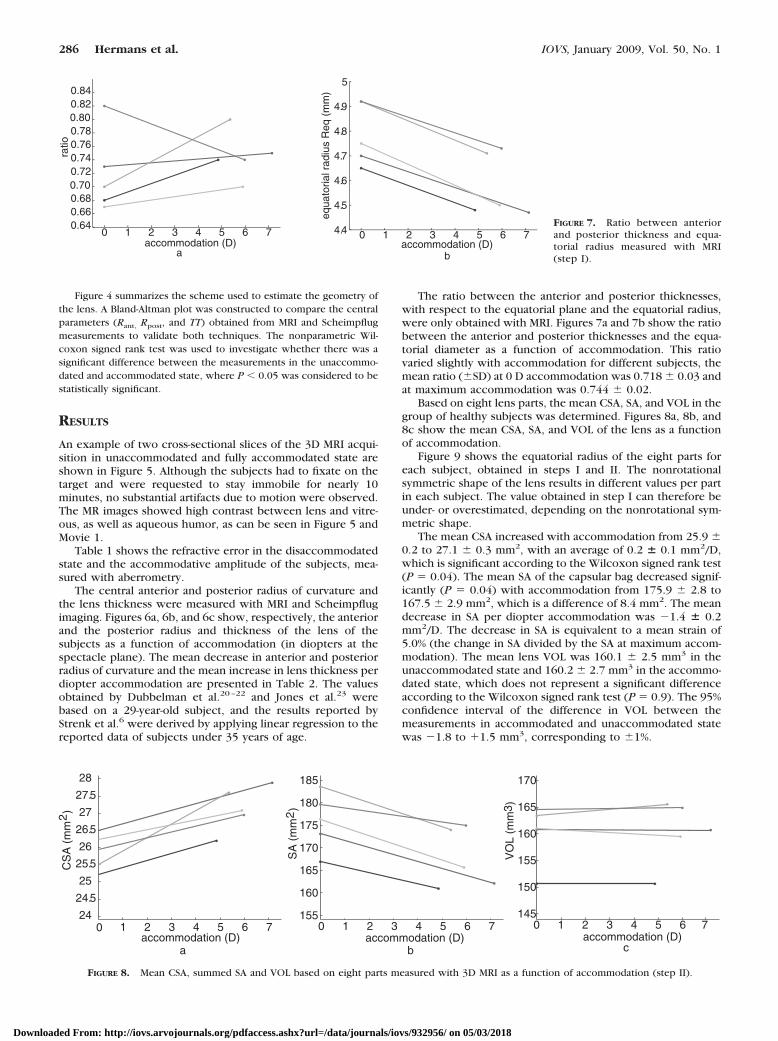
Figure 4 summarizes the scheme used to estimate the geometry ofthe lens. A Bland-Altman plot was constructed to compare the centralparameters (Rant, Rpost, and TT) obtained from MRI and Scheimpflugmeasurements to validate both techniques. The nonparametric Wil-coxon signed rank test was used to investigate whether there was asignificant difference between the measurements in the unaccommo-dated and accommodated state, where P � 0.05 was considered to bestatistically significant.
RESULTS
An example of two cross-sectional slices of the 3D MRI acqui-sition in unaccommodated and fully accommodated state areshown in Figure 5. Although the subjects had to fixate on thetarget and were requested to stay immobile for nearly 10minutes, no substantial artifacts due to motion were observed.The MR images showed high contrast between lens and vitre-ous, as well as aqueous humor, as can be seen in Figure 5 andMovie 1.
Table 1 shows the refractive error in the disaccommodatedstate and the accommodative amplitude of the subjects, mea-sured with aberrometry.
The central anterior and posterior radius of curvature andthe lens thickness were measured with MRI and Scheimpflugimaging. Figures 6a, 6b, and 6c show, respectively, the anteriorand the posterior radius and thickness of the lens of thesubjects as a function of accommodation (in diopters at thespectacle plane). The mean decrease in anterior and posteriorradius of curvature and the mean increase in lens thickness perdiopter accommodation are presented in Table 2. The valuesobtained by Dubbelman et al.20–22 and Jones et al.23 werebased on a 29-year-old subject, and the results reported byStrenk et al.6 were derived by applying linear regression to thereported data of subjects under 35 years of age.
The ratio between the anterior and posterior thicknesses,with respect to the equatorial plane and the equatorial radius,were only obtained with MRI. Figures 7a and 7b show the ratiobetween the anterior and posterior thicknesses and the equa-torial diameter as a function of accommodation. This ratiovaried slightly with accommodation for different subjects, themean ratio (�SD) at 0 D accommodation was 0.718 � 0.03 andat maximum accommodation was 0.744 � 0.02.
Based on eight lens parts, the mean CSA, SA, and VOL in thegroup of healthy subjects was determined. Figures 8a, 8b, and8c show the mean CSA, SA, and VOL of the lens as a functionof accommodation.
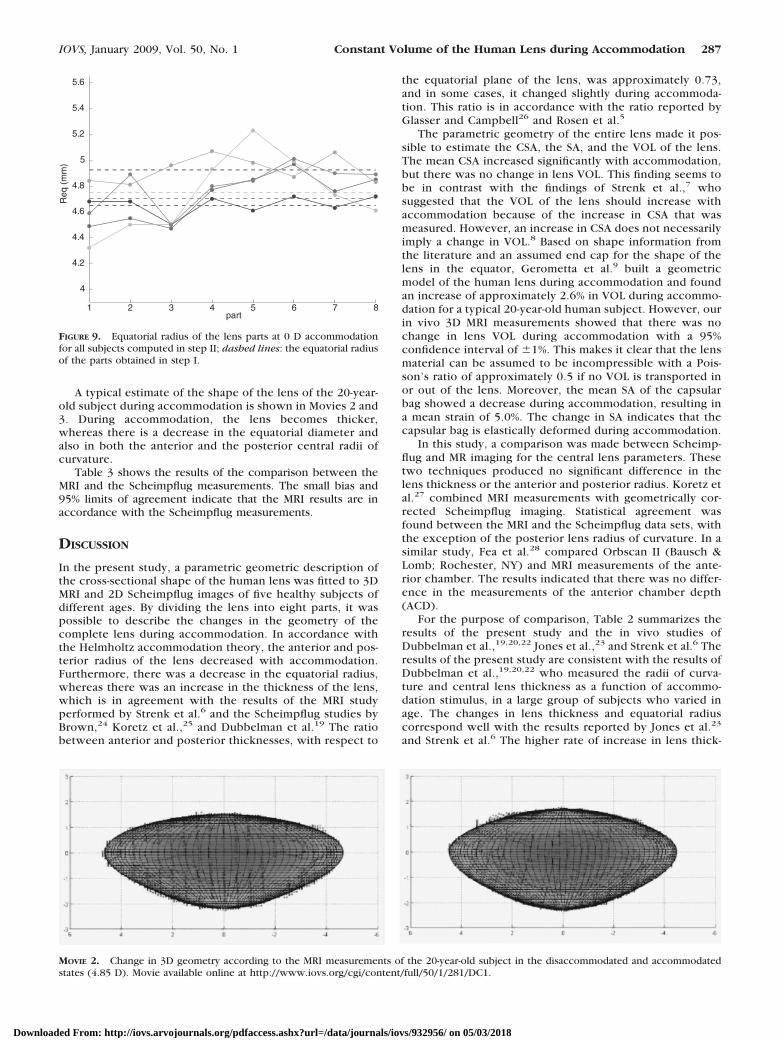
Figure 9 shows the equatorial radius of the eight parts foreach subject, obtained in steps I and II. The nonrotationalsymmetric shape of the lens results in different values per partin each subject. The value obtained in step I can therefore beunder- or overestimated, depending on the nonrotational sym-metric shape.
The mean CSA increased with accommodation from 25.9 �0.2 to 27.1 � 0.3 mm2, with an average of 0.2 � 0.1 mm2/D,which is significant according to the Wilcoxon signed rank test(P � 0.04). The mean SA of the capsular bag decreased signif-icantly (P � 0.04) with accommodation from 175.9 � 2.8 to167.5 � 2.9 mm2, which is a difference of 8.4 mm2. The meandecrease in SA per diopter accommodation was �1.4 � 0.2mm2/D. The decrease in SA is equivalent to a mean strain of5.0% (the change in SA divided by the SA at maximum accom-modation). The mean lens VOL was 160.1 � 2.5 mm3 in theunaccommodated state and 160.2 � 2.7 mm3 in the accommo-dated state, which does not represent a significant differenceaccording to the Wilcoxon signed rank test (P � 0.9). The 95%confidence interval of the difference in VOL between themeasurements in accommodated and unaccommodated statewas �1.8 to 1.5 mm3, corresponding to �1%.
0 1 2 3 4 5 6 7 0.64 0.66 0.68 0.70 0.72 0.74 0.76 0.78 0.80 0.82 0.84
accommodation (D)
ratio
0 1 2 3 4 5 6 7 4. 4
4. 5
4. 6
4. 7
4. 8
4. 9
5
accommodation (D)
equa
toria
l rad
ius
Req
(m
m)
a b
FIGURE 7. Ratio between anteriorand posterior thickness and equa-torial radius measured with MRI(step I).
1 2 3 4 5 6 724
24.5
25
25.5
26
26.5
27
27.5
28
accommodation (D)0 1 2 3 4 5 6 7
155
160
165
170
175
180
185
accommodation (D)0 1 2 3 4 5 6 7
145
150
155
160
165
170
accommodation (D)0
b ca
FIGURE 8. Mean CSA, summed SA and VOL based on eight parts measured with 3D MRI as a function of accommodation (step II).
286 Hermans et al. IOVS, January 2009, Vol. 50, No. 1
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/932956/ on 05/03/2018
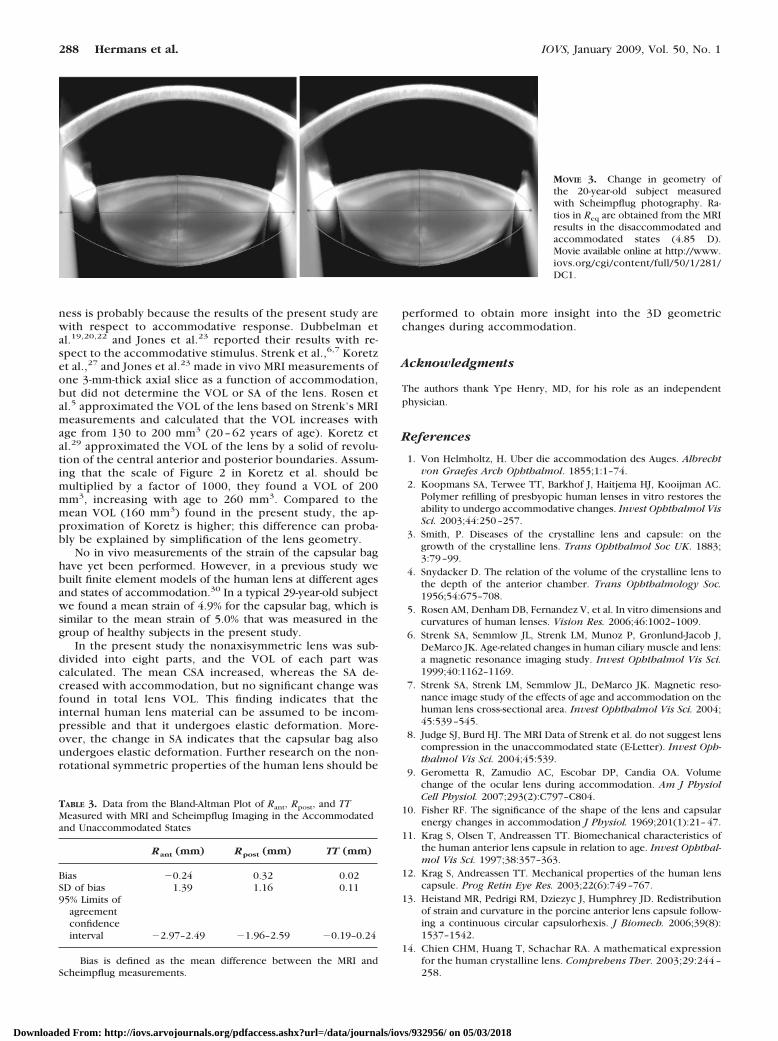
A typical estimate of the shape of the lens of the 20-year-old subject during accommodation is shown in Movies 2 and3. During accommodation, the lens becomes thicker,whereas there is a decrease in the equatorial diameter andalso in both the anterior and the posterior central radii ofcurvature.
Table 3 shows the results of the comparison between theMRI and the Scheimpflug measurements. The small bias and95% limits of agreement indicate that the MRI results are inaccordance with the Scheimpflug measurements.
DISCUSSION
In the present study, a parametric geometric description ofthe cross-sectional shape of the human lens was fitted to 3DMRI and 2D Scheimpflug images of five healthy subjects ofdifferent ages. By dividing the lens into eight parts, it waspossible to describe the changes in the geometry of thecomplete lens during accommodation. In accordance withthe Helmholtz accommodation theory, the anterior and pos-terior radius of the lens decreased with accommodation.Furthermore, there was a decrease in the equatorial radius,whereas there was an increase in the thickness of the lens,which is in agreement with the results of the MRI studyperformed by Strenk et al.6 and the Scheimpflug studies byBrown,24 Koretz et al.,25 and Dubbelman et al.19 The ratiobetween anterior and posterior thicknesses, with respect to
the equatorial plane of the lens, was approximately 0.73,and in some cases, it changed slightly during accommoda-tion. This ratio is in accordance with the ratio reported byGlasser and Campbell26 and Rosen et al.5
The parametric geometry of the entire lens made it pos-sible to estimate the CSA, the SA, and the VOL of the lens.The mean CSA increased significantly with accommodation,but there was no change in lens VOL. This finding seems tobe in contrast with the findings of Strenk et al.,7 whosuggested that the VOL of the lens should increase withaccommodation because of the increase in CSA that wasmeasured. However, an increase in CSA does not necessarilyimply a change in VOL.8 Based on shape information fromthe literature and an assumed end cap for the shape of thelens in the equator, Gerometta et al.9 built a geometricmodel of the human lens during accommodation and foundan increase of approximately 2.6% in VOL during accommo-dation for a typical 20-year-old human subject. However, ourin vivo 3D MRI measurements showed that there was nochange in lens VOL during accommodation with a 95%confidence interval of �1%. This makes it clear that the lensmaterial can be assumed to be incompressible with a Pois-son’s ratio of approximately 0.5 if no VOL is transported inor out of the lens. Moreover, the mean SA of the capsularbag showed a decrease during accommodation, resulting ina mean strain of 5.0%. The change in SA indicates that thecapsular bag is elastically deformed during accommodation.
In this study, a comparison was made between Scheimp-flug and MR imaging for the central lens parameters. Thesetwo techniques produced no significant difference in thelens thickness or the anterior and posterior radius. Koretz etal.27 combined MRI measurements with geometrically cor-rected Scheimpflug imaging. Statistical agreement wasfound between the MRI and the Scheimpflug data sets, withthe exception of the posterior lens radius of curvature. In asimilar study, Fea et al.28 compared Orbscan II (Bausch &Lomb; Rochester, NY) and MRI measurements of the ante-rior chamber. The results indicated that there was no differ-ence in the measurements of the anterior chamber depth(ACD).
For the purpose of comparison, Table 2 summarizes theresults of the present study and the in vivo studies ofDubbelman et al.,19,20,22 Jones et al.,23 and Strenk et al.6 Theresults of the present study are consistent with the results ofDubbelman et al.,19,20,22 who measured the radii of curva-ture and central lens thickness as a function of accommo-dation stimulus, in a large group of subjects who varied inage. The changes in lens thickness and equatorial radiuscorrespond well with the results reported by Jones et al.23
and Strenk et al.6 The higher rate of increase in lens thick-
1 2 3 4 5 6 7 8
4
4.2
4.4
4.6
4.8
5
5.2
5.4
5.6
part
Req
(m
m)
FIGURE 9. Equatorial radius of the lens parts at 0 D accommodationfor all subjects computed in step II; dashed lines: the equatorial radiusof the parts obtained in step I.
MOVIE 2. Change in 3D geometry according to the MRI measurements of the 20-year-old subject in the disaccommodated and accommodatedstates (4.85 D). Movie available online at http://www.iovs.org/cgi/content/full/50/1/281/DC1.
IOVS, January 2009, Vol. 50, No. 1 Constant Volume of the Human Lens during Accommodation 287
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/932956/ on 05/03/2018
ness is probably because the results of the present study arewith respect to accommodative response. Dubbelman etal.19,20,22 and Jones et al.23 reported their results with re-spect to the accommodative stimulus. Strenk et al.,6,7 Koretzet al.,27 and Jones et al.23 made in vivo MRI measurements ofone 3-mm-thick axial slice as a function of accommodation,but did not determine the VOL or SA of the lens. Rosen etal.5 approximated the VOL of the lens based on Strenk’s MRImeasurements and calculated that the VOL increases withage from 130 to 200 mm3 (20 – 62 years of age). Koretz etal.29 approximated the VOL of the lens by a solid of revolu-tion of the central anterior and posterior boundaries. Assum-ing that the scale of Figure 2 in Koretz et al. should bemultiplied by a factor of 1000, they found a VOL of 200mm3, increasing with age to 260 mm3. Compared to themean VOL (160 mm3) found in the present study, the ap-proximation of Koretz is higher; this difference can proba-bly be explained by simplification of the lens geometry.
No in vivo measurements of the strain of the capsular baghave yet been performed. However, in a previous study webuilt finite element models of the human lens at different agesand states of accommodation.30 In a typical 29-year-old subjectwe found a mean strain of 4.9% for the capsular bag, which issimilar to the mean strain of 5.0% that was measured in thegroup of healthy subjects in the present study.
In the present study the nonaxisymmetric lens was sub-divided into eight parts, and the VOL of each part wascalculated. The mean CSA increased, whereas the SA de-creased with accommodation, but no significant change wasfound in total lens VOL. This finding indicates that theinternal human lens material can be assumed to be incom-pressible and that it undergoes elastic deformation. More-over, the change in SA indicates that the capsular bag alsoundergoes elastic deformation. Further research on the non-rotational symmetric properties of the human lens should be
performed to obtain more insight into the 3D geometricchanges during accommodation.
Acknowledgments
The authors thank Ype Henry, MD, for his role as an independentphysician.
References
1. Von Helmholtz, H. Uber die accommodation des Auges. Albrechtvon Graefes Arch Ophthalmol. 1855;1:1–74.
2. Koopmans SA, Terwee TT, Barkhof J, Haitjema HJ, Kooijman AC.Polymer refilling of presbyopic human lenses in vitro restores theability to undergo accommodative changes. Invest Ophthalmol VisSci. 2003;44:250–257.
3. Smith, P. Diseases of the crystalline lens and capsule: on thegrowth of the crystalline lens. Trans Ophthalmol Soc UK. 1883;3:79–99.
4. Snydacker D. The relation of the volume of the crystalline lens tothe depth of the anterior chamber. Trans Ophthalmology Soc.1956;54:675–708.
5. Rosen AM, Denham DB, Fernandez V, et al. In vitro dimensions andcurvatures of human lenses. Vision Res. 2006;46:1002–1009.
6. Strenk SA, Semmlow JL, Strenk LM, Munoz P, Gronlund-Jacob J,DeMarco JK. Age-related changes in human ciliary muscle and lens:a magnetic resonance imaging study. Invest Ophthalmol Vis Sci.1999;40:1162–1169.
7. Strenk SA, Strenk LM, Semmlow JL, DeMarco JK. Magnetic reso-nance image study of the effects of age and accommodation on thehuman lens cross-sectional area. Invest Ophthalmol Vis Sci. 2004;45:539–545.
8. Judge SJ, Burd HJ. The MRI Data of Strenk et al. do not suggest lenscompression in the unaccommodated state (E-Letter). Invest Oph-thalmol Vis Sci. 2004;45:539.
9. Gerometta R, Zamudio AC, Escobar DP, Candia OA. Volumechange of the ocular lens during accommodation. Am J PhysiolCell Physiol. 2007;293(2):C797–C804.
10. Fisher RF. The significance of the shape of the lens and capsularenergy changes in accommodation J Physiol. 1969;201(1):21–47.
11. Krag S, Olsen T, Andreassen TT. Biomechanical characteristics ofthe human anterior lens capsule in relation to age. Invest Ophthal-mol Vis Sci. 1997;38:357–363.
12. Krag S, Andreassen TT. Mechanical properties of the human lenscapsule. Prog Retin Eye Res. 2003;22(6):749–767.
13. Heistand MR, Pedrigi RM, Dziezyc J, Humphrey JD. Redistributionof strain and curvature in the porcine anterior lens capsule follow-ing a continuous circular capsulorhexis. J Biomech. 2006;39(8):1537–1542.
14. Chien CHM, Huang T, Schachar RA. A mathematical expressionfor the human crystalline lens. Comprehens Ther. 2003;29:244 –258.
MOVIE 3. Change in geometry ofthe 20-year-old subject measuredwith Scheimpflug photography. Ra-tios in Req are obtained from the MRIresults in the disaccommodated andaccommodated states (4.85 D).Movie available online at http://www.iovs.org/cgi/content/full/50/1/281/DC1.
TABLE 3. Data from the Bland-Altman Plot of Rant, Rpost, and TTMeasured with MRI and Scheimpflug Imaging in the Accommodatedand Unaccommodated States
Rant (mm) Rpost (mm) TT (mm)
Bias �0.24 0.32 0.02SD of bias 1.39 1.16 0.1195% Limits of
agreementconfidenceinterval �2.97–2.49 �1.96–2.59 �0.19–0.24
Bias is defined as the mean difference between the MRI andScheimpflug measurements.
288 Hermans et al. IOVS, January 2009, Vol. 50, No. 1
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/932956/ on 05/03/2018

15. Kasprzak HT. New approximation for the whole profile of thehuman crystalline lens. Ophthalmic Physiol Opt. 2000;20:31– 43.
16. Drexler W, Findl O, Menapace R. et al. Partial coherenceinterferometry: A novel approach to biometry in cataract surgery.Am J Ophthalmol. 1998;126:524–534.
17. Arfken GB, Weber HJ. 1. Vector analysis. Mathematical Methodsfor Physicists. San Diego, CA: Academic Press; 2001.
18. Canny JA Computational approach to edge-detection. IEEE TransPattern Anal Mach Intel. 1986;8:679–698.
19. Dubbelman M, Van der Heijde GL, Weeber HA. Change in shape ofthe aging human crystalline lens with accommodation. Vision Res.2005;45:117–132.
20. Dubbelman M, Van der Heijde GL. The shape of the aging humanlens: curvature, equivalent refractive index and the lens paradox.Vision Res. 2001;41:1867–1877.
21. Dubbelman M, Van der Heijde GL, Weeber HA. The thickness ofthe aging human lens obtained from corrected Scheimpflug im-ages. Optometry Vis Sci. 2001;78:411–416.
22. Dubbelman M, Van der Heijde GL, Weeber HA, Vrensen GF.Changes in the internal structure of the human crystalline lenswith age and accommodation. Vision Res. 2003;43:2363–2375.
23. Jones CE, Atchison DA, Pope JM. Changes in lens dimensions andrefractive index with age and accommodation. Optometry Vis Sci.2007;84(10):990–995.
24. Brown N. Change in shape and internal form of lens of eye onaccommodation. Exp Eye Res. 1973;15:441–459.
25. Koretz JF, Cook CA, Kaufman PL. Aging of the human lens:changes in lens shape upon accommodation and with accommo-dative loss. J Opt Soc Am A Opt Image Sci Vis. 2002;19:144–151.
26. Glasser A, Campbell MCW. Biometric, optical and physicalchanges in the isolated human crystalline lens with age in relationto presbyopia. Vision Res. 1999;39(11):1991–2015.
27. Koretz JF, Strenk SA, Strenk LM, Semmlow JL. Scheimpflug andhigh-resolution magnetic resonance imaging of the anterior segment:a comparative study. J Opt Soc Am A. 2004;21(3):346–354.
28. Fea AM, Annetta F, Cirillo S, et al. Magnetic resonance imaging andOrbscan assessment of the anterior chamber. J Cataract RefractSurg. 2005;31:1713–1718.
29. Koretz JF, Cook CA, Kaufman PL. Aging of the human lens:changes in lens shape at zero-diopter accommodation. J Opt SocAm A Opt Image Sci Vis. 2001;18:265–272.
30. Hermans EA, Dubbelman M, Van der Heijde GL, Heethaar RM.Change in the accommodative force on the lens of the human eyewith age. Vision Res. 2008;48(1):119–126.
IOVS, January 2009, Vol. 50, No. 1 Constant Volume of the Human Lens during Accommodation 289
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/932956/ on 05/03/2018