Consolidation report (2009) - from testing to spread
32
NHS NHS Improvement Transforming Inpatient Care Programme Consolidation Report (2009) From testing to spread HEART LUNG CANCER DIAGNOSTICS STROKE
-
Upload
nhs-improvement -
Category
Health & Medicine
-
view
316 -
download
2
description
This publication reports back on a review undertaken by NHS Improvement to examine the progress and impact of 25 Acute Trusts who took part in the Transforming Cancer Inpatient Care Programme (July 2007-2008) and the subsequent spread of the Winning Principles and models of care across England (Published July 2010).
Transcript of Consolidation report (2009) - from testing to spread

NHSNHS Improvement
Transforming Inpatient Care Programme
Consolidation Report (2009)From testing to spread
HEART
LUNG
CANCER
DIAGNOSTICS
STROKE


Consolidation Report - From testing to spread | 3
ContentsForeword
Summary
Introduction
25 NHS acute test trusts: Progress, impact and benefits
Reported benefits and investments
Impact of the Winning Principles and Models of Care
Winning Principle 1
Winning Principle 2
Winning Principle 3
Winning Principle 4
Summary: Consolidation of testing
Beyond testing: Coverage and spread
Levers for spread
Conclusion
Acknowledgements and references
4
5
8
9
10
11
12
16
22
23
24
25
28
29
30

4 | Consolidation Report - From testing to spread
Foreword
Celia Ingham Clark
The NHS has to identify ways to improve both quality and productivity in
order to continue to improve patient care in a tight economic climate.
This report provides significant encouragement that we can achieve the
joint aims of quality and productivity in the care of people with cancer.
It describes a range of ways in which cancer care can be streamlined and
become more patient-centred. The techniques all follow the four
Winning Principles. The report contains details of the spread of these
techniques accompanied by an estimate of the potential savings that
they can deliver in terms of bed-days and costs, and it demonstrates
effective implementation of the Cancer Reform Strategy.
I hope that Trust Medical Directors and Cancer Managers who have not
yet adopted the ‘Winning Principles’ will be motivated to do so on
reading this report. For those who have already delivered some quality
improvements, many of whom are mentioned in the report, the
challenge now is to implement the other improvements too!
Celia Ingham ClarkColorectal Surgeon and Medical Director, Whittington Hospital, London.National Clinical Lead Transforming Inpatient Care Programme

SummaryThe Cancer Reform Strategy (CRS 2007) highlighted the need to focus attention on inpatientcare. Too many patients were being admitted into hospital and lengths of stay were oftenunnecessarily prolonged. The CRS established the Transforming Cancer Inpatient CareProgramme to take this forward and test out ideas that would improve quality and reduceunnecessary inpatient bed days.
This report is the product of a review undertakenby NHS Improvement examining the progress andimpact of 25 Acute Trusts who took part in theTransforming Cancer Inpatient Care Programme(July 2007-2008) and the subsequent spread ofthe Winning Principles and models of care acrossEngland.
The report forms part of NHS Improvementevaluation strategy, and provides evidence ofprogress to the Department of Health CancerProgramme Board supporting the quality,innovation, productivity and prevention(QIPP) agenda.
Achievements of the 25 Acute TrustsThe 25 Acute Trusts incorporates 37 hospital siteswhich covered 16% of acute providers for cancerservices across England. In terms of improvingquality and productivity good progress was madeagainst the baseline position (see Figure 2).
• Through testing the Trusts identified four simplequality principles, published as ‘The WinningPrinciples’ (July 2008); fundamental toimproving emergency and elective pathways,clinical decision-making and enhancing patientself-management.
• Across the Trusts 108,067 potential bed daycapacity was released (Figure 2).
• Based on the lower estimate of £200 perpatient, per bed day, the potential releasedefficiency saving for the 25 trusts was £21.6m.
From testing to spreadThe learning from testing was disseminated widelythroughout the testing period (July 2007-2008) toencourage early adopters. Spreading the WinningPrinciples Strategy was launched in July 2008.Evidence from the subsequent spread survey(December 2009) identified:
• 54 NHS Trusts (covering 72 hospital sites) werespreading the quality principles and models.
• 183 improvement activities have been reported.• The main focus for spread surrounds WinningPrinciples 1 and 2; emergency and elective care,the application of communication alert systems,enhanced recovery approaches, 23 hour breastmodel and symptom specific pathways e.g.febrile neutropenia.
• Coverage increased across England from 16%to 34% of secondary acute providers(see Figure 1).
• The 2008/09 national picture shows that thetotal of bed days peaked at 5.25m in 2005/06.Since then there has been a 15% fall. The‘Spread activity’ contribution to the nationalpicture over the last two years saw a shiftedfrom 2.4% bed capacity released during testingto 34.17% as subsequent spread.
• Nationally, 264,340 bed days were releasedtowards saving a million beds days (2012).Progress is being made but the pace of spreadneeds to be accelerated.
• The four key levers identified by Trusts toaccelerate spread were planning for spread,having communication and awarenessstrategies, identify and the use of opinionleaders and sharing comparative data (seeFigure 24).
Consolidation Report - From testing to spread | 5

6 | Consolidation Report - From testing to spread
Figure 1: What contribution are the 54 Trusts making tothe national picture and the potential impact?
54 Trusts episodes ( emergency/electiveinpatients)
54 Trusts bed days
54 Trusts reduction in length of stay from2007-2008 Year
54 Trusts reduction potential savings inlength of stay from 2007-2008 Year
54 Trusts % contribution bed days towardsnational coverage 2007-2008 Year
298,595
1,750,564
0
£0
0.00%
288,527
1,660,251
90,313
£18,062,600
34.17%
309,657
1,730,149
20,415
£4,082,933
16.03%
2007-2008 2008-2009 2009-2010 Fullyear projection(provisional)
Spread strategylaunchedJuly 2008
The national picture shows that the total bed days peaked at 5.25m in 2005/2006.Since then there has been a 15% fall to around 4.5m.
National Episodes (emergency/electiveinpatients)
National bed days
National reduction in length of stay from2007-2008 Year
National potential savings in length of stayfrom 2007-2008 Year (£200 per patient perbed day lower estimate)
National bed day saving from2007-2008 Year
775,279
4,759,067
0
£0
0.00%
757,494
4,494,727
264,340
£52,868,000
5.55%
807,621
4,631,701
127,366
£25,473,133
2.68%
2007-2008 2008-2009 2009-2010 Fullyear projection(provisional)

Consolidation Report - From testing to spread | 7
Where to next: A focus on spreadRetaining the focus on accelerating the pace ofspread remains a priority.
This review provides a useful baseline upon whichto build the next stage of the TransformingInpatients Spread Strategy (2010-2012). This willinclude:
• Emergency and Urgent Care Initiative led byNHS Improvement. Due to the increasingnumber of emergency admissions, the focusneeds to be retained on spreading WinningPrinciple 1 and the new models of emergencyand urgent care that include:• Triage, Treat, Transfer Pathways• Telephone triage• Crisis resolution teams and integratedcommunity working
• Improved patient signposting to urgentcare settings
• Proactive risk management by telephone toavoid unnecessary admissions
• Communication Alerts• Emergency Care Practitioner assessmentand triage
• Home tele-monitoring - Diagnostics andtesting at home
• Patient ownership of health records andemergency/urgent care plans
• 24 hour pharmacies holding emergency drugbox (for OOH GPs)
• Pain management without hospital admission• Acute Oncology Models
1. Unscheduled (emergency) patientsshould be assessed prior to the decisionto admit. Emergency admission shouldbe the exception not the norm.
The Winning Principles
• Spreading Winning Principle 2, key models:• The 23 hour breast model of ambulatory careacross cancer networks.
• Enhanced Recovery approaches• Shifting procedures from inpatient toalternative care settings.
• Repeating the spread survey during thesummer of 2010 and 2011.
3. Clinical decisions should be madeon a daily basis to promote proactivecase management.
4. Patient and carers need to knowabout their condition and symptomsto encourage self-management and toknow who to contact when needed.
2. All patients should be on a definedinpatient pathways based on theirtumour type and reasons foradmission.

IntroductionThe report draws on 180 pieces of evidence from qualitative and quantitative sources, including;learning diaries, case studies spread planners, local data and a spread survey (October 2009 -December 2009). Hospital Episode Statistics (HES) provided baseline measures (2006/7) andmeasures of progress (2009).
Review objectivesThe objectives of the review were firstly toconsolidate the progress of the 25 testtrusts by:• Examining the progress and quantifyingbenefits, investments and potential reductions inlengths of stay and bed days.
Secondly to:• Assess the coverage, spread of the WinningPrinciples and models
• Provide direction for the next stage of theTransforming Cancer Inpatient Care ProgrammeSpread Strategy.
SpreadThe definition of spread in the context of thisreport has been used as a measure not only ofincreasing numbers but also indicating whichwinning principles and models have been spreador adopted and what local levers are being usedto support this.
Since the commencement of the TransformingInpatient Care Programme 2007, the learninggained has been disseminated nationally(Transforming Care for Cancer Inpatients 2008-2009) and shared with the Department of HealthEnhanced Recovery Partnership Programme (2009)to accelerate the pace of spread; of WinningPrinciple 2 across the NHS.
Continuous ImprovementThere is a danger in a report of this nature, tojudge progress and success on ‘bottom linedeliverables’, particularly at a time whenproductivity and cost savings are high on thehealth agenda. It is therefore important torecognise that the improvements tested involvemany dimensions of change including systems,process redesign, changes in behaviour andclinical and managerial practice. This report isbased on the evidence received which may notreflect all the local variables. In most cases, thespread reported is ongoing and therefore thefindings in this report should be read within thiscontext.
8 | Consolidation Report - From testing to spread

25 NHS acute test trusts: Progress, impactand benefitsAchievementsContinuous incremental progress hasbeen achieved across the 25 testtrusts. The majority of sites achieved areduced length of stay from theoriginal 2006/07 Hospital EpisodeStatistics* baseline position (Figure 2).
• 80% - Reduced length of stayduring the testing period (July2007/08). Releasing 73,582potential bed day capacity
• 80% - Continued to reduce lengthof stay following the testing period
• Overall - 76% reduced length ofstay from the 2006/07 baselineposition, releasing potentially108,067 bed days, which is a 12%reduction from the 2006/07baseline position (Figure 3)
• The contextual information aroundthe trusts where length of stay wasnot reduced or sustained indicatedissues surrounding data collection,improvement work discontinuedand changes in leadership.
*All the HES data used in the review refers to:LoS = HES Length of Episode (Epiend - Epistart).If more than one episode was present in spellthen episode LoS may not equal full spelllength.
All HES data used is retrospective.
HES Baseline Data - April 2006/07 - Used as aretrospective baseline.
HES Testing Data – 2007/08 – Testingcommenced July 2007 to July 2008HES 2008/09 - Spread phase
Figure 2: Average Length of Stay - All Cancers(All episodes emergency and elective inpatients)25 Test Trusts Emergency and Elective Inpatient Cancer AdmissionsAverage LOS 2006/07 Baseline, 2007/08 Testing
1. Barking, Havering and RedbridgeHospitals NHS Trust
2. Barts and The London NHS Trust3. Blackpool, Fylde and Wyre Hospitals NHS
Foundation Trust4. Brighton and Sussex University Hospitals
NHS Trust5. The Christie Hospital NHS Foundation Trust6. East Sussex Hospitals NHS Trust7. Great Western Hospitals NHS Foundation Trust8. Hull and East Yorkshire Hospitals NHS Trust9. King’s College Hospital NHS Foundation Trust10. Milton Keynes Hospital NHS Foundation Trust11. North West London Hospitals NHS Trust12. Northampton General Hospital NHS Trust13. Oxford Radcliffe Hospitals NHS Trust
14. Royal Berkshire NHS Foundation Trust15. Sandwell and West Birmingham Hospitals
NHS Trust16. Scarborough and North East Yorkshire Health
Care NHS Trust17. Sherwood Forest Hospitals NHS
Foundation Trust18. South London Healthcare NHS Trust19. St Helens and Knowsley Hospitals NHS Trust20. The Hillingdon Hospital NHS Trust21. The Whittington Hospital NHS Trust22. United Lincolnshire Hospitals NHS Trust23. University Hospital Birmingham NHS
Foundation Trust24. University Hospitals of Morecambe Bay NHS Trust25.Whipps Cross University Hospital NHS Trust
9
8
7
6
5
4
3
2
1
0
Ave
rag
eLe
ng
tho
fSt
ay(d
ays)
2006 - 2007 2007 - 2008 2008 - 2009
Trust
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25
NHS Trusts
Figure 3: Inpatient episodes and bed day data
2006/07Baseline
2007/08Testing
2008/09CommenceSpread
25 Test Trusts
Episodes
Bed days
RangeAverage LOS
144,442
894,417
7.8 - 4.286.9
148,222
859,932
7.57 - 3.975.8
141,650
786,350
6.9 - 3.615.5
108,067Bed day capacityreleased
Hospital Episode Statistics
Consolidation Report - From testing to spread | 9
Review of the qualitative informationidentified common themes aligned tothe current Quality, Innovation,Productivity and Prevention (QIPP)agenda.
QualityKey elements for improving the qualityof patients, and carers, experiencewere identified by the sites as:• Valuing patient’s time• Setting and managing patientsexpectations
• Improving communication andinformation
• Removing duplication, and non-value adding time throughstreamlining the pathway of care.
InnovationChanges in clinical practice such asthe enhanced recovery approachesand 23 hour breast care model:• Improved the knowledge ofoutcomes
• Reduced postoperativecomplications.
This reflects the Varadhanstudy (2010) that indicated theimplementation of four or moreelements of Enhanced Recovery leadsto a reduction in length of stay bymore than two days and an almost50% reduction in complication ratesin patients undergoing major opencolonic/colorectal surgery.
These clinical models use the most upto date surgical and anaesthetictechniques, challenge traditionalpractices and promote themanagement of patientexpectations.
Alert systems have improvedcommunication, reduced length ofstay and in some cases avertedunnecessary admissions and enhancedtimely clinical decision-making.
Productivity and preventionReductions in unnecessary admissionsand reductions in prolonged lengthsof stay can reduce the risk of hospitalacquired infections, reduce demandson staff and releases bed capacity.
Capturing the benefitsHow trusts individually captured thereleased capacity and finances in realterms was a local decision and notcaptured in the review. Feedbackfrom test sites indicated someorganisations utilised the releasedcapacity to achieve the18 week waitand the cancer 62-day target.
InvestmentInvestment during testing varied fromsite to site dependent on trusts,individual starting point and localcapacity and capability. Investmentreported was predominately time,support from clinicians, managementand service improvement and changemanagement expertise. Costsidentified were minimal and oftenoffset by cost savings from reductionin use of unnecessary equipment suchas drains and by re-organisingresources.
Example: Breast 23 Hour CareModelA reduction in wound drains and theintervention of not draining seromas.Saved patients extra visits to thehospital and released clinic time whichwas utilised for breast pre-assessment.
Example: Enhanced RecoveryModelsThe current work of the EnhancedRecovery Partnership Programme hasidentified the potential costs (Figure 4)and investments required to supportimplementation, if organisations havenone of the enhanced recoveryelements in place. Dedicated time,clinical leadership and changemanagement skills are the keyinvestments required.
Figure 4: Enhanced recoverymodel estimated costs per patient(8 major surgical procedures)
Pre-referral
Pre-operative
Admission
Surgery
Post- surgery
Total net cost
£9 - 35
£20 - 82
£4 - 10
£69 -111
£30 - 73
£142 to £311
Department of Health EnhancedRecovery Partnership Programme(2009)
10 | Consolidation Report - From testing to spread
Reported benefits and investments

Testing identified four qualityfocused ‘winning principles’ andpractical models of care.
The Winning PrinciplesWinning Principle 1Unscheduled (emergency) patients should be assessed prior to the decisionto admit. Emergency admission should be the exception not the norm.
Winning Principle 2All patients should be on defined inpatient pathways based on theirtumour type and reasons for admission.
Winning Principle 3Clinical decisions should be made on a daily basis to promote proactivecase management.
Winning Principle 4Patient and carers need to know about their condition and symptoms toencourage self-management and to know who to contact when needed.
www.improvement.nhs.uk/cancer/inpatients
Impact of the Winning Principles and Models of Care
The Transforming Inpatient Programmehas been acknowledged as providingexcellent examples of ‘Quality, Innovationand Productivity in Practice’ (DavidNicholson CEO NHS, 2009), and theTransforming Inpatient publication (2009)Sharing the Learning, was commendedas best professional education initiativein Oncology (Excellence in Oncology2009).
Consolidation Report - From testing to spread | 11
Winning Principle 1
Unscheduled (emergency)patients should beassessed prior to thedecision to admit.Emergency admissionshould be the exceptionnot the norm.
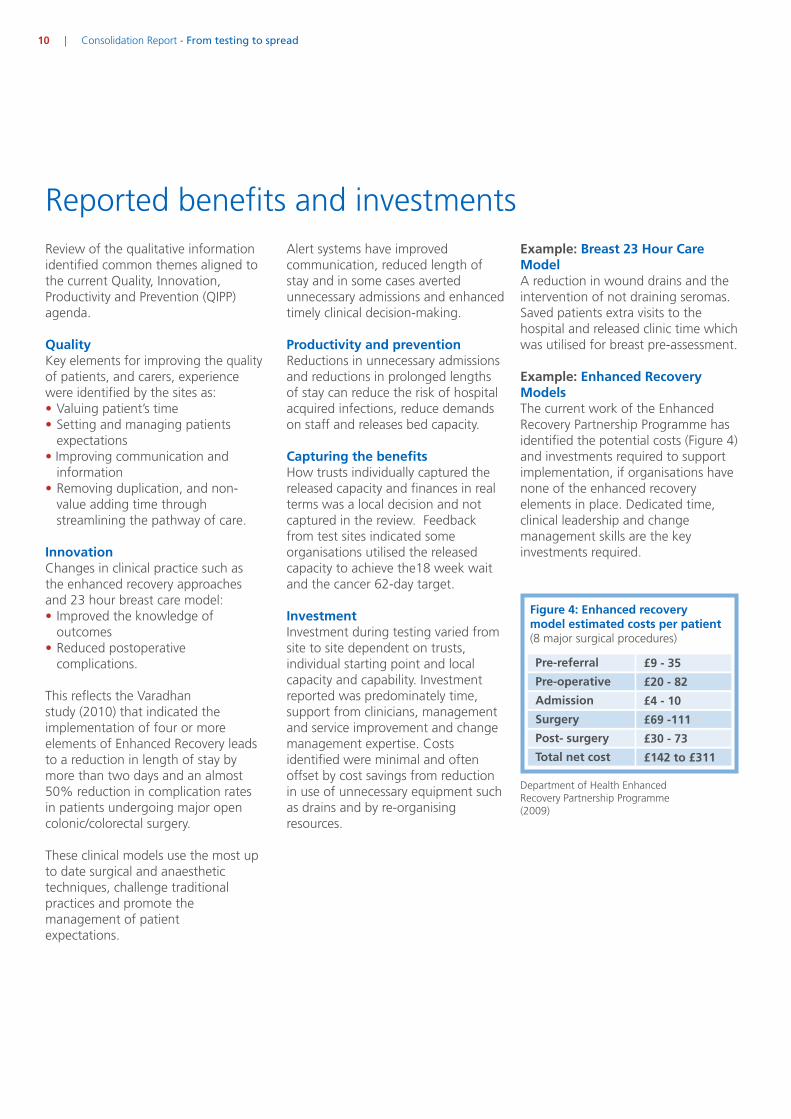
Fifteen trusts tested differentmodels that included definingemergency pathways forsymptoms, palliative care andspecific conditions such asneutropenic sepsis. Trusts tested arange of communication alertsystems and approaches for rapidaccess to timely clinical decisionmaking, which supports WinningPrinciple 3.
Across the 15 test sites, thepotential of 42,147 bed daycapacity (from the baselineposition) was released(Figure 5).
WINNINGPRINCIPLE1
Figure 5: Winning Principle 1 - Baseline and potential impact
2006/07Baseline
2007/08Testing
2008/09CommenceSpread
15 Test Trusts
Episodes
Bed days
Range LOS
95,361
560,516
7.57 - 4.25
96,668
540,418
7.57 - 3.97
96,764
518,371
6.85 - 3.72
42,147Bed day capacityreleased
The average length of stay for cancerrelated emergency admissionsnationally by PCT is 6.5 days acrossEngland, ranging from 4.1 days to9.0 days. (HES. 2008/09).
• Emergency bed days average 11.3bed days per new cancer case,ranging from 7.1 to 17.7 bed days.
Model of Care: CommunicationAlertsThree trusts tested communicationalert systems across specific tumourgroups. Local data showed that alertsystems had an impact on reducinglength of stay by 25% in sometumour groups (Figures 6 - 9).
Communication alerts weresignificantly effective for patientspreviously diagnosed with canceradmitted as an emergency (SherwoodForest Hospitals NHS FoundationTrust case study 2008). Local dataidentified a number of admissionsaverted, this data is not captured byHES.
Emergency
12 | Consolidation Report - From testing to spread

10
9
8
7
6
5
4
3
2
1
0
Ave
rag
eLe
ng
tho
fSt
ay(d
ays)
2006 - 2007 2007 - 2008 2008 - 2009
NHS Trust
NorthamptonGeneral Hospital
NHS Trust
United LincolnshireHospitals NHS Trust
Sherwood ForestHospitals NHS
Foundation Trust
Figure 6: Average Length of Stay: Emergency Lung Inpatients
Figure 7: Communication Alert for Recurring Admissions AcrossTumour Sites - Kings Mill Hospital.
15
10
5
0
Tim
e(d
ays)
Breast Gynaecological Lower GI Lung
15
Pre RAPA April 2009Post RAPA
Feb 2007RAPA Trial
6
9.58
665
6
43 3
4
Comparison of median length of stay for non-elective breast, gynaecological,lower GI and lung patients, pre, during and post implementation of RAPA
Consolidation Report - From testing to spread | 13
Based on local trust data.
HES data.
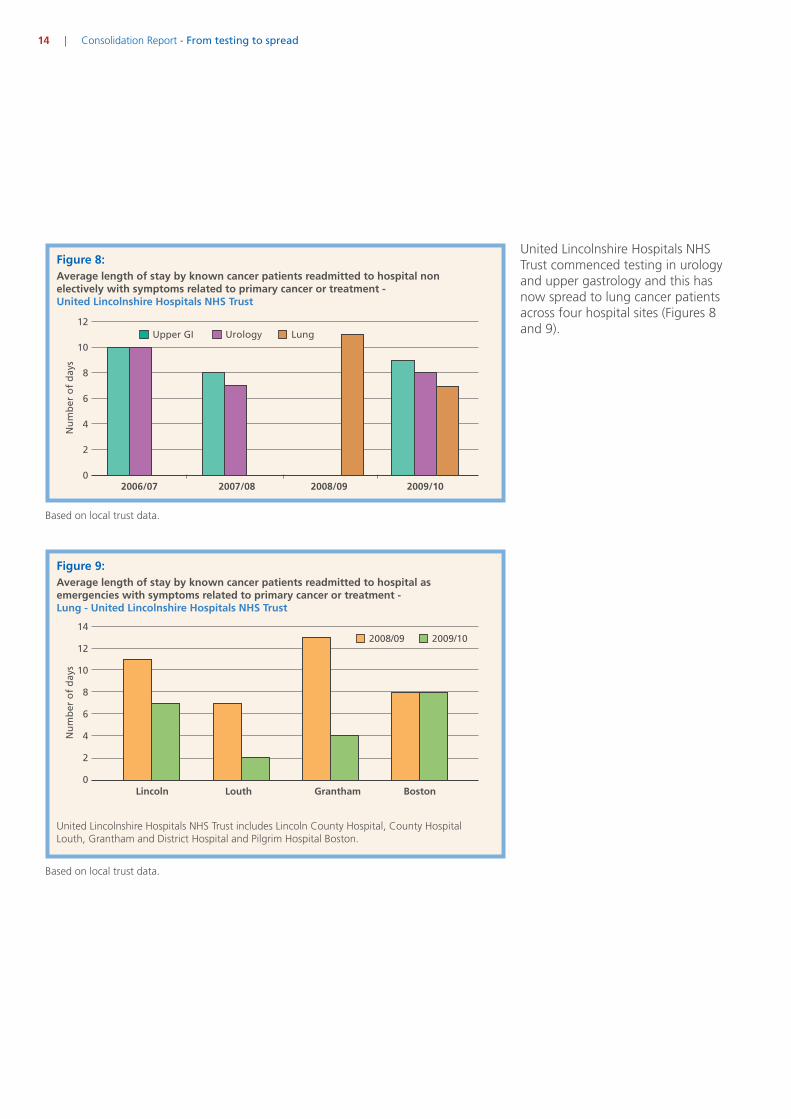
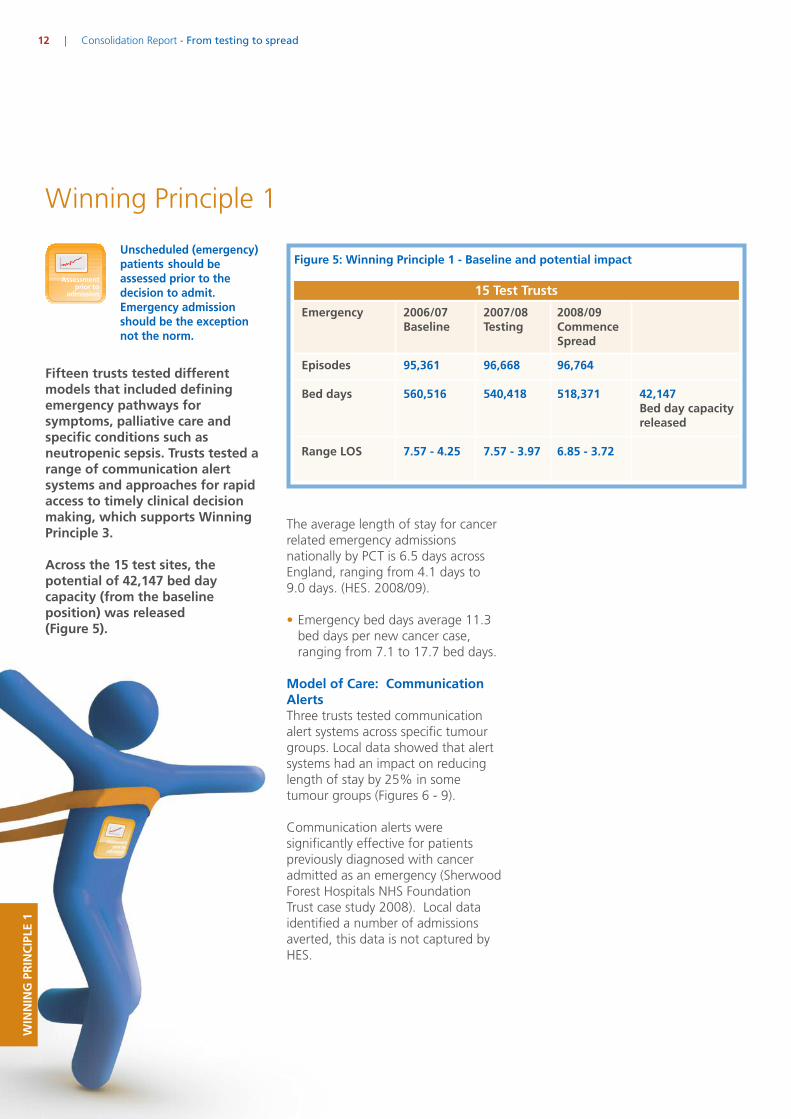
Figure 8:
14 | Consolidation Report - From testing to spread
12
10
8
6
4
2
0
Nu
mb
ero
fd
ays
Upper GI Urology Lung
2006/07 2007/08 2008/09 2009/10
Average length of stay by known cancer patients readmitted to hospital nonelectively with symptoms related to primary cancer or treatment -United Lincolnshire Hospitals NHS Trust
Figure 9:Average length of stay by known cancer patients readmitted to hospital asemergencies with symptoms related to primary cancer or treatment -Lung - United Lincolnshire Hospitals NHS Trust
14
12
10
8
6
4
2
0
Nu
mb
ero
fd
ays
2008/09 2009/10
Lincoln Louth Grantham Boston
United Lincolnshire Hospitals NHSTrust commenced testing in urologyand upper gastrology and this hasnow spread to lung cancer patientsacross four hospital sites (Figures 8and 9).
Based on local trust data.
Based on local trust data.
United Lincolnshire Hospitals NHS Trust includes Lincoln County Hospital, County HospitalLouth, Grantham and District Hospital and Pilgrim Hospital Boston.

Model of Care: Emergency andSymptom Pathways13 trusts defined emergencypathways and symptom specificpathways. Models of care to improvedaily clinical decision-making(Winning Principle 3), emergencytriage approach to identify thepatients preferred place of care(Figure 10).
9
8.5
8
7.5
7
6.5
6
5.5
5
4.5
4
Ave
rag
eLe
ng
tho
fSt
ay(d
ays)
2006 - 2007 2007 - 2008 2008 - 2009
Trust
Barts andThe LondonNHS Trust
BlackpoolFylde
& WyreHospitals
NHSFoundation
Trust
Brighton& Sussex
UniversityHospitalsNHS Trust
ChristieHospital
NHSFoundation
Trust
GreatWesternHospital
NHSFoundation
Trust
Hull &East
YorkshireHospital
NHSTrust
MiltonKeynesHospital
NHSFoundation
Trust
OxfordRadcliffeHospitalsNHS Trust
RoyalBerkshire
NHSFoundation
Trustt
St Helensand
KnowsleyHospitalsNHS Trust
TheHillingdonHospital
NHS Trust
TheWhittington
HospitalNHS Trust
UniversityHospitals ofMorcambeBay NHS
Trust
Figure 10: Emergency and Symptom PathwaysAverage Length of Stay All Cancers (All Episodes). Diagnosis = All Admission.Method Group = Emergency. Class of Patient = Ordinary Admission
Consolidation Report - From testing to spread | 15
HES data.

Winning Principle 2
Ten trusts defined electivepathways and models includingthe 23 hour for Breast CareModel, enhanced recoveryapproaches and shifting inpatientprocedures to an ambulatorysetting.
The trusts potentially released67,953 bed days (from thebaseline position) (Figure 11).
WINNINGPRINCIPLE2
Figure 11: Winning Principle 2 - Baseline and potential impact
2006/07Baseline
2007/08Testing
2008/09CommenceSpread
10 Test Trusts
Episodes
Bed days
Range LOS
52,852
358,884
7.81 - 5.08
53,149
344,064
7.36 - 4.97
48,182
290,931
7.07 - 4.79
67,953Bed day capacityreleased
The average length of stay for cancerrelated elective admissions nationallyby PCT is 7.2 elective bed days pernew case. The range was from 4.9days to 11.5 (HES 2008/09).
Clinical Models of Care: Breast 23Hour Care ModelThe Breast 23 hour care model wassignificantly successful. It started inone trust with one clinician andspread across the Pan BirminghamCancer Network. Clinicians engagedwith the testing following a visit toKings College Hospital NHSFoundation Trust where clinicians hadtested not inserting wound drains.This practice was incorporated intothe 23-hour pathway and formedpart of testing with furtherimprovements in clinical decision-making, clinical practice, design ofthe pathway, pre-assessment,discharge planning and teamworking.
All patients should beon defined inpatientpathways based on theirtumour type and reasonsfor admission. Elective
16 | Consolidation Report - From testing to spread

Pan Birmingham local data (April -December 2009) demonstrates thespread and adoption position of the23 hour breast care model across thecancer network. Figure 12 shows theoverall delivery of wide local excisionsis 94% with 548 patientsexperiencing this pathway approach.Mastectomies are currently at 49%(348 patients) and the approachcontinues to spread.
Consolidation Report - From testing to spread | 17
MastectomyHOSPITAL SITE
April to December 2009 (9 months)
11+ 6 to10 2 to 5 1 0
0% 0% 15% 43% 42%
0% 6% 6% 22% 67%
0% 0% 1% 46% 53%
1% 0% 1% 16% 83%
0% 10% 10% 30% 50%
1% 0% 5% 43% 51%
0% 1% 10% 74% 14%
0% 1% 5% 39% 55%
11+ 6 to10 2 to 5 1 0
2% 5% 51% 37% 5%
0% 13% 31% 31% 25%
5% 10% 25% 56% 5%
0% 4% 16% 52% 29%
0% 27% 55% 9% 9%
9% 12% 43% 30% 6%
1% 6% 54% 36% 3%
3% 9% 39% 38% 10%
94% 49%
Breast Conserving Surgery (wide local excisions)
LENGTH OF STAY (DAYS)
City Hospital provides 94% of all breast surgery within 0 to 1 days.The network achieves a combined total of 74% in 0 to 1 days
Data taken from CBSA and relates to payments made.
Figure 12: 23 Hour Breast Care Model across the Pan Birmingham Cancer Network
Pan Birmingham Cancer Networkoverall delivered the 23 hour breastcare model (at the time of the review)to 74% of all breast surgery patients(excluding reconstructions).
The original test site at the CityHospital now delivers the 23 hourbreast care model to 94% of allbreast surgery patients (excludingreconstructions).

Figure 13: 23 Hour Breast Model - Potential Value for Money
Test sites
Sandwell & WestBirmingham
University HospitalBirmingham
BirminghamHeartlandsHospital
Good HopeHospital
Walsall Hospital
Network Total
Total numberof episodes
473
394
270
156
231
1524
Potential cost savings for breast across the Pan Birmingham Cancer Network
Averagelength ofstay
5.32
4.04
5.19
5.03
3.95
4.70
Inpatientcost at £200per day
503,272
318,352
280,260
156,936
182,490
1,432,560
Day casecost at £250per day
118,250
98,500
67,500
39,000
57,750
381,000
Potentialsavings
385,022
219,852
212,760
117,936
124,740
1,051,560
7.57
6.56
5.55
4.54
3.53
2.52
1.51
0.50
Ave
rag
eLe
ng
tho
fSt
ay(d
ays)
2006 - 2007 2007 - 2008 2008 - 2009
SHA of Trust/Admission Method
Elec
tive
Emer
gen
cy
EastMidlands
SHA
Elec
tive
Emer
gen
cy
East ofEngland
SHA
Elec
tive
Emer
gen
cy
LondonSHA
Elec
tive
Emer
gen
cy
NorthEastSHA
Elec
tive
Emer
gen
cy
NorthWestSHA
Elec
tive
Emer
gen
cy
SouthCentral
SHA
Elec
tive
Emer
gen
cy
South EastCoastSHA
Elec
tive
Emer
gen
cy
SouthWestSHA
Elec
tive
Emer
gen
cy
WestMidlands
SHA
Elec
tive
Emer
gen
cy
Yorkshire &the Humber
SHA
Figure 14: Average Length of Stay: Breast Inpatient AdmissionsAcross the West Midlands 15 out of17 PCTs had the lowest averagelength of inpatient stay for breastsurgery (Figure 14).
The future potential of the 23hour Breast Care Model issignificant if spread• National average length of stay forbreast surgery is 2.8 days (HES2009)
• 34,000* new cases are registeredper annum in England.
• 34,000 x 2.8 days = 95,200 beddays. Lower estimate £200 per bedday = £560 per patient.Net cost £19.04m
• 23 Hour Breast Model - 34,000new patients = 34,000 bed days= £6.8m.
*Cancer Registrations in England 2000
18 | Consolidation Report - From testing to spread
Potential savings identifiedThe realisation of these efficiencybenefits across the Pan BirminghamCancer Network was a by-product ofimproving quality. It was locallydetermined how to use the releasedcapacity and capture the efficiencygains (Figure 13).
During testing the figure of £200 perday inpatient bed day is based on thelower estimate of costs used toprovide a baseline figure and toillustrate the potential.
Based on local trust data.

Clinical Models of Care: Enhancedrecovery approachesEnhanced recovery approachestested in colorectal (Figure 15),gynaecology (Figure 16), and urology,reduce length of stay from thebaseline position.
The learning from this testing hasbeen shared with the Department ofHealth Enhanced Recovery Partnershipprogramme.
14
12
10
8
6
4
2
0
Ave
rag
eLe
ng
tho
fSt
ay(d
ays)
2006 - 2007 2007 - 2008 2008 - 2009
Trust/Hospital Site
City HospitalSandwell and West
Birmingham HospitalsNHS Trust
Whipps CrossUniversity Hospital
Whipps Cross UniversityHospital NHS Trust
Queen Mary’s HospitalSouth London
Healthcare NHS Trust
Figure 15: Colorectal Enhanced Recovery - Winning Principle 2Average Length of Stay: Elective Inpatients Lower GI Procedures.(Lower GI Neoplasm. Procedure L1 = Colectomy, Excision of Rectum)
9
8
7
6
5
4
3
1
0
Ave
rag
eLe
ng
tho
fSt
ay(d
ays)
2006 - 2007 2007 - 2008 2008 - 2009
Trust/Hospital Site
Queen Elizabeth The Queen Mother HospitalEast Kent Hospitals University
Figure 16: Gynaecology Enhanced Recovery - Winning Principle 2Average Length of Stay: Elective Inpatients Gynaecological Procedures.(Gynaecological Neoplasm. Procedure L1 = Procedure on Uterus)
Consolidation Report - From testing to spread | 19

Model of Care: Shifting carefrom an inpatient settingShifting care to an alternative settingwas tested by Barking Havering andRedbridge Hospital NHS Trust.
The testing focused on shiftingprocedures traditionally carried out inhaematology and oncology inpatientbeds to a day case setting (Figure 17).
The local data in figure 18 illustratesthe potential investment and thevaluing of patients’ time.
Figure 17: Barking, Havering and Redbridge Hospital NHS Trust - Baseline & progress
(Elective Day Care and Inpatients Breast. Gynaecology, Haematology, Head & Neck,Lower GI, Thorax, Upper GI, Urology)
20 | Consolidation Report - From testing to spread
700
600
500
400
300
200
100
0
Nu
mb
ero
fEp
iso
des
Breast Gynaecology Haematology Head & Neck
2006
-200
7
2007
-200
8
2008
-200
9
2006
-200
7
2007
-200
8
2008
-200
9
2006
-200
7
2007
-200
8
2008
-200
9
2006
-200
7
2007
-200
8
2008
-200
9
Tumour Group/Year
Day case admission - Barking, Havering andRedbridge Hospitals NHS Trust - Queen’s Hospital
Ordinary admission - Barking, Havering andRedbridge Hospitals NHS Trust - Queen’s Hospital
700
600
500
400
300
200
100
0
Nu
mb
ero
fEp
iso
des
Lower GI Thorax Upper GI Urology
2006
-200
7
2007
-200
8
2008
-200
9
2006
-200
7
2007
-200
8
2008
-200
9
2006
-200
7
2007
-200
8
2008
-200
9
2006
-200
7
2007
-200
8
2008
-200
9
Tumour Group/Year
Based on local trust data.

Barking, Havering and Redbridge NHSTrust is continuing testing andspreading the principles makingimprovements in:
• Direct access for Sickle Cellpatients.
• Further reducing wasted patientstime for some procedures inassessment beds.
• Testing protocols for outpatientmanagement of NeutropenicSepsis.
• Further shifting care to andreducing unnecessary inpatientadmissions.
• Testing whether assessment bedscould be included in the 4-hourbed wait target?
Hickman line insertion
Blood Transfusion
Ascitic Drain
CT Guided Biopsy
US Guided Biopsy
HDR Full Insertion
IV Antibiotics
Total Cost Saving
Average no.of hoursspent asinpatient(baseline data)
Procedure
92
35
76
128
20
24
113
Average no.of hoursspent asday case(baseline data)
Average no.of hourssaved perprocedure
Average costper inpatientprocedure(baseline data basedon £8.30 per hour)
Average costper day case(audit databased on £18.75per hour)
Number ofpatientsthrough dayunit duringaudit
Releasedcost forauditperiod
4.5
7.5
9
6.5
6
7
7.5
87.5
27.5
67
121.5
14
17
105.5
£763.60
£290.50
£630.80
£1062.40
£166.00
£199.20
£937.90
£84.37
£140.62
£168.75
£121.87
£112.50
£131.25
£140.62
5
14
9
6
3
9
2
£3393.15
£2098.32
£4158.45
£5643.18
£160.50
£611.55
£1594.56
£17,659.71
Fig 18: Quantifying the impact and valuing patients time
Consolidation Report - From testing to spread | 21
Model of Care: Parencentesis inthe hospice settingEast Sussex NHS Trust tested avertinginpatient admissions for patients fromthe local hospice that required aparencentesis, and tested this beingundertaken at the hospice. Theconcept was tested successfully, andspread to another site, althoughnumbers of patients are small. Theoutcomes of testing has spread andintegrated into local emergencyimprovement work.

Winning Principle 3
This is not a stand-alone principleas timely clinical decision-makingis a key component integratedwithin all the principles,pathways and models of care.Two trusts, Brighton and SussexUniversity Hospitals NHS Trustand The Whittington HospitalNHS Trust tested this principleacross oncology.
WINNINGPRINCIPLE3
The Whittington HospitalNHS TrustThe local approach was to have theavailability of an acute oncologist andrapid access clinics.
Access to daily clinical decisionmaking has:
• Reduced unnecessary lengths ofstay for new unknown cancers -from 17.1 days to 12.1 days. Areduction of five days forpreviously unknown cancerpatients who were admitted asemergencies compared with theyear before adopting WinningPrinciple 3 for acute oncology.
• Made a reduction in averagelength of stay of 3.7 days forknown cancer patients.
• Significantly decreased the numberof unnecessary tests patientswould have undergone. This valuespatients’ time and improves thepatient experience.
Clinical decisions shouldbe made on a daily basisto promote proactive casemanagement.
22 | Consolidation Report - From testing to spread
Brighton and Sussex UniversityHospitals NHS TrustTested several strategies to maximisetimely clinical decision-making whichincluded improved communicationsbetween clinical teams, weekly MDTward discussions, Daily paper reviewof inpatients including outliers,admission priority assessment andagreed pathway trigger points toavoid discharge delays.
Evidence relating to surgical, medicaland haematology daily clinicaldecision making appears to be wellestablished and built into consultantjob plans. This does not appear to bethe case in oncology. Furtherevidence may emerge in this areafrom the National ChemotherapyImplementation Group.

Winning Principle 4
WINNINGPRINCIPLE4
Patient and carers need toknow about their conditionand symptoms to encourageself-management and toknow who to contactwhen needed.
As part of the testing, all sites wereencouraged to engage patients inpromoting self-care. Variousapproaches were used during thetesting including patient education,information, production of a DVD andtelephone help lines as central contactpoints. The view from the reviewteam was that testing had notdemonstrated or captured ‘real self-management’ and only a few siteshad been able to quantify the impactof the interventions during testing. Itappeared that once implemented orproducts produced the capture ofimpact data/audit was discontinued,although patient satisfaction auditscontinue.
We know that patients are receivinginformation and that for example,Blackpool, Fylde and Wyre NHSFoundation Trust has distributed aDVD to over 500 patients across thecancer network. The DVD is given topatients on chemotherapy, helpingthem to identify the signs andsymptoms of neutropenic sepsis. TheDVD has been acknowledged as goodpractice and has been adopted byother areas.
There will be the opportunity tocapture more information from theNational Patient Survey regardinginpatient care and with the newemergency initiative this will providethe opportunity to focus on somespecific areas of self-caremanagement.
Consolidation Report - From testing to spread | 23
The patient’s stories in theDVD are very powerful andmake much more impact onother patients and carersabout the importance ofpresenting early.Lead cancer nurse
“”
This DVD is a good idea.Verbal information andleaflets don’t really sink inbecause it’s such a difficulttime. You can’t take it all in,it’s a bit too much, but I thinkthe DVD will stick in people’sminds.
“
”Husband of a patient

Summary: Consolidation of testingThe 25 test sites provided evidence ofprogress, potential impact and theongoing implementation of thewinning principles and models of carethat improve quality of the patientexperience and productivity. Theprogress reported here demonstratesthat test trusts have moved frominitial testing and that improvementcontinues. The quantitative figureshowever should not be judged inisolation of the organisational contextand complexities of change involved.
24 | Consolidation Report - From testing to spread
4 10 26
2 6 16
1 9 17
4 6 9
1 18
8 12 26
3 6 8
1 2 13
2 2 14
8
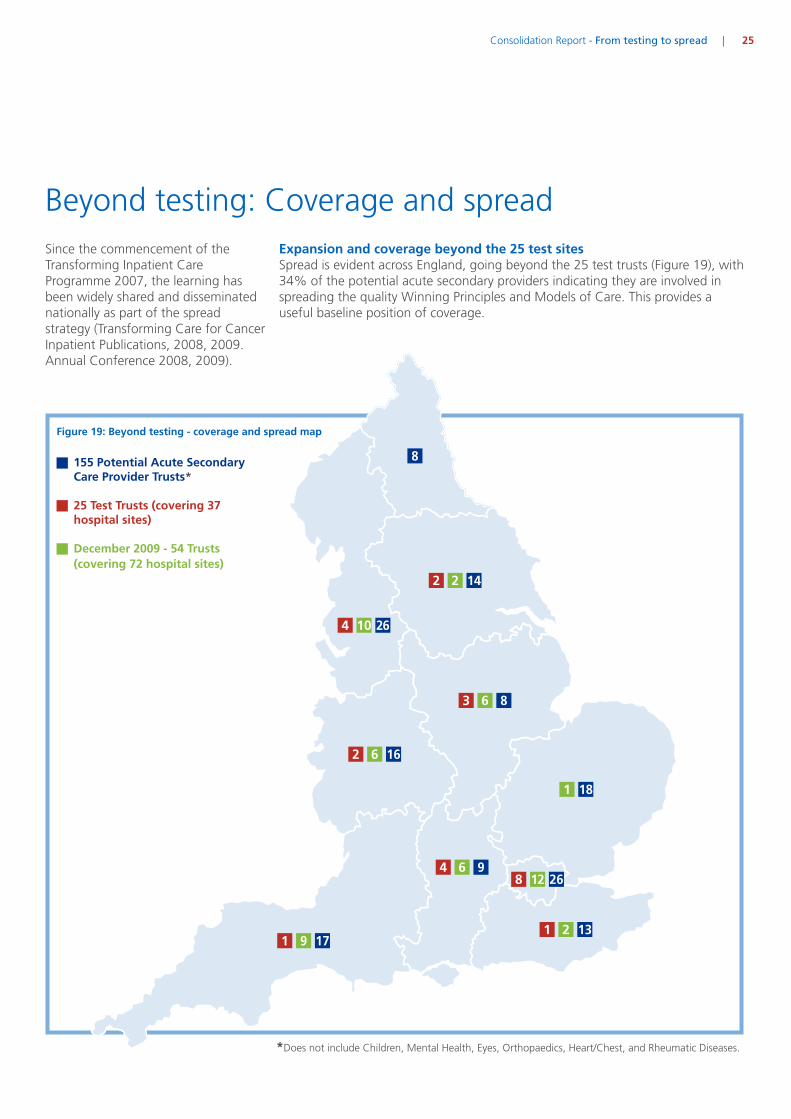
*Does not include Children, Mental Health, Eyes, Orthopaedics, Heart/Chest, and Rheumatic Diseases.
Beyond testing: Coverage and spreadSince the commencement of theTransforming Inpatient CareProgramme 2007, the learning hasbeen widely shared and disseminatednationally as part of the spreadstrategy (Transforming Care for CancerInpatient Publications, 2008, 2009.Annual Conference 2008, 2009).
Consolidation Report - From testing to spread | 25
Figure 19: Beyond testing - coverage and spread map
155 Potential Acute SecondaryCare Provider Trusts*
25 Test Trusts (covering 37hospital sites)
December 2009 - 54 Trusts(covering 72 hospital sites)
Expansion and coverage beyond the 25 test sitesSpread is evident across England, going beyond the 25 test trusts (Figure 19), with34% of the potential acute secondary providers indicating they are involved inspreading the quality Winning Principles and Models of Care. This provides auseful baseline position of coverage.

EmergencyPathways
SHA NeutropenicSepsis
EnhancedRecovery
23 HourBreast
ShiftingProcedures
Figure 20: Spread and adoption activity by SHA
East Midlands
East of England
London
North West
South Central
South East Coast
South West
West Midlands
Yorkshire & the Humber
North East
CommunicationAlerts
Clinical DecisionMaking
SelfManagement
Spread activityIn some areas, to accelerate the paceof spread, the tested models of carehave been identified as a healthcommunity priority and brought in aspart of local commissioning for qualityand innovation framework qualityaccounts (CQuINS).
26 | Consolidation Report - From testing to spread

Spread SurveyDecember 2009 - January 2010
Number of Hospital Sites
0 5 10 15 20 25 30
Communications Alert Systems - Winning Principle 1
Emergency Pathways - Winning Principle 1
Palliative Care Pathways - Winning Principle 1
23 Hour Breast Care Surgical Model - Winning Principle 2
Enhanced Recovery Pathway - Winning Principle 2
Patient Transfers/Repatriation - Winning Principle 2
Shifting Procedures from Inpatients to Day Care - Winning Principle 2
Carcinoma of Unknown Primary - Winning Principle 2
Clinical Decision Making - Winning Principle 3
Neutropenic Sepsis - Winning Principle 1 & 4
23 Hour Helpline - Winning Principle 4
Acute Oncology Model - Winning Principle 1 & 3
Figure 21: Extent of spread
Consolidation Report - From testing to spread | 27
Figure 21 highlights which quality Winning Principle is being adopted and spread.
• 72 hospital sites are activelyspreading the improvements. Somesites are embarking on more thanone improvement activity.
• From the evidence reviewed(December 2009) - there arecurrently 183 improvement activitiessupporting spread across England.
Good ideas and innovations arespreading and being adopted byorganisations, clinicians and managersacross England with quality as thekey driver.

35
30
25
20
15
10
5
0
Nu
mb
ero
fPa
tien
ts
ImplementationPlan
Use of OpinionLeaders
Benchmarking PatientGroups
CommissioningAgreements
NoneCommunications& Awareness
SharedComparative Data
Figure 24: Reported levers for spreadDecember 2009
When comparing the reported leversof spread (Figure 24) against theTransforming Inpatient Framework,seven of the elements have beenidentified. Figure 23 highlights theseelements.
28 | Consolidation Report - From testing to spread
Levers for spread
Fig 22: The Transforming InpatientFramework for Spread
SpreadMaking theConnections
A Visionfor QualityImprovement Systematic
ImprovementApproach
OrganisationalCultureand Fit
SpreadSimple
Principles &Messages
LeadershipEngagementAccountability
Alignmentwith
Opportunities& LeversPatient
Centred
Learning& Unlearning
CollaborationPartnerships& TeamWorking
ContinuousMonitoringProgress &Impact
LinkedStrategic &OperationalChange
SpreadStrategy
The learning from the TransformingCancer Inpatient Care Programmeremains practically based as it drawson real experiences and the challengesof taking a good idea and spreading itfurther to benefit more patients. Thelearning from the test sites has beenused to develop a TransformingInpatient Framework for Spread(2009); Driver (2008); Williamson(2007); (Figure 22). The framework isa tool to help support otherorganisations and teams in their questto spread good quality innovations.
(NHS Improvement 2009)
Figure 23: Sites identifying seven elements of theTransforming Inpatient Framework for Spread
SpreadMaking theConnections
A Visionfor QualityImprovement Systematic
ImprovementApproach
OrganisationalCultureand Fit
SpreadSimple
Principles &Messages
LeadershipEngagementAccountability
Alignmentwith
Opportunities& LeversPatient
Centred
Learning& Unlearning
CollaborationPartnerships& TeamWorking
ContinuousMonitoringProgress &Impact
LinkedStrategic &OperationalChange
SpreadStrategy

Consolidation Report - From testing to spread | 29
ConclusionFrom testing to spreadThe review has shown that theTransforming Inpatient CareProgramme continues to makeprogress. Spreading and encouragingadoption and adaption of the winningprinciples and new models of careacross England, but there is still moreto be done and the pace needs to beaccelerated.
The new levers supporting spreadsuch as QIPP, GP commissioning and apatient led NHS will support the drivefor change and further adoption ofgood practice.
Spread and adoption is not easy andrequires a multi-level of methods,levers and factors to create, inspireand connect to people, organisationsand within the nature of the currenthealth landscape. The programme willcontinue to support spread anddisseminate the practical learningacross the NHS to benefit all patients.

30 | Consolidation Report - From testing to spread
Acknowledgements and referencesAcknowledgements
Transforming Inpatient CareProgramme Test Sites
Professor Sir Mike RichardsNational Director for Cancer andEnd of Life Care, National CancerAction Team
Celia Ingham ClarkNational Clinical Lead and Chair ofTransforming Inpatient CareProgramme
NATCANSAT (National CancerServices Analysis Team) with aspecial thanks to Neal Jones
Thank you to the organisationswho responded to the spreadsurvey.
Enhanced Recovery PartnershipProgramme
References
NHS Improvement - TransformingInpatient Care ProgrammeAn integrated approach - Thetransferability of the WinningPrinciples - Sharing the learning(July 2010)
NHS Improvement - TransformingInpatient Care ProgrammeFrom Testing to Spread - Sharing theknowledge and learning fromorganisations spreading the WinningPrinciples (July 2010)
NHS Improvement - TransformingCare for Cancer Patients: Spreadingthe Winning Principles and GoodPractice (July 2009)
NHS Improvement – TransformingInpatient Case Studies (July 2009)
NHS Cancer Reform Strategy (2009) -Achieving Local Implementation -second annual report
NHS Improvement - Meeting thechallenge together... delivering care inthe most appropriate setting (October2008)
NHS Improvement - The WinningPrinciples: Transforming Inpatient CareProgramme for Cancer Patients (July2008)
Letter from David Nicholson CBE ,NHS Chief Executive. Implementingthe Next Stage Review visions: thequality and productivity challenge(Gateway ref: 12396)
Department of Health, EnhancedRecovery Partnership Programme:Delivering Enhanced Recovery:Helping patients to get better soonerafter surgery (2010)
National Chemotherapy AdvisoryGroup Guidance (August 2009).National Cancer Action Team.
Driver A. (2008). Factors effectingachievement of cancer waiting timetargets in NHS Trusts; an exploratorystudy. Unpublished thesis, DoctorateProfessional Studies in Health;Middlesex University, London
Williamson J. (2007). The criticalfactors for whole system change of aclinical specialty identified through theCancer Services Collaborative‘Improvement Partnership’.Unpublished thesis, DoctorateProfessional Studies in Health;
Middlesex University, London
Cancer Reform Strategy 2007
Excellence in Oncology Awards 2009 -British Oncology Association
NHS Improvement websitewww.improvement.nhs.uk
Krishna K Varadhana, Keith R. Nealb,Cornelius H.C. Dejongc, Kenneth C.H.Fearond, Olle Ljungqviste, Dileep N.Loboa.
The enhanced recovery after surgery(ERAS) pathway for patientsundergoing major elective opencolorectal surgery. A meta-analysis ofrandomised controlled trials.
Key contacts
Angie RobinsonNational Improvement [email protected]
Marie TarpleeNational Improvement [email protected]
Catherine [email protected]


3rd Floor | St John’s House | East Street | Leicester | LE1 6NB
Telephone: 0116 222 5184 | Fax: 0116 222 5101
www.improvement.nhs.uk
NHS Improvement
With over ten years practical service improvement experience in cancer,diagnostics and heart, NHS Improvement aims to achieve sustainableeffective pathways and systems, share improvement resources andlearning, increase impact and ensure value for money to improve theefficiency and quality of NHS services.
Working with clinical networks and NHS organisations across England,NHS Improvement helps to transform, deliver and build sustainableimprovements across the entire pathway of care in cancer, diagnostics,heart, lung and stroke services.
Delivering tomorrow’simprovement agendafor the NHS
HEART
LUNG
CANCER
DIAGNOSTICS
STROKE
©NHSIm
provem
ent20
10|AllRigh
tsRe
served
|July20
10
NHSNHS Improvement