Considering and Starting Treatment for Depression & Anxiety
29
4/7/2021 1 Considering and Starting Treatment for Depression & Anxiety Abigail Schlesinger MD Goals and Objectives 2 At the completion of this program, participants should be able to: 1. Recognize the importance of the behavioral health differential diagnosis when prescribing medication for depression/anxiety 2. Describe a method to deploy components of their behavioral health toolbox(therapy strategy, safety plan, and/or medication) 3. Recognize the importance of appropriate follow-up for behavioral health interventions provided in pediatric primary care 1 2
Transcript of Considering and Starting Treatment for Depression & Anxiety

4/7/2021
1
Considering and Starting Treatment for Depression & Anxiety
Abigail Schlesinger MD
Goals and Objectives
2
At the completion of this program, participants should be able to:
1. Recognize the importance of the behavioral health differential diagnosis when prescribing medication for depression/anxiety
2. Describe a method to deploy components of their behavioral health toolbox(therapy strategy, safety plan, and/or medication)
3. Recognize the importance of appropriate follow-up for behavioral health interventions provided in pediatric primary care
1
2

4/7/2021
2
Therapeutic Toolbox
3
Follow-up
Non-medication Interventions
Safety Planning
Medication
Referral and Coordination
Nonmedication Interventions
4
Relationship
HELLPP Skills
Assessment
Health Behavior Interventions
BH Interventions
3
4

4/7/2021
3
Organizing the Session
5
Set Agenda
Recognize frustration/fears/anger/strengths & instill hope
• Listen and Ask targeted questions sleep, appetite, routines, school, friends, mood, hope/helplessness
Clarify Needs(assessment, differential, safety planning)
• I understand you are here for depression. Today I am going to ask questions and listen to you so that I can better understand your concerns.Then we will come up with initial goals/strategies to improve your mood
Create clear plans
GAD-7
6
5
6

4/7/2021
4
PHQ-9
7
8
Depression: Assessment with SIG-E-CAPS
Depressed and/or irritable mood PLUS….
Sleep problem(up or down)
Interest deficit (anhedonia)
Guilt (worthlessness, hopelessness, regret)
Energy deficit
Concentration deficit
Appetite changes(up or down)
Psychomotor agitation or retardation
Suicidality
7
8

4/7/2021
5
9
DSM 5 Criteria: Major Depressive Disorder
1. Sad, down, negative mood, empty feeling, hopelessness, irritability in children
2. Anhedonia, decreased interest or loss of pleasure
3. Changes in sleep
4. Changes in appetite
Irritable, easily frustrated, argumentative. Focused on negative events, interprets events as negative, discounts positives. “I don’t care” attitude
Not enjoying or quitting activities; Subjective report or observed by others
May sleep/eat more or less.
10
DSM 5 Criteria: Major Depressive Disorder
5. Decreased concentration,
decisiveness
6. Psychomotor agitation or
retardation, observable by others
Easily swayed by others, changes mind, may question if developed ADHD, amotivation
Complaints of feeling agitated, noted pacing/ increased negative energy, or “couch potato”, amotivation
9
10

4/7/2021
6
11
DSM 5 Criteria: Major Depressive Disorder
7. Complaints of fatigue or
decreased energy
8. Feelings of
worthlessness or
excessive/inappropriate
guilt
9. Death wish, suicidal
ideation
Regardless of increased or decreased sleep
Negative about self, low self esteem, may feel responsible for events out of their control, discount positives and focus on negatives
May think family would be better off without them for fleeting moments or chronically think life isn’t worth it, want to hurt self but no plan, or have a plan, and/or intent
12
DSM 5 Anxiety Disorders• Generalized Anxiety Disorder
• Social Anxiety Disorder
• Separation Anxiety Disorder
• Selective Mutism
• Specific Phobia
o Animal, natural environment, blood-injection-injury, situational, other
• Panic Disorder
• VS Panic as a part of depression
• Other Specified Anxiety Disorder
• Also consider: Somatoform Disorder, OCD
11
12
4/7/2021
7
13
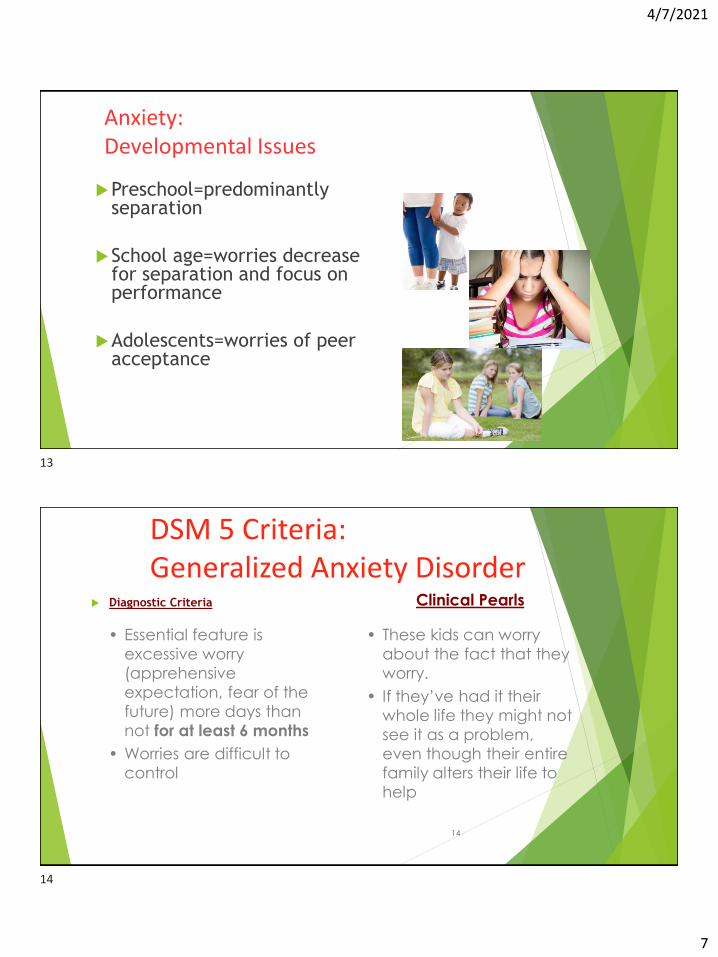
Anxiety: Developmental Issues
Preschool=predominantly separation
School age=worries decrease for separation and focus on performance
Adolescents=worries of peer acceptance
14
DSM 5 Criteria: Generalized Anxiety Disorder
Diagnostic Criteria Clinical Pearls
• Essential feature is
excessive worry
(apprehensive
expectation, fear of the
future) more days than
not for at least 6 months
• Worries are difficult to
control
• These kids can worry
about the fact that they
worry.
• If they’ve had it their
whole life they might not
see it as a problem,
even though their entire
family alters their life to
help
13
14

4/7/2021
8
15
DSM 5 Criteria:Generalized Anxiety Disorder Diagnostic Criteria Clinical Pearls
• In children, must have one of
the following:
o c/o restlessness
o easily fatigued
o difficulty concentrating
o irritability
o muscle tension
o sleep disturbance
• Be alert for this diagnosis
when a child and/or
family is concerned
about ADHD but the
teacher reports only
minimal inattentive
symptoms.
• Teachers often love
these kids.
16
GAD: Assessment
Most common anxiety disorder diagnosis
Screening questions Would you describe yourself as a worrier?
Ask the kid or parents about bedtime.
“What if” questions
Give examples of common worries—the weather, robbers, grades, terrorism, health concerns.
Ask teens if they worry about their future
15
16

4/7/2021
9
17
DSM 5 Criteria:Social Anxiety Disorder Diagnostic Criteria Clinical Pearls
• Anxiety caused by exposure to a feared social situation
o Exposed to scrutiny
o Must include peer settings
o Fear of embarrassment/rejection by peers
• Attempt to avoid social situations or endure at great distress
o Children may cry, tantrum, freeze, or shrink from the exposure
• Symptoms present for at least 6 months
• May take a bad grade or skip school in order to avoid situation.
• Doesn’t mean that they are not social…they must have some age appropriate friendships.
• Will overuse texting/internet for communication
18
SAD: Assessment• Would you describe yourself as shy?
• When you are around your peers, do you worry about
saying the wrong thing? Getting embarrassed?
• Will you raise your hand in class?
• Will you order food at a restaurant?
17
18

4/7/2021
10
19
DSM 5 Criteria: Separation Anxiety Disorder
3+ of the following symptoms are present:
Distress with separation or anticipated separation
Worry about losing caregiver or harm coming to them
Illness, injury, disasters, death
Worry of untoward event causing separation
lost, kidnapped, illness
Physical complaints w/ separation or anticipated separation
Headaches, stomachaches. Sunday nights.
Persistent reluctance to leave home because of fear of separation
Persistent reluctance to sleep away from home or sleep without having caregiver near
Repeated nightmares of separation
20
DSM 5 Criteria: Separation Anxiety Disorder Onset from preschool until 18 years of age
Duration at least 4 weeks
Developmentally inappropriate worry related to separation from home or to
whom one is attached
19
20

4/7/2021
11
21
Separation Anxiety Disorder: Assessment • Question parents but sometimes children may have insight.
• Ask about difficulties separating in general. Start with younger years—
preschool, school age.
• Ask how they did in preschool/kindergarten separating from parents
• Where do they sleep? Do they sleep alone?
• Will they go on overnights/sleepovers?
• History of separation anxiety increases risk of other anxiety disorders.
22
DSM 5 Criteria: Panic Disorder Recurrent, unexpected panic
attacks
Panic attack: an abrupt surge of
intense fear that reaches peak
within minutes
4+ symptoms
Attacks followed by 1+ months:
Persistent concern/worry about
more panic or their
consequences
Significant, maladaptive change
in behaviors
Chills or flushed
Dizzy, unsteady,
light-headed
Derealization depersonalization
Sweating Chest pain
Choking Palpitations, fast HR
Shaking GI distress Fear of dying
Fear of losing control/”going
crazy”
SOB, suffocating Paresthesias
21
22

4/7/2021
12
23
Panic Disorder: Assessment
• Have you ever had a panic attack?
o Describe it.
• Have you ever had anxiety so extreme that you noticed symptoms in your body?
• How long did it last?
• Are there precipitants?
• Are you avoiding certain things out of fear of having another panic attack?
• Panic disorder vs. panic attack specifier.
24
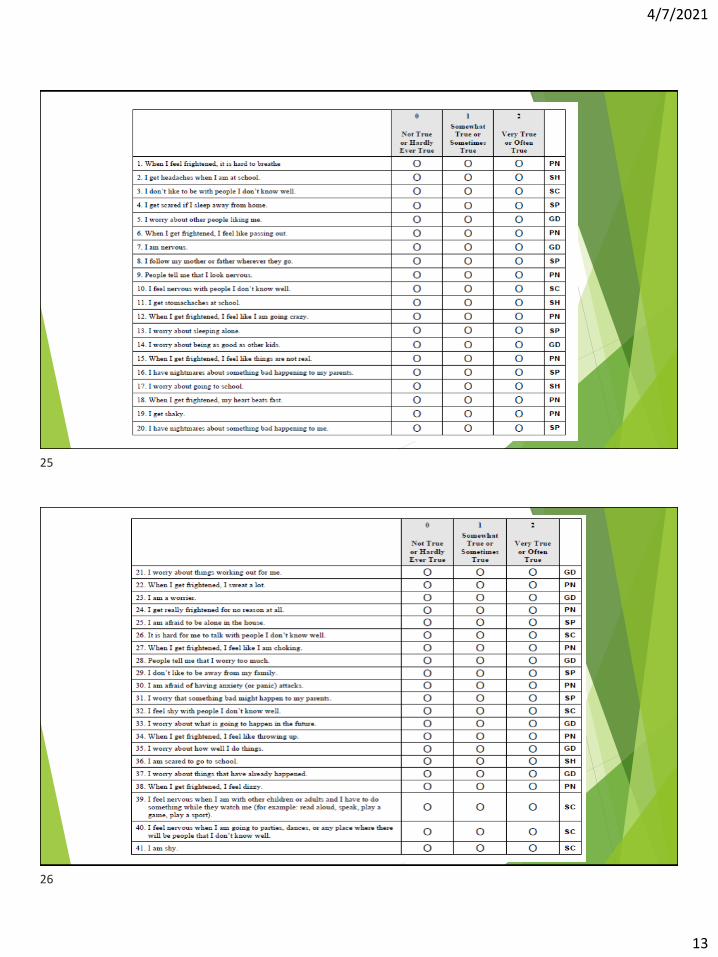
SCAReD Scoring
23
24
4/7/2021
13
25
26
25
26

4/7/2021
14
Initiation
Check(s)
27
1.Validate Diagnosis & Safety
2.Review Family History
3.Complete Consent/Assent
4.Clarify
Goals/Expectations/Safety Plan
5.Start Medication
6.Schedule follow-up
1. Validate Diagnosis & Safety
Review work-up - medical diagnosis & comorbid psychiatric
ASSURE SAFETY
Confirm Diagnosis
Review Behavioral Scales
SCARED parent and child(7-18) or GAD-7(13 and over 18)
PHQ9(or PHQ9a)
Consider Comorbidities that can Complicate Treatment
28
27
28

4/7/2021
15
Consider Psychiatric Comorbidities that
Could Complicate Treatment
Bipolar Disorder
Autistic Spectrum Disorder
Trauma
Substance Use
Eating Disorder
Suicidality
ADHD & ODD
Assess personal history
Are ASD driving “anxiety behaviors”
Acute or Chronic Trauma
Consider Substance Screen
Medication won’t work if you don’t have enough food to feed the brain
Assess past and Current
Consider Vanderbilts
29
Screening for Bipolar Disorder
“Was there ever a period of time, for more than a few days, that you(or
your child) didn’t need sleep, was on top of the world, and significantly
different than usual”
Note
This should be a clear change from baseline.
Child should be energetic during the day, ie not need a nap, not go to bed early
There is the most concern for bipolar disorder if the child was euphoric(more
happy than normal) or grandiose(felt that they were special, had special powers
etc) and there is no reason for it(ie it’s not the day before a holiday)
30
29
30

4/7/2021
16
Safety
Safety should be assessed in all
children and adolescents
31
32
Depression & Suicide
Untreated depression is the number one cause of suicide
Over 90% of children and teens who complete suicide have a mental health diagnosis (Mental Health: A Report of the Surgeon General)
Suicide is the #2 cause of death in the U.S. in those 10-24 years-old (NCHS)
31
32

4/7/2021
17
Risk Assessment
Begin with general questions: “Have you ever thought you would be better off
dead….your family would be better off without you”
Death wish: 20% prevalence
Progress to more specific questions: “Have you ever had a plan?” Means to
carry out?
Much less common
Gave away possessions?
Normalize:
Many times children who are feeling down or depressed describe having
thoughts that they don’t want to be alive. Have you ever felt that way?
Self-Injury and Suicidal behavioral
Having self-injury is risk-factor for suicide
There is a continuum from superficial self-injury to a suicide attempt
It is important to be able to differentiate in order to assess current risk
Most-often people can tell you that they were harming themselves to
Kill themselves and/or
Harm themselves(often described as coping mechanism to deal with psychological pain)
Ask what their method of self-injury is(where and with what)
Must ask about plans when kids have thoughts of suicide (even if they say “I would never
do it”)
34
33
34

4/7/2021
18
2. Review Family History
Bipolar Disorder
Response to Antidepressants
35
3. Consent/Assent
Parent should consent
Adolescent(and preferably child) should assent
36
35
36

4/7/2021
19
Consent/Assents Warn about side effects
More common that will probably go away if not too
bothersome(if they even occur)
Rare and concerning
Suicidality
Mania
Serotonin Syndrome
Other
Activation – some kids get increased energy during
the day, but have no trouble with sleep
37
SSRI Side Effects
• GI: nausea, abdominal pain, diarrhea, weight loss,
weight gain
• Headaches
• Easier bruising
• Sweating
• Light-headedness/dizziness
• Nervousness/restlessness
• Sleep difficulties: sedation/insomnia, vivid dreams
• Sexual dysfunction
• Irritability/activation
• Potential risk for suicidal thinking
• Precipitation of mania38
37
38

4/7/2021
20
FDA Black Box Warning
Based on a 2004 FDA review of reported adverse events
in 23 clinical trials which involved 4300 children and
adolescents, 9 different medications
Studies used two different measures for suicidal thoughts
and behavior
FDA clumped both thoughts and behaviors as “suicidality”
39
FDA Black box
First measure “event report”
Second measure – 17 of 23 studies “standardized forms”
questioned suicidality at each visit
Second measure technique considered more accepted
40
39
40

4/7/2021
21
FDA Black Box warning
Studies that used event reporting noted that 2% who
received placebo expressed increased suicidality
compared to 4% on medication.
Studied that used standardized forms that questioned
suicidality at each visit demonstrated a slight reduction
in suicidality for the medication group.
41
Black Box Warning
“Less than 2% of kids who start an SSRI will see an
increase in suicidality – often suicidal thoughts/ &
thoughts about self-injury. I am recommending this
medication because the benefits of treating this
depression/anxiety far outweigh any risk associated with
increased suicidality. But, because we take behavioral
health seriously I will follow-up with you closer while
starting medication to make sure that you are safe.”
42
41
42

4/7/2021
22
4. Clarify Goals/
Expectations/Safety
GOALS
What does the family/child want to get out of treatment?
Do you anticipate that this intervention will help?
Are goals aligned with treatment
43
Clarify Expectations: Roles
Providers in the practice
Help design & support the treatment plan that includes
evidence-based intervention
Maintain confidentiality, with caveats
Help child/adolescent get better
Parents & Patients
Participate in treatment
Help design and support the treatment plan
Speak up if things aren’t going well
44
43
44

4/7/2021
23
Expectations of Treatment
45
Expectation of Treatment
Getting better takes time
SSRIS take time – 4-12 weeks at therapeutic dose
Dose may need to be adjusted over time
So response needs to be monitored
Treatment works better if you participate in therapy
Safety Plan
1. Coping strategies
2. Adult(s) who child will contact if distressed
3. Emergency numbers
Write the plan down
Share with the family
45
46

4/7/2021
24
Safety Plan
1. Coping strategies
2. Adult(s) who child will contact if distressed
3. Emergency numbers
Write the plan down
Share with the family
5. Start Medication
You can increase medication weekly
You can start at typical starting dose or low starting dose
We often start at low dose for kids with a lot of
anxiety, somatic symptoms, young kids, or kids with
developmental concerns
48
47
48

4/7/2021
25
Choose a medication
Factors to consider in choosing
Fluoxetine has the most data
Sertraline has more data for anxiety
If you have any concern about bipolarity don’t use
Prozac
Celexa has histaminergic properties – helps belly pain
49
SSRI Titration Schedule
Medication Low
Starting
Dose
Typical
Starting
Dose
Typical
Effective
Dose
Typical
Dose
Range
Typical
Escalation
amount
Fluoxetine 5mg 10mg 20mg 60mg 10mg
Sertraline 25mg 50mg 100-150mg 200mg 25mg
Citalopram 5mg 10mg 20mg 40mg 10mg
Escitalopram 2.5mg 5mg 10mg 20mg 5mg
50
49
50

4/7/2021
26
SSRI General Information
51
Medication Typical
Effective Dose
Typical Dose
Range
Half-life Half-life of Active
Metabolites
Fluoxetine 20mg 60mg 2-3 days 2 weeks
Sertraline 100-150mg 200mg Males – 22.4
hours
females 32-
36
NA
Citalopram 20mg 40mg 20-35 hours NA
Escitalopram 10mg 20mg 20-35 hours NA
FIRST SSRI
CHECK
52
When
1-2 Weeks after starting medication
1.Check Side Effects
2.Check for Response
3.Review Expectations/Goals/Safety
4.Increase medication(if you started low)
51
52

4/7/2021
27
FIRST SSRI CHECK
We don’t expect clinical response yet.
So condition may continue to worsen
This check is predominantly to check
Side effects
Assure safety
Get medication to therapeutic dose
(Have a check in – in case it appears a higher level of care is needed)
53
FIRST SSRI Check Check side effects
“Are you concerned about side effects? Has anything changed that you are worried might
be related to medication”
“Have you had any thoughts about hurting yourself or anyone else?”
Check for response
“How are you doing?”
“On a scale of 1-10, 10 being as good as you could feel, how are you doing?”
Review goals
“Are you still hoping to work on ___”
Review safety plan
“Have you had to use your safety plan? Or How close have you come to using your safety
plan? Do you still feel like you could use your safety plan”
“Could you repeat your safety plan?”
Review expectations
“It’s early to see an impact of medication but you should see some positive response in 2-
4 weeks.”
“We look forward to your next check-in in 1-2 weeks”
Increase medication (if you started low) 54
53
54

4/7/2021
28
First SSRI Check
1. Check Side Effects
Are you concerned about side effects? Has anything changed that you are
worried might be related to medication”
“Have you had any thoughts about hurting yourself or anyone else?”
2. Check for Response
How are you doing?”
“On a scale of 1-10, 10 being as good as you could feel, how are you doing?”
3. Review Expectations/Goals/Safety
4. Increase medication(if you started low)
55
First SSRI Check1. Check Side Effects
2. Check for Response
3. Review goals
“Are you still hoping to work on ___”
→ Review safety plan
“Have you had to use your safety plan? Or How close have you come to using
your safety plan? Do you still feel like you could use your safety plan”
“Could you repeat your safety plan?”
→Review expectations
“It’s early to see an impact of medication but you should see some positive
response in 2-4 weeks.”
“We look forward to your next check-in in 1-2 weeks”
4.. Increase medication (if you started low)
56
55
56

4/7/2021
29
Ongoing Follow-up
General Comments
Remember these medications
actually work slowly
4 weeks for depression
Up to 12 weeks for anxiety
Assure patient has frequent
follow-up until getting better
And then at least monthly follow-
up until in full remission
What to do other than “how
have things been going”
1. Check Side Effects
2. Check for Response(GAD7, PHQ9)
3. Review Expectations/Goals/Safety
• Are expectations too high(or low)?
• Are their roving expectations?
4. Increase medication and/or
psychotherapy if not in full remission
and not generally improving weekly
57
Thank-you!
“Move Your Feet”/ “DANCE” /
“It's A Sunshine Day ... –
YouTube
58
57
58