Christer Carlsson, “The religious orders of knighthood in medieval ...
Upload
clementine-goldenCategory
view
217download
0
Consensus-based priority setting for elderly NSTEMI patients with
multi-morbidity
Niklas Ekerstad, MD Rurik Löfmark, MD Per Carlsson, Professor
National Centre for Priority Setting in Health Care, Sweden

Statistics Sweden. Population projection for Sweden 2004-2050
Background - Demography

Background – Key components regarding medical priority setting in Sweden
• The ethical platform (parliamentary decision)
• The Swedish national model for priority setting
• Evidence-based guidelines for priority setting

Background - Problems regarding evidence-based priority setting for elderly
patients with multi-morbidity
• Lack of a relevant description of needs (severity;potential effect of treatment) in terms of subgrouping (heterogenous population).
• Lack of evidence/limited applicability of evidence
”Our base of scientific expertise is weakest for the age groups (75+) that most often receive various types of treatments.” (The Swedish Council on Technology Assessment in Health Care)

Background – a critical case
Setting priorities within health care
when the evidence base is weak
- A critical case: Decision-making for frail elderly with acute cardiovascular disease and co-morbid conditions

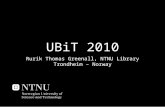
Background – Cardiologists´attitudes to suggested ways of improving clinical priority setting for elderly
NSTEMI patients with multi-morbidity
0
50
100
150
200
250
300
Betteradherence to
Nationalguidelines forheart disease
Specificevidence-
basedguidelines for
multiple-diseasedelderly
Localguidelines forthe care for
multiple-diseasedelderly
Moretreatmentstudies
includingmultiple-diseasedelderly
Positive
Negative
Ekerstad, N., Löfmark, R., Carlsson, P. Elderly with Multimorbidity and Acute Cardiac Disease: Doctors´ Views on Decision-Making. Accepted 091015. Scand J Public Health

Background – Description of the needs of NSTEMI patients in the national guidelines
AAA
A B
National guidelines regarding the measure coronary angiography for NSTEMI patients:Two categories based on disease-specific risk (cardiovascular risk)
A - high or medium cardiovascular risk: rank 2B - low cardiovascular risk: rank 6

Background – Proposed description of the needs of elderly patients with multi-morbidity

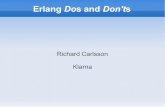
Background – Proposed categorization of the needs of elderly NSTEMI patients with multi-morbidity
Hög/måttlig risk Låg risk
CM+ CM- CM+ CM-
CFS+ CFS- CFS-CFS+ CFS+ CFS- CFS+ CFS-
I II III IV V VI VII VIII
High CVR Low CVR
CM+ CM-
CFS+ CFS+
CM+ CM-
CFS+ CFS+CFS- CFS- CFS- CFS-
CVR = Cardiovascular riskCM = Co-morbidityCFS = Clinical Frailty Scale

Background – Tentative relative ranking of the categories regarding coronary angiography from a theoretical standpoint
High cardiovascular risk
IV High rank
III Low-medium rank
II Low-medium rank
I Low rank
Low cardiovascular risk
VIII Medium-high rank
VII Low rank
VI Low rank
V Very low rank

Background – a pilot study regarding experts´priority setting for elderly NSTEMI
patients with multi-morbidity
• 6 experts validated 15 authentic NSTEMI cases, each case belonging to one of the eight model categories, and the model´s components
• For each case the measure coronary angiography was individually ranked; the convergence between the experts´rankings was evidently good.

Objectives• To re-validate the clinical cases and the model´s
components regarding their relevance
• To evaluate the interrater reliability concerning the experts´rankings regarding each category
• To compare the rankings of the experts and the guidelines
• To compare the rankings of the experts with the model´s suggested relative rankings

Methods
• Selection process of experts
• A questionnaire study
• Intra class correlation test

Results of the interimistic analysis (n=28) – Validation of the selected cases
0%
20%
40%
60%
80%
100%
Were the cases realistic?
Do you consider the cases to be realistic?
No
Yes,partly
Yes
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Intensive cardiac care Non-intensive cardiac care
Do you find the cases representative?
No
Yes,partly
Yes
“Very realistic cases! Daily problems!” (A male cardiologist at a small hospital)
“A few of the cases are typically found in non-cardiac care departments. “(A male cardiologist at a university hospital)

Results of the interimistic analysis – Convergence among the experts´rankings
Intra-class correlation test, two-way random, absolute:Single: 0,530 (0,359 – 0,751)Average: 0,964 (0,931 – 0,986)
The inter-rater reliability was good. The experts´rankings converge well.

Results of the interimistic analysis – Comparisons between different sources of rankings: guidelines and experts
Category Guidelines´ rankings
Experts´ rankings (mean)
IV 2 3.6
III 2 7.7
II 2 8.2
I 2 10
Category Guidelines´ rankings
Experts´rankings (mean)
VIII 6 3.6
VII 6 8.1
VI 6 9.5
V 6 10.5
High cardiovascular risk Low cardiovascular risk

Results of the interimistic analysis (n=28) – Estimated relevance of the model´s components

Conclusions
• Evidence-based guidelines should be adapted to be applicable for elderly patients with multi-morbidity.
• Consensus-based experts´ priority setting for elderly patients with multi-morbidity could be one way to achieve this.
• The tentative model contains three components: disease-specific risk, comorbidity and frailty
• The interimistic analysis indicates that the model´s components are considered relevant and that the inter-rater reliability of the experts´ rankings is good.