Connecticut SIM VBID Consortium Meeting: …...•Employer-led Consortium: peer-to-peer sharing of...
60
Connecticut SIM VBID Consortium Meeting: February 2, 2016 1 © 2016 Freedman Health Care, LLC
Transcript of Connecticut SIM VBID Consortium Meeting: …...•Employer-led Consortium: peer-to-peer sharing of...

Connecticut SIMVBID Consortium Meeting: February 2, 2016
1© 2016 Freedman Health Care, LLC

Connecticut SIM:Program Overview
December 7, 2015
2

Agenda
7. Value-based Insurance Design
6. Quality Measure Alignment
5. Value-based Payment Reform
4. What care delivery reforms are we promoting?
3. What problems are we trying to address?
2. What are the components of CT’s SIM?
1. What is the State Innovation Model Initiative?

What is a State Innovation Model Grant?
SIM grants are awarded by the federal government through the Center for Medicaid and Medicare Services (CMS) Innovation center. Grants are awarded to states that have demonstrated a commitment to developing and implementing multi-payer health care payment and service delivery models that will:
Connecticut awarded a $45 million test grant in December 2014 which will be implemented over the next five years.
1
2
3
Improve health system performance
Increase quality of care
Decrease Costs

Vision
Establish a whole-person-centered healthcare system that:
• improves population health
• eliminates health inequities
• ensures superior access, quality, and care experience
• empowers individuals to actively participate in their healthcare
• improves affordability by reducing healthcare costs

Our Journey from Current to Future: Components
6
Transform Healthcare Delivery System
$13m
Reform Payment & Insurance Design
$9m
Build Population Health Capabilities
$6m
Transform the healthcare delivery system to make it more coordinated,
integrate clinical and community services, and distribute services locally
in an accessible way.
Build population health capabilities that reorient the healthcare toward a
focus on the wellness of the whole person and of the community
Reform payment & insurance designto incent value over volume, engage consumers, and drive investment in
community wellness.
Invest in enabling health IT infrastructure
Engage Connecticut’s consumers throughout
Evaluate the results, learn, and adjust
CT SIM Component Areas of Activity
$376k
$10.7m
$2.7m

Healthcare today – 1.0
7
Connecticut’s Current Health System: “As Is”
Limited accountability
Unsustainable growth in costs
Pays for quantity without regard to quality
Limited data infrastructure
Uneven quality and health inequities
Poorly coordinated
Fee For Service Healthcare
1.0

Escalating costs mean…
….patients will experience ….communities will experience
Money for programs that support housing, education, the environment, and community development
Insurance premiums resulting in less take-home pay
Deductibles and co-pays for needed medical care
Access to social services and Medicaid

Escalating costs mean…
….the business community will experience
Competitiveness
Economic development

How about Connecticut?
Better Care
Affordability

Connecticut Healthcare Costs
Connecticut - healthcare spending = More than $30 billion, fourth highest of all states for healthcare spending per capita
CMS (2011) Health Spending by State of Residence, 1991-2009. http://www.cms.gov/mmrr/Downloads/MMRR2011_001_04_A03-.pdf

Connecticut: Uneven Quality of Care
Better Care
Better Health
Rising rate of Emergency Department utilization
D.C. Radley, D. McCarthy, J.A. Lippa, S.L. Hayes, and C. Schoen, Results from a Scorecard on State Health System Performance, 2014, The Commonwealth Fund, April 2014.
CT ranking out of 50 states
High Hospital Readmissions CT ranks 36th out of 50 states

Age-adjusted Death Rate for Diabetes, Connecticut Residents, by Race and Ethnicity, 2008-2012
8.8
13.4
20.8
31.9
14.8
0 9 18 27 36
Asian
White
Hispanic or Latino
Black or African American
All Connecticut Residents
Age-adjusted Deaths per 100,000 Population
Data Source: CT DPH, Vital Records Mortality Files, 2008-2012 data.
Health disparities persist in Connecticut

Health disparities persist in Connecticut
Better Care
Better Health
Affordability
Health disparities devastate individuals, families and communities, and are costly:
The cost of the disparity for the Black population in Connecticut is between $550 million - $650 million a year
Source: LaVeist, Gaskin & Richard (2009). The Economic Burden of Health Inequalities in the US.The Joint Center for Political & Economic Studies. As reported by DPH

Stages of Transformation

Stages of Transformation
Connecticut’s Current Health System: “As Is”
Accountable Care 2.0
Accountable for patientpopulation
Rewards• better healthcare outcomes• preventive care processes• lower cost of healthcare
Coordination of care acrossthe medical neighborhood
Competition on healthcare outcomes, experience & cost
Community integration to address social & environmental factors that affect outcomes
Accountable for allcommunity members
Rewards• prevention outcomes• lower cost of healthcare &
the cost of poor health
Shared governance including ACOs, employers, non-profits, schools, health departments and municipalities
Cooperation to reduce risk and improve health
Community initiatives to address social-demographic factors that affect health
Our Vision for the Future: “To Be”
Health EnhancementCommunities 3.0
Fee for Service 1.0
Limited accountability
Unsustainable growth incosts
Lack of transparency
Pays for quantity withoutregard to quality
Unnecessary or avoidable care
Health inequities
Limited data infrastructure

Targeted Initiatives
Statewide Initiatives
17

Model Test Hypothesis for SIM Targeted Initiatives
High percentage of patients in value-based payment arrangements
+Resources to develop advanced primary care and organization-wide capabilities
=Accelerate improvement on population health goals of better quality and affordability
MQISSPMedicare SSP
Commercial SSP
• Advanced Medical Home Program
&• Community & Clinical
Integration Program (CCIP)
+
MQISSP is the Medicaid Quality Improvement and Shared Savings Program
18

Primary care partnerships for accountability
19
Advanced Network
Primary care practice
Advanced Network = independent practice associations, large medical groups, clinically integrated networks, and integrated delivery system organizations that have entered into shared savings plan (SSP) arrangements with at least one payer

Accountability for quality and total cost
20
Advanced Network

Connecticut has many Advanced Networks
AN
AN
AN
AN
AN
AN
AN
AN
AN
AN
AN
AN
ANAN
AN
AN = Advanced Network chosen in Wave 1 to participate in
Medicaid Quality Improvement & Shared Savings Program (MQISSP)
AN
AN
AN
AN
AN
21

Resources aligned to support transformation
Advanced Network
Community & Clinical Integration Program (CCIP)
Awards & technical assistance to support Advanced Networks in enhancing their capabilities across the network
Advanced Medical Home (AMH) ProgramSupport for individual primary care practices to achieve Patient Centered Medical Home NCQA 2014 recognition and additional requirements
Advanced Network
Improving care for all populationsUsing population health strategies
22

Improving capabilities of Advanced Networks
Advanced Network
Comprehensive Medication Management
E-Consults
Oral health
Integrating Behavioral Health
Network wide screening, assessment, treatment/referral, coordination,
& follow-up
Supporting Individuals with Complex Needs
Comprehensive care team, Community Health Worker , Community linkages
Reducing Health Equity GapsCHW & culturally tuned materials
Analyze gaps & implement custom intervention
Co
mm
un
ity He
alth C
ollab
orative
s
Community & Clinical Integration Program Awards & technical assistance to support Advanced Networks in enhancing their capabilities in the following areas:
23

Whole-Person Centered
Patient Centered Access
Team Based Care
Population Health Management
Care Coordination/Transitions
Performance Measurement
Quality Improvement
Advanced Medical Home Program Webinars, peer learning & on-site support for individual primary care practices to achieve Patient Centered Medical Home NCQA 2014 and more
Advanced Network
Improving capabilities of practices in Advanced Networks
24

Value Based Payment
ValueQuality & Care Experience
Total Cost of Care

Expanding the reach of Value-Based Payment
26
Advanced Network
Medicare SSP
Commercial SSP
MQISSP

Reaching the tipping point
27
Commercial SSP
MQISSP
Medicare SSP
Commercial SSP
% of consumers in an Advanced Network in value-based payment arrangement
Medicare SSP
MQISSP

Reaching the tipping point
28
MQISSP
Medicare SSP
Commercial SSP
Culture of Volume
Culture of Value
% of consumers in an Advanced Network in value-based payment arrangement

Putting it all together
29
Advanced Network
Community & Clinical Integration Program
(CCIP)
Advanced Medical Home (AMH) Program
Commercial SSP
MQISSP
Medicare SSP

Targeted Initiatives
Statewide Initiatives
30

Statewide Initiatives
AN
AN
AN
AN
AN
AN
AN
AN
AN
AN
AN
AN
ANAN
AN
ANQuality Measure Alignment
Value-Based Insurance Design
AN
AN
AN
AN
AN
AN AN
AN
AN
AN
AN
AN
ANAN
AN
ANAN
31

Quality Measure Alignment
32

Quality Measure Alignment
Goals outlined in the test grant:
1. Core quality measurement set for primary care, select specialists, and
hospitals
2. Common cross-payer measure of care experience tied to value based
payment
3. Common provider scorecard

Common Quality Measure Set and Scorecard
Quality Performance Scorecard30% 40% 50% 60% 70% 80% 90%
Care Experience
PCMH CAHPS
Care Coordination
All-cause Readmissions
Prevention
Breast Cancer Screening
Colorectal Cancer Screening
Health Equity Gap
Chronic & Acute Care
Diabetes A1C Poor Control
Health Equity Gap
Hypertension Control
Health Equity Gap

Outcomes Measures Quality Performance Scorecard
30% 40% 50% 60% 70% 80% 90%
Care Experience
PCMH CAHPS
Care Coordination
All-cause Readmissions
Prevention
Breast Cancer Screening
Colorectal Cancer Screening
Health Equity Gap
Chronic & Acute Care
Diabetes A1C Poor Control
Health Equity Gap
Hypertension Control
Health Equity Gap
Health Plan
Quality Performance Scorecard30% 40% 50% 60% 70% 80% 90%
Care Experience
PCMH CAHPS
Care Coordination
All-cause Readmissions
Prevention
Breast Cancer Screening
Colorectal Cancer Screening
Health Equity Gap
Chronic & Acute Care
Diabetes A1C Poor Control
Health Equity Gap
Hypertension Control
Health Equity GapHealth Plan
EHR DataProcess & Outcome Measures
(E.g., diabetes A1C control, blood pressure control, depression remission)
Claims Data
Today:
National consensus to move towards outcomes:
Process MeasuresClaims Data
(E.g., Diabetes foot exam, well-care visits, medication adherence)

Value-based Insurance Design
36

New and innovative approaches
...the use of plan incentives to encourage employee adoption of one or more of the following:
Value-based Insurance Design
Use high value services (e.g., preventative services, certain prescription drugs)
Adopt healthy lifestyles (e.g. smoking cessation, physical activity)
Use high performance providersWho adhere to evidence-based treatment
Health promotion & disease management
Health coaching & treatment support
37

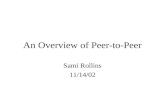
SIM VBID Components
• Employer-led Consortium: peer-to-peer sharing of best practices
• Prototype VBID Designs: using latest evidence, to make it easy for employers to implement
• Annual Learning Collaborative: including panel discussions with nationally recognized experts and technical assistance
CT’s Health Insurance Market Exchange) will implement VBID in Year 2 of the Model Test (subject to Board approval)

Aligning strategies to engage consumers and providers
Advanced Network
39Value-based Insurance Design Value-based Payment

Value-Based Insurance Design - Accountability Metrics
Year Percent adoption
2016 44%*
2017 53%
2018 65%
2019 74%
2020 87%
*Estimate – will establish empirical baseline 2015

Questions
41

THOMAS WOODRUFF, PHD, OFFICE OF THE STATE COMPTROLLER
VBID Landscape in Connecticut
42

V-BID Principles
Clinical Nuance:
1) Medical services differ in the amount of health produced
2) Clinical benefit derived from specific service depends on the consumer using it
With a Value-Based Insurance Design, consumer cost-sharing level is based on clinical benefit – not acquisition price – of the service
• Reduces or eliminates financial barriers to high-value clinical services and providers
43

V-BID Principles
An effective V-BID plan uses carrots and sticks
• Reduce barriers to high value services
• Preventive care screenings
• Chronic condition treatment
• Reduce prescription drug co-pays
• Members maintain medical choice
• Personal autonomy key union value
44

Connecticut’s Health Enhancement Program (HEP)
• Joint Labor/Management Healthcare Cost Containment Committee
• Between 2007-2011 HCCCC discussed Value Based Purchasing and Value Based Insurance Design
• In 2010 the state required ASOs to enter Patient Centered Medical Home arrangements to improve healthcare delivery and lower costs
• Labor members of HCCCC explored VBID to increase member engagement and lower costs
• In 2011, Malloy administration took office with a $3.8B deficit–Administration proposed savings through traditional cost shifting
– Labor coalition countered with VBID proposal to make employees healthier
– Labor proposal turned win/loss fight to win/win
45

HEP
Targets preventive care and chronic disease through:
• Voluntary enrollment for employees
• Required age appropriate preventive screenings and care
• Lower co-pays for medications/care associated with five chronic diseases and conditions
• Chronic disease management education program
Lowers costs for participating/compliant employees by:
• Waiving co-pays for preventive care and chronic disease management
• Reducing monthly premium share ($100 per month)
46

JOHN FREEDMAN, MD, FREEDMAN HEALTHCARE
ALYSSA URSILLO, MPH, FREEDMAN HEALTHCARE
About the Project
47

Goal
This initiative aims to increase uptake of V-BID in Connecticut
by developing a V-BID prototype of recommended practices and plans,
with strategies and tools to select and promote V-BID plans
48

Deliverables
1. Assess and index V-BID models both in Connecticut and nationally
2. Make recommendations for the best models for Connecticut markets
3. Develop templates and employer guidance for recommended content of a V-BID benefit plan that is applicable to self and fully-insured employers, and public and private exchanges
4. A web-based V-BID Toolkit for employers
5. Targeted communications materials for employers and consumers
6. Disseminate best practices through V-BID Learning Collaborative
49

Role of Consortium
The Consortium will serve as an advisory body for the V-BID Initiative: Advise on strategies for health plan/employer engagementMake recommendations for employer adoption of V-BIDAdvise on structure and goals of Learning CollaborativeRecommend members/networks for Learning CollaborativeInform development of
• V-BID plan template(s)• V-BID Toolkit• Communications materials• Employer guidance for V-BID adoption
50

Timeline
Meetings and Deliverables Date
First Consortium Meeting February 2, 2016
• Introduce VBID framework and HEP, feedback on VBID concepts as part of plans
Second Consortium Meeting March 22, 2016
• Recommendations and feedback on assessments of VBID plans for CT markets, employer barriers to uptake
Third Consortium Meeting April 27, 2016
• Recommendations and feedback on VBID templates, Toolkit, communications materials
Finalize VBID templates, employer guidance and Toolkit May 23, 2016
First Learning Collaborative Meeting Mid June
51

JOHN FREEDMAN, MD, FREEDMAN HEALTHCARE
MARK FENDRICK, MD, VBID HEALTH
THOMAS WOODRUFF, PHD, OFFICE OF THE STATE COMPTROLLER
What Does a Model V-BID Plan Look Like?
52

Building a Framework for V-BID Assessment
Purpose of assessment framework: • To guide recommendations of value based insurance design concepts to
be adopted by employers, health plans and exchanges as part of VBID plan templates for various Connecticut market segments
Concepts Adapted from CMS Medicare Advantage Model• 5 year demonstration program for state grantees
• Testing utility of structuring consumer cost-sharing and other health plan design elements to encourage patients to use high value services and providers
53

V-BID Concepts
V-BID Concept Reduced cost sharing for high value services and drugs
Purpose Encourage healthy patient choices; Encourage use of high value, evidence-based services and treatments
Leverage point Patient-based: clinically nuanced
Examples Waive copay for biennial colonoscopy in ulcerative colitis (nuanced)
54
V-BID Concept Increased cost sharing for low value services and drugs
Purpose Discourage unhealthy patient choices; Discourage use of low value services and treatments
Leverage point Patient-based: clinically nuanced
Examples Increase co-pay on inappropriate imaging for acute low back pain

V-BID Concepts
VBID Concept Reduced cost sharing for high value providersPurpose Encourage healthy patient choices. Encourage prudent provider practice.
Leverage point Patient-based: clinically nuancedProvider-based: specialty, affiliation, or past behavior
Examples Lower copay if MD affiliated with high-performing ACO (tiering).
55

V-BID Concepts
VBID Concept Reduced cost sharing for disease management programsPurpose Encourage healthy patient choices for targeted groups
Leverage point Patient-based: clinically nuanced. Based on participation
Examples Waive co-pay for recommended medications for patients with asthma who participate in medication adherence program
56

V-BID Concepts
VBID Concept Coverage of supplemental, high value benefitsPurpose Encourage healthy patient choices for targeted groups
Leverage point Patient-based: clinically nuanced
Examples Coverage of transportation to primary care appointments for patients with multiple chronic diseases.
57

Building a Framework for V-BID Assessment
How are VBID concepts implemented in health plan design? Consider:
1. Are VBID concepts present?
2. What percent of members do they apply to?
3. What percent of spending do they apply to?
4. What percent of conditions do they apply to?
5. How strong are the incentives (e.g., how big is cost differential)?
6. How closely targeted (how close to Evidence Based Medicine)?
7. How easy is it to implement?
8. Are the outcomes/impact measurable?
9. Are the outcomes/impact significant?
58

Discussion: Challenges and opportunities of adopting V-BID in Connecticut
59

60
Next Steps:
V-BID plans in Connecticut survey and assessment
SWOT analysis of employer uptake of V-BID
Executive Team Meeting: TBD
Second Consortium Meeting: March 22, 2016