Congestive Heart Failure (CHF)
83
-
Upload
mara-leach -
Category
Documents
-
view
45 -
download
2
description
Congestive Heart Failure (CHF). Presented To:. Presented By:. Overview of CHF Review cardiac physiology and pathophysiology Etiology Classification of CHF Stages of CHF Early recognition of CHF Diagnosis of CHF Early and aggressive management of CHF. Heart Failure. - PowerPoint PPT Presentation
Transcript of Congestive Heart Failure (CHF)


Congestive Heart Failure
(CHF)

Presented To:
Sir M. Khalid Tipu
Dr. Amir Riaz
Presented By:
Ayesha Faiqa Sunaila Saba Saliha Andleeb Mehreen


Overview of CHF Review cardiac physiology and
pathophysiologyEtiology Classification of CHFStages of CHF Early recognition of CHFDiagnosis of CHFEarly and aggressive management of CHF

Heart Failure
The term “ cardiac failure” or “heart failure” means simply failure of heart to pump enough blood to satisfy the needs of body.

CONGESTIVE HEART FAILURE
Definition:“Congestive heart failure (CHF) occurs when the heart can't meet the metabolic demands of the body (failure of the heart to supply the tissue with their needs of blood”.

Heart Physiology

Physiology
Systole:The contraction of the cardiac muscle tissue in the ventricles is called systole. When the ventricles contract, they force the blood from their chambers into the arteries leaving the heart. The left ventricle empties into the aorta and the right ventricle into the pulmonary artery. The increased pressure due to the contraction of the ventricles is called systolic pressure.

Physiology Cont…
Diastole:The relaxation of the cardiac muscle tissue in the ventricles is called diastole. When the ventricles relax, they make room to accept the blood from the atria. The decreased pressure due to the relaxation of the ventricles is called diastolic pressure.

Physiology Cont…
Electrical Conduction System:The heart is composed primarily of muscle
tissue. A network of nerve fibers coordinates the contraction and relaxation of the cardiac muscle tissue to obtain an efficient, wave-like pumping action of the heart.

1. Sinoatrial node (SA node)
2. Atrioventricular node (AV node
3. Common AV Bundle
4. Right & Left Bundle Branches
Conduction System

PATHOPHYSIOLOGY
Abnormal changes occur to right ventricle, left ventricle or both.
Cardiac output in heart failure is below the normal range.
The myocardium becomes very weak because of low blood and oxygen supply and myocardium contractility is reduced.
The ejection fraction falls from its normal values of about 0.6to 0.2.

PATHOPHYSIOLOGY
The falling myocardium decreases myosin ATPase.
Abnormal Actin and Tropomyosinis formed. Relaxation is slowed, possibly because of
slowed uptake of ca+2 by sarcoplasmic reticulum.
Venous return is reduced because of lack of proper cardiac pump and edemais caused.

PATHOPHYSIOLOGY
Compensatory mechanism causes the increased secretion of aldosteron and arginine vasopressin and makes this CHF situation mor aggressive

Etiology
Ischemic heart diseases Systemic Hypertension Cardiomyopathy Coronary artery disease
MAIN CAUSES

ETIOLOGY
congenital heart disease Valvular heart disease Hyperthyroidism Anemia Alcohol Miscellaneous
OTHER CAUSES

People Live with Atherosclerosis – But Die of Thrombosis!
The formation, progression
and rupture of an
atherosclerotic plaque

Hypertension Hypertrophic Cardiomyopathy

CATEGORIES FOR CLASSIFICATION
Anatomically
Physiologically
Functionally

CLASSIFICATION OF CHF
There are many different ways to categorize CHF:Left heart failure Vs Right heart failureDiastolic dysfunction Vs Systolic dysfunctionBackward Vs Forward failureLow output heart failure Vs High output heart failure

New York Heart Association Functional
classification Class 1: Asymptomatic Class 2: Symptomatic with mild activity Class 3: Symptomatic with moderate activity Class 4: symptomatic at rest

STAGES OF CHF STAGE A:Includes pts at risk for developing heart failure
STAGE B:Includes pts with structural heart disease but no recognized symptom of heart failure
STAGE D:Includes relatively small group of pts that have become refractory to usual therapies
STAGE Structural heart disease with current or prior symptoms of heat failure.

Diagnosis
1) Clinical findings (Signs and symptoms)
2) Laboratory findings

`Age Heart rate/min
Birth 6m1y
2-4ys5-10ys
10-15ys
140110100959080

Symptoms Tachycardia Shortness of breath Exertional dyspnea at first,orthopnea, proximal
nocturnal dyspnea and rest dyspnea. Non-productive cough Nocturia fatigue & exercise intolerance

Symptoms Edema Hepatic congestion occasionally loss of appetite and nausea impaired GI perfusion or ascites Pulmonary edema

Acute Pulmonary Edema is a true Life
Threatening Emergency for which the clinical picture is
hard to forget!

SYMPTOMS

SIGNS Vital signs may be normal but: Tacchycardia, hypotension & reduced pulse
pressure increased sympathetic nervous system activity: cold extremities &diaphoresis Physical exam shows following signs:

Physical Exam Anxious Pale Clammy Dyspnea Tachypnea Confusion Edema
Tachycardia Pink Frothy Sputum Cyanosis Diaphoretic Hypertension

Diagnosis(II-Laboratory findings)
CBC
Serum electrolyte
BNP
ECG
MUGA scan
Chest X-ray
Angiography

Lab Analysis cont…
BLOOD COUNT:
Low blood cell count may cause symptoms like CHF or contribute to the condition.

Lab Analysis cont…
. B-TYPE NATRIURETIC PEPTIDE(BNP):
This is a hormone produced at higher levels by the failing heart muscle. This is a good screening test; the levels of this hormone generally increase as the severity of heart failure worsens.
SERUM ELECTROLYTE: Sodium, potassium, and other electrolyte levels, especially if the person
has been treated with diuretics and/or has kidney disease

Lab Analysis cont…
MUGA -SCAN TEST: A small amount of a mildly radioactive dye is injected into a vein
and travels to the heart.
STRESS TEST: A treadmill or medication (nonwalking) stress test is used to help
evaluate the cause or causes of heart failure, in particular, regarding coronary artery disease. This test is frequently combined with nuclear imaging or echocardiography to improve accuracy.

Echocardiogram
An echocardiogram is a noninvasive test that uses reflected sound waves off the heart to determine its size,
structure, and function.
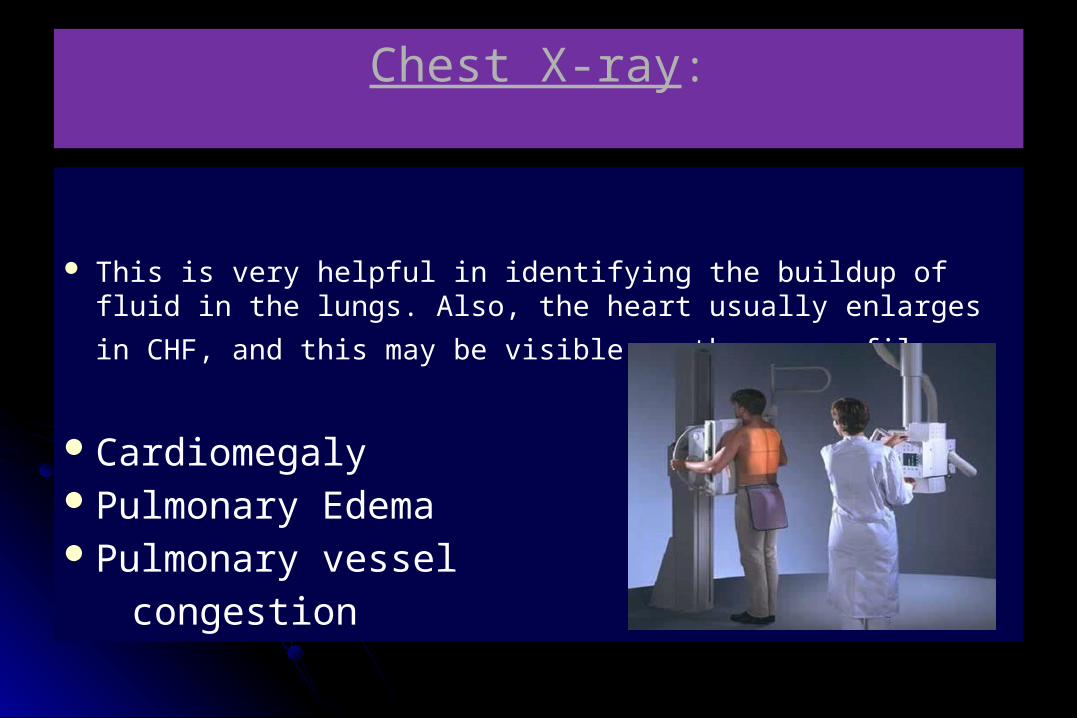
Chest X-ray:
This is very helpful in identifying the buildup of fluid in the lungs. Also, the heart usually enlarges in CHF, and this may be visible on the x-ray
film.
Cardiomegaly Pulmonary Edema Pulmonary vessel
congestion
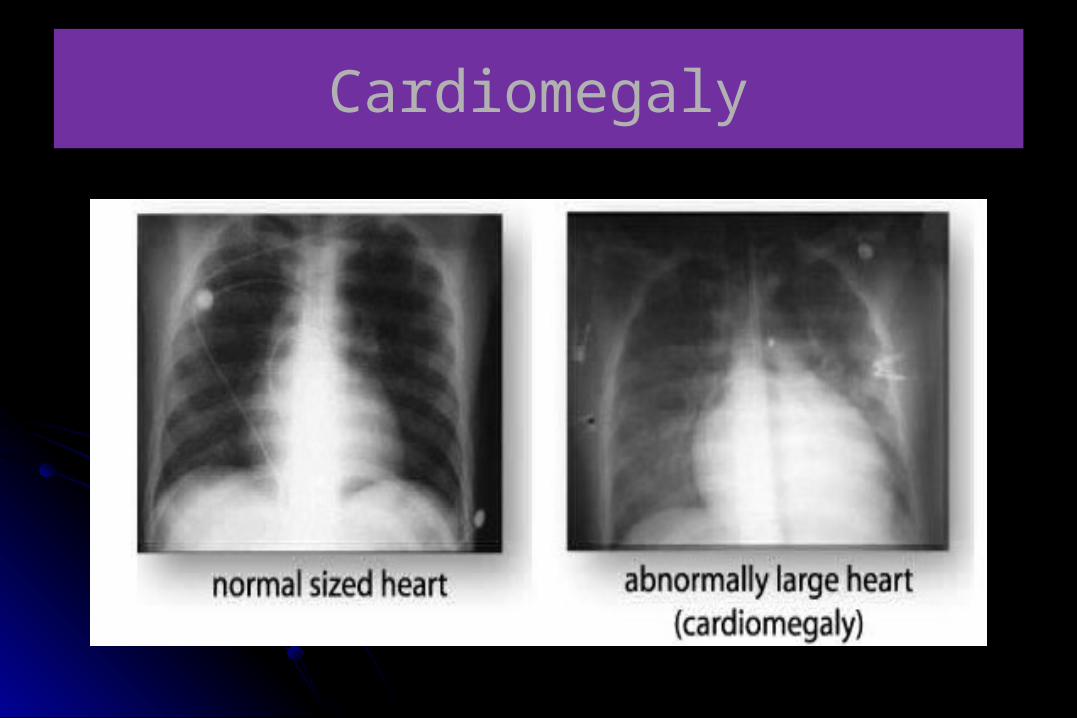
Cardiomegaly

Pulmonary Edema

Pulmonary vessel congestion

Electrocardiogram
This painless test measures the electrical activity (rhythm) of the heart.
• Rhythm disorders…

Angiography
coronary catheterization may be used to identify possibilities for revascularisation through percutaneous coronary intervention or bypass surgery.

Precipitating CausesNon Compliance with Meds and DietAcute MIArrhythmiaPneumonia Increased Sodium Diet (Holiday Failure)AnxietyPregnancy
Emergency Dept. Management
Sit uprightHigh flow O2
Ventilatory supportDiuretics MorphineDopamineDobutrexAntihypertensivesDigitalis

The Management of CHF
I) General measures
Improving oxygen delivery: Administration of oxygen (40-50% ) with humidity.
Sedation :morphine sulfate

The Management of CHF
Salt restriction: low salt consumption in diets,
less than 3g/day and avoidance of salty snacks.Healthy life styleTreatment of the cause as hypertension

The Management of CHF
Elimination and correction of predisposing factors as anemia, infection.
Nutrition :CHF increases the metabolic demands while making food intake itself more difficult.
Enhanced Caloric Content DIET , nasogastric or gastrostomy feedings.

PHARMACOLOGICAL TREATMENT
GROUPS OF DRUGS
DIURETIC THERAPY
INHIBITORS OF RENINANGIOTENSIN ALDO SYSTEM
B-BLOCKERS
DIGITALIS GLYCOSIDE
VASODILATORS
COMBINATION OF MEDICAL THERAPIES
STATIN THERAPY
ANTICOAGULATION
ANTIARRHYTHMIC THERAPY
CALCIUM CHANNEL BLOCKER

The Management of CHF
II) Drug therapyA- Diuretics: Diuretics are the most effective means
of providing the symptomatic relief to pts with moderate to severe CHF.“A COMBINATION OF DIURETIC AND ACE INHIBITOR SHOULD BE THE INITIAL TREATMENT IN MOST SYMPTOMATIC PATIENTS”

A- Diuretics
I) Thiazide diuretic as Hydrochlorothiazide (25-100mg) Metolazone (2.5-5mg) Chlorthalidone (25-50mg)Onset: 1-2 hoursDuration of action: 12-24 hour.
Metolazne has relatively higher efficacy.

A- Diuretics
II) Loop diuretic: patient with more severe heart failure should be treated with one of the loop diuretic.
these include: Furosemide (Lasix 20-320mg/day), Bumetanide (1-8mg/day), Torsemide (2-200mg/day)
Onset: rapid, Duration of action: short

A- Diuretics
Side effects: hypokalemia Intravascular volume depletion Hypotension Skin rashes hyperurecemia

A- Diuretics
III) Potassium sparing Agents Include:
Spirnolactone: (Aldacpone 25-50mg po qd)
Triamterene
Amiloride
These are useful in combination with loop diuretic and thiazides.
Side effects:
Hyperkalemia, GI symptoms, kidney dysfunction

B- ACE Inhibitors
Captopril: Capoten (Bristol- Myers Squibb)
Dose: 50-100mg 3 times daily.
Half life: 8 hours
Lisinopril: Zestril
Dose: 20-35 once daily.
Half life: 12 hours
Side effect: Dizziness, Cough

Angeotensin-II Receptor Blocker
Losartan potassium:
Eziday (Werrick)
Hyzaar (Merck & Dohme)
Sartan-H (Berret Hodgson)
Dose: 50mg/day, once daily or two divided doses.
Side effects: Hyponatremia, Angioedema, Dry cough, Anaphylactic reaction.

BETA BLOCKERS
Beta blockers: We know that increased Sympathetic activity
in HF --- Increase in circulating norepinephrine ---- stimulation of alpha and beta-receptors. This chronic elevation causes-Myocardial damageProgressive LV dysfunction and dilation

BETA BLOCKERS
Doses of Beta blockers:
Beta-blockers should be adjusted to maximum tolerated doses
Side effects: Cold extremities,dry mouth, dizziness, Muscular fatigue.
Contraindications:Hypersensitivity, Bradycardia.
Brand Starting dose Target dose
Blokium (Atenolol) 50mg once daily 100mg once daily
Lo-Pressor 12.5mg/day 50-100mg bid.
Bisoprolol 1.25mg/day 10mg/day

Digitalis Therapy Digoxin should given for the pts who remain
symptomatic even when taking diuretics and ACE inhibitors.
Digoxin:Lanoxin(gsk)
Adults and children over 10yrs
Dose(tab):rapid oral loading:0.75- 1.5mg as a single dose.
slow oral loading:0.25-0.75mg daily for 1week.
maintenance:0.125- 0.75mg daily

Digitalis Therapy Emergency parenteral loading: 0.5-1mg
(depending on age, lean body weight and renal function).
Half life: 24-36 hours
Side effects: ventricular arrhythmia, conduction disturbances, Anorexia.
Contraindication: Arrhythmias caused by cardiac glycoside intoxication.

Vasodilators
Classes of Vasodilatores
1. Nitrates
2. Nesiritide
3.Hydralazine

Nitrates SODIUM NITROPRUSSIDE (IV infusion,
powder for reconstitution sodium nitroprusside 10 mg/mL)
Dose
By intravenous infusion, initially 10–15 micrograms/minute, increased every 5–10 minutes as necessary; usual range 10–200 mic.g/minute normally for max. 3 days
Hypotension
Nausea
Perspiration
Retching Headache
Dizziness
Side-effects

Nesiritide
Nesiritide (Natrecor): Administered intravenously, usually by bolus, followed by IV infusion
Dose:For most adults and the elderly, a normal dosage is 2 micrograms/kg followed by a continuous IV infusion of 0.01 mcg/kg/minute. This may be increased every three hours for a maximum of 0.03 mcg/kg/mi
Side Effects
Low blood pressure
Headache
Nausea
Slow heart rate

Hydralazine
HYDRALAZINE HYDROCHLORIDE: (Tablets 25mg)
Dose:
25 mg 3–4 times daily, increased every 2 days if necessary; usual maintenance dose 50–75 mg 4 times daily
Side effects
Fluid retention
Headache
Dizziness
HypotensionFlushing
Palpitation
Tachycardia

Contra-indications
Idiopathic systemic lupus erythematosus
Severe Tachycardia
High output heart failure
Myocardial insufficiency due to mechanical obstruction
Acute porphyria

Combination Therapy
To obtain optimal management, combination therapy is used.
In addition to ACE inhibitors and B- blockers, certain specific therapies are used if patients remain symptomatic:
ARBs (best in class II-III heart failure)Spironolactone (current or recent class IV heart
failure).Hydralazine & Isosorbide dinitrate(Americans).

Other Groups..
Other groups occasionally used considering safety factors along with other conditions are:
Positive Ionotropic agents
Calcium channel blockers
Anticoagulation therapy
Antiarrhythemic therapy
Statins

Common drug-drug Interactions
DRUGINTERACTS
WITH RESULT OF INTERACTION
Diuretic NSAIDs Decreased effect of Diuretics
ACE inhibitors or ARB
Diuretics Enhanced hypotensive effect. Increased risk of hyperkalemia with potassium sparing drugs
Digoxin Diureticverapamil
Increased risk of hypokalemia and therefor toxicity.Increased risk of AV block
Nitrates Heparin Increased excretion of heparin
Spironolactone Digoxin Interferes with the measurement of Digoxin plasma level, resulting in inaccurate interpretation
B- blockers VerapamilDiltiazem
Increased risk of hypotension, heart failure and asystoleIncreased risk or AV block and bradycardia

Chronic CHF TreatmentAdjunctive Treatment:
Lifestyle changes
Weight loss
Decrease dietary salt
Increase O2

Goals of Treatment
Relieve Symptoms
Treat cause
Delay progression
Reduce hospitalization
Reduce mortality

Non pharmacological Treatment
Implantable cardioverter defibrillators. Biventricular pacing (Resynchrnization) Case management, diet, and exercise training Coronary revascularization Cardiac transplantation Other surgical treatment options Palliative care

CPAP
CPAP is a non-invasive procedure that is easily applied and can be easily discontinued without untoward patient discomfort.
CPAP is an established therapeutic modality, recently introduced into the prehospital setting.
In the primary phase CPAP application in cardiogenic pulmonary edema, thus far, appears to be beneficial to patient outcome.

Key Points of CPAP
CPAP has been successfully demonstrated as an effective adjunct in the management of pulmonary edema secondary to congestive heart failure.
CPAP may prove to be a viable alternative in many patients previously requiring endotracheal intubation by prehospital personnel.

CPAP Mechanism
Increases pressure within airway.
Airways at risk for collapse from excess fluid are stented open.
Gas exchange is maintained Increased work of breathing
is minimized

Prehospital Indications
Congestive Heart FailurePulmonary Edema associated with volume
overload ( renal insufficiency, iatrogenic volume overload, liver disease , etc)
Near Drowning

Contraindications
Respiratory Arrest Agonal Respirations Unconscious Shock associated with cardiac insufficiency Pneumothorax Facial Anomalies e.g. burns, fractures, etc. Facial trauma

Hazards
Gastric DistentionCorneal DryingHypotensionPneumothorax

Important Points
Pulmonary edema patients, properly selected, quickly improve with CPAP in a matter of minutes.
CPAP is to CHF like D50 is to insulin shock.
Visual inspection of chestwall movement reveals improved respiratory excursion.

Important Points (Continued)
COPD and Asthmatic patients do not respond predictably to CPAP. They have a higher risk of
complications such as pneumothorax, and thus should not be treated in the field with CPAP

Data Comparison1996 – 1997 1997 – 1998
Intubated 22 8
CPAP 0 50
Hospital Stay 14.8 8
ICU Admission 100% 48%

CPAP vs. Intubation
CPAP INTUBATION
• Non-invasive• Easily discontinued• Easily adjusted• Use by EMT-B• Doesn’t require
sedation• Comfortable
• Invasive• Usually gets difficult• Potential to infection• Requires highly
trained personnel• It Can require
sedation• Traumatic

Summary
CPAP provides an adjunct between oxygen by NRB and endotracheal intubation.
Reduces length of hospital admission.Reduces trauma of intubationReduces costs

References Guyton. (2003). Medical Physiology. (10th ed. Vol.1). H.I.E. Sanunders.
McPhee, S. J. (2010). Current Medical Diagnosis & Treatment (49th ed.). USA: McGraw Hill Companies, Inc.
Roger Walker.(2007). Clinical Pharmacy & Therapeutics. (4th ed.).
BNF.org. BNF 58. (2009)
BNF.org. BNF. 56. (2008)
Wallsun. (20008). Review of Medical physiology.
Richard, A. (2000). Pharmacology. (2nd ed.). Philadelphia.
Kulick, D. (2008). Congestive Heart Failure. Retrieved June 05, 2010 from
http://www.medicinenet.com/congestive_heart_failure/article.htm.