Congenital ichthyosis
75
CONGENITAL ICHTHYOSIS Dr Yugandar
-
Upload
dr-yugandar -
Category
Health & Medicine
-
view
74 -
download
1
Transcript of Congenital ichthyosis

CONGENITAL ICHTHYOSIS
Dr Yugandar

The word ichthyosis comes from the Greek word for a
fish.
ichthyosis : is a group of disorders that are characterized
by a persistent, non-inflammatory scaling disorder of the
skin surface.
It is caused by abnormality in keratinization and
exfoliation of the horny cell layer.

The ichthyoses are a clinically and genetically
heterogeneous group of skin disorders,
characterized by a diffuse, generally uniform and persistent
pattern of scaling without mucosal or extracutaneous
(except in ichthyosiform syndromes) involvement.




Cutaneous features can be isolated (non syndromic ichthyosis),
or associated with extra-cutaneous (syndromic ichthyosis)
Types of Non syndromic ichthyosis
Congenital ichthyosis
Ichthyosis vulgaris
X-linked ichthyosis
Bullous congenital ichthyosiform erythroderma (BCIE)
Nonbullous congenital ichthyosiform erythroderma (NBCIE)
Lamellar ichthyosis
Acquired ichthyosis
Acquired ichthyosis
Types of syndromic ichthyosis
Sjögren-Larsson syndrome
Netherton syndrome
KID syndrome
Refsum syndrome
Rud syndrome

Congenital ichthyosis
Ichthyosis vulgaris
X-linked ichthyosis
Bullous congenital ichthyosiform erythroderma (BCIE)
Nonbullous congenital ichthyosiform erythroderma (NBCIE)
Lamellar ichthyosis

Ichthyosis vulgaris It is the common inherited disorder. inheritance is autosomal dominant
Etiology : caused by mutation in the gene coding
for filaggrin, a key protein involved in skin barrier function.
Decreased convesrion of Profilaggrin to Filaggrin.

Pathogenesis :
decrease in the production of filaggrin,defective aggregation of
Keratin intermediate filaments,
abnormal exfoliation and dryness and scaling
Keratohyalin synthesis is affected because of the filaggrin
mutation.
Filaggrin is an epidermal protein that normally functions as a
barrier molecule against environmental allergens, water loss,
and infection
Pathology :
There is thickening of the horny cell layer
reduction or loss of granular cell layer.

Histopathology:
Mild hyperkeratosis
diminished or absent granular layer in the epidermis.
The dermis is normal.
Electron microscopy reveals scanty and fragmented
keratohyaline granules in granular layer cells

Diminished or absent granular layer
Absent of filaggrin with immunostaining

Age of Onset :
early 3 – 12 months of age
Clinical features :
This is the mildest form of ichthyosis.
main symptoms are dryness and scaling of the skin (fine
scale).
Present, mostly on the extensor surfaces of extremities and
trunk.
back > abdomen ,extensor surface > flexor surface

Scaling is most prominent over the trunk, abdomen, buttocks
and legs.
The flexural areas, such as the antecubital fossa, are spared.

The symptoms subside during the summer and aggravate
during the winter
scaling may be present on the eyelid skin,punctate
epithelial keratitis and recurrent corneal erosion
Linkage analysis has identified an ichthyosis
vulgaris locus on band 1q22

An association may be present between ichthyosis vulgaris
and atopic diseases
Mutations in the coding of the filaggrin gene have been
identified in both ichthyosis vulgaris and atopic dermatitis.
Treatment : symptomatic treatement



X-Linked Recessive Icthyosis
Its uncommon type
Etiology : It is caused by loss or marked reduction of steroid
sulfatase enzyme
delayed exfoliation of the horny cell layer.
inheritance : X-linked recessively inherited,male children
Its k/a Ichthyosis nigra due to dark brown scales


Pathogenesis :
the lack of steroid sulfatase causes accumulation of
cholesterol sulfate, leading to delayed exfoliation of horny
cells and hyperkeratosis
Histopathology :
Thickening of the horny cell layer.
normal or mildly thickened granular and suprabasal cell
layers.

Compact hyperkeratosis
Accentuated granular layer
Clinical features:
ichthyosis manifests shortly after birth and does not improve
with age.
The symptoms are severer than ichthyosis vulgaris,
the scales are large and dark brown.
The scalp also scaly.
Eruptions also appear on the flexures of joints.
The whole body of newborns may be encased in a translucent
covering (collodion baby) .

Scales : Large & DARK BROWN more
Prominent over flexural areas

Complication :
Corneal opacification may occur.
White opacities in slit lamp &
blue arc
D.D:
ichthyosis vulgaris is differentiated from X-linked ichthyosis by the
decrease of steroid sulfatase in the case of the latter.


Treatment:
symptomatic and the same as those for ichthyosis vulgaris
The retinoids drugs may give good improvements, but the
side effects limit their use in infants and young children.


LAMELLAR ICTHYOSIS
Etiology :
Defect in Transglutaminase – 1 enzyme
its a calcium-dependent enzyme that is necessary for the
formation of cornified cell envelopes in keratinocytes
Age of onset : begins usually at birth
Inheritance : as an autosomal recessive trait (AR).
K/a ARCI

The transglutaminase 1 enzyme is involved in the
formation of the cornified cell envelope
The formation of the cornified cell envelope is an essential
for normal intercellular lipid layer formation in the stratum
corneum.
mutations cause defects in the intercellular lipid layers in
the stratum corneum, leading to defective barrier function
of the stratum corneum

6 genes for lamellar ichthyosis have been localized and 5 of them
TGM1 (14q11)
ABCA12 (2q34)
19p12-q12
19p13
ALOXE3-ALOX12B (17p13)
ichthyin (5q33)



The areas involved in mild cases are the antecubital,
popliteal and the neck
The palms and soles may present with mild
hyperkeratosis( PPK)
Ectropion





Hyperkeratosis ,Hypergrannulosis
Parakeratosis Prominent rete
ridgesMild perivascular infiltrate in the upper dermis and mitosis

Skin biopsies can aid in the diagnosis of lamellar ichthyosis
and detection of transglutaminase-1 expression.
At birth, electron microscopy can be used to differentiate a
severe collodion baby affected by lamellar ichthyosis from a
baby affected by harlequin ichthyosis by demonstrating the
absence of the marginal band

Bathing suit ichthyosis:
unique clinical form of autosomal recessive congenital
ichthyosis
characterized by marked scaling on the bathing suit
areas but sparing of the extremities and the central face.
caused by transglutaminase-1 deficiency
it is a temperature-sensitive phenotype



Shedding of membrane
Ichthyosiform
Erythroderms

Bullous congenital ichthyosiform erythroderma (BCIE)
it is rare disorder
autosomal dominantly inherited
sometimes born as collodion babies
Diffuse flushing and blistering recur for several weeks after
birth

Pathogenesis
intermediate filament of suprabasal cells composed of
keratin 1 and keratin 10.
Because of mutation in the keratin 1 or keratin 10 gene
abnormal keratin fiber formation & cytoskeleton distortion
epidermal blistering occur, leading to secondary thickening
of the horny cell layer
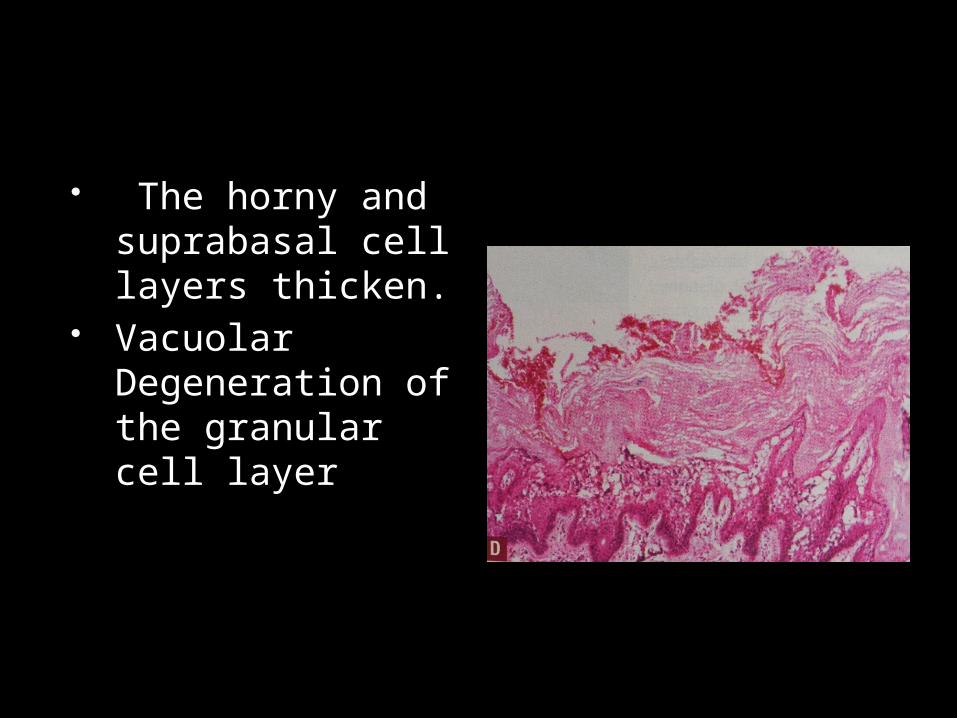
The horny and suprabasal cell layers thicken.
Vacuolar Degeneration of the granular cell layer

Clinical features
At birth child looks as Burned with widespread blisters &
erosions
May have verrucous,dirty,firm, hyperkeratotic (hystrix)
spines over erythematous background often in flexural
creases
blisters

may have erythroderma
palmar/plantar keratoderma
Frequent skin infections
characteristic pungent odor due to super infection
by mixed flora

D.D :
epidermolysis bullosa
incontinentia pigmenti
impetigo contagiosa
Treatment : oral retinoid and application of
moisturizer

Nonbullous congenital ichthyosiform
It is rare autosomal recessively inherited
Most of the patients are born as collodion babies.
The affected sites include the flexures of joints.
Defects in enzymes Trans glutaminase ,Two
Lipoxygenases

Pathogenesis
Six or more genes are thought to be associated with
occurrence of NBCIE.
the mechanism of NBCIE is known to be a
marked decrease in physical and functional
strength of keratin

Clinical features
Born as Collodion babes
Covered by fine white scales, 2-3 days after birth, the
collodion covering exfoliates,
leaving the whole body surface
with diffuse flushing and scaling

Scarring alopecia,short stature,
Cardiac anomolies
Erythroderma,
ectropion

NBCIE progresses until the age of 10,at which point it stops
and subsides.
Oral retinoid (a vitamin A derivative) is effective.
The skin should be kept clean to prevent secondary infection.

HARLEQUIN ICHTHYOSIS
very rare condition
autosomal recessively inherited
There is abnormality of the lamellar granules in harlequin
ichthyosis
Abnormalities of Profilaggrin & K 6,K16
Ichthyosis Congenita Gravis

In Italy,Comic servants characters from Italian commedia dell’arte
In french ,Black faced emissary of devil ,chasing damned souls of evil people to hell

Baby skin affected in Utero
patient is covered with an extremely thick stratum corneum
at birth causing thick, horny, armor-like plates that cover the
entire skin surface.
Cracks in the skin
ectropion of eyelids
eclabium,Ears absent

difficulty of opening the mouth are so severe that most patients die within 2 weeks after birth,still birth
Abnormal Lamellar Bodies
Under EM


Neonate after retinoid theraphy after 6 months

Ultrasound findings:
Head: cracked skin; open eyes, due to severe eversion of the
eyelids (ectropion); wide lips, (eclabium)
Skin: thickened with multiple fissures
Extremities: deformation, hypoplasia of fingers and toes
3D ultrasound helps to make the diagnosis.

thickened, Harlequin lips cracked skin on the fetal face

Transverse view of the fetal abdomen on
the image shows a thickened skin
with a crack indicated by arrow.
the foot with hypoplastic toes,

Differential diagnosis
Sjögren-Larsson syndrome
Netherton syndrome
Gaucher disease
Keratitis-ichthyosis-deafness syndrome
Trichothiodystrophy ("sulfur-deficient hair")
Chanarin-Dorfman syndrome
Conradi-Hünermann syndrome (X-linked dominant
chondrodysplasia punctata)
Hypohidrotic ectodermal dysplasia
Bullous autosomal dominant ichthyoses


Treatment



Prevention
In congenital ichthyosis syndromes, excessive intra-amniotic
debris and polyhydramnios on ultrasonography scanning in
utero may be the first indication of disease
Using USG in utero, fetal foot length may be an important &
first marker, seen in the second trimester, for the diagnosis of
harlequin ichthyosis
Other findings may include a persistently open mouth, dense
amniotic fluid, and fixed flexion of the extremities.

low maternal serum unconjugated estriol during pregnancy
screening may be a good indication of placental STS deficiency
and X-linked recessive ichthyosis
Microdeletion of STS gene can be confirmed by fluorescence in
situ hybridization (FISH) analysis of cultured amniotic fluid in X-
linked ichthyosis
Prenatal diagnosis of lamellar Ichthyosis can be made by direct
mutational analysis of the keratinocyte transglutaminase gene


Thank
You
For
Your
Att
enti
on