
Congenital Disease & Tumours of Kidney and Bladder Dr. Barbara Dunne.
60
Congenital Disease & Tumours of Kidney and Bladder Dr. Barbara Dunne
-
Upload
joshua-mcbride -
Category
Documents
-
view
224 -
download
5
Transcript of Congenital Disease & Tumours of Kidney and Bladder Dr. Barbara Dunne.

Congenital Disease & Tumours of Kidney and Bladder
Dr. Barbara Dunne

Congenital Anomalies of Kidney Agenesis Hypoplasia Ectopic Horseshoe kidney

Cystic Diseases of Kidney
Hereditary /Developmental Acquired Miscellaneous

Cystic Diseases of Kidney- Hereditary
Adult Polycystic Kidney Disease Autosomal Dominant- APKD1 on
chrom 16 Usually progress to chronic renal
failure Can get cysts in liver (40%) and in
circle of willis (up to 30%)


Cut section of adult polycystic kidney disease
Cysts of various sizes
Some containing fluid and blood clot
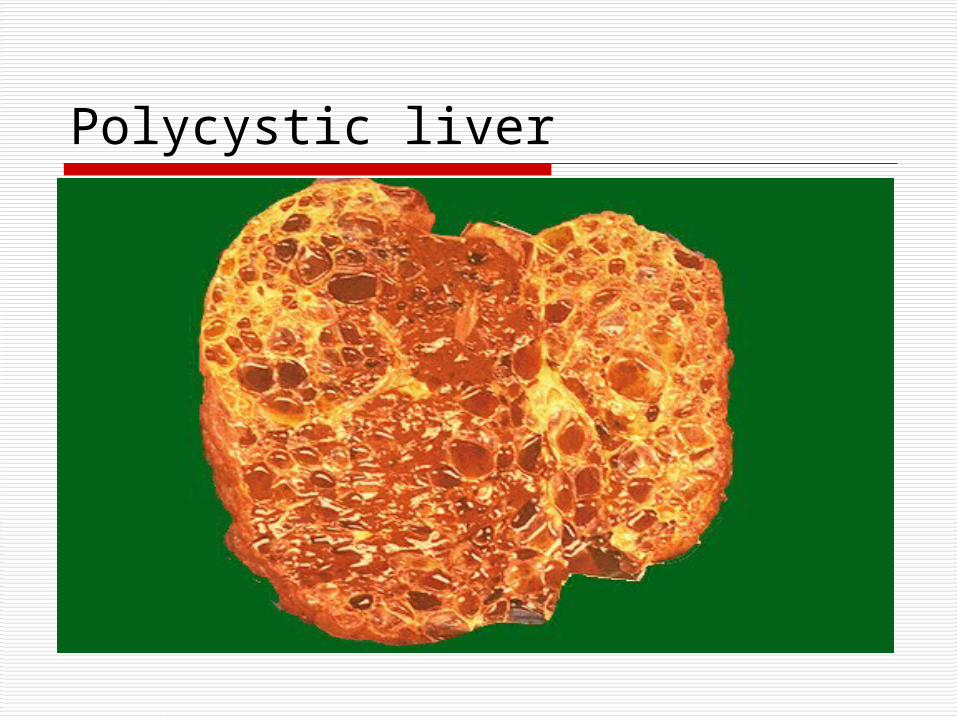
Polycystic liver

Cystic Diseases of Kidney- Hereditary
Infantile Polycystic Kidney Disease Autosomal recessive Renal failure in infancy Congenital Hepatic Fibrosis

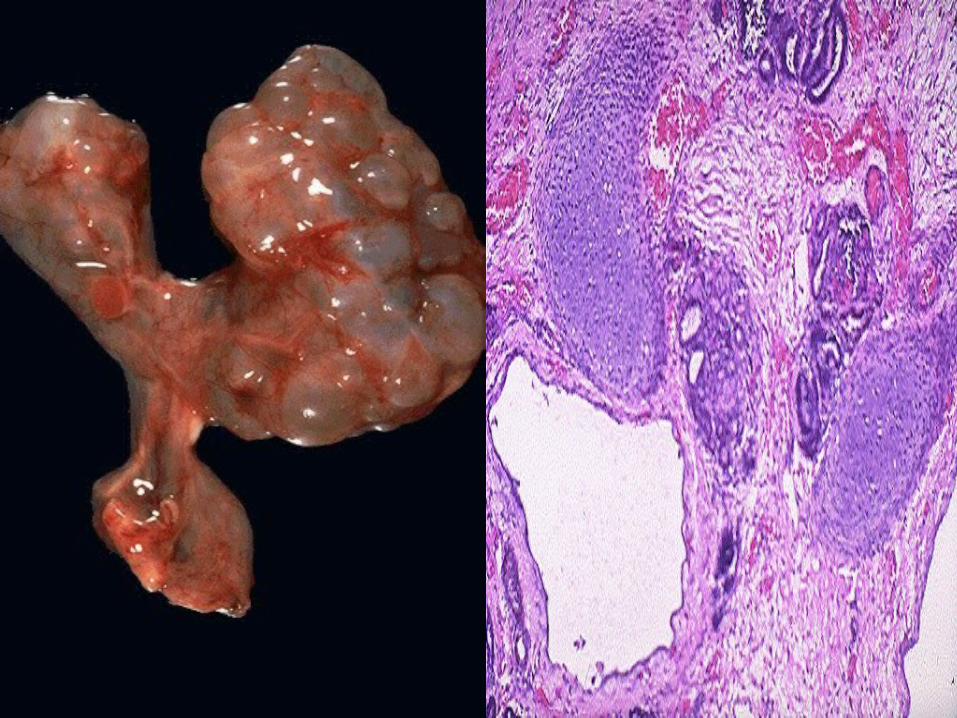
Cystic Disease of Kidney- Developmental
Cystic Renal Dysplasia Sporadic Associated with ureteropelvic
abnormality Can be unilateral or bilateral

Cystic Diseases of Kidney
Medullary Cystic Disease Medullary Sponge Kidney- adults Familial nephronophthisis- medullary
cystic disease (FN-MCD complex)- childhood
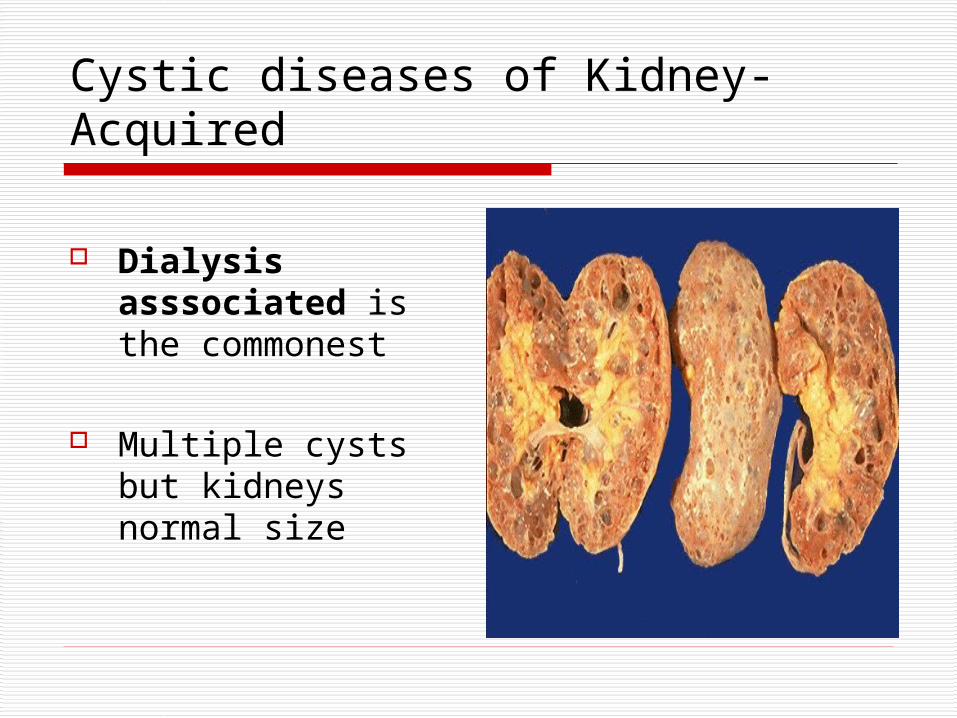
Cystic diseases of Kidney- Acquired
Dialysis asssociated is the commonest
Multiple cysts but kidneys normal size

Cystic diseases of Kidney-misc Simple Cyst Common finding at
autopsy Variable size Lined by cuboidal
epithelium

Renal neoplasms- Benign
Adenoma (papillary adenoma)
<5mm - bland papillary structures
common- seen in up to 1/3 autopsies

Renal neoplasms- Benign
Oncocytoma 3-5% of renal
tumours
Tan/ mahogany brown with central scar

Renal neoplasms- Benign
Oncocytoma Nests of oncocytic
(pink) cells Important to
differentiate from carcinoma- lack of atypia
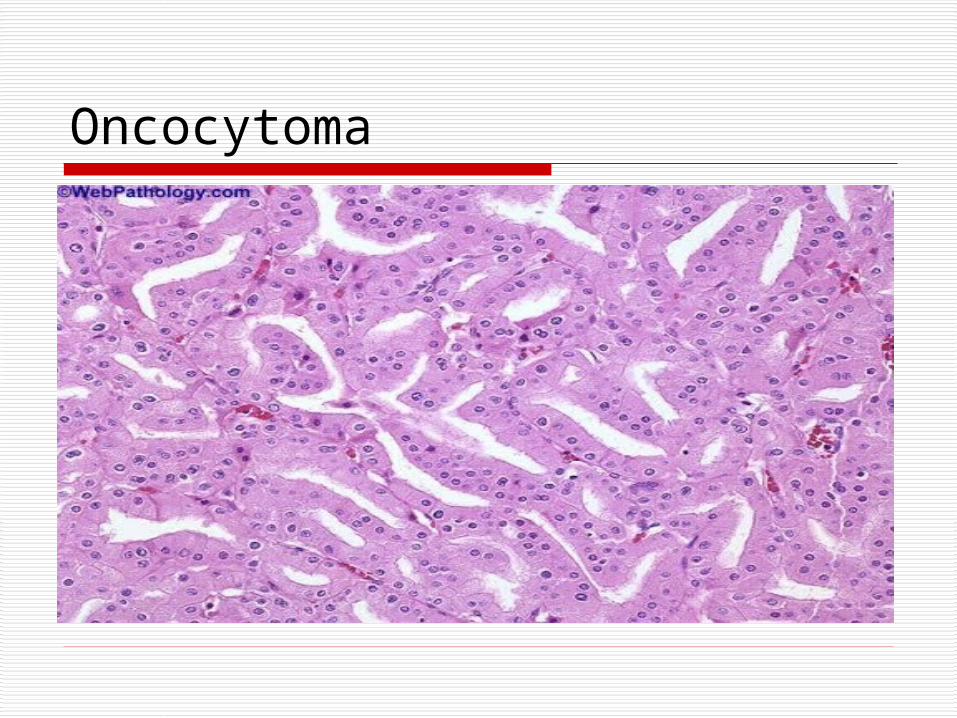
Oncocytoma

Renal neoplasms- Benign
Metanephric adenoma
Closely packed tubules/papillae
Can grow to a large size

Metanephric adenoma

Renal Cell Carcinoma:Epidemiology
Overall 12th commonest cancer in males and 17th commonest cancer in females
2-3 times more common in men Peak age in 6th and seventh decade Commoner in developed countries

Renal Cell Carcinoma:Aetiology
Tobacco smoking Arsenic compounds, asbestos ,
cadmium and pesticides ↑ Risk with ↑ BMI Long term haemodialysis

Renal Cell Carcinoma: Symptoms
Haematuria, flank pain, mass Weight loss, anorexia, fever Paraneoplastic endocrine syndromes:↑ Epo, ↑ ca ++, ↑ renin, prolactin Hepatic Dysfunction Amyloidosis

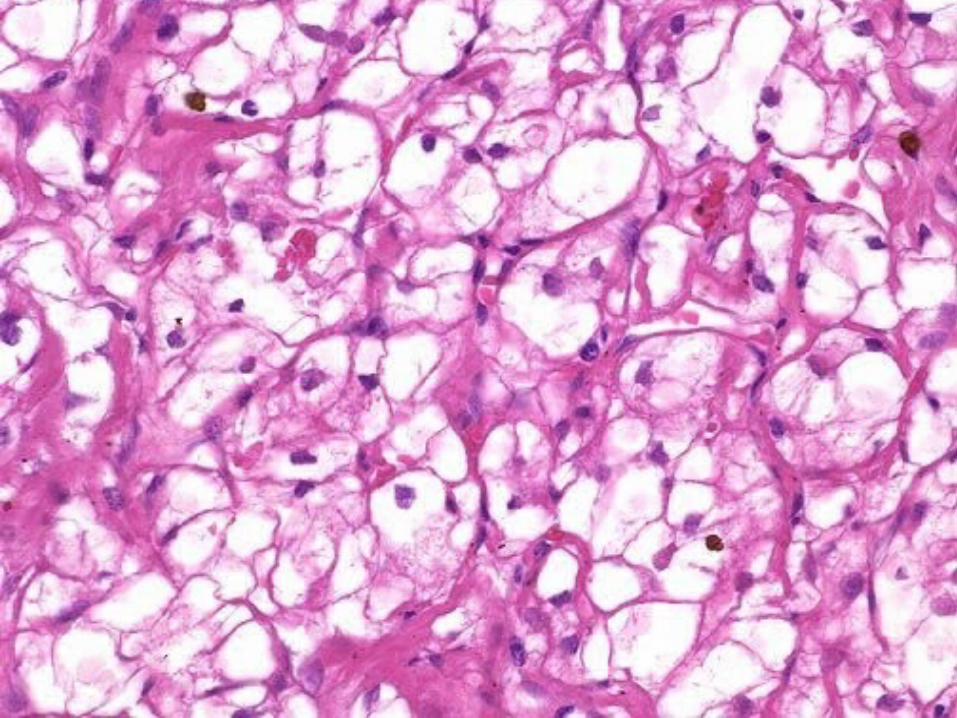
Renal Cell Carcinoma
Clear cell (conventional ) :75% Papillary:7-15% Chromophobe:3-5% Collecting Duct Carcinoma-<1% RCC unclassified eg sarcomatoid Others eg urothelial

Clear Cell Carcinoma:Genetics 95% sporadic: most have somatic 3p
deletions
5% familial: Von- Hippel Lindau disease (VHL) RCC, haemangioblastomas,
phaeochromocytoma Germline 3p25-26 deletions Loss of pVHL protein

Function of pVHL Involved in cell cycle regulation and
angiogenesis HIF1α stimulates VEGF, PDGFb, TGFa pVHL degrades HIF1α When pVHL absent- HIF1 α
accumulates-tumorigenesis is facilitated
VEGF is potential target for treatment in RCC

Classic renal cell carcinoma
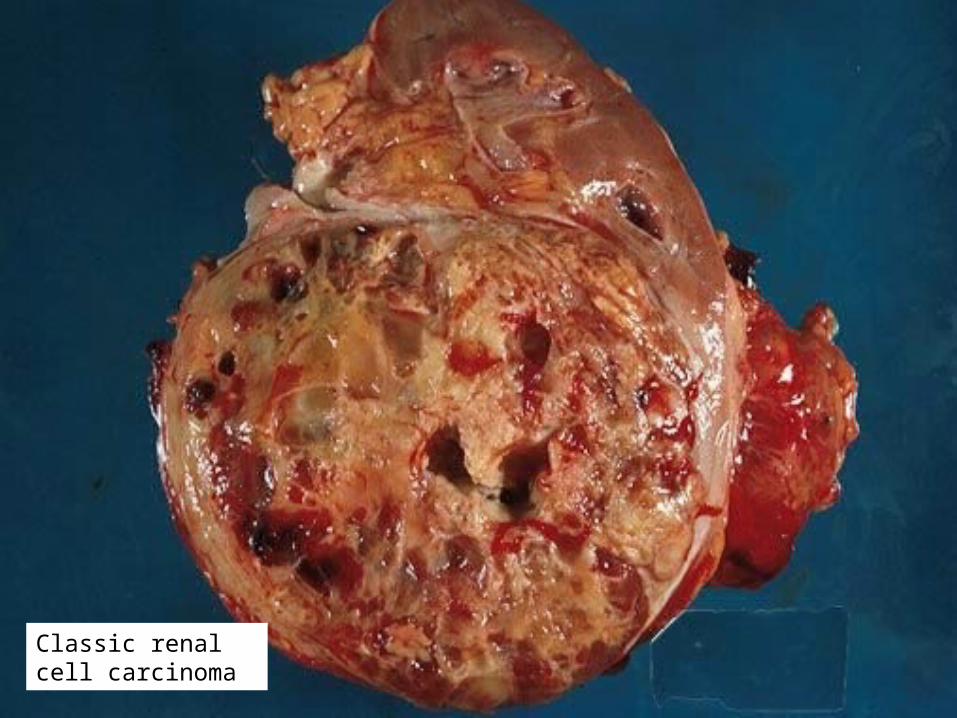
Classic renal cell carcinoma

Renal Cell Carcinoma
Clear cell (classic) :75% Papillary:7-15% Chromophobe:3-5% Collecting Duct Carcinoma-<1% RCC unclassified eg sarcomatoid Others eg urothelial

Papillary Renal Cell Carcinoma-Genetics
Sporadicvast majorityTrisomy 7, 17, loss of chromosome Y Hereditary (HPRC)Multiple bilateral tumoursMutations of MET oncogene 7q31

Papillary renal cell carcinoma

Renal Cell Carcinoma
Clear cell (conventional ) :75% Papillary:7-15% Chromophobe:3-5% Collecting Duct Carcinoma-<1% RCC unclassified eg sarcomatoid Others eg urothelial
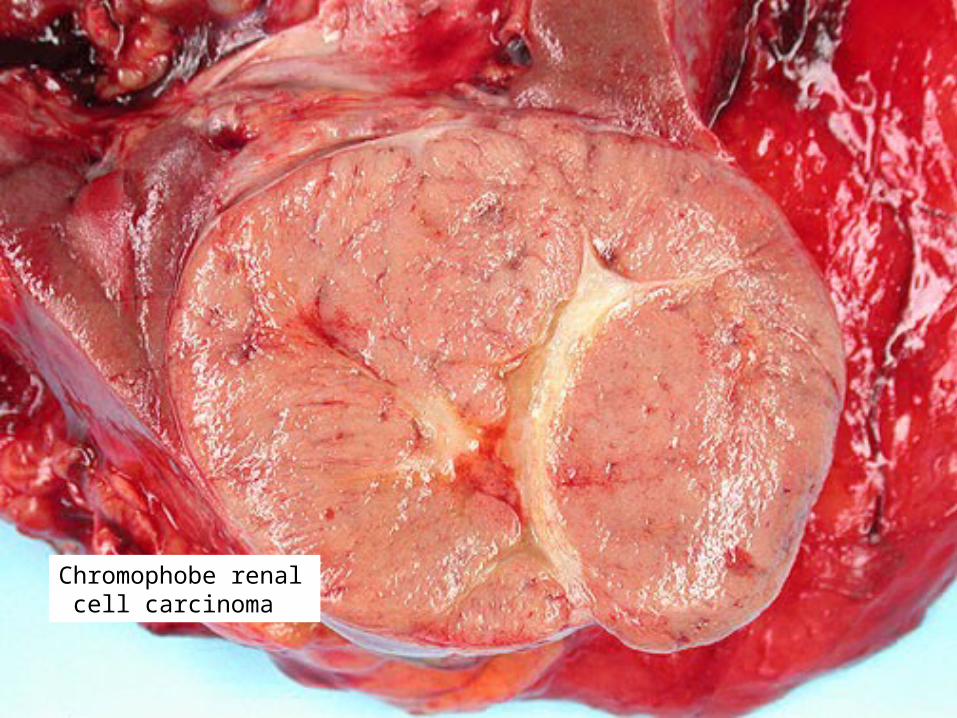
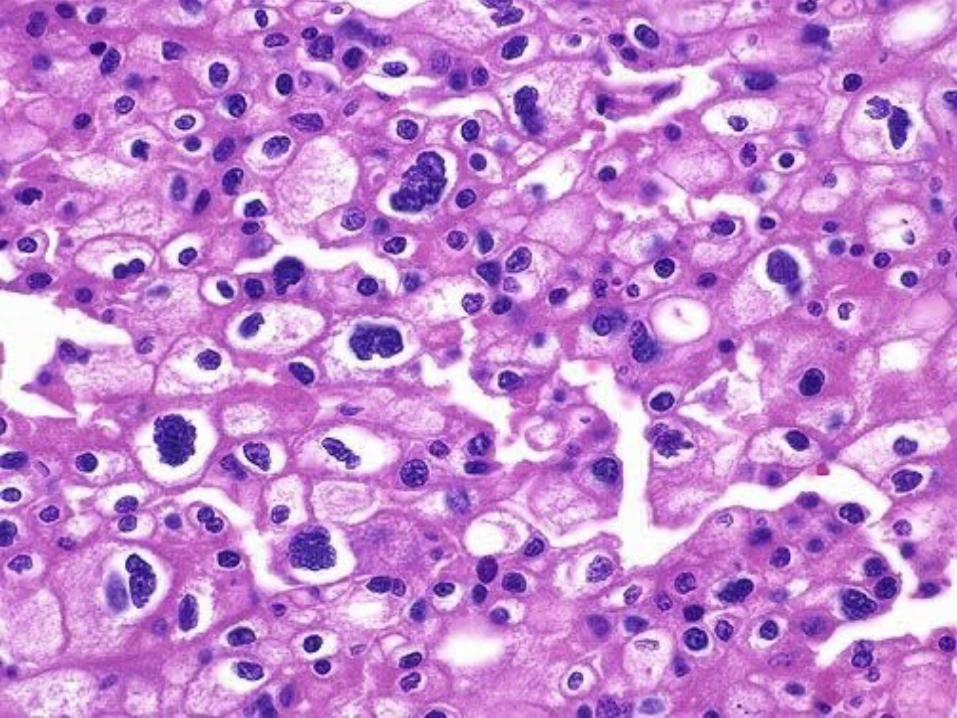
Chromophobe renal cell carcinoma
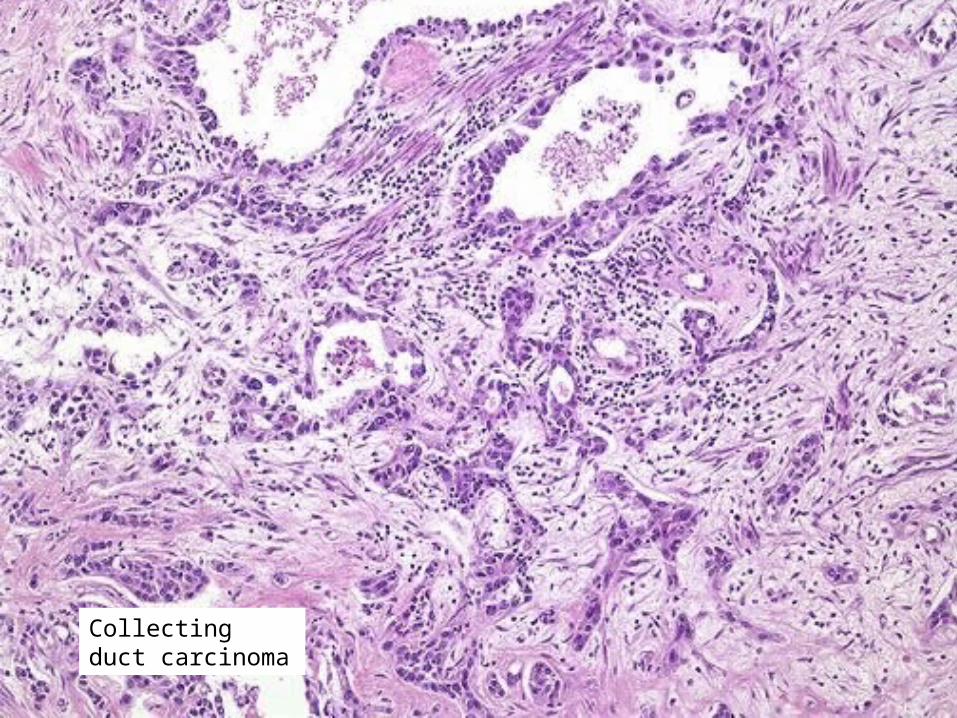
Collecting duct carcinoma

Renal Cell Carcinoma
Clear cell (conventional ) :75% Papillary:7-15% Chromophobe:3-5% Collecting Duct Carcinoma-<1% RCC unclassified eg sarcomatoid Others eg urothelial
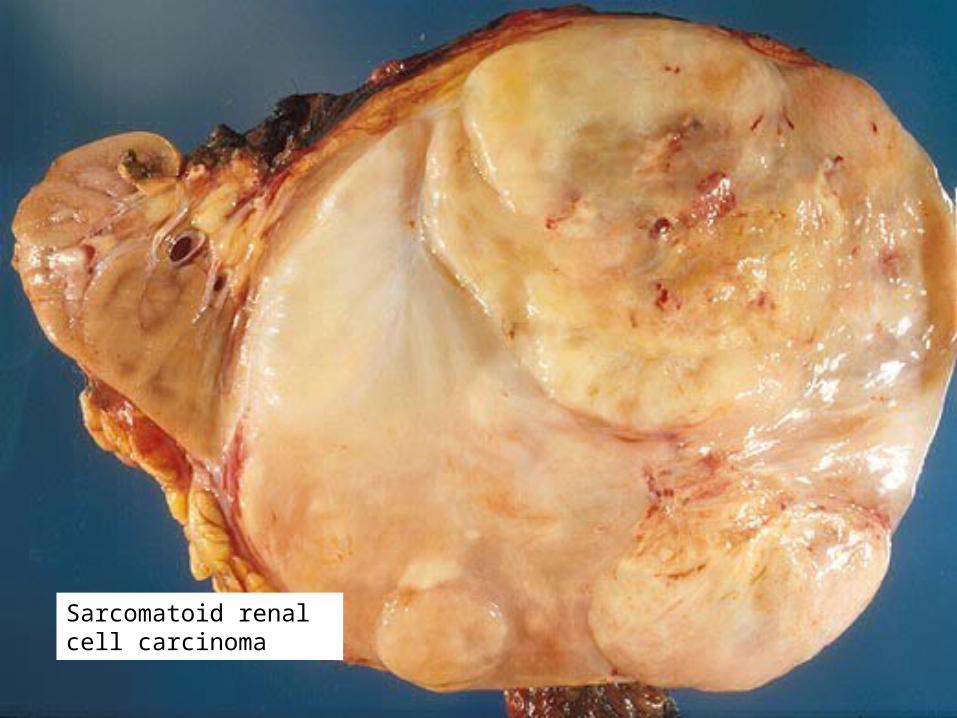
Sarcomatoid renal cell carcinoma


Renal Cell Carcinoma- Spread of Disease
Haematogenous spread via renal vein/IVC
→ Lungs→ Bone→ Liver Direct spread through capsule into
adjacent organs

Urothelial carcinoma of renal pelvis


Staging of Renal Carcinoma
pT1- < 7cm, limited to kidney pT2->7cm, limited to kidney pT3-adrenal/perinephric/major vein
invasion pT4- Beyond Gerotas fascia

Nephroblastoma (Wilms Tumour)
2-5 year olds 90% sporadic 10% associated with syndromesWAGR-WT1 mutations, 11p13Beckwith-Wiedemann-WT2 mut, 11p15

Wilms tumour

Non-epithelial renal neoplasm Angiomyolipoma Benign Sporadic (80%)or
Associated with tuberous sclerosis(20%)
autosomal dominant, caused by LOH at
TSC1( 9q34) or TSC2 (16p13)

Congenital Anomalies of Bladder
Diverticulum (can also be acquired) Exstrophy- failure of closure of
anterior wall of bladder Anormality of vesicoureteral junction Vesical fistulas (to vagina, rectum,
uterus) Persistant urachas

Bladder Carcinoma- Epidemiology
2nd commonest cancer in the UK Male:female ratio 3:1 Predominantly 5th, 6th and 7th
decade

Aetiology of bladder carcinoma
Occupational- aniline dyes, chlorinated HC
Cigarette smoking Drugs eg phenacetin,
cyclophosphamide Chronic irritation eg Shistosoma
haematobium ~ squamous ca Most are non- familial

Types of Bladder Carcinoma Urothelial/transitional cell carcinoma-90% Squamous Cell -5% Adenocarcinoma- 2% Other-3%
small cell carcinoma spindle cell carcinoma
lymphoepithelioma-like carcinoma nested variant of TCC micropapillary carcinoma


Types of Urothelial Carcinoma
Non-invasive-papillary (pTa) ca in-situ (pTis)
Invasive TCCpT1- invasion of submucosapT2- invasion of musclepT3- beyond musclepT4- invades other organs





Natural History of Bladder Carcinoma Superficial TCC
95% 5 year survival frequent recurrences
10-20% risk of disease progression Carcinoma in-situ >50% risk of disease progression Muscle invasive TCC 35% 5 year survival

Mesenchymal Lesions in Bladder
Leiomyoma Leiomyosarcoma Post-operative spindle cell nodule Inflammatory pseudotumour

Thank You


















