
Computerized triage: One department's process
6
Computerized triage: One department'sprocess Authors: Donna Mason, RN, BS, CEN, Pamela Gibson, RN, and Darnell Sanders, RN, Nashville, Tennessee I 'n the constantly evolving atmosphere of emer- ,gency nursing, nurses and nurse managers are continuously seeking new methods to (1) expedite patient flow through the emergency department, (2) provide a standard of care that is consistent from nurse to nurse, (3) place patients in the appropriate health care setting in the most cost-efficient manner, and (4) provide documentation that can be carried throughout the continuum if the patient is admitted. This article shares our experience of how our emer- gency department planned, implemented, and per- forms ongoing evaluation of our computerized triage system. Historical information Baptist Hospital is a not-for-profit hospital located in the Middle Tennessee area. The facility is licensed for 759 inpatient beds and serves as a tertiary care cen- ter for the Middle Tennessee region. The emergency department has an annual census of 54,000 visits. It consists of a 25-bed acute care area, an 8-bed fast track, and a 6-bed chest pain center located in the acute care area. The chest pain center has an annual census of 8500 visits per year. In 1995 the emergency department completed a renovation project that allowed placement of personal computers in 17 of the 25 acute care rooms. Computers continue to be placed in additional rooms, pending departmental budget approvals. The acute care area is divided into four patient care pods. Each pod has its own nursing station with a computer and a laser printer. In the early 1990s our hospital-based computer system was strictly a data entry and financial system. In July 1990 the hospital purchased arld~-implemented a clinical system. The Information Mana~'ement De- partment hired personnel from the computer company to be on-site and available to initiate programs and better use the system. The staff were nurses who were familiar with nursing care plans, diagnosis, and docu- mentation requirements from regulatory agencies. Before computerization of clinical date, one of the quality improvement mechanisms for assessment Donna L. Mason is director; Pamela Gibson is a staff nurse; and Darnell Sanders is ER supervisor, Emergency Pavilion, Baptist Hospital, Nashville, Tennessee. J Emerg Nurs 1997;23:330-335. Copyright © 1997 by the Emergency Nurses Association. 0099-1767/97 $5.00 + 0 18/1/83995 and treatment in the emergency department was the random review of patient charts by the educational coordinator. The clarity, of documentation was reviewed to ensure that the minimum standards of documentation had been used in the triage process. Charts were edited and returned to the particular nurse who had performed the triage, pointing out per- tinent information that was not documented regard- ing a specific chief symptom. This proved to be a thought-provoking process and enhanced the triage skills of the nursing staff. It was also during this peri- od that the emergency department accepted new graduates for the first time. During this period we determined that staff com- petency varied a great deal. Although new graduates could not perform the "initial" triage until 1 year of emergency nursing was completed, they did perform bedside assessments of urgent and emergent patients. The educational coordinator developed a card file system to address key chief symptoms, assessment associated with the chief symptoms, common nursing diagnosis, and what determined the urgency rating system of certain assessment find- ings. This file was strategica]ly located in the depart- ment as a resource guide. This method worked well for approximately 2 years. The new clinical computer system and our deter- mination that documentation of assessment had improved with the card file system initiated the idea to use computers to document triage. These two sys- tems would ensure that a less experienced nurse would be directed to ask pertinent questions of the patient or significant others to gather the information needed to determine urgency and assist with the decision-making process. Planning phase In 1993 a performance improvement team (PIT) was developed in the department to address these needs. The committee was composed of nurses who were experienced and considered to have expertise in the triage process. This committee was given the task of determining whether the computer system could be developed and programmed to meet the triage needs in the department. Other members of the team included an emergency physician and a representa- tive from the Information Management Department (MIS). Other health care members were invited to 330 Volume 23, Number 4
-
Upload
donna-mason -
Category
Documents
-
view
214 -
download
2
Transcript of Computerized triage: One department's process

Computerized triage: One department's process Authors: Donna Mason, RN, BS, CEN, Pamela Gibson, RN, and Darnell Sanders, RN, Nashvi l le , T e n n e s s e e
I 'n the cons t an t ly evolv ing a t m o s p h e r e of emer - ,gency nurs ing , nu r ses a n d nurse m a n a g e r s a re
con t inuous ly s e e k i n g n e w m e t h o d s to (1) e x p e d i t e p a t i e n t flow th rough the e m e r g e n c y d e p a r t m e n t , (2) p rov ide a s t a n d a r d of ca re tha t is c o n s i s t e n t from nurse to nurse , (3) p l ace p a t i e n t s in t he app rop r i a t e hea l th care s e t t i ng in t he m o s t cos t -ef f ic ient manner , a n d (4) p rov ide d o c u m e n t a t i o n tha t can b e car r ied t h roughou t t he c o n t i n u u m if t he p a t i e n t is admi t t ed . This ar t ic le sha res our e x p e r i e n c e of h o w our emer - g e n c y d e p a r t m e n t p lanned , i m p l e m e n t e d , and per- forms ongoing eva lua t ion of our c o m p u t e r i z e d t r i age sys tem.
Historical information Bapt i s t Hosp i ta l is a not-for-profi t hosp i ta l l oca ted in t h e Midd le T e n n e s s e e area. The facil i ty is l i c ensed for 759 i n p a t i e n t b e d s and se rves as a t e r t i a ry care cen- ter for t he Midd le T e n n e s s e e region. The e m e r g e n c y d e p a r t m e n t has an annua l c ensus of 54,000 visi ts . It cons i s t s of a 25-bed a c u t e care area, an 8-bed fast t rack, and a 6 -bed c h e s t pa in cen te r l oca t ed in t he a c u t e care area. The c h e s t pa in cen te r has an annua l c e n s u s of 8500 v is i t s per year. In 1995 the e m e r g e n c y d e p a r t m e n t c o m p l e t e d a r enova t i on p ro jec t t h a t allowed p l a c e m e n t of pe r sona l c o m p u t e r s in 17 of t he 25 a c u t e ca re rooms. C o m p u t e r s con t inue to b e p l a c e d in add i t iona l rooms, p e n d i n g d e p a r t m e n t a l b u d g e t approvals . The a c u t e care a rea is d iv ided into four p a t i e n t care pods . E a c h pod has i ts own nu r s ing s ta t ion wi th a c o m p u t e r a n d a laser printer .
In t he ear ly 1990s our h o s p i t a l - b a s e d c o m p u t e r s y s t e m w a s s t r ic t ly a d a t a en t ry and f inancia l sys t em. In July 1990 the hosp i ta l p u r c h a s e d arld~-implemented a cl inical sys tem. The Informat ion Mana~ ' emen t De- p a r t m e n t h i red pe r sonne l from the c o m p u t e r c o m p a n y to be on-s i te and ava i lab le to in i t ia te p r o g r a m s and be t t e r use t he sys t em. The staff were nu r ses who were familiar w i th nu r s ing ca re plans, d iagnos i s , and docu- m e n t a t i o n r e q u i r e m e n t s from regula tory agenc ie s .
Before c o m p u t e r i z a t i o n of cl inical date , one of the qual i ty i m p r o v e m e n t m e c h a n i s m s for a s s e s s m e n t
Donna L. Mason is director; Pamela Gibson is a staff nurse; and Darnell Sanders is ER supervisor, Emergency Pavilion, Baptist Hospital, Nashville, Tennessee. J Emerg Nurs 1997;23:330-335. Copyright © 1997 by the Emergency Nurses Association. 0099-1767/97 $5.00 + 0 18/1/83995
a n d t r e a t m e n t in t he e m e r g e n c y d e p a r t m e n t w a s the r a n d o m rev iew of p a t i e n t char t s by the educa t i ona l coordinator. The c la r i ty , of d o c u m e n t a t i o n w a s r e v i e w e d to ensu re tha t t he m i n i m u m s t a n d a r d s of d o c u m e n t a t i o n h a d b e e n u s e d in the t r i age process . Char ts we re e d i t e d and r e tu rned to t he par t icu la r nurse who h a d pe r fo rmed the t r iage, p o i n t i n g out per- t i nen t informat ion t ha t was no t d o c u m e n t e d regard- ing a spec i f ic ch ief s y m p t o m . This p roved to b e a t hough t -p rovok ing p roces s a n d e n h a n c e d the t r iage skills of t he nur s ing staff. It w a s also du r ing th i s peri- od t ha t t he e m e r g e n c y d e p a r t m e n t a c c e p t e d n e w g r a d u a t e s for t he first t ime.
Dur ing this pe r iod w e d e t e r m i n e d t ha t staff com- p e t e n c y va r ied a g rea t deal. A l though n e w g r a d u a t e s could not perform the "initial" t r i age unt i l 1 year of e m e r g e n c y nurs ing w a s comple ted , t h e y d id per form b e d s i d e a s s e s s m e n t s of u r g e n t a n d e m e r g e n t pa t i en t s . The educa t i ona l coord ina tor d e v e l o p e d a ca rd file s y s t e m to a d d r e s s key chief s y m p t o m s , a s s e s s m e n t a s s o c i a t e d wi th t he chief s y m p t o m s , c o m m o n nurs ing d iagnos i s , and w h a t d e t e r m i n e d the u r g e n c y ra t ing s y s t e m of cer ta in a s s e s s m e n t find- ings. This file was s t ra tegica] ly l oca t ed in t he depa r t - m e n t as a r e source guide . This m e t h o d w o r k e d well for app rox ima te ly 2 years .
The n e w cl inical c o m p u t e r s y s t e m and our de ter - m i n a t i o n tha t d o c u m e n t a t i o n of a s s e s s m e n t had i m p r o v e d wi th t he ca rd file s y s t e m in i t i a t ed the idea to u se c o m p u t e r s to d o c u m e n t t r iage. T h e s e two sys- t e m s would ensu re tha t a less e x p e r i e n c e d nurse would b e d i r e c t e d to ask p e r t i n e n t q u e s t i o n s of the p a t i e n t or s ign i f i can t o thers to ga the r t he informat ion n e e d e d to d e t e r m i n e u r g e n c y and a s s i s t w i th the d e c i s i o n - m a k i n g process .
Planning phase In 1993 a pe r fo rmance i m p r o v e m e n t t e a m (PIT) was d e v e l o p e d in the d e p a r t m e n t to a d d r e s s t h e s e needs . The c o m m i t t e e w a s c o m p o s e d of nu r se s w h o were e x p e r i e n c e d and c ons ide r e d to have expe r t i s e in the t r i age process . This c o m m i t t e e w a s g iven the t a sk of d e t e r m i n i n g w h e t h e r t he c o m p u t e r s y s t e m could be d e v e l o p e d and p r o g r a m m e d to m e e t t he t r i age n e e d s in t he d e p a r t m e n t . Other m e m b e r s of t he t e a m i n c l u d e d an e m e r g e n c y p h y s i c i a n a n d a r e p r e s e n t a - t ive from the Informat ion M a n a g e m e n t D e p a r t m e n t (MIS). Other hea l th ca re m e m b e r s w e r e inv i t ed to
330 Volume 23, Number 4

Mason, Gibson, and Sanders/JOURNAL OF EMERGENCY NURSING
TRIAGE GENB~AL NOTES ~UNABLE TO OBTAIN PRIOR HISTORY
PT HISTORY OF YES CARDIOVASCULAR PROBLEMS... * *
CARCB~ . . . . . . . . . . . . . . . . . . . . * *
DIABETES . . . . . . . . . . . . . . . . . . * *
GASTROINTESTINAL PROBLEMS. * *
HEPATITIS . . . . . . . . . . . . . . . . . * *
HIV . . . . . . . . . . . . . . . . . . . . . . . * *
KIDNEY PROBLEMS . . . . . . . . . . . * *
RESPIRATORY PROBLEMS . . . . . . * *
SEIZURES . . . . . . . . . . . . . . . . . . * *
SICKLE CELL . . . . . . . . . . . . . . . * *
THYROID PROBLEMS . . . . . . . . . . * *
DENIES ANY/ANY OTHER SIGNIFICANT MEDICAL PROBLEMS
xNEXT
Figures l a n d 2
TRIAGE GENERAL NOTES CURRENT MEDS
Ct.RRENTLY TAKING
xNO MEDICATIONS
MED:
DOSAGE:
FREQUENCY:
LAST DOSE TAKEN:
ADDITIONAL MEDS *YES xNO
xCURRENT/ADDITIONAL CURRENT MEDS RECORDED MANUALLY
Examples of information obtained during the general information section on all patients.
a t t e n d if the i r spec i f ic a rea of expe r t i s e w a s n e e d e d (e.g., admiss ions ) .
The c o m m i t t e e ' s goal w a s to improve the s t an - da rd of t r i age a s s e s s m e n t for all nurses . Other goals we re to d i rec t t he nurse to ask p e r t i n e n t in format ion r e g a r d i n g a spec i f i c ch ief s y m p t o m . This would also al low a s y s t e m a t i c a p p r o a c h of d o c u m e n t a t i o n for h is tor ica l a n d phys i ca l f indings. One of t he advan - t a g e s of t he p r o g r a m w a s to force a less e x p e r i e n c e d nurse w i th w e a k e r a s s e s s m e n t skills to ask t h e r igh t ques t i ons of p a t i e n t s a n d to have the d o c u m e n t a t i o n of t he i n t e rv i ew reflect t hose ques t ions .
The first m e e t i n g s we re b r a i n s t o r m i n g sess ions . The m e m b e r s d e c i d e d t ha t t r i age ques t i ons for a dif- f icul t c h i e f s y m p t o m w o u l d b e d e v e l o p e d first. B e c a u s e a b d o m i n a l pa in is a f r equen t t h o u g h of ten difficult s y m p t o m to assess , i t wou ld b e first. E a c h m e m b e r of t h e group d e v e l o p e d ques t ions t ha t t h e y a s k e d of all p a t i e n t s w i th a b d o m i n a l pain. Af ter all p e r t i n e n t in format ion w a s p r e sen t ed , t he MIS nu r se p r o g r a m m e d t h e ques t ions in a s y s t e m a t i c m a n n e r tha t fol lowed a s m o o t h course in t he c o m p u t e r sys- tem. M e e t i n g s l a s t ing 1 to 2 hours w e r e he ld w e e k l y to work on o the r ch ief s y m p t o m s .
We d e t e r m i n e d tha t it w a s i m p o r t a n t to l imit t he n u m b e r of ques t i ons to l imit t he t r i age p roce s s to 5 to 7 minu tes , a d e p a r t m e n t s t a n d a r d a c c o r d i n g to t i m e s t u d i e s pe r fo rmed . The in fo rma t ion a s k e d of all p a t i e n t s w a s c o n s i d e r e d genera l informat ion (F igures 1 and 2) and would b e t he first informat ion asked . E a c h pe r son on t h e PIT d e t e r m i n e d t h e course of his or her own q u e s t i o n i n g a n d t h e MIS nu r se fo rma t t ed the p a t h w a y s to inc lude all t he n e c e s s a r y informa- tion. Ques t i ons t ha t were c o n s i d e r e d m o s t i m p o r t a n t
we re to b e a n s w e r e d before t he nex t s c r een a p p e a r e d on the computer . This i n c l u d e d informat ion on bo th ma le a n d female pa t i en t s .
The nex t nu r s ing t a sk w a s to m a n d a t e a s c r een t ha t a s s i s t e d the nurse in d e t e r m i n i n g the app rop r i a t e nu r s ing d i agnos i s and u r g e n c y dec is ion . We d e c i d e d t ha t e a c h poss ib l e nu r s ing d i agnos i s and condi t ion tha t a s s i s t e d in t he u r g e n c y ra t ing p roc e s s would pre- s en t on the c o m p u t e r sc reen . The las t dec i s ion in- volved s e e k i n g a s s i s t a n c e of t he ED A d m i s s i o n s office in d e t e r m i n i n g the t e c h n i c a l r e q u i r e m e n t s for pro- c e s s i n g paperwork , d e c i d i n g w h e r e i t ems n e e d e d to b e pr in ted , and i n p u t t i n g n e c e s s a r y m a n a g e d care information.
Education o f staff After t he t r i age ques t i ons for the first ch ief s y m p t o m were c o m p l e t e d and a p p r o v e d by the commi t t ee , the staff e d u c a t i o n began . The c o m m i t t e e be l i eved the l ea rn ing p roc e s s w i th one p r imary s y m p t o m would not h inde r t he t r i age s t a n d a r d s y e t would al low the staff to b e c o m e famil iar w i th t he p rogram. The com- pu te r a l lowed a "test" p a t i e n t so staff could p rac t i ce at any t ime on any c o m p u t e r wi th in the d e p a r t m e n t .
The cha i rpe r son of t he c o m m i t t e e p rov ided staff e d u c a t i o n a n d pe r fo rmed c o m p e t e n c y c o m p o n e n t s for e a c h ind iv idua l staff member . Other c o m m i t t e e m e m - be r s b e c a m e "super users" of t he s y s t e m and covered all shif ts a s r e source persons . After staff e d u c a t i o n w a s comple ted , t he p h y s i c i a n s in t he d e p a r t m e n t r ece ived t r a in ing on the project . The p h y s i c i a n s a p p r o v e d each p r imary s y m p t o m b y a major i ty vote, and e a c h phys i - c ian h a d inpu t on h o w the format w a s p r in t ed to ass i s t thei r needs . Each se s s ion l a s t ed 2 hours. After all edu-
August 1997 931

JOURNAL OF EMERGENCY NURSING/Mason, Gibson, and Sanders
T R I A G E GENERAL NOTES
LAST MENSTRUAL PERIOD
( E A R L Y ) ( J A N ) ( J U L ) ( 9 6 ) ( M I D ) ( F E B ) ( A U G ) ( L A T E ) ( M A R ) ( S E P ) ( 9 5 )
( A P R ) ( O C T ) (NOW) ( M A Y ) ( N O V ) ( 9 4 )
( J U N ) ( D E C )
( N / A , HYSTERECTOMY) ( N / A , POST-MENOPAUSE) ( N / A , PREMENSES)
Figure 3 The system has the ability to meet the needs of each female pat ient 's last menstrual period. This information must be obtained on all patients.
TRIAGE NOTES CHEST PAIN
AGGRAVATING FACTORS NONE DEEP BREATH EXERTION MOVEMENT
A L L E V I A T I N G FACTORS *NONE
FOOD MEDICATIONS NITROGLYCERINE
~NEXT
Figure 5 The process mandates relief or aggravation for most pat ients who are in pain.
TRIAGE NOTES ABDOMINAL PAIN
PT C/O PT DENIES ( , ) NO C/O PT APPEARS TO HAVE (AND)
CONSTANT INTERMIT PROGRESSIVE CRUSHING MILD RADIATING DECREASED MODERATE SEVERE DULL OCCASIONAL SHARP GENERAL PERSISTANT SUDDEN INCREASED PHANTOM
ACHING GAS PAIN SPASM BURNING H E A D A C H E TENDERNESS CRAMP H U M M I N G TENSENESS DISCOMFORT PAIN THROBBING DISTENSION S O R E N E S S TIGHTNESS
xNEXT
Figure 4 Only a small amount of typing i~ necessary. Most information is selectable. There is al~a-y-s .~ "Type- in" section for addition of unusual information.
ca t ion w a s comple ted , a t a r g e t da t e w a s se t for ac tua l imp lemen ta t ion . A t th is point , the c o m m i t t e e h a d c o m p l e t e d t r i age ques t i ons for the major i ty of ch ief s y m p t o m s a n d thei r p a t h w a y s . As the nur s ing staff b e c a m e familiar w i th one chief symptom, ano ther w a s i m p l e m e n t e d . Current ly all n e w staff m e m b e r s are ed- u c a t e d in t he s a m e m a n n e r and c o m p e t e n c y is veri- f ied dur ing t h e or ien ta t ion process . Nur se s who have no t ye t a t t a i n e d 1 yea r of ED e x p e r i e n c e are still t r a ined to u se t he s a m e s y s t e m at the beds ide .
Triage process format C o m p u t e r t r i age w a s d iv ided into t h ree major ca te- gories: (1) genera l in format ion d e e m e d n e c e s s a r y of all p a t i e n t s t ha t en t e r t he sys t em: m e t h o d of arrival, c o n s e n t for t r e a tme n t , t ime of in terview, p r iva te phys i c i an , p r imary ca re phys ic i an , l a s t m e n s t r u a l pe r iod (Figure 3), vi ta l s igns, al lergies, a n d p r e s e n t med ica t i ons ; (2) ch ief s y m p t o m and p e r t i n e n t infor- m a t i o n n e e d e d r e g a r d i n g the s y m p t o m (Figures 4 and 5); (3) c lass i f ica t ion of t he pa t ien t , t he genera l a rea for t r ea tmen t , a n d the nu r s ing d iagnos i s .
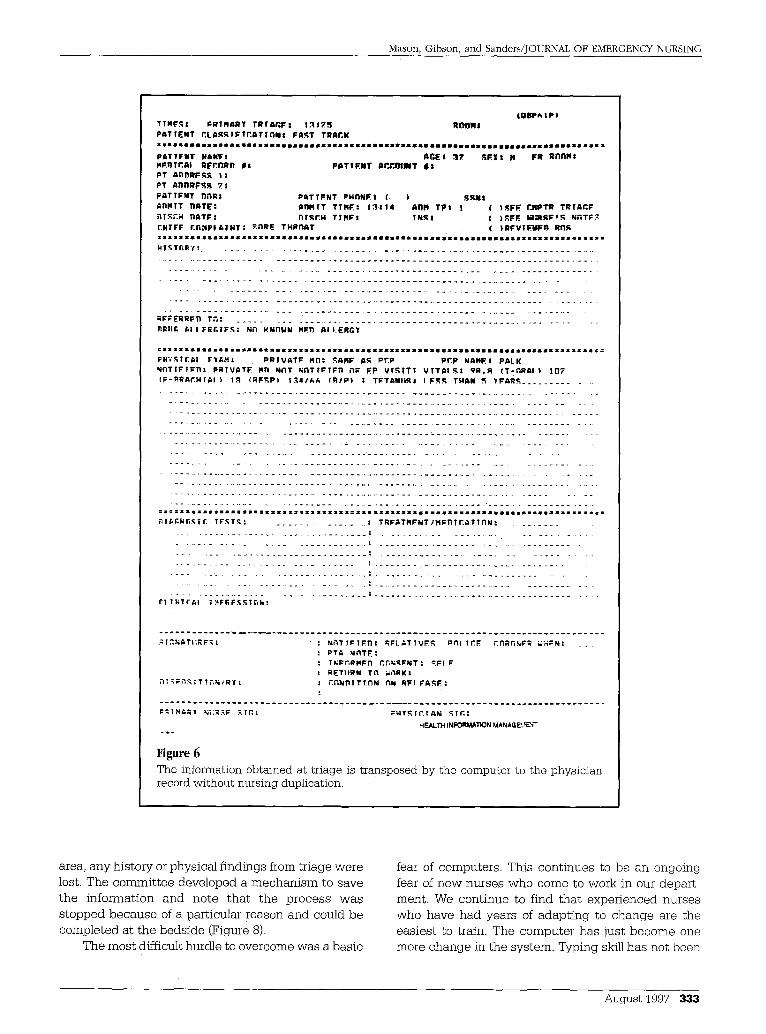
Once the p a t i e n t w a s p l a c e d in a t r e a t m e n t area, t h e ini t ia l eva lua t ion could b e u p g r a d e d a n d add i - t ions m a d e t h rough the c o m p u t e r sys t em. B e c a u s e of th is p r o c e s s and fol low-through, t he m e d i c a l record (also on compute r ) could b e g e n e r a t e d for t he phys i - c i an w i th t he vi tal s igns, al lergies, p r iva te phys i c i an , p r ima ry ca re phys ic i an , and c o n s e n t for t r e a t m e n t to b e p l a c e d on the record w i thou t dup l i ca t ion from the nu r s ing staff (Figure 6).
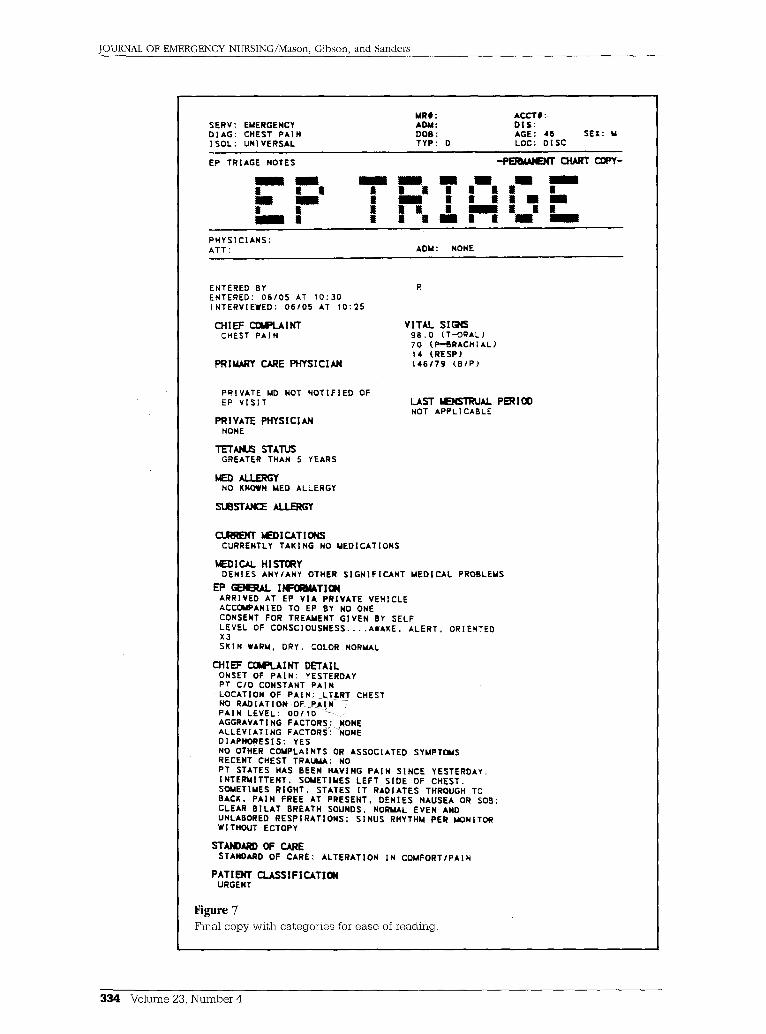
Upgrades and changes We have m a d e some c h a n g e s s ince t he i m p l e m e n t a - t ion of t he t r i age sys tem. The p h y s i c i a n s h a d t rouble l oca t i ng informat ion on the ha rd copy t ha t w a s pro- duced . The c o m m i t t e e r e c o n v e n e d a n d d e v e l o p e d a format t ha t c a t e g o r i z e d ce r ta in a s p e c t s of t r i age tha t we re i m p o r t a n t to phys i c i ans . T h e s e c a t e g o r i e s were also p r i n t e d in bold t ype to a s s i s t in ea sy r e a d i n g (Figure 7). We iden t i f i ed ano the r p roblem: If a p a t i e n t w a s s ick e n o u g h to b e b r o u g h t d i rec t ly to a t r e a t m e n t
:932 Volume 23, Number 4
Mason, Gibson, and Sanders/JOURNAL OF EMERGENCY NURSING
T T M F K I PRTHARY T R f A K F 8 I ~ S ~ RI~r)NI P A T I E N T ~ L A R ~ I F T E A T I n N $ FART TRACK S S S S S I m S S S l S S m S S 8 4 S S m S I B S S S J S I I m S I ~ I S ~ I I ~ I S S S ~ B S m S m O O I B B B ~ B B B S # ~ S S S S ~ B M ~ 8 ~ S S S
P 6 T T F N T N ~ H F ! A ~ E I ] ? ~ E ~ I H F R R n n N I
~ F R I ~ A I R F C ~ R f l ~$ P ~ T T ~ N T ~ r ~ ' ~ l ~ T l l ~T ~ n n R F R R t :
PT n n n w F ~ ? :
P A T T F N T ~ n R $ P ~ T T F N T ~ ; ~ N ~ I ( ) ~ R N I a ~ R I T ~ T E : ~n f f iTT T T R F : 1~ .114 ~ T P t I ( } R F ~ F ~ p T R T R T A ~ F R ; R ~ H B A T F ! ~ T ~ H T T H P | T N ~ I ( I R F E B ~ R F t R M ~ T F ~ £HTFF £ ~ P I ~ | N T : R~RE T ~ R n A T ( t R F V T F W F f l R~R
z : Z l I Z ~ I I I I I I I i I I I I I ~ I I I I I I I ~ I I I S ~ I ~ 8 ~ a I I I I I I ~ I I B ~ I m I I I I ~ B I I I I i ~ S ~ S l I I I ~ I I I S H T ~ T ~ R ~ : . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
R F ~ E R R F ~ T ~ : . . . _ . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ~ I i £ ~ I I F ~ T F ; : N~ R N n I N H~O A I I . E R ~ ¥
==z = • • • z • == z I s l z l I l l = ~ I I Z ~ I I S : l l l l l l l l l l Z ~ l ~ = l I ~ I I I I I I I I I I I I I I I I S ~ I S l I Z I Z = Z : :
F W ; ; T ~ I F X ~ : P R | V A T P ~ B : RARF ~R P ~ P PCP MANEt P A L K M ~ T T F T ~ : PRTVATF" ~ N ~ T N ~ T T F T F n ~ ~ P V T ~ | T : V T T ~ I ~ I 9 R . R ( T - ~ R G I ) fOR ( P - R R A ~ H T A I ) I R ( R F R P ) I ~ 4 1 k ~ ( R / P ) ; T P T & i I ~ I I F ~ THAN ~ ¥ F A R ~ . . . . . . . . . . . . .
IlI II II: IZ I : Illlll IIIIiI IIlillII III I l l l i l I I I I IIII !ill ii Ill I i i i I i I ii II II IIIIIIiI
~ A C ~ n R | ~ T F ~ T ~ : . . . . . . . . . . . . . . . T R F A T M F N T I H r n T ~ R T T n M : . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . o . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
: IT ,%t- , IATi~F~: " : N ~ T T I = T F . n : R~L~ ,TTVER p r l i TI'I.F. I~i~RI'INF~ ~:-i l=N: . : p T ~ NI~TIE : : t ~;f:r, RMFn ~.F,1;qI~NT : .~.FI F : RETI IRN TI~ ;;,'~RKz
~ T ~ - , ~ T T T ~ ' , ~ i i R ~ : : ~ n N n T T T n N ~ l l RF; F A R I ~ :
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
P;THC, Ry N; ;R~F .'~Tr,: : k i Y ~ | I ' ~ T A N ~ T ~ |
~F_ALTH I N F ~ I ~ O N MANAG~.~E~ -
Figure 6 The information obtained at triage is transposed by the computer to the physician record without nursing duplication.
area, any history or physical f indings from tr iage were lost. The commi t t ee developed a m e c h a n i s m to save
the in fo rmat ion and no te tha t the p rocess wa s s topped b e c a u s e of a part icular reason and could be comple ted at the beds ide (Figure 8).
The mos t difficult hurdle to overcome was a bas ic
fear of computers . This con t inues to be an ongoing fear of n e w nurses who come to work in our depart- ment . We con t inue t o find that exper ienced nurses who have had years of adap t ing to change are the eas ies t to train• The compute r has just b e c o m e one more change in the system• Typing skill has not b e e n
August 1997 339
JOURNAL OF EMERGENCY NURSING/Mason, Gibson, and Sanders
MR#: ACCT#: SERV: EMERGENCY AOM: DIS: DIAG: CHEST PAIN DOB: AGE: 4E ISOL: UNIVERSAL TYP: D LOC: DISC
SEX: M
EP TRIAGE NOTES
/ I / I l I I I II I n I II I I I / l l n • l i I l l l I I I l l i l H l l
~ ~ ~ ~ -
l l | | l i l l | I
i i
PHYSICIANS: ATT: ADM: NONE
ENTERED BY ENTERED: 06/05 AT 10:30 INTERVIEWED: 06/05 AT 10:25
CHIEF C014~LA I NT CHEST PAIN
PRIMARY CARE PHYSICIAN
VITAl. SIGNS 98.0 (T--ORAL) 70 (F~"BRACHIAL) 14 (RESP) 146179 (B/P)
PRIVATE MD NOT NOTIFIED OF EP VISIT
PRIVATE PHYSICIAN NONE
TETANU~ STATUS GREATER THAN 5 YEARS
~ I~'~GY NO KNOWN MED ALLERGY
SUBSTANCE AtI~,GY
LAST MENSTRUAL PERiO0 HOT APPLI CABLE
MEDICATIONS CURRENTLY TAKING NO MEDICATIONS
MEDICAL HISTORY DENIES ANY/ANY OTHER SIGNIFICANT MEDICAL PROBLEMS
EP GENERAL INF01~IATIOR ARRIVED AT EP VIA PRIVATE VEHICLE ACCOtPANIED TO EP BY NO ONE CONSENT FOR TREAMENT GIVEN BY SELF LEVEL OF CONSCIOUSNESS . . . . AWAKE. ALERT, oRIENTED X3 SKIN WARM, DRY. COLOR NORMAL
CHIEF COMPLAINT DETAIL ONSET OF PAIN: YESTERDAY PT C/O CONSTANT PAIN UOCATION OF RAIN: LTLRT CHEST NO RADIATION OF P~IN PAIN LEVEL: 0 0 / I 0 " ~ - . ~ AGGRAVATING FACTORS: ~ONE ALLEVIATING FACTOR~rNONE DIAPHORESIS: YES NO OTHER COMPLAINTS OR ASSOCIATED SYMPTOMS RECENT CHEST TRAUMA: NO PT STATES HAS BEEN HAVING PAIN SINCE YESTERDAY. INTERMITTENT. SOMETIMES LEFT SIDE OF CHEST. SOMETIMES RIGHT, STATES IT RADIATES THROUGH TO BACK. PAIN FREE AT PRESENT, DENIES NAUSEA OR SOB; CLEAR BILAT BREATH SOUNDS, NORMAL EVEN AND UNLABORED RESPIRATIONS: SINUS RHYTHM PER MONITOR WITHOUT ECTOPY
STANDAi~ OF CARE STANDARD OF CARE: ALTERATION IN COMFORT/PAIN
PATI ~IT CLASSIFICATION URGENT
Figure 7
Final copy w i t h ca tegor ie s for e a se of reading.
334 Volume 23, N u m b e r 4

Mason, Gibson, and Sanders/JOURNAL OF EMERGENCY NURSING
INTERRUPT TRIAGE
~TO BE RESUMED Wl SECONDARY TRIAGE
xUNABLE TO CONTINUE W/ TRIAGE DUE TO PT'S ACUITY LEVEL
CONTINUE TRIAGE
PT LEVEL OF CONSCIOUSNESS
xADULT/CHI LD
I N FANT
Figure 8 The screens have the adaptabil i ty to continue assessment if an interruption for care has occurred.
an i s sue b e c a u s e the s c r eens are mos t ly p r o d u c e d b y a m e n u se lec t ion m a d e wi th t he mouse . There is also a type - in s c r een avai lable for add i t iona l informat ion at the end of e a c h a s s e s s m e n t .
T h e m o s t d i f f i cu l t h u r d l e to o v e r c o m e w a s a b a s i c f e a r of c o m p u t e r s .
Initially t he c o m p u t e r s y s t e m u s e d a l ight p e n to se lec t a s s e s s m e n t f indings. B e c a u s e of t he conf iden- t ia l i ty of pa t i en t information, p r ivacy s c r eens we re p l aced on each c o m p u t e r monitor. This m a d e the l ight pen nonfunct ional , so a m o u s e s y s t e m w a s imp lemen ted . This skill p roved difficult for s o m e nurs - ing staff m e m b e r s bu t the i r skills i m p r o v e d after abou t a month .
We con t inue to e n h a n c e the c o m p u t e r t r i age sys- tem. Our . commi t t ee d e v e l o p e d a un ive rsa l d a t a sheet . This informat ion o b t a i n e d allergies, p a s t m e d - ical history, s u b s t a n c e allergies, and food a l lergies tha t can b e fo rwarded wi th t he a d m i t t e d p a t i e n t s to
d e c r e a s e dup l i ca t ion efforts of the i npa t i en t nurse . The e m e r g e n c y d e p a r t m e n t has further a d v a n c e d i n f o r m a t i o n to i n c l u d e p r e s e n t m e d i c a t i o n s t h e p a t i e n t is taking, dosage , f requency, and las t dose t aken b y the pa t ien t . This informat ion follows the p a t i e n t s to the nu r s ing uni ts . B e c a u s e of an u p g r a d e in our cl inical sys t em, th is in format ion a p p e a r s on the app rop r i a t e t r i age s c r e e ns a n d n o w m u s t be upg rad - ed or r e p l a c e d only a t s u b s e q u e n t visi ts . The nu r s ing staff n o w has t he abi l i ty to pr in t a ha rd copy for p a t i e n t s to carry wi th t h e m to d e c r e a s e t ime s p e n t g iv ing information. This also p roved to i n c r e a s e effi- c i ency of bo th t r i age and the i npa t i en t a s s e s s m e n t and history.
E a c h nurse and a d m i t t i n g clerk has t he capabi l i - ty of v i e w i n g the avai labi l i ty of b e d s in the depa r t - m e n t and the loca t ion of spec i f ic p a t i e n t s to a s s i s t v is i tors and other family m e m b e r s w i thou t phys ica l ly wa lk ing to a p a t i e n t care area.
By con t inu ing to c h a n g e the a s s e s s m e n t accord - ing to our needs , t he nu r s ing staff in the t r i age a rea n o w are able to perform an a d v a n c e d a s s e s s m e n t . As n e w ideas are s u g g e s t e d by the staff, c h a n g e s are m a d e eas i ly b y the Informat ion M a n a g e m e n t Depar tmen t .
Fu tu re goals for our d e p a r t m e n t inc lude c ompu t - er iz ing the e m e r g e n c y logbook, c o m p u t e r i z i n g the care r e n d e r e d for a spec i f ic s y m p t o m , and eventua l ly b e c o m i n g a p a p e r l e s s d e p a r t m e n t . The c o m p u t e r s y s t e m has m a d e r e a d i n g a n d ob t a in ing the init ial a s s e s s m e n t bo th s t a n d a r d i z e d and efficient. With the c o n t i n u u m of ca re go ing ac ross hosp i ta l walls, the informat ion o b t a i n e d on e m e r g e n c y p a t i e n t s is n o w avai lable to ca reg ive rs in all a reas of the hosp i ta l i n c l u d i n g p r iva te p h y s i c i a n s . The t r i age p r o c e s s al lows for the p a t i e n t w i th mul t ip le symptoms . The p roc e s s con t inues as hea l th care c h a n g e s and the informat ion n e e d e d from p a t i e n t s also changes . This p roces s has b e e n success fu l for our d e p a r t m e n t . We n o w c h a n g e the p roc e s s as our n e e d s c h a n g e i n s t e a d of p u r c h a s i n g an u p g r a d e or n e w software.
We wish to give special thanks to Mary Jane Brown, MD, staff physician, Baptist Hospital, and Sandy Pomerantz, RN, clinical systems manager, Management Information Sys- tems, Baptist Hospital, Nashville, Tennessee.
August 1997 335


















