Computerized axial tomography: the normal EMI scan · J. Gawler,J. W. D. Bull, G. H. duBoulay,...
13
Journal of Neurology, Neurosurgery, and Psychiatry, 1975, 38, 935-947 Computerized axial tomography: the normal EMI scan J. GAWLER, J. W. D. BULL, G. H. DU BOULAY, AND J. MARSHALL From the National Hospital for Nervous Diseases, Queen Square, London SYNOPSIS Computerized axial tomography using the EMI Scanner s a new method of using x-rays in diagnosis. The technique displays intracranial and orbital structures in the transverse plane. The appearances of normal EMI Scans are described and correlated with cerebral and orbital anatomy seen in transverse section. Computerized transverse axial tomography with the EMI Scanner-a revolutionary method of utilizing x-rays in diagnosis developed by G. N. Hounsfield-provides images of transverse 'slices' of the brain without the use of contrast media. Normal structures, such as the internal capsule, which could not be shown by conven- tional techniques, and structures, such as the ventricular system, which could be seen only with the aid of contrast media, may now be displayed without prior disturbance. The present paper describes the normal intra- cranial anatomy as revealed by the EMI Scan. As normal volunteers have not been examined, the composite picture described here has been built from experience with 2 500 patients investi- gated for intracranial disease, in some of whom the EMI Scan and other investigations proved negative. Full descriptions of the scanning technique have been published elsewhere (Houns- field, 1973) and only relevant features will be considered here. Each transverse 'slice' of brain is considered as a matrix of cells. Initially, an 80 by 80 matrix containing 6 400 cells each 3 mm by 3 mm was used, but currently a 160 by 160 matrix of 25 600 cells measuring 1.5 mm by 1.5 mm is employed. The depth of each cell is 8 or 13 mm depending upon the adjustable width of the x-ray beam. The image of the brain is constructed from measurements of the amount of x-ray absorbed by each of the cells as the x-ray beam scans the head. The absorption values are expressed on an arbitrary scale where air has a (Accepted 23 May 1975.) 9: + 500 -J cU CO, 100- 50- c- C,) z LL a / 100 ADJUST WINDOW WIDTH -500 - FIG. 1 Oscilloscope display represented graphically. The ten divisions (peak black, peak white and eight shades of grey) may be applied to the entire density range used by the EMI system or restricted to any segment of the range. 35 0 0 z 3: -J -J c1 C' a \/ Protected by copyright. on April 13, 2021 by guest. http://jnnp.bmj.com/ J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.38.10.935 on 1 October 1975. Downloaded from
Transcript of Computerized axial tomography: the normal EMI scan · J. Gawler,J. W. D. Bull, G. H. duBoulay,...

Journal of Neurology, Neurosurgery, and Psychiatry, 1975, 38, 935-947
Computerized axial tomography: the normal EMI scan
J. GAWLER, J. W. D. BULL, G. H. DU BOULAY, AND J. MARSHALL
From the National Hospital for Nervous Diseases, Queen Square, London
SYNOPSIS Computerized axial tomography using the EMI Scanner s a new method of usingx-rays in diagnosis. The technique displays intracranial and orbital structures in the transverse plane.The appearances of normal EMI Scans are described and correlated with cerebral and orbitalanatomy seen in transverse section.
Computerized transverse axial tomography withthe EMI Scanner-a revolutionary method ofutilizing x-rays in diagnosis developed by G. N.Hounsfield-provides images of transverse'slices' of the brain without the use of contrastmedia. Normal structures, such as the internalcapsule, which could not be shown by conven-tional techniques, and structures, such as theventricular system, which could be seen onlywith the aid of contrast media, may now bedisplayed without prior disturbance.The present paper describes the normal intra-
cranial anatomy as revealed by the EMI Scan.As normal volunteers have not been examined,the composite picture described here has beenbuilt from experience with 2 500 patients investi-gated for intracranial disease, in some of whomthe EMI Scan and other investigations provednegative. Full descriptions of the scanningtechnique have been published elsewhere (Houns-field, 1973) and only relevant features will beconsidered here.Each transverse 'slice' of brain is considered
as a matrix of cells. Initially, an 80 by 80 matrixcontaining 6 400 cells each 3 mm by 3 mm wasused, but currently a 160 by 160 matrix of25 600 cells measuring 1.5 mm by 1.5 mm isemployed. The depth of each cell is 8 or 13 mmdepending upon the adjustable width of thex-ray beam. The image of the brain is constructedfrom measurements of the amount of x-rayabsorbed by each of the cells as the x-ray beamscans the head. The absorption values areexpressed on an arbitrary scale where air has a
(Accepted 23 May 1975.)9:
+ 500
-J
cUCO,
100-
50-
c-C,)zLLa
/
100
ADJUST WINDOWWIDTH
-500 -
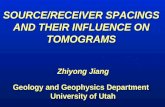
FIG. 1 Oscilloscope display represented graphically.The ten divisions (peak black, peak white and eightshades of grey) may be applied to the entire densityrange used by the EMI system or restricted to any
segment of the range.35
00z3:
-J
-Jc1C'
a
\/
Protected by copyright.
on April 13, 2021 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.38.10.935 on 1 October 1975. D
ownloaded from

J. Gawler, J. W. D. Bull, G. H. du Boulay, and J. Marshall
FIG. 2 Paired transverse axial tomograms, each 13mm deep, are centred at regular intervals above theorbitomeatal line to cover the supratentorial compart-ment.
value of -500, water has zero value, and densebone a mean value of + 500. Cerebrospinal fluidgives values of 0 or 1, white matter 10 to 18, andgrey matter 18 to 30. Calcified structures suchas the pineal body or choroid plexus give highervalues.The absorption values may be expressed
numerically by a line printer or displayed as an
image by a cathode ray oscilloscope whoseadjustable grey scale has 10 divisions from peak
FIG. 3 Tomograms are centred specifically forposterior fossa and orbital examination.
black (low density) to peak white (high density).The scale can be adjusted to cover the entiredensity range (-500 to + 500) or a segmentfrom any part of the range (Fig. 1). Absorptionvalues are calculated to an accuracy better thanhalf per cent so that on the arbitrary scale adifference of4 or 5 points is significant. When theoscilloscope scale covers 0 to 40 of the densityrange, each change in the grey scale represents4 points of density difference permitting cerebro-spinal fluid, grey and white matter to bedistinguished.For examination of supratentorial structures
a series of four scans yielding eight 13 mm tomo-grams is employed. The tomogram pairs arecentred 3, 5.5, 8, and 10 cm above and parallelto the orbitomeatal line (Fig. 2). For posteriorfossa examination the beam is centred 3 or3.5 cm above the orbitomeatal line, with thepatient's head flexed 15 or 20 degrees, and forthe orbits a pair of 8 mm 'slices' centred 1 or1.5 cm above the orbitomeatal line with thehead extended 10 to 15 degrees are employed(Fig. 3).
ANATOMY DEFINED BY THE EMI SCAN
Intracranial compartment (Fig. 4)
Because the size and shape of the skull varies fromperson to person a 'slice' at a given level above theorbitomeatal line will contain different structures indifferent patients. For this reason, a series ofidealized 'slices' will not be described and, instead,the appearance and relationship of normal structuresin the transverse plane as revealed by computerizedtomography will be considered.
VENTRICULAR SYSTEM The lateral ventricles are seenin three or four contiguous 'slices' (Fig. 5). Con-sidered from above downwards the highest 'slice'may incorporate only 1 or 2 mm of each lateralventricle, which then appear as bilateral vague areasof slightly lower density (Fig. 6a). With slightobliquity of the head, one ventricle may just presentwithin the 'slice', while the other lies below it. Thiscan lead to the mistaken interpretation that a patho-logical diminution of white matter density exists inthe centrum semiovale on this side (Fig. 6b). Itmust be remembered that as a 'slice' is 13 mm deepit may incorporate both cerebrospinal fluid andbrain tissue with absorption values varying between1 and 10 (Fig. 7). The precise limits of the ventriclescannot therefore be defined. In practice, this is not a
936
Protected by copyright.
on April 13, 2021 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.38.10.935 on 1 October 1975. D
ownloaded from

Computerized axial tomography: the normal EMI scan
I semiovOle
*S
kt..-:X<s t. k...
..t { ,K, 18-#4 s R S.s ..a ^ w N
.9.s ._... , *e ..s . .l X . .P ^ / \ -ro X, ii_- .4, /
< _*.
:\' s ' j a:,.
*"B;S ffi
(1(1. 4 1
F-niC. 4 2
FIG. 4 Normal EMI Scan. Three scan pairs centred 3 (4/5 and 6), 5.5 (4/3 and 4), and 8 (4/1 and 2) cmabove the orbitomeatal line provide a sequence of six contiguous tomograms. A normal brain (left) has beencut at appropriate levels to match the scan and the diagram (right) shows those structures which may beidentified on the scan. When comparing the cut surface of the brain and EMI Scan, it is important toremember the latter represents all the tissues in a 'slice' 13 mm thick. (See over.)
problem because, when the absorption values arecontrasted on the oscilloscope, fairly sharp definitionof the ventricles is obtained. When the ventricularmargin lies within cells that contain principallycerebral tissues, a significant reduction in densitymay not be apparent and the ventricles would thusappear smaller than their true dimensions. Con-versely, when a cell contains sufficient fluid to reduce
its density, the whole cell is registered as ventricle,even though only a segment of the ventricle isprojected into the cell, and this would make theventricle appear larger than its real size. Overall, thetechnique makes the ventricles appear slightlysmaller than in a fixed specimen of a normal brain,and this is allowed for in the interpretation.The highest tomogram to pass clearly through the
937
Protected by copyright.
on April 13, 2021 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.38.10.935 on 1 October 1975. D
ownloaded from

J. Gawler, J. W. D. Bull, G. H. du Boulay, and J. Marshall
0iy;h _ W _ ,S / \\N Sephurn pe'!LIcdLFront' h.
Q. Cu
orda
.ffi.*:11! ^-- L _ _- : r' t e r ,t ti C a p s u-~~~~~~~~~~~it r riPs l,;
AInt.rior a.imt
Posta--IC.r -~
.. r .} /, I / 'd _ ____ pOsts-SclF'm-'~~~~Ari~ rd
t= X ffi . . . I s s / + ~~~~~~~p qJjA5Z>---6Xi3 : #X .^ *< 4 t Q ) _ - ¢ @ ~~~~~~~~~~~~~~T h c r,: -
T1111-XiilEX11 il e w t~~~~~~~~~~~~~~~~~~~~~~~~~~~~~I'- r C.4.
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~ine rn a __,..[Icap u 'c'
.~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~i 'C.-,J
c-dU n
CzzL-.......... ., . .... ! , w
l__ As-.-._,Sff~~~~~~~~~~~~~~~~b
lateral ventricles contains the superior segments ofthe cellae mediae (Fig. 4/2). While these are fairlysymmetrically displayed with respect to the midline,they commonly show some difference in size andcontour. The body of the corpus callosum liesbetween the cellae mediae on this plane, with theforceps minor diverging anteriorly and the forcepsmajor posteriorly along the medial aspects of theventricles. Laterally lies the white matter of thecorona radiata. The superior segments ofthe trigonesand occipital horns may also be incorporated intothis tomogram. Marked asymmetry of the occipitalhorns is common and not infrequently one or bothcontain insufficient cerebrospinal fluid for their cleardelineation on the scan. A thin occipital horn may
appear as a vague area of low density extendingbackward towards the occipital pole and should notbe mistaken for a lesion. The next contiguoustomogram, descending through the series, incor-porates the frontal horns anteriorly and the trigonesand occipital horns posteriorly (Fig. 4/3). A degree ofasymmetry in lateral ventricular contour is common,partly because of true anatomical difference andpartly because any obliquity of the head will resultin slightly different ventricular segments beingincorporated on the two sides. Between the frontalhorns, the septum pellucidum can be regularlyidentified on the 160 by 160 matrix but not alwayson the 80 by 80 matrix. At the posterior end of theseptum the anterior columns of the fornix can be
938
H;(. 4+
Protected by copyright.
on April 13, 2021 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.38.10.935 on 1 October 1975. D
ownloaded from

Computerized axial tomography: the normal EMI scan
I Itio. 4-5.
i...
46
seen in the midline bulging into the posterior seg-ments of the frontal horns. The site of the foraminaof Monro is thus marked, for they open into thelateral ventricles posterolateral to the columns of thefornix. Immediately lateral to the frontal horns liethe heads of the caudate nuclei which are generallyidentifiable as discrete structures. The trigones arewell shown at this level, although their margins arenot always crisply defined. Often they have asomewhat triangular appearance, with the baselaterally and the apex directed anteromedially. Theposterior angle of the triangle may continueposteriorly as the occipital horn. The apex of thetriangle continues medially towards a group ofcerebrospinal fluid filled spaces which lie in themidline at this level. These represent a complex ofsubarachnoid cisterns and the posterosuperior
segment of the third ventricle (Fig. 8). The pinealbody lies at the centre of this fluid-containing area,the anatomy of which will be considered in detaillater. The thin fluid-containing zone between thetrigone and the midline complex of cisterns is thelateral wing of the ambient cistern which runs outinto the choroid fissure behind the pulvinar of thethalamus (Fig. 4/3). The lateral ambient wing isseparated from the ventricle by the choroid plexuswhich can often be seen projecting into the trigone.The choroid plexus is frequently identified by thecalcium it often contains. Anteromedial to thetrigone lies the pulvinar ofthe thalamus identifiable inits own right. The tail of the caudate nucleus lies atthe anterolateral extremity of the trigone but is notseen as a discrete structure. The optic radiationsweeps laterally around the trigone, and is recogni-
939P
rotected by copyright. on A
pril 13, 2021 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.38.10.935 on 1 O
ctober 1975. Dow
nloaded from

J. Gawler, J. W. D. Bull, G. H. du Boulay, and J. Marshall
zable as a band of white matter density extendingbackward from the posterior limb of the internalcapsule.The lowest tomogram incorporating the lateral
ventricles usually shows only the inferior segments ofthe frontal horns (Fig. 4/4). The temporal hornscannot be identified with certainty, although theirposition can be gauged from related structures. Attheir predicted site, it is possible to find a vague areawhere the density is slightly less than the surroundingbrain substance. In our experience, clear delineationof the temporal horns implies that they are dilated.The third ventricle usually lies within the compass
of two contiguous tomograms (Fig. 4/3 and 4). Onthe higher its posterosuperior segment is seen ex-tending anteriorly from the pineal region, where itforms the anterior angle of a diamond-shaped,midline, fluid-containing area surrounding thepineal body. The latter is nearly always identified,even when it contains insufficient calcium to bevisible on a conventional radiograph. The posteriorangle of the diamond-shaped space represents thecistern of the Great vein of Galen, while the lateralangles are formed by the wings of the ambientcisterns. The third ventricle may be considered asthat part of the fluid-containing area anterior to thepineal body. The superior margin of the third
FIG. 5 The ventricular system in relation to trans-verse axial tomography.
ventricle and its suprapineal recess cannot bedefined for they are superimposed on the crura of thefornices anteriorly and the splenium of the corpuscallosum posteriorly. What is seen of the postero-superior part of the third ventricle tapers rapidly as itextends forward from the pineal region and it maydisappear anteriorly, being lost by its incorporationwith the massa intermedia. The anterosuperior
FIG. 6 (a) The tomogram has grazed the superior aspects of the lateral ventricles which canonly just be identified. (b) Slight obliquity of the head causing only the superior aspect of onelateral ventricle (the right) to lie within the tomogram.
940P
rotected by copyright. on A
pril 13, 2021 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.38.10.935 on 1 O
ctober 1975. Dow
nloaded from

Computerized axial tomography: the normal EMI scan
80X80C ELLS
FIG. 7 Because each tomo-gram is 13 mm deep theventricular margin appearsas a numerical gradientbetween cells containingonly cerebrospinal fluid andthose containing only braintissue.
10 98 7 4 20 0 0 7 0 3 6 9 11CELL ABSORPTION VALUES
segment of the third ventricle may be apparentimmediately behind the anterior pillars of the forniceswhich, as noted previously, allow the foramina ofMonro to be located. The thalami, identifiable bytheir density, form the lateral relations of the thirdventricle throughout its anteroposterior course. Thelower tomogram containing the third ventricleusually shows the anteroposterior extent moreclearly, from the columns of the fornices anteriorlyback to the upper midbrain posteriorly where itbecomes continuous with the aqueduct. This lowertomogram may also contain the suprasellar cisternsand the superimposition of cerebrospinal fluid-containing spaces prevents clear definition of theanteroinferior recesses of the third ventricle. Theaqueduct, because of its small diameter and obliquecourse in the plane of the tomogram, cannot beresolve clearly. A slight diminution in density cansometimes be measured in the midbrain at a sitewhich would correspond with the aqueduct, but inpractice this structure must be regarded as invisibleon the scan unless it is enlarged.The normal fourth ventricle can always be seen on
the appropriate tomograms (Fig. 4/5 and 6) but itsshape varies slightly with different angulation of thehead in the plane of the tomogram. When the tomo-gram series lie parallel to the orbitomeatal line, thelowest of the stack usually incorporates the uppersegment of the fourth ventricle and it appears as anoval area of low density at the centre of the posteriorfossa. The bony orbital roof is likely to be includedon a tomogram at this angle and can cause artefactualstreaking on the scan which impairs resolution of theposterior fossa. For clear display of the fourthventricle, it is necessary to flex the head by 10 to 20degrees with respect to the orbitomeatal line. Thisprojects the posterior fossa upward into the tomo-gram while the orbital roof is projected below it. Apair of scans taken with this angulation will displaythe entire fourth ventricle, its lower segment on the
CistrernnCollosol c. _
C. Lqmina }terminolis
Chaosmotic c
Cisternsb IT
cerebellarC of the Greotvein of Golen
Ouodriqeminol c.
Interpeduncular c.
Pontine c.
Medullory c
FIG. 8 Diagram to illustrate the relationshlip ofsubarachnoid cisterns to the third ventricle.
inferior and its upper segment on the superior tomo-gram. This head position may also make the postero-superior recesses of the ventricle more obvious and sochanges its contour on the scan (Fig. 9). An outlineof the pons is obtained from the pontine cisternanteriorly, the cerebellopontine angle cisternslaterally, and the fourth ventricle posteriorly. Themiddle cerebellar peduncles turn back from the ponsto flank the lateral aspects of the fourth ventricle andthe vermis can be resolved as a grey matter bandextending in the midline from the posterior limit ofthe ventricle towards the occipital bone.
SUBARACHNOID CISTERNS Cisterns are visible becausethey contain fluid but their margins may be lost ifthey are superimposed on a segment of the ventricularsystem. Cisterns adjacent to the skull base will not bevisible if a tomogram includes the bone beneaththem. A thin low density line, one cell deep, can oftenbe recognized on the scan immediately beneath theskull vault. This rim within the skull is a by-productof the mathematical method used to reconstruct theimage and does not represent fluid in the sub-
941
I
Protected by copyright.
on April 13, 2021 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.38.10.935 on 1 October 1975. D
ownloaded from

J. Gawler, J. W. D. Bull, G. H, du Boulay, and J. Marshall
FIG. 9 Scan pair 6A/B (top) are parallel to the orbitomeatal line and the fourth ventricle is seen only on thelower tomogram. Scan pair 9A/B (bottom) are taken with the head flexed 15° with respect to the orbito-meatal line and the fourth ventricle is now visible on both tomograms. The appearance of the fourth ventriclediffers slightly with these two projections.
arachnoid space over the cerebral hemispheres. Thesubarachnoid spaces cannot normally be defined overthe convexity on an 80 by 80 scan, but on the 160by 160 matrix image cortical sulci can sometimes beseen on the higher tomograms as fine low densitylinear markings extending inward from the surface.(Fig. 4/1). Deepening of the subarachnoid space orwidening of the sulci is readily apparent when
cerebral atrophy is present and atrophy also improvesthe definition of the subarachnoid cisterns.The cisterna magna can be seen only when its
vertical extent is sufficient for the superior segmentto be incorporated into a tomogram passing clear ofthe skull base. The lower segment of the cistern andthe vallecula cannot be shown, for they lie too closeto the bony floor of the posterior fossa in the region
942P
rotected by copyright. on A
pril 13, 2021 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.38.10.935 on 1 O
ctober 1975. Dow
nloaded from

Computerized axial tomography: the normal EMI scan
of the foramen magnum. The superior segment ofthe cistern, usually seen only when the head isexamined in the flexed position, appears as a midlinearea of fluid density immediately subjacent to theskull posteriorly. Its depth is generally greatest in themidline where the cerebellar vermis lies anterior to it.Laterally, the cistern tapers as it caps the posterioraspects of the cerebellar hemispheres and its lateralextent is often different on the two sides. Themedullary cistern and its lateral recesses are tooclosely related to the skull base to be shown but thepontine and cerebellopontine-angle cisterns canbe seen. The pontine cistern appears as a narrowzone of fluid density immediately behind the clivusand it extends laterally and posteriorly on each sideto encircle, and so demarcate, the anterior border ofthe pons. The cisterns continue further laterally oneach side, behind the inner ends of the petrous ridges,to become the cerebellopontine-angle cisterns (Fig.4/6). The apparent depth of these cisterns and theclarity with which they are shown depends in partupon the angulation of the head. When the clivus isalmost vertical to the plane of the tomogram thecisterns are well shown (those cells which lie behindthe clivus and petrous ridges will contain chieflycerebrospinal fluid). When the clivus has a moreparallel course with respect to the beam, the cisternsare likely to be obscured by superimposition of theclivus anteriorly and the brain stem posteriorly. Anyhead movement during scanning is likely to causeartefactual streaking backward from the clivus andpetrous bones into the posterior fossa so maskingthese cisterns. Even without head movement, anartefactual low density streak often extends betweenthe tips of the petrous ridges and obscures theanterior border of the pons. The prepontine cisternis continuous anterosuperiorly with the interpedun-cular and crural cisterns. When sharply delineated,these cisterns outline the anterior border of the mid-brain and display the cerebral peduncles. Anteriorly,the cisterns encircling the anterior midbrain arecontinuous with the chiasmatic cistern, whichappears as a median area of fluid density above thesella (Fig. 4/5). The anterior clinoid processes,tuberculum, and dorsum sellae are often projectedinto this low density zone from below, while theanteroinferior segment of the third ventricle is pro-jected from above. The anterior limit of the supra-sellar cisterns may give rise to a midline band of fluiddensity representing the interhemispheric fissurebetween the frontal lobes, while its anterolateralcorners continue into the lateral fissures as theyextend forward and laterally towards the pteryon. Itis possible to identify the circular (insular) cisterns onsome normal scans as semilunar zones of fluiddensity, concave medially, which lie parallel and
deep to the surface of the hemisphere overlying theisland of Reil (Fig. 4/4). Widening of the lateral andinterhemispheric fissures together with prominenceof the insular cisterns occurs in cerebral atrophy.The posterior aspect of the midbrain is capped by
the quadrigeminal cistern, which can be regularlyidentified on both the 80 by 80 and 160 by 160 matrixscans (Fig. 4/4). It provides a landmark on the scansdefining not only the midbrain but also the level ofthe tentorial hiatus. The lateral extremities of thequadrigeminal cistern extend anterolaterally aroundthe midbrain to become continuous with the cruralcisterns. The lateral conduits are termed the ambientcisterns and it is often possible to demonstrate theentire midbrain from its encircling cisterns. Thequadrigeminal cistern continues upward over thesuperior colliculus into the cistern of the great veinof Galen, which, as was noted previously lies im-mediately behind the posterosuperior aspect of thethird ventricle (Fig. 4/3). The lateral extremities ofthe Galenic cistern are prolonged behind thepulvinar of the thalamus as the lateral wings of theambient cistern. Posteriorly, the Galenic cistern iscontinuous with the subarachnoid space beneath thetentorium and overlying the superior vermis. This isthe superior cerebellar cistern. On a normal scan, itis possible to detect fine semilunar zones of reduceddensity radiating anterolaterally into each cerebellarhemisphere from the superior cerebellar cistern.These linear areas represent fluid present in thespaces between cerebellar folia. While the superiorcerebellar cistern is variable in size, widening of thespaces between the folia indicates cerebellaratrophy.
CEREBRAL HEMISPHERES Because computerizedtomography can detect the slight measurable dif-ference in x-ray absorption between grey (absorptionvalue 18-30) and white matter (11-18), certaincerebral structures may be identified in their ownright. The density difference between grey and whitematter almost certainly depends upon several factors.First, grey matter is the more vascular and the densityof unclotted blood is relatively high (absorptionvalues 13-31; Scott et al. (1974). Second, the accumu-lation of high atomic number substances, like iron,will affect the grey matter preferentially and third,white matter contains more lipid material (myelinsheaths) than grey.
Further definition of certain cerebral structurescan be gained from the outline provided by theventricular system or subarachnoid cisterns.The cortical grey matter mantle is recognizable
over the surface of the cerebral hemispheres not onlysubjacent to the skull but also as a midline band inrelation to the interhemispheric fissure (Fig. 4/1).
943
Protected by copyright.
on April 13, 2021 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.38.10.935 on 1 October 1975. D
ownloaded from

J. Gawler, J. W. D. Bull, G. H. du Boulay, and J. Marshall
FIG. 10 Scan pairs 2A/B (top) before, 3A/B (bottom) after the injection of 100 ml sodium iothalamate(Conray 420) intravenously, to demonstrate normal enhancement of tissue density.
The distinction between cortical mantle and under-lying white matter is least obvious in infants and thedensity difference tends to become more obviouswith advancing age. These changes may reflect theincreasing degree of myelination in infancy and theaccumulation of high atomic number substanceswith ageing. Further, the total accumulation ofcalcium in the vasculature might be expected toaffect the grey matter more obviously. Converselywith increasing age, the enlargement of those sulciwhich are not defined as discrete structures might be
expected to lower the density of the cortical mantleby their contained cerebrospinal fluid. On tomogramsincorporating the insula, it is possible to recognizea vague area of grey matter density extending inwardfrom the cortical mantle to lie along the margins ofthe circular cistern.The heads of the caudate nuclei are regularly seen
as oval zones of grey matter density immediatelylateral to the frontal horns (Fig. 4/3). Asymmetry ofthese nuclei is commonly seen and presumablyrepresents their differential incorporation; a result of
944
Protected by copyright.
on April 13, 2021 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.38.10.935 on 1 October 1975. D
ownloaded from

Computerized axial tomography: the normal EMI scan
slight obliquity of the tomogram. The thalami arerecognizable in the majority of patients, their medialmargins can be gauged from the third ventricle forthey extend along it from the foramina of Monroto its posterior extremity. The posterior aspect of thepulvinar is outlined by the trigone and wing of theambient cistern. The lateral thalamic margins aredefined by the posterior limbs of the internal capsules.The putamen and globus pallidus (lentiform
nuclei) are not as well defined as the foregoing deepnuclei and they merge laterally with the grey matterof the insula. It is always possible to locate theinternal capsule as a band of white matter densitylying between the head of the caudate and lentiformnucleus anteriorly and the thalamus and lentiformnucleus posteriorly. The posterior limb is generallyrather better demarcated than the anterior. Theposterior limb of the internal capsule is prolongedbackward as the optic radiation, while the anteriorlimb continues forward as the frontal radiation. Thegeneral course of both these large white tracts canbe discerned. Oedema associated with cerebraltumours or abscesses tends to follow white matterpathways and widening of the internal capsule cansometimes be seen. The external capsule, which isnot normally visible, may be highlighted in this way.
Scans taken after the intravenous injection of aniodine-containing contrast medium (Fig. 10) enablethe larger intracranial blood vessels to be seen. Theanterior cerebral arteries cause enhancement intissue density at the posterior end of the interhemis-pheric fissure anterior to the septum pellucidum. Themiddle cerebral artery trunks may be identified in the
lateral fissures and their branches cause enhancementin the insular cistern. Occasionally, the posteriorcerebral arteries are seen as ring-like, enhanced zonesaround the brain stem. The choroid plexus of thethird and lateral ventricles may be identified by theirenhancement following intravenous contrast, andenhancement along the interhemispheric fissure abovethe lateral ventricles reflects the vessels in relation tothe falx. Constant enhancement of the great vein ofGalen, inferior sagittal, and straight sinuses allowsthese structures to be defined. Some overall increasein tissue density in the cortical grey mantle, basalganglia, and thalamus follows large intravenousiodine injections and may allow clearer delineation ofthese structures.
CEREBELLUM AND BRAIN-STEM It is possible to definewithin each cerebellar hemisphere a zone of whitematter density which corresponds with the corpusmedullare and the cerebellar cortex and vermis aredetected by their higher density (Fig. 4/5). The site ofthe middle cerebellar penduncles is given by thepontine, cerebellopontine angle cisterns, and thefourth ventricle. The brain-stem itself is delineatedby its encircling subarachnoid cisterns and themidbrain is often sufficiently well encompassed toshow the cerebral peduncles and collicular plate. Theupper pons is similarly displayed by its anteriorcisterns but the lower pons and medulla are generallyobscured by their proximity to the skull base. Noneof the brain-stem nuclei can be seen in their ownright but the position of the larger nuclei may be
FIG. 1 1 Normal EM! Scan of orbits.
945
Protected by copyright.
on April 13, 2021 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.38.10.935 on 1 October 1975. D
ownloaded from

J. Gawler, J. W. D. Bull, G. H. du Boulay, and J. Marshall
anticipated from the brain-stem contour at a givenlevel.
Orbital compartment(Fig. 11)
With careful positioning of the head, it is possible toobtain a pair of contiguous tomograms each 8 mmdeep, through the orbits which pass clear of theirsuperior and inferior bony margins. It is importantto avoid incorporating either the roof or floor of theorbit into these tomograms, since their bony densitywill obscure adjacent structures. Seen in transversesection, the orbits lie on either side of the nasal andparanasal cavities. The bony medial and lateralorbital walls mark out a triangular space with theglobe anteriorly at its base. The retrobulbar space isfilled chiefly by fat whose very low absorption values(-10 to -70) provide a natural contrast againstwhich the optic nerves and some extraocular musclesare contrasted.The globe, seen in transverse section, appears as a
ring whose absorption values fall between 5 and 25surrounding the less dense vitreous whose values arebetween -15 and + 5. The high peripheral density isproduced by the sclera and its attached musculature.Within the ring, on the 160 by 160 matrix, the lenscan be identified anteriorly, for it is more dense thanthe vitreous. When the tomogram incorporateseither the inferior or superior pole of the globe,rather than passing through its equator, the ring-likeappearance is replaced by a sphere of even density.Any obliquity of the head will result in the beampassing through the eyes at different levels and thismay result in one eye appearing larger than theother. The apparently larger eye will project furtherforward and an erroneous impression of proptosiscan be given.The optic nerve can always be seen extending
forward and laterally from the orbital apex to theglobe. While the optic nerve is always identifiable onthe 80 by 80 matrix scan, its delineation is greatlyimproved by the high resolution system. With the160 by 160 matrix system, it is also possible to definethe medial and lateral rectus muscles in the majorityof patients and the other extraocular muscles areoccasionally seen. The extraocular muscles are notshown by the 80 by 80 matrix and as yet other intra-ocular nerves are not resolved by either matrix.
DISCUSSION
Computerized tomography produces an imagewhich cannot be thought of in quite the sameway as a radiograph. The result is a mathematicalreconstruction of a 'slice' of the patient's head
in terms of its density, and it is therefore possibleto have areas of abnormal density on the imagewhich are not due to abnormal tissue but to somefault in the mathematical reconstruction. Sucherrors may occur when the patient's head movesduring scanning, when certain faults in theapparatus occur, and also when the tomogramincludes marked density changes sequentiallythroughout the 'slice'. The latter situationobtains in the region of the skull base when asequence of bone and brain are present. Theabnormal areas that result can nearly always berecognized as artefacts and with experience theyrarely lead to diagnostic confusion.The anatomy of the brain as seen in the trans-
verse plane is seldom considered in the inter-pretation of conventional radiographs, neurolo-gists, neurosurgeons, and radiologists beingmore familiar with lateral and anteroposteriorprojections. Because a vertical series of trans-verse tomograms is achieved by computerizedtomography, it is possible to gain a three-dimensional representation of the intracranialand orbital compartments. It must be stressedagain, however, that each tomogram representsthe superimposition of all those structures con-tained within a 'slice' of the head either 13 or8 mm in thickness. As a result of normalanatomical variation, tomograms at a given levelin different patients may have a dissimilarappearance and it is wrong to think in terms ofstandardized slices. Changing the vertical planeof a tomogram in one patient by only a fewmillimetres can strikingly change its appearance,and altering the angulation of the head may havethe same effect. These considerations are perhapsmost important when interpreting scans takenthrough the posterior fossa. When the tomogram' grazes' the skull base, the incorporation of boneeffectively masks the overlying soft tissues, anessential consideration when trying to delineatethe inferior frontal or temporal lobes, thesuprasellar cisterns, brain stem, and the inferioraspects of the cerebellar hemispheres. It isimportant to recognize that tomograms at theappropriate level will include structures on eitherside of the tentorium, and this occasionally givesrise to difficulties in siting lesions above or belowit. Any lateral obliquity of the head may causedifferent structures from the right and lefthemicrania to be incorporated in the tomogram,
946
Protected by copyright.
on April 13, 2021 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.38.10.935 on 1 October 1975. D
ownloaded from

Computerized axial tomography: the normal EMI scan
and so lead to a confusing asymmetry in itsappearance.The 160 by 160 matrix scans undoubtedly give
an image of far greater definition than the 80 by80 matrix allows. This, together with the 225°scan providing 54 000 transmission readings, hasproved especially valuable in delineating posteriorfossa and orbital structures. When outlining theperiphery of a structure, not only must the cellsize in the transverse plane be considered, butalso the depth of the cells. Thus, numericalgradients in density occur at the edges of de-finable structures which pass obliquely throughthe tomogram, and this is significant whenestimating dimensions.
Computerized tomography is perhaps themost significant advance in the use of x-rays fordiagnosis since their inception. Certainly thetechnique is already revolutionizing the investi-gative routine of patients suspected of structuralintracranial or orbital disease. It also promises to
increase our understanding of many pathologicalprocesses; their natural history and responseto treatment, without exposing patients tohazard. Images of the brain can now be obtainedduring life, without anaesthetizing the subjectand without introducing contrast media such asair which may distort the findings. A new chapterin neurology has clearly been opened.
We should like to thank Dr W. G. P. Mair for his helpin preparing the brain slices, Miss V. Fullom for herradiographic assistance, Mr A. H. Prentice and Mr J.Mills for photography and Miss S. Andrews for hersecretarial aid.
REFERENCES
Hounsfield, G. N. (1973). Computerized transverse axialscanning (tomography). Part I. Description of the system.British Journal of Radiology, 46, 1016-1022.
Scott, W. R., New, P. F. J., Davis, K. R., and Schnur, J. A.(1974). Computerized axial tomography of intracerebraland intraventricular haemorrhage. Radiology, 112, 73-80.
947
Protected by copyright.
on April 13, 2021 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.38.10.935 on 1 October 1975. D
ownloaded from