Compressed tetralogy basic course 4-10-13(1)
93
Adult Congenital Heart Disease Basic Teaching Course Tetralogy of Fallot Dr. Gary Webb Cincinnati
-
Upload
olivierfischer -
Category
Education
-
view
252 -
download
1
Transcript of Compressed tetralogy basic course 4-10-13(1)

Adult Congenital Heart Disease Basic Teaching Course
Tetralogy of Fallot
Dr. Gary Webb
Cincinnati

Adult Congenital Heart Disease Basic Teaching Course
Tetralogy of Fallot
Dr. Gary Webb
Cincinnati

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse DDx Cyanotic Congenital
Heart Disese5Ts•Tetralogy.•Transposition.•Tricuspid atresia.•Truncus arteriosus.•Total anomalous pulmonary venous drainage.
2Es•Ebstein anomaly.•Eisenmenger syndrome.

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse
Components of Tetralogy

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse Pulmonary Atresia Form of
Tetralogy

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse Associated Anomalies in
Tetralogy• Right aortic arch (25%).
• Consider 22Q11 deletion.
• Coronary artery anomalies (5%).• Left anterior descending arises from the
proximal right coronary and crosses the right ventricular outflow tract.
• Complete AV septal defect.

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse
The Essence of Tetralogy

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse Pathophysiology of
Tetralogy• The degree of cyanosis reflects the
severity of RVOT obstruction.
• Right to left shunting across the VSD.
• Unrepaired patients are prone to “spells”. These are acute drops in arterial saturation due to dynamic RVOT obstruction. The child may squat.

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse
Natural History of Tetralogy
• Hypoxia tends to progress early in life.
• Survival to adult life is rare without palliation or correction.

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse Figure 4. Palliative surgical shunts.
Bashore T M Circulation 2007;115:1933-1947
Copyright © American Heart Association

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse Physical Findings in
Repaired Tetralogy• Right ventricular lift.
• Low-pitched diastolic murmur.
• Systolic ejection murmur.
• Pansystolic murmur.
• High-pitched diastolic murmur.

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse
ECG in Repaired Tetralogy

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse
CXR in Repaired Tetralogy
DO112

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse
CXR in Repaired Tetralogy
DO112

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse Echo Findings in Repaired
Tetralogy• Moderate to severe pulmonary
regurgitation (usual).
• RVOT obstruction (unusual).
• VSD patch leak (usually small).
• RV dilation (due to the PR).
• RV systolic dysfunction (late finding).
• Significant TR (when RV failing).
• Ascending aortic dilation (15%).

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse
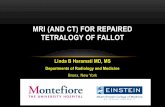
MRI in Repaired Tetralogy
• Ventricular volumes.
• Stroke volumes.
• Ejection fractions.
• Pulmonary regurgitant fraction.

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse
Davlouros 2001Davlouros 2001
Forward flow in PA
Regurgitant flow in PA

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse
MRI in Repaired Tetralogy
• Ventricular volumes.
• Stroke volumes.
• Ejection fractions.
• Pulmonary regurgitant fraction.
• Pulmonary arterial morphology.
• Aortic dilation.
• Coronary anomalies.
• Aortopulmonary collateral arteries.

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse Arrhythmias in Repaired
Tetralogy• SCD is an issue.
• SCD occurs in patients with:• Severe PR.
• Ventricular dysfunction.
• Past history of cardiac arrhythmias.
• ICDs placed for primary and secondary prevention.
• Primary prevention if SCD rate estimated at ≥ 4% per year

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse
ICDs in Repaired Tetralogy
• Primary prevention in high risk patients.• Left ventricular dysfunction.
• Inducible VT.
• QRS duration ≥ 180 msecs.

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse SCD in Congenital Heart
Defects• Repaired tetralogy.
• Mustard/Senning repairs.
• Aortic stenosis.
• Aortic coarctation.
• Eisenmenger syndrome.
• CCTGA.
• Ebstein anomaly.

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse Sustained VT in Repaired
Tetralogy• Occurs in about 14% of patients.
• Almost always in the setting of severe PR.
• Mechano-electric relationships:• Dilated right ventricle.
• Irritable right ventricle.
• Treatment needed for both the electrical and hemodynamic problems.

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse Atrial Flutter in Repaired
Tetralogy• Occurs in about 20% of patients.
• Associated with:• Severe PR.
• RV systolic dysfunction.
• Moderate-severe TR.

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse Reintervention After
Tetralogy Repair• VSD with > 1.5/1.0 shunt.
• RVOT obstruction with an RV systolic pressure > 2/3 systemic.
• Severe PR with:• Exercise intolerance;
• Sustained arrhythmias;
• Severe RV dilation.
• Severe aortic regurgitation.

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse Reintervention After
Tetralogy Repair

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse Reintervention After
Tetralogy Repair

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse Pregnancy After Tetralogy
Repair

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse Closing Remarks re
Tetralogy Repair Patients

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse
Tetralogy of Fallot
Dr. Gary Webb
Cincinnati

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse
Tetralogy of Fallot
Dr. Gary Webb
Cincinnati

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse
Nollert JACC 1997Nollert JACC 1997
Munich Tetralogy Long-Term Survival

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse
Brickner M et al. N Engl J Med 2000;342:334-342

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse
Source: http://www.nhlbi.nih.gov/health/dci/Diseases/tof/tof_what.html

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse
Tetralogy of Fallot - Apitz, Christian; Webb, Gary D; Redington, Andrew N. Lancet, 10/2009, Volume 374, Issue 9699, pp. 1462 - 1471

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse
PVR and the RV – Toronto 2
Therrien AJC 2005

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse Plot of QRS duration in 182 patients.
Gatzoulis M A et al. Circulation 1995;92:231-237
Copyright © American Heart Association

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse
From: Becker et al – Fallot’s Tetralogy A Morphometric and Geometric Study. American Journal of Cardiology, Vol 35, p. 402-412, 1974

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse
Segmental duplications: an 'expanding' role in genomic instability and disease. Beverly S. Emanuel & Tamim H. Shaikh Nature Reviews Genetics 2, 791-800 (October 2001)

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse
Park: Pediatric Cardiology for Practitioners, 4th ed., Copyright © 2002 Mosby, Inc..

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse
Park: Pediatric Cardiology for Practitioners, 4th ed., Copyright © 2002 Mosby, Inc..

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse RVOT Obstruction in
Tetralogy• The dominant site of obstruction is
subvalvar.
• The pulmonary valve is often stenotic as well.
• Pulmonary arterial abnormalities.
• In some cases the outflow tract is atretic (pulmonary atresia). This form is often associated with aortopulmonary collateral arteries.

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse
Park: Pediatric Cardiology for Practitioners, 4th ed., Copyright © 2002 Mosby, Inc..

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse
Tex Heart Inst J. 1994; 21(4): 272–279. wikipedia

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse
Born et al. Visual Analysis of Cardiac 4D MRI Blood Flow Using Line Predicates. IEEE Transactions and Computer Graphics. Vol 19, No 6, June 2013.

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse
Born et al. Visual Analysis of Cardiac 4D MRI Blood Flow Using Line Predicates. IEEE Transactions and Computer Graphics. Vol 19, No 6, June 2013.

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse
Copyright © The American College of Cardiology. All rights reserved.
From: Pulmonary valve replacement in adults late after repair of tetralogy of Fallot: are we operating too late?J Am Coll Cardiol. 2000;36(5):1670-1675. doi:10.1016/S0735-1097(00)00930-X
Right ventricular (RV) end-systolic volume at rest. Pre-PVR = before pulmonary valve replacement, Post-PVR = after pulmonary valve replacement.
Figure Legend:

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse
Date of download: 4/24/2013
Copyright © The American College of Cardiology. All rights reserved.
From: Pulmonary valve replacement in adults late after repair of tetralogy of Fallot: are we operating too late?
J Am Coll Cardiol. 2000;36(5):1670-1675. doi:10.1016/S0735-1097(00)00930-X
Right ventricular (RV) end-diastolic volume at rest. Pre-PVR = before pulmonary valve replacement, Post-PVR = after pulmonary valve replacement.
Figure Legend:

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse Palliative Surgery for
Tetralogy• Seldom done any more.
• The purpose is to increase pulmonary blood flow and improve oxygenation.
• Types: • Blalock/Taussig/Thomas shunt.
• Waterston shunt.
• Potts shunt.
• Central shunt.

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse
Repair of Tetralogy
• Alleviation of RVOT obstruction.
• Patch closure of VSD.
• Variable amount of RVOT and pulmonary arterial patching.
• Surgical approach through right atrium and the pulmonary artery.
• A few patients need a valved conduit from RV to PA.

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse Course after Tetralogy
Repair

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse
Of patients surviving tetralogy repair, > 90% will live at least 25 years.
We have some data beyond that, but
treatment keeps changing, and so must
our analysis..

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse
Pulmonary regurgitation is overwhelmingly the dominant issue after tetralogy repair!!

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse
Echocardiography is not reliable in assessing the
adult right ventricle. MRI is best, with CT
angiography a close second when needed.

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse
Ventricular volumes should be indexed.
Should they be indexed to BSA or to height?

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse
We need to learn what aspect of right ventricular size and function should drive our decision-making:
•RV diastolic volume index?•RV systolic volume index?•RV ejection fraction?•Absolute values or changes?
I believe diastolic volume index is most important.

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse
The severity of PR is assessed best by MR, and
quite well by echo in skilled hands.

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse
The indications for and impact of pulmonary
valve replacement are becoming clearer.

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse
The probability of SCD after TOF repair is
~0.06% annually for the first 10 years, and ~0.2%
annually thereafter.

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse
Most repaired TOF patients who die suddenly
have had sustained arrhythmias or heart
failure.

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse
Repaired TOF patients with sustained VT should have both the arrhythmia
and the underlying hemodynamic problems
treated.

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse
Els Pieper’s Suggestion
• Text level 2• Text level 3• Text level 3
• Text level 2
• Text level 2

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse
Michigan Tetralogy Long-Term Survival
162 survivors
Followed 15-26 years (mean 20.2)
Late deaths = 9
25 year survival = 94.4%
Rosenthal ATS 1984

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse
Hickey EJCTS 2009
Toronto Tetralogy Late Outcomes
Inception cohort
1181 children born before 1984 repaired HSC.
Follow-up 2003-2006
1965 group outcomes– 1 year survival 72%– 40 year survival 64%
1985 group outcomes– 1 year survival 97%– 40 year survival 88%

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse
Hickey EJCTS 2009

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse
Hickey EJCTS 2009
Instantaneous hazard for death:0.25% annually at 10 years0.37% 200.49% 300.59% 40

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse
Munich Tetralogy Long-Term Survival
490 patients surviving at least 1 year
Surgery 1958-1977
Follow-up mean 25.3 ± 5.8 yrs
Survival– 10 years 97%– 20 years 94%– 30 years 89%
Nollert JACC 1997

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse Repaired Tetralogy and PR
#1
Most repaired TOF patients have substantial PR
PR is the dominant issue in their surveillance
PR is well tolerated by most for at least 20 years
In late follow-up to date, a significant minority will die or develop complications

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse Repaired Tetralogy and PR
#2
Most of the deaths and complications occur in patients with substantial PR
PR can be eliminated (for a time) by PVR
PVR is a low-risk procedure in skilled hands
PVR will require re-intervention at a predictable rate over time

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse Repaired Tetralogy and PR
#3
Patients who will not need PVR are those without “laminar PR”, & perhaps with a PR regurgitant fraction of < 20%, or a PR pressure half-time > 100 msec.
The other patients should be considered “at risk” of needing PVR at some time

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse Repaired Tetralogy and PR
#4
Indications for the timing of PVR are becoming clearer for patients with moderate-severe PR, and include:– Attributable symptoms– Sustained arrhythmias– Severe RV dilation (?RVEDVi > 150-170 cc/m2)– Modulating factors (QRS 180 msec, LV
dysfunction, inducible VT)

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse
What Can MRI Give Us?
RV end-diastolic volume (& index)
RV end-systolic volume (& index)
RVEF
PR fraction (main & branch PAs)
LV volumes & LVEF
Other data

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse
MRI is Best for the RV

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse Knauth
Heart 2008
Z-score 7 = 172 cc/m2 women & 185 cc/m2 in men

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse
Pressure Half-time is Very Good
Silversides JASE 2003
MildPR

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse
Pressure Half-time is Very Good
Silversides JASE 2003
SeverePR

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse
JACC 36; 1670-75; 2000

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse
PVR and the RV – Toronto 1
Conclusion:– RVEF did not improve after PVR
Therrien JACC 2000

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse
PVR and the RV - Leiden
Vliegen et al JACC 2002

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse
PVR and the RV - Leiden
Vliegen et al JACC 2002

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse
EHJ 2005

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse
The Melody Valve
Coats EJCTS 2005

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse
The Melody Valve

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse
Incidence of SCD in Congenital Heart DiseasePopulation-based study3,600 patients < 19 yearsSurgery for common CHDBetween 1958-199641 SCD in total1/1,118patient-years FU
Event rate was lesion specific
Silka JACC 1998Silka JACC 1998

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse
Khairy Circulation 117: 363-370; 2008

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse
Khairy Circulation 117: 363-370; 2008

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse
ECG in Repaired Tetralogy

ISA
CH
D C
onge
nita
l Hea
rt D
isea
se B
asic
Cou
rse
Components of Tetralogy
• Ventricular septal defect.
• Pulmonary stenosis (right ventricular outflow tract obstruction).
• Overriding of the aorta (located above the VSD and partially over the right ventricle).
• Right ventricular hypertrophy.