
Compliance, motivation, and health behaviors
77
+ Compliance, Motivation, and Health Behaviors of the Learner
-
Upload
stanbridge -
Category
Education
-
view
174 -
download
3
Transcript of Compliance, motivation, and health behaviors

+
Compliance, Motivation,
and Health Behaviors
of the Learner
+Kelly, OTS
● Bachelors of Science, Health Science
● Chapman University
● 6 years experience with Pediatrics ○ Worked at pediatric clinics, hospitals, and camps
○ I currently work as a Teacher aide
● Fun fact: I want to try to go to all National Parks in the US
before I die!

+Paola, OTS
● Bachelor of Arts, Psychology
● University of California, Riverside
● 6 years experience in Mental Health ○ 5 years working as an Applied Behavior Analysis Therapist
○ 1 year working as a Behavioral Health Specialist at a Health
Plan
● Fun fact: I love giraffes

+Natasha, OTS
● Bachelors of Science, Exercise Science
● Rutgers University
● 4 years experience as a PT aide
● 3 years experience as a teacher’s aide
● Fun fact: I was a vegetarian for most of my life but started eat
meat a couple of years and I LOVE it!

+Objectives
1. Define the terms compliance, adherence, and motivation relevant to behaviors of the
learner.
2. Discuss compliance and motivation concepts and theories.
3. Identify incentives and obstacles that affect motivation to learn.
4. State axioms of motivation relevant to learning.
5. Assess levels of learner motivation.
6. Outline strategies that facilitate motivation and improve compliance.
7. Recognize the role of the health professional as educator in health promotion.

+Ice Breaker Game!

+
Are you a visual learner or
an auditory learner?
+
Are you more motivated to study if
you are not stressed/anxious at all
or if you are have a moderate level
of stress/anxiety?
+
Are you compliant when it
comes to learning new
things or noncompliant?

+
Are you more internally
motivated or externally
motivated?

+
Does your relationship with
your educator impact how
you learn or not?

+
Are you more of a dreamer
or a realist?
+
Do you think uncertainty
is a motivating factor or
an unmotivating factor?
+
Do you get more done
when you have more time
or less time?
+
Do you feel like you are in a
collaboration with your healthcare
provider or do you feel like a
submissive participant?
+
Do you follow through with what
you say or do you forget about
those commitments?
+Vocab
○ Compliance:
■ submission or yielding to the recommendations or will of
others
○ Noncompliance
■ Failure or refusal to comply
○ Adherence:
■ commitment or attachment to a regimen

+Compliance
■ Observable behavior■ Can be directly measured■ In healthcare compliance
is seen with an authoritative tone ■ Practitioner =
Authority■ Consumer =
Submissive

+Adherence/ Nonadherence
● Compliance○ Obedience or passive acceptance of the healthcare regimen
● Adherence ○ Support or commitment to a plan of care
● An individual can comply with a regimen and not be committed to it.
● Nonadherence → cognitive function, social support, financial constraints
+Vocab Matching!
Compliance
Adherence
Nonadherence
Commitment or attachment to a regimen
Can be intentional or unintentional and can
be affected by such variables as cognitive
function, social support and financial
constraints
Submission or yielding to the
recommendations or will of others
VOCAB DEFINITION

+Perspectives on Compliance● Theories and models are used to explain compliance from a
multidisciplinary approach that includes psychology and education ○ 1.) Biomedical theory: links compliance with patient characteristics
○ 2.) Behavioral/Social Learning Theory: includes external factors based on an social
environment that influences their behaviors
○ 3.) Communication models: communication between client and health care professional
○ 4.) Rational Belief theory: clients decide to comply or not comply by weighing the
benefits of treatment and the risks of disease through the use of cost-benefit logic
○ 5.) Self-regulatory systems: patients are the problem solvers , regulatory behavior based
on perception of illness, cognitive skills, and past experiences affect planning and coping
to illness
+Vocab
● Locus of control ○ Refers to an individual's sense of responsibility for his
behaviors and the extent to which motivation to take action
originates from within self (internal) or is influenced by others
(external)
+Locus of Control
● Educator will make an attempt to partly control decision
making by the learner
● Internal:
○ self-directed, they have their own control
● External:
○ influenced by health outcomes, fate
● Inconclusive data on compliance and internals vs externals
● Has connection with compliance in some therapeutic
regimen but not all

+Vocab
● Noncompliance ○ Nonsubmission or resistance of the individual to follow a
prescribed, predetermined regimen
+Noncompliance
● Noncompliant behavior:○ Blaming
○ Judgemental
○ Disobedience
● People tend to make excuses for noncompliance, even if they have nothing to lose.
● Places client under unnecessary health risk and increases health care costs.
+Reasons for Noncompliance
Why clients are noncompliant remains unanswered.
○ Knowledge
○ Motivation
○ Treatment factors → side effects
○ Disease issues → prognosis
○ Lifestyle issues → transportation
○ Sociodemographic factors → social and economic status
○ Psychosocial variables → depression and fear
Noncompliant behavior could be desirable and prove beneficial in stressful situations.

+Vocab Matching!
Locus of control
Noncompliance
Resistance of the individuals to
follow a predetermined regimen
Refers to an individual's sense of
responsibility for his behaviors
and the extent to which
motivation to take actions
originates from internal or
external motivators
VOCAB DEFINITION
+Vocab
● Motivation○ A psychological force that moves a person to take action in the
direction of meeting a need or goal, evidenced by willingness or
readiness to act.
● Motivational factors ○ Factors that influence motivation can serve as incentives or obstacles
to achieve desired behaviors
● Motivational incentives ○ Factors that influence motivation in the direction of the desired goal

+Motivation
● Internal factors● External factors ● Implicit motivation
○ Movement in the direction of meeting a need or toward
reaching a goal
● Health provider’s role → facilitator to reach desired goal and prevent delays

+Hierarchy of Needs
● Maslow’s Motivational Theory ○ Complexity of the concept of motivation
○ Not all behavior is motivated
○ Hierarchy of Needs
■ Physiological, safety, love/belonging, self-esteem, and
self actualization
■ Needs are related to their level of potency

+Motivational Factors ● Creating incentives and decreasing obstacles are
challenging for healthcare professionals as educators
● Facilitating/blocking factors that influence individuals to learn:
○ Personal attributes
○ Environmental factors
○ Learner relationship systems

+ Motivational Factor:
Personal Attributes
● Can be:
○ physical
○ developmental
○ psychological components of the individual learner
● Can shape an individual’s motivation to learn ● Learners views about the complexity and the extent of
changes that are needed can shape motivation
+ Motivational Factor:
Environmental Influences ● Can be: physical and attitudinal climate, physical characteristics of
the learning environment, availability of human resources, and different types of behavioral rewards
● Promotes learning:
○ pleasant, comfortable, adaptable surroundings
● Detract from learning:
○ noise, confusion interruptions, lack of privacy

+ Motivational Factor:
Learner Relationships Systems
○ What influences motivation: ■ family or significant others in
the support system
■ cultural identity
■ work
■ school
■ community
■ roles
■ teach-learner interactions
○ Relationships are not
theory on their own but
just a force that acts on
motivation
+Match the Vocab!
Motivation
Motivational factors
Motivational Incentives
Factors that influence motivation in
the direction of the goal
Psychological force that moves a
person toward some kind of action;
means to set in motion
Facilitating/blocking factors that
influence individuals to learn
VOCAB DEFINITION
+Vocab
● Motivational axioms
○ Rules that set the stage for motivation
● Axioms
○ Premises on which an understanding of phenomenon is based

+Motivational Axioms
● Health professional as an educator must understand the premises
involved to promote motivation of the learner
● Motivational axioms set the stage for the learner:
1. The state of optimum anxiety
2. Learner readiness
3. Realistic goal setting
4. Learner satisfaction/success
5. Uncertainty reduction/maintaining dialogue

+Break!
10 minutes!

+State of Optimum Anxiety
● Learning occurs best when a state of moderate anxiety exists ○ Low levels of anxiety: low level of motivation
○ Moderate levels of anxiety: comfortably managed & promotes learning
○ high/severe levels of anxiety: reduces ability to perceive environmental, concentration,
& learning
● Optimum state for learning- when perception, abstract thinking,
concentration, and information processing are enhanced
● Learning is achieved during learning/challenging situation- this is
how learning works in an anxiety provoking situation
+Learner Readiness
● What factors influence motivation- desire to move towards a goal and
readiness to learn
● Desire cannot be imposed on a learner but it can be influenced by
external forces and promoted by the educator
● Incentives as rewards and reinforcers
○ Tangible
○ Intangible
○ External
○ Internal

+Realistic Goal ● Individual will work towards goals:
○ Within his/her grasp
○ Possible to achieve
● Individual will give up:
○ When goals are unrealistic → loss of valuable time
○ Beyond his/her grasp → frustration and counterproductiveness
● Setting realistic goals is a motivating factor
● Goals:
○ Should equal behavioral change needed
○ Should be created collaboratively between learner and educator
■ reduces negative effects of hidden agendas or sabotaging
educational plans
○ Should be created after the learner knows what to change
+Learner Satisfaction/Success
● Learners are motivated by success
● Success is self satisfying and feeds the learners self-
esteem
● Focus on success as positive reinforcement to promote
learner satisfaction and a sense of accomplishment

+Uncertainty Reduction
■ Uncertainty is a motivating
factor
■ Individuals have internal
dialogues that can reduce or
maintain uncertainty.
■ Uncertainty of outcomes can =
uncertainty of bx = maintaining
uncertainty
■ Premature uncertainty
reduction can be
counterproductive
+Assessment of Motivation
● Part of the general health assessment ● Parameters for motivational assessment of the learner
○ Previous attempts
○ Curiosity
○ Goal setting
○ Self-care ability
○ Stress factors
○ Survival issues
○ Life situations
+Assessment of Motivation cont’d
Subjective■ Dialogue
■ Nonverbal cues■ Self-reports
Objective
■ Observation of expected
behaviors
+Vocab
Motivational Interviewing
Concept mapping
Enables the learner to integrate previous
learning with newly acquired knowledge
through diagrammatic mapping
Method of being ready to change in order to
promote desired health behaviors
+Motivational Strategies
● Motivational strategies in the educational setting → clear communication, clarifying directions and
expectations, organizing material in a meaningful way for the learner, environmental manipulation, positive
verbal feedback, and providing opportunities for success
● Attention, Relevance, Confidence and Satisfaction (ARCS) model: main focus is to create and maintain
motivational strategies used for instructional design
○ Attention
○ Relevance
○ Confidence
○ Satisfaction
● Motivational interviewing
○ THE EDUCATOR MUST ASK: “what specific behavior, under what circumstances, in what time frame, is
desired by the learner?”
○ Client eventually comes to realization and will self-report that they are ready to make a change
○ Interviewer seeks to gain knowledge about health beliefs
○ Explore client’s motivation for adherence to health regimens
+Selected Models and Theories
● These models and theories describe, explain, and predict health
behaviors that can be used as a tool for health-promotion
● Understanding these theories allows educator to promote compliance to
a health regime or facilitate motivation :
○ Health Belief Model
○ Self Efficacy theory
○ Protection Motivation Theory
○ Stages of Change Model,
○ Theory of reasoned action
○ Therapeutic alliance model
+Health Belief Model
● A framework or paradigm used to explain or predict health behavior composed of the interaction between individual perceptions, modifying factors, and likelihood of action.
● Developed in 1950s to examine why people did not participate in
health screening programs.
● 2 premises on which model is built○ Eventual success of disease prevention
○ Belief that health is highly valued

+Health Belief Model Components
○ Individual perception
■ Subcomponents of perceived susceptibility or perceived severity
of a specific disease
○ Modifying factors
■ Demographics variables (age, sex, etc)
■ Sociopsychological variables (personality, locus of control, etc.)
■ Structurable variables (knowledge about and prior contact with
disease)
○ Likelihood of action
■ Subcomponents of perceived benefits of preventive action
minus perceived barriers to preventive action

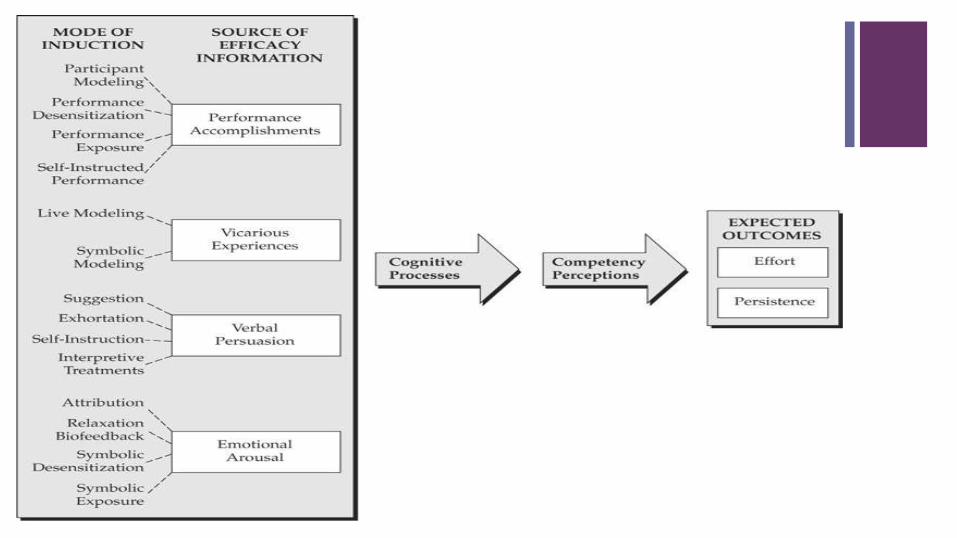
+Self-Efficacy Theory
● A framework that describes the belief that one is capable of accomplishing a specific behavior.
● Self-efficacy is an accurate predictor of the course of health behavior
● Self efficacy is appraised and processed through the following sources of information:
1. Performance accomplishments through self-mastery
2. Vicarious experiences; such as observing expected behavior through modeling of others
3. Verbal persuasion from others who present realistic beliefs that the individual is capable
of the expected behavior
4. Emotional arousal through self-judgement of physiological states of distress
+
+Protection Motivation Theory
● A linear motivational theory that explains behavioral
change in terms of threat and coping appraisal, which
leads to intent and ultimately to action.

+Protection Motivation Theory cont...
● A threat to health is a stimulus to protection motivation
● Has researched what are the antecedents to health behaviors such as:
○ Drug abuse
○ AIDS
○ Smoking
○ Sun protection
○ Drinking behaviors
+Stages of Change Model
● A model developed by Prochaska that forms the phenomenon of
health behaviors of the learner, particularly applied to addictive
and problem behaviors, and includes the six distinct stages of
change:
● Also known as the transtheoretical model
● Stage the client’s intentions and behaviors for change as well as
strategies that will enable completion of the specific stage
● The extent to which people are motivated and ready to change is
seen as an important construct

+ Stages of Change Model:
Six Components
● There are six time related stages of change:
1. Precontemplation: individuals have no current intention of changing
2. Contemplation: individuals accept or realize they have a problem and
begin to think seriously about changing it
3. Preparation: individuals are planning to take action within the time frame
of one month
4. Action: there is overt/visible modification of the behavior
5. Maintenance: may last six months to a lifetime, difficult to achieve
6. Termination: when the problem no longer presents any temptation

+Theories of Reasoned Action
● A framework that is concerned with prediction and understanding of human behavior within a social context.
● Emerged from a research program that began in the 1950s
● Humans behave in a way that is consistent with their beliefs
● Behavior is determined by:
1. Beliefs, attitude toward the behavior, and intention
2. Motivation to comply with influential persons known as referents, subjective norms, and intention
+Vocab
● Therapeutic Alliance Model
○ An interpersonal provider-client model that addresses the
continuum of compliance, adherence, and collaboration in
therapeutic relationships.
● Concordance:
○ Consultation that allows for mutual respect for the patient’s and the
professional’s beliefs, allows negotiation to take place about the best
course of action for the patient

+Therapeutic Alliance Model
● Caregiver and receiver have therapeutic alliance in
which both of them have equal power
● Shift towards self-determination and control over one’s
own life is fundamental in this model
● Learner is active and responsible
● Educator and learner have common goal self-care

+Educators Agreement with Model
Conceptualizations
Health belief model Likelihood of action
Protection motivation theory Attain positive health outcomes
Theory of reasoned action Attitude and intention
Self-efficacy theory Belief in one's capabilities
Therapeutic alliance model Reduce noncompliance through an educator-learner collaboration
Stages of change model Stage individual's readiness for change and develop strategies for interventions

+Match Theories!
Health belief model a) Attain positive health outcomes
Protection Motivation Theory b) Stage individual's readiness for change and develop strategies for interventions
Theory of Reasoned Action c) Reduce noncompliance through an educator-learner collaboration
Self-Efficacy Theory d) Likelihood of action
Therapeutic Alliance Model e) Belief in one's capabilities
Stages of change model f) Attitude and intention
+Functional Utility of Models
Questions to be asked to determine functional
utility :
● Who
● What
● When
● Where
+ Functional Utility of Models:
Who?
Who is target learner?
○ Target learner could be individual, family, or group
○ Many different models can be used with the target
learners
○ Probability of individual variation
+ Functional Utility of Models:
What?
● What is the timing of the educational experience?
● What setting will the client be in?
● What is focus of the learning?
○ Content to be taught → disease, treatment,
adaptation techniques, promotion of wellness,
expectations of specific health practice, or focus on
self-care

+ Functional Utility of Models:
When?
When is optimal time?
○ Readiness of the learner, a mutually convenient
time, and prevention of untimely delays in moving
toward a desired goal
○ Time is often neglected in the models

+ Functional Utility of Models:
Where?
Where is the process to be carried out?
○ Settings of home, workplace, school, institution, or
specific community locations
+Integration of Models for Use in
Education ● Model integration - a multitheory approach to promote health
behaviors
○ Use more of an integrative approach using goal theories and
stages of change rather than unidirectional and nondynamic
approaches to behavioral change
● In order to meet needs of the learner, principles of
pedagogy(teaching children), andragogy(teaching adults), and
gerogogy(teaching older adults) are incorporated

+The Role of Health Professional as
Educator in Health Promotion● Health professionals role is to promote healthy lifestyles
● They can combine content that is specific to their scope of practice and
knowledge of educational theories and health behavior models to come up
with an integrated approach in order to shape health behaviors of
individuals through education
+Facilitator of Change
● Effective ways to facilitate change in education :
○ Explain
○ Analyze
○ Divide Complex Skills
○ Demonstrate
○ Practice
○ Ask Questions
○ Provide Closure
● Focus on promotion of health!

+Contractor
● Informal or formal contracts can delineate and promote learning
objectives
● Educational contracting - state mutual goals to be accomplished, devise
an agreed upon plan of action, evaluate the plan, and derive alternatives
● Plan of action has to be specific and includes who, what, when, where,
and how
● Clearly state responsibilities help in evaluating the plan and directing plan
revisions
● Health care worker needs to be
○ Approachable
○ Trustworthy
○ Culturally sensitive
+Organizer
● Organization includes:
○ manipulating materials and space
○ organizing content from simple to complex
○ prioritizing subject matter
● Organization decreases obstacles for the learner and
simplifies the situation
+Evaluator
● Evaluations of educational programs in the form of
outcomes are necessary to show accountability to the
learner
● Application of knowledge that improves the health of
individuals, families, and groups is the evaluative
measure of learning
+State of Evidence
● Less than adequate evidence for implementing health care
interventions focused on compliance and motivation in regards to
the health behaviors of the learner
● “ a clarion call is needed for both qualitative and quantitative
conceptually grounded research to be infused into the teaching-
learning process” pg 22-23

+Summary
● Compliance and motivation aspects
● Assessments of learner motivation
● Incentives and obstacles

+Concluding Thoughts
● Foundation for learning is set when information is
imparted, accepted, applied and the foundation is set
for a change is health behaviors
● When people are motivated and they know they can
make a difference in their own lives, a barrier to health
is lifted

+References
Richards, E. & Digger, K. (2011). Compliance, Motivation, and
Health behaviors of the Learner. In Health professional as
educator: principles of teaching and learning. (pp.199-223).
Jones and Bartlett Learning.
(lets double check this)

+
Thank you!
“We can appeal to
people’s motives
be we can’t
motivate them” -
Green & Kreuter(1999)


















