
Complex regional pain syndrome Review -...
11
For personal use. Only reproduce with permission from The Lancet. THE LANCET Neurology Vol 2 November 2003 http://neurology.thelancet.com 687 Complex regional pain syndrome (CRPS) is the result of changes to the somatosensory systems that process noxious, tactile, and thermal information; to the sympathetic systems that innervate skin (blood vessels, sweat glands); and to the somatomotor systems. The changes suggest that the CNS representations of the systems have been altered. Patients with CRPS also have peripheral changes (eg, oedema, signs of inflammation, sympathetic-afferent coupling [the basis for sympathetically maintained pain], and trophic changes) that cannot be explained by central changes. On the basis of clinical observation and research in human beings and animals, we hypothesise that CRPS is a systemic disease involving the CNS and peripheral nervous system. The most important question for future research is what causes CRPS? In this article, we suggest a change to the focus of research efforts and treatment. We also suggest there be diagnostic reclassification and redefinition of CRPS. Lancet Neurol 2003; 2: 687–97 Complex regional pain syndromes (CRPSs) are painful disorders that develop as a disproportionate consequence of traumas. These disorders are most common in the limbs and are characterised by pain (spontaneous pain, hyperalgesia, allodynia), active and passive movement disorders (including an increased physiological tremor), abnormal regulation of blood flow and sweating, oedema of skin and subcutaneous tissues, and trophic changes of skin, organs of the skin, and subcutaneous tissues. 1–6 CRPS I (previously known as reflex sympathetic dystrophy 7 ) typically develops after minor trauma with no obvious or a small nerve lesion (eg, bone fracture, sprains, bruises, skin lesions, or surgery). CRPS I can also develop after remote trauma in the visceral domain or even after a CNS lesion (eg, stroke). Important features of CRPS I are that the severity of symptoms is disproportionate to the severity of trauma and pain has a tendency to spread distally in the affected limb. The symptoms are not confined to the innervation zone of an individual nerve. Thus, all symptoms of CRPS I may be present irrespective of the type of the preceding lesion. Furthermore, the site of the lesion at the limb does not determine the location of symptoms. CRPS II (previously known as causalgia) develops after a large nerve lesion. This classification of CRPS is based on a consensus between clinicians and basic scientists and is practice-based, not mechanism-based. 5,8,9 Although both CRPS I and CRPS II are categorised under neuropathic pain they seem to be mechanistically rather different syndromes. CRPS II (nerve lesion present) is by definition a neuropathic pain syndrome. However, the more common CRPS I is unlikely to be a neuropathic pain syndrome. Patients with CRPS I do not have an obvious nerve lesion, but the neuropathic pain results from injuries or diseases that affect the peripheral nervous system or the CNS. 8 CRPS I is a fascinating syndrome for basic and clinical scientists. Various traumas can trigger combinations of clinical phenomena in which the somatosensory system, the sympathetic nervous system, the somatomotor system, and peripheral (vascular, inflammatory) systems are involved. Also, intensity and combination of clinical symptoms are out of proportion with the causal lesion. This situation has been extensively described since Silas Weir (causalgia/CRPS II), 10–12 Paul Sudeck (CRPS I), 13,14 René Leriche, 15,16 John Bonica, 17 and others. The work has created the present jungle of names, theories about the mechanisms that underlie this syndrome, 5,18,19 and recommended treatment options. 20 By use of an integrative approach with basic and clinical research we argue that the mechanisms that underlie this syndrome can be explained. 4,21 In this review we primarily focus on CRPS I because this syndrome is much more prevalent than CRPS II. However, mechanisms that underlie CRPS II are included in-so-far as patients with CRPS II may have all the symptoms seen in patients with CRPS I. Observations in patients and mechanisms Results of experiments in patients with CRPS and quantitative clinical data clearly set the stage to formulate hypotheses that can be tested experimentally with various in vivo or in vitro animal models, or in human beings. Any model is an approximation of the clinical situation and research on mechanisms should focus on quantifiable symptoms seen in patients (eg, mechanical allodynia, spontaneous pain, tremor, changes of blood flow, swelling, etc). Each symptom can be generated by more than one mechanism depending on the patient. Experimental models used to study the underlying mechanisms of CRPS cannot represent CRPS I or CRPS II as such, at least not in the first approach. For this purpose patients are the best. Review Complex regional pain syndrome WJ is at the Department of Physiology and RB is at the Neurological Clinic, Christian-Albrechts-University of Kiel, Kiel, Germany. Correspondence: Prof Wilfrid Jänig, Physiologisches Institut, Christian-Albrechts-Universität zu Kiel, Olshausenstrasse 40, 24098 Kiel, Germany. Tel +431 880 2036; fax +431 880 5256; email [email protected] Complex regional pain syndrome: mystery explained? Wilfrid Jänig and Ralf Baron
Transcript of Complex regional pain syndrome Review -...

For personal use. Only reproduce with permission from The Lancet.
THE LANCET Neurology Vol 2 November 2003 http://neurology.thelancet.com 687
Complex regional pain syndrome (CRPS) is the result ofchanges to the somatosensory systems that processnoxious, tactile, and thermal information; to the sympatheticsystems that innervate skin (blood vessels, sweat glands);and to the somatomotor systems. The changes suggest thatthe CNS representations of the systems have been altered.Patients with CRPS also have peripheral changes (eg,oedema, signs of inflammation, sympathetic-afferentcoupling [the basis for sympathetically maintained pain], andtrophic changes) that cannot be explained by centralchanges. On the basis of clinical observation and research inhuman beings and animals, we hypothesise that CRPS is asystemic disease involving the CNS and peripheral nervoussystem. The most important question for future research iswhat causes CRPS? In this article, we suggest a change tothe focus of research efforts and treatment. We also suggestthere be diagnostic reclassification and redefinition of CRPS.
Lancet Neurol 2003; 2: 687–97
Complex regional pain syndromes (CRPSs) are painfuldisorders that develop as a disproportionate consequence oftraumas. These disorders are most common in the limbs andare characterised by pain (spontaneous pain, hyperalgesia,allodynia), active and passive movement disorders(including an increased physiological tremor), abnormalregulation of blood flow and sweating, oedema of skin andsubcutaneous tissues, and trophic changes of skin, organs ofthe skin, and subcutaneous tissues.1–6
CRPS I (previously known as reflex sympatheticdystrophy7) typically develops after minor trauma with noobvious or a small nerve lesion (eg, bone fracture, sprains,bruises, skin lesions, or surgery). CRPS I can also developafter remote trauma in the visceral domain or even after aCNS lesion (eg, stroke). Important features of CRPS I arethat the severity of symptoms is disproportionate to theseverity of trauma and pain has a tendency to spread distallyin the affected limb. The symptoms are not confined to theinnervation zone of an individual nerve. Thus, all symptomsof CRPS I may be present irrespective of the type of thepreceding lesion. Furthermore, the site of the lesion at thelimb does not determine the location of symptoms. CRPS II(previously known as causalgia) develops after a large nervelesion.
This classification of CRPS is based on a consensusbetween clinicians and basic scientists and is practice-based,not mechanism-based.5,8,9 Although both CRPS I and CRPSII are categorised under neuropathic pain they seem to bemechanistically rather different syndromes. CRPS II (nerve
lesion present) is by definition a neuropathic painsyndrome. However, the more common CRPS I is unlikelyto be a neuropathic pain syndrome. Patients with CRPS I donot have an obvious nerve lesion, but the neuropathic painresults from injuries or diseases that affect the peripheralnervous system or the CNS.8
CRPS I is a fascinating syndrome for basic and clinicalscientists. Various traumas can trigger combinations ofclinical phenomena in which the somatosensory system, thesympathetic nervous system, the somatomotor system, andperipheral (vascular, inflammatory) systems are involved.Also, intensity and combination of clinical symptoms areout of proportion with the causal lesion. This situation hasbeen extensively described since Silas Weir (causalgia/CRPSII),10–12 Paul Sudeck (CRPS I),13,14 René Leriche,15,16 JohnBonica,17 and others. The work has created the presentjungle of names, theories about the mechanisms thatunderlie this syndrome,5,18,19 and recommended treatmentoptions.20
By use of an integrative approach with basic and clinicalresearch we argue that the mechanisms that underlie thissyndrome can be explained.4,21 In this review we primarilyfocus on CRPS I because this syndrome is much moreprevalent than CRPS II. However, mechanisms that underlieCRPS II are included in-so-far as patients with CRPS II mayhave all the symptoms seen in patients with CRPS I.
Observations in patients and mechanismsResults of experiments in patients with CRPS andquantitative clinical data clearly set the stage to formulatehypotheses that can be tested experimentally with various invivo or in vitro animal models, or in human beings. Anymodel is an approximation of the clinical situation andresearch on mechanisms should focus on quantifiablesymptoms seen in patients (eg, mechanical allodynia,spontaneous pain, tremor, changes of blood flow, swelling,etc). Each symptom can be generated by more than onemechanism depending on the patient. Experimental modelsused to study the underlying mechanisms of CRPS cannotrepresent CRPS I or CRPS II as such, at least not in the firstapproach. For this purpose patients are the best.
ReviewComplex regional pain syndrome
WJ is at the Department of Physiology and RB is at theNeurological Clinic, Christian-Albrechts-University of Kiel, Kiel,Germany.
Correspondence: Prof Wilfrid Jänig, Physiologisches Institut,Christian-Albrechts-Universität zu Kiel, Olshausenstrasse 40,24098 Kiel, Germany. Tel +431 880 2036; fax +431 880 5256;email [email protected]
Complex regional pain syndrome: mysteryexplained?
Wilfrid Jänig and Ralf Baron

For personal use. Only reproduce with permission from The Lancet.
THE LANCET Neurology Vol 2 November 2003 http://neurology.thelancet.com688
Somatosensory abnormalities and painUntil recently, experimental investigations of CRPS havemainly concentrated on pain, sympathetically maintainedpain (SMP), and abnormalities at the skin. This led to arather limited view with the tendency to put the nociceptivesystem and its peripheral (and maybe central) coupling tothe sympathetic nervous system into the foreground. Yetclinical observations of CRPS I show that the pain iscommonly projected into the deep somatic tissues, thatmany patients do not have SMP (as judged by clinicalcriteria; eg, significant decrease in pain followingsympathetic blocks), and that 5% of the patients do not evenhave spontaneous pain but have evoked pathological pains.
Sensory systemsMost patients with CRPS I have a burning spontaneous painfelt mostly deep in the distal part of the affected limb.2
Characteristically, the pain is disproportionate in intensity tothe initial event. The pain usually increases when the limb is ina dependent position. Stimulus-evoked pains includemechanical, cold and heat allodynia, and hyperalgesia. Thesesensory abnormalities appear early in many patients, are mostpronounced distally, and have no consistent spatial relation toindividual nerve territories or to the site of the trauma.22–25 Painis typically elicited by movements and pressure at the joints(deep somatic allodynia), even if the joints are not the site ofthe causal lesion, which indicates that the deep somatic tissuesare involved. On the basis of experimental findings in animals,spontaneous pain and various forms of allodynia/hyperalgesiain the distal portion of the limb are thought to be generated byprocesses of peripheral and central sensitisation.26
50% of patients with chronic CRPS I develophypoaesthesia and hypoalgesia on the whole half of the bodyor in the associated quadrant on the same side as the affectedarm. In these patients quantitative sensory testing has shownthat thresholds to mechanical, cold, warmth, and noxiousheat stimuli are higher on the affected side than on thehealthy body side (figure 1).27 Patients with these extendedsensory deficits have a longer illness, greater pain intensity, ahigher frequency of mechanical allodynia, and a highertendency to develop changes in the somatomotor systemthan do patients with spatially restricted sensory deficits.27–29
The anatomical distribution suggests that these deficits aredue to CNS changes that may cause widespread alterationsin the perception of painful and non-painful sensations.
The central representation of somatosensory sensationsis changed, probably in the thalamus and cortex.22,27 Thistheory has been supported by two recent studies of patientswith CRPS by use of PET or magnetoencephalography.30,31 Ifgeneralised sensory deficits in patients with chronic CRPS Iare permanent and irreversible, it would be the firstdocumented case of such irreversible changes in the brainthat are triggered by trauma with minor or no nerve lesion.
These findings lead to several important questions. Arethe generalised sensory changes correlated with neglect-likephenomena in these patients32 also present in patients withdisuse syndrome?33 And, therefore, is one commondenominator of CRPS, neglect-syndrome, and disusesyndrome an absent input from deep somatic tissues(skeletal muscles, joints, fascia) to the centralrepresentations? Most patients with CRPS I have deepsomatic spontaneous pain and mechanical
Review Complex regional pain syndrome
30·5,34·32·1
28·5,35·1,42·32·2
29·2,35·5,42·92·4
29·5,36·8,42·82·6
28·3,36·3,42·6
30·6,34·42·1
28·4,36·0,42·12·4
28·8,35·9,42·43·0
27·7,36·3,42·65·1
27·7,37·2,42·6
27·9,35·94·0
28·0,37·5,42·95·7
25·8,37·8,43·86·9
26·2,39·3,43·012·9
26·7,37·6,43·3
30·0,34·32·1
30·4,35·4,42·32·2
30·3,35·3,42·32·7
28·5,36·2,42·52·7
28·5,36·1,42·3
Figure 1. Detection thresholds to cold, warm, and heat stimuli (upper numbers [�C]) and to von Frey filament stimulation (lower rows [g/mm2]) in patientswith CRPS I and sensory impairment spatially restricted to the affected limb (left) and in CRPS I patients with generalised sensory impairment (right).Numbers show mean values. Significant differences between left-hand side and right-hand side and right are indicated in bold. Reproduced withpermission from Elsevier Science.27

For personal use. Only reproduce with permission from The Lancet.
THE LANCET Neurology Vol 2 November 2003 http://neurology.thelancet.com 689
hyperalgesia/allodynia. Are the non-painful sensationselicited from muscle and joints changed too? Finally, do thegeneralised sensory changes depend on a continuousnociceptive input from the affected region and disappearafter successful treatment of the pain? After all, thecontinuous nociceptive afferent input could be subthresholdfor the conscious perception of pain, but high enough tomaintain the central changes.
Sympathetically maintained pain (SMP)On the basis of experience and clinical studies the term SMPwas redefined. Patients who present with similar clinicalsigns and symptoms can clearly be divided into two groupsby the positive or negative effect of selective blockade of the sympathetic nervous system or blockade of �-adrenoceptors34,35 into those with SMP and those withsympathetically independent pain. SMP is now defined as asymptom in a subset of patients with neuropathic disordersand not a clinical entity and not essential for the diagnosis ofCRPS I.9,36
Influence of sympathetic activity and catecholamines onprimary afferents in patients with CRPSClinical studies support the idea that cutaneous nociceptorsdevelop catecholamine sensitivity after partial nerve lesions(CRPS II). Intracutaneous application of norepinephrineinto a symptomatic skin area rekindles spontaneous painand dynamic mechanical hyperalgesia or allodynia that hadbeen relieved by sympathetic blockade.37,38 Intracutaneousinjection of norepinephrine in control individuals does notelicit pain.
The question arises whether the mechanisms of SMP aresimilar in CRPS I, even though there is no major nervelesion present. We used physiological stimuli to excitesympathetic neurons in patients with CRPS I.21 Cutaneoussympathetic vasoconstrictor outflow to the painful area wasexperimentally activated to the highest possiblephysiological degree by whole body cooling. Thisexperimental intervention selectively changes sympatheticcutaneous vasoconstrictor activity without influencing othersympathetic systems innervating the deep somatic tissues(eg, muscle vasoconstrictor neurons39,40). During the thermalchallenge the affected region was kept at 35°C in order toavoid thermal effects at the nociceptor level. The intensity ofspontaneous pain and mechanical hyperalgesia or allodynia(dynamic and punctate) and the area of dynamicmechanical hyperalgesia or allodynia increased significantlyin patients that had been classified as having SMP bypositive sympathetic blocks but not in patients withsympathetically independent pain (figure 2).
In these patients, the relief of spontaneous and evokedpain after sympathetic blockade was more pronounced thanchanges in spontaneous and evoked pain that could beinduced experimentally by sympathetic activation. Oneexplanation for this discrepancy might be that a completesympathetic block affects all sympathetic outflow channelsprojecting to the affected region. It is very likely that inaddition to a coupling in the skin, a sympathetic-afferentinteraction may also occur in other tissues, in particular
ReviewComplex regional pain syndrome
0 40 80 40 80
200
300
400
Ski
n bl
ood
flow
(PU
)
100
29
34
Ski
n te
mpe
ratu
re (ºC
)
24
0
Affected limb
Unaffected limb
Unaffected limb
Affected limb
Duration of cooling (%) Duration of warming (%)
High sympathetic activity
Dynamicmechanicalhyperalgesia
Low sympathetic activity
Figure 2. Experimental modulation of cutaneous sympatheticvasoconstrictor neurons by physiological thermoregulatory reflexstimuli in 13 CRPS patients. With the help of a thermal suit, whole-bodycooling and warming was done to change sympathetic skin nerveactivity. Top: high sympathetic vasoconstrictor activity during coolinginduces considerable drop in skin blood flow on the affected andunaffected region (laser Doppler flowmetry). Middle: on the unaffectedside a secondary decrease of skin temperature was documented. On the affected side the forearm temperature was clamped at 35°C by a feed-back-controlled heat lamp to exclude temperature effects on the sensory receptor level. Bottom: effect of cutaneous sympatheticvasoconstrictor activity on dynamic mechanical hyperalgesia in one patient with CRPS with SMP. Activation of sympathetic neurons (during cooling) leads to an increase of the area of dynamic mechanical hyperalgesia. Reprinted with permission fromElsevier Science.21

For personal use. Only reproduce with permission from The Lancet.
THE LANCET Neurology Vol 2 November 2003 http://neurology.thelancet.com690
bone, muscle, and joint tissues which are especially painfulin some patients with CRPS.2,41
Mechanisms of SMP Quantitative measurements in patients with CRPS I withSMP clearly show that the underlying mechanism of SMPmust be a coupling of sympathetic noradrenergic neuronswith primary afferent neurons in the periphery of the bodyand that the mechanism is different in CRPS II comparedwith CRPS I.
Animal models lend support for peripheral mechanismsbeing involved in SMP in CRPS II (figure 3).4,42–45 It shouldbe kept in mind that coupling of sympathetic neurons notonly to nociceptive afferent neurons but also to non-nociceptive ones (eg, mechanosensitive, cold) may turn outto be important. Sympathetic activation of these afferentneurons may excite sensitised or hyperexcitable centralneurons of the somatosensory system (eg, in the dorsalhorn) and contribute to mechanical or cold allodynia inpatients with CRPS II.
The mechanisms of SMP in CRPS II (ie, after trauma withnerve lesion) are unlikely to be the same as those in CRPS I, inwhich only a small part of the coupling occurs in the skin. Wesuggest that an important sympathetic afferent couplingoccurs in the deep somatic tissues and that the mechanism ofthis coupling is indirect and involves the vascular bed andpossibly other non-neural components (figure 4). This way ofcoupling has been repeatedly postulated42–45 but has neverbeen explored experimentally in animal models.
Other potential ways of coupling between sympatheticneurons and afferent nociceptive neurons have beenidentified in animal experiments, but have not beenexplored in patients (figure 3). These modes of coupling donot involve activity in the sympathetic nerve fibres, but thesympathetic fibres may mediate the effects of inflammatory(eg, bradykinin) or other compounds (eg, nerve growthfactor) to nociceptive fibres in the peripheral tissue. Thissympathetic afferent coupling may turn out to be importantin inflammatory pain and in CRPS I.44,46–48
Finally, the sympathetic nervous system may be coupledwith nociceptive neurons via the adrenal medulla (figure 3).This mechanism has been inferred on the basis ofbehavioural experiments in rats that suggests thatepinephrine released by the adrenal medulla (during itsactivation by preganglionic neurons) causes sensitisation ofnociceptors for mechanical stimulation. The process ofsensitisation has a slow time course of days to 2 weeks todevelop fully.44,49–51
Pain relief from sympathetic blockadePain relief outlasts the conduction block of sympatheticneurons by at least one order of magnitude.52 Sometimes onlya few (in extreme cases, only one) temporary sympatheticblockades produce permanent pain relief. The long-lastingpain-relieving effects of sympathetic blockade suggest thatactivity in sympathetic neurons, which is of central origin,maintains a positive feedback circuit via the primary afferentneurons. Animal models for positive feedback circuits areabsent. We postulate that activity in sympathetic neuronsmaintains a central state of hyperexcitability (eg, of neurons inthe spinal dorsal horn), via excitation of afferent neuronsinitiated by an intense noxious event. The persistent afferentactivity needed to maintain such a central state ofhyperexcitability is probably low. This central state ofhyperexcitability is switched off during a temporary block ofconduction in the sympathetic chain lasting only a few hoursand cannot be switched on again when the block wears off andthe sympathetic activity (and therefore also thesympathetically-induced activity in afferent neurons) returns.
Review Complex regional pain syndrome
Nociceptiveterminal
BKB2 PGE
Dorsal root ganglion
Sympathetic Afferent
Lesioned nerve
Periphery
Nociceptiveterminal
NGFtrkA Inflammatory
mediators
Nociceptiveterminal
Sympathetic
Preganglionic
Epinephrine?
•Activity- dependent
•Via adrenoceptors•Via blood vessels
A
B
D
C
Figure 3. Possible couplings between sympathetic neurons and afferentneurons. Coupling with primary afferent neurons depends on activity inthe sympathetic neurons and the expression of functional adrenoceptorsby the afferent neurons, or is mediated indirectly via the blood vessels(blood flow). It can occur in the periphery, in the dorsal root ganglion, or,possibly, in the lesioned nerve (A). The inflammatory mediator bradykinin(BK) reacts with B2 receptors in the membrane of the sympatheticvaricosities, inducing release of prostaglandin E2 (PGE2; B). Nerve growthfactor (NGF) released during inflammation reacts with the high-affinityreceptor trkA for NGF in the membrane of the sympathetic varicosities,inducing release of an inflammatory mediator or inflammatory mediators(C). Activation of the adrenal medulla (AM) by sympathetic preganglionicneurons leads to release of a hormone (possibly adrenaline) (D).Reproduced with permission from Elsevier Science.44

For personal use. Only reproduce with permission from The Lancet.
THE LANCET Neurology Vol 2 November 2003 http://neurology.thelancet.com 691
Finally, unanimous assumption made isthat cutaneous (sympathetic andafferent) systems are mainly involved.However, sympathetic systems andafferent systems innervating deepsomatic tissues may be more importantin this hypothetical positive feedbackcircuit and need to be investigatedexperimentally (figure 2).21
Sympathetic systems andregulation in skin and deepsomatic tissuesIn CRPS, abnormalities related to thesympathetic nervous system includechanges of sweating and skin bloodflow.41,53–59 In the acute stages of CRPS Ithe affected limb is commonly warmerthan the contralateral limb.60
Hypohidrosis or, commonly in acutestages, hyperhidrosis are present inmany patients with CRPS I.
Evidence for a central autonomicdysregulationSympathetic denervation and mechan-isms of denervation hypersensitivitycannot account for vasomotor andsudomotor abnormalities in CRPS Ibecause there is no visible nerve lesion.61
In fact, there is direct evidence for areorganisation of central autonomiccontrol in these syndromes.
Resting sweat output, as well asthermoregulatory and axon reflexsweating, are increased in patients withCRPS I.54,57 Increased sweat productioncannot be caused by a peripheralmechanism because, unlike bloodvessels, sweat glands do not developdenervation supersensitivity.62
We have analysed centralsympathetic reflexes in cutaneoussympathetic vasoconstrictor innervationinduced by thermoregulatory (whole-body warming, cooling) and respiratorystimuli41,55,60 by the measuring of skintemperature and skin blood flow in thelimbs. In normal conditions thesereflexes do not show differencesbetween the two sides of the body(figure 5). In patients with CRPS threedistinct vascular regulation patterns were identified related tothe duration of the disorder.
In the warm regulation type (acute stage, <6 months),the affected limb was warmer and skin perfusion values werehigher than in the contralateral limb. Even massive bodycooling or respiratory stimuli did not activate sympatheticvasoconstrictor neurons.41 Norepinephrine concentrations
in the venous effluent above the area of pain were low in theaffected region.41,63,64 In the intermediate type, temperatureand perfusion were either high or low depending on thedegree of sympathetic activity. In the cold type (chronicstage), temperature and perfusion were low whilenorepinephrine concentration remained low on the affected side.60
ReviewComplex regional pain syndrome
Sympatheticfibres
A�
C
3
1
2
Varicosities
Macrophage
Macrophage
Macrophage
Mast cell
Afferentfibres
Receptiveendings
Capillaries
4
VenulesArterioles
SP
SP
NE
NE
NE
6
NK receptors
Sympathetic
Afferent
Adrenoceptors
5
TNF�
IL1
Figure 4. The microenvironment of primary afferents is thought to affect the properties of thereceptive endings of myelinated and unmyelinated afferent fibres. Top: the micromilieu depends onseveral interacting components: Neural activity in postganglionic noradrenergic fibres (1) supplyingblood vessels (2) causes release of noradrenaline (NA) and possibly other substances andvasoconstriction. Excitation of primary afferents (A�-fibres and C-fibres; 3) causes vasodilation inprecapillary arterioles and plasma extravasation in postcapillary venules (C-fibres only) by the releaseof substance P (SP) and other vasoactive compounds. Some of these effects may be mediated bynon-neuronal cells such as mast cells and macrophages (4). Other factors that affect the control ofthe microcirculation are the myogenic properties of arterioles (2) and more global environmentalinfluences such as a change of the temperature and the metabolic state of the tissue. Reproducedwith permission from John Wiley and Sons Ltd.45 Bottom: hypothetical relation between sympatheticnoradrenergic nerve fibres, peptidergic afferent nerve fibres, macrophages (5), and blood vessels(6). The activated and sensitised afferent nerve fibres activate macrophages (via substance Prelease). The immune cells start to release cytokines, such as tumour necrosis factor � (TNF �) andinterleukin 1 (IL 1) which further activate afferent fibres by enhancing sodium influx into the cells.Vasoactive compounds, released from the afferent nerve fibres, react with neurokinin 1 receptors inthe blood vessels (arteriolar vasodilation, venular plasma extravasation; neurogenic inflammation).

For personal use. Only reproduce with permission from The Lancet.
THE LANCET Neurology Vol 2 November 2003 http://neurology.thelancet.com692
The few microneurographic studies of small sympatheticnerve fascicles in patients with CRPS do not confirm thepresence of sympathetic reflex abnormalities. However,recordings were not done selectively from vasoconstrictorand sudomotor neurons. The analysis of skin sympatheticactivity might conceal subtle changes in selectivesympathetic channels.65,66
Mechanisms of autonomic dysregulationThe unilateral changes in thermoregulatory and respiration-related sympathetic reflex activity in patients with acuteCRPS I, seen as changes of cutaneous blood flow andtemperature, can only be attributed to central changes of thecutaneous vasoconstrictor system. These central changes arefully reversible after successful treatment of CRPS. However,secondary changes of neurovascular transmission that leadto development of supersensitivity of the vascular smoothmuscle, as a consequence of chronically decreased activity inthe vasoconstrictor neurons, may account for the severevasoconstriction and cold skin in chronic CRPS I.61 Thedensity of �-adrenoceptors is high in skin biopsy samplesfrom patients with CRPS I.67,68
We know neither where these central changes occur northe mechanisms behind them. However, because thechanges in patients are restricted to the affected side wepostulate that they occur in the spinal autonomic circuits. Asa consequence, descending systems that mediate signals tothese spinal autonomic circuits from supraspinal centresnormally involved in thermoregulation (eg, in thehypothalamus and brainstem) may no longer have access tothese spinal autonomic circuits that are linked to peripheralcutaneous vasoconstrictor pathways. This disruption to thesystem may also explain the dysregulation of sweat glands.Animal experiments indicate that experimental nerve lesions
lead to chronic (up to years) changes of chemoreceptor,baroreceptor, and nociceptor reflexes in cutaneousvasoconstrictor neurons but not in muscle vasoconstrictorneurons. The differentiation in reflex patterns betweenmuscle and cutaneous vasoconstrictor neurons39,40,69,70 is lostand cutaneous vasoconstrictor neurons tend to have reflexesthat are identical to those in muscle vasoconstrictorneurons.43,71–73
Somatomotor systemEvidence for motor abnormalities About 70% of patients with CRPS have weakness of allmuscles of the affected region and a decrease of active rangeof motion.74 Small accurate movements are typicallyimpaired. Nerve conduction and electromyography studiesare normal, except in patients in very chronic stages. Abouthalf of the patients have a postural or action tremor thatrepresents an increased amplitude of physiological tremor.75
In about 10% of patients dystonia of the affected hand orfoot develops.76,77 Furthermore, a neglect-like syndrome maylead to the disuse of the limb.32,78
Mechanisms involved in motor abnormalities The motor changes are unlikely to be related to a peripheralprocess (eg, influence of sympathetic nervous system onneuromuscular transmission or contractility of skeletalmuscle79,80). Because they are lateralised, these changes arepossibly related to changes in spinal reflex circuits linked tothe motor neurons (ie, they have a central origin). Motorchanges may be induced by the continuous nociceptiveinput. However, why these motor changes may disappearafter sympathetic blocks are given is unclear.75 There are noanimal models in which these motor changes can be studiedsystematically.
The results of kinematic analyses of target reaching aswell as grip force analysis to quantitatively assess motordeficits point to a cerebral abnormality in patients withCRPS.81 A pathological sensorimotor integration in theparietal cortex may induce abnormal central programmingand processing of motor tasks. Interestingly, the motorability was also slightly impaired on the contralateralunaffected side.82 A recent controlled study also supports adiscrepancy between central motor output and sensoryinput as underlying mechanism in CRPS. By use of a mirror,the visual input from a moving unaffected limb to the brainwas able to re-establish the pain-free relationship betweensensory feedback and motor execution. After 6 weeks oftherapy, pain and function were improved as compared withthe control group.83
Inflammation and oedema: role of the sympatheticnervous systemThe role of oedema and inflammation and their underlyingmechanisms in CRPS (in particular CRPS I) arecontroversial. Swelling is a very common symptom inpatients with acute CRPS and mostly extends far beyond theterritory of the trauma. The extent of swelling depends verycrucially on the aggravating stimuli and may decrease aftersympathetic blocks. These findings indicate that activity in
Review Complex regional pain syndrome
25 35
2
3
Diff
eren
ce in
tem
pera
ture
(ºC
)
1
0
30
Cooled WarmedSkin temperature (ºC)
Figure 5. Average absolute side differences in skin temperature in 25patients with CRPS I (circles), in 20 healthy controls (squares), and in 15control patients with extremity pain of other origin (triangles) during acontrolled change in cutaneous vasoconstrictor activity. The overallcutaneous sympathetic vasoconstrictor activity was estimated indirectlyby using the skin temperature on the unaffected side (or right side inhealthy controls) as reference value (see figure 2). A skin temperature onthe healthy side of 25°C indicates a high activity, a temperature of 30°C,an intermediate activity, and a temperature of 35°C a complete inhibitionof sympathetic vasoconstrictor activity to the skin. Reproduced withpermission from Oxford University Press.62
For personal use. Only reproduce with permission from The Lancet.
THE LANCET Neurology Vol 2 November 2003 http://neurology.thelancet.com 693
sympathetic neurons maintainsswelling;84 but the underlyingmechanism is unknown.
Capillary filtration pressure mightbe high owing to an imbalance of theactivity or pattern of activity betweenvasoconstrictor neurons innervatingprecapillary blood vessels andvasoconstrictor neurons innervatingpostcapillary blood vessels (veins).Venous congestion plethysmographyshowed that the hydrostatic pressureto achieve net capillary filtration washigh on the affected side in patientswith CRPS.85 However, venules andsmall deep veins are not or onlysparsely innervated by sympatheticnoradrenergic fibres (figure 4). Thus,the sympathetic fibres do not formclose contacts with the smooth musclecells of the venules as they do with theprecapillary resistance vessels.
Sympathetic fibres may be coupledto peptidergic unmyelinated fibres that lead to release of peptides withsubsequent precapillary vasodilationand postcapillary (venular) plasmaextravasation (neurogenic inflamma-tion; figure 4).
The idea that patients with CRPS Ihave inflammatory processes in theaffected region,86 in particular in thedeep somatic tissues including bones, goes back to Sudeck whobelieved that this syndrome is an inflammatory bone atrophy(“entzündliche Knochenatrophie”).13,14
Accordingly, bone scintigraphyrevealed periarticular tracer uptake inacute CRPS87 and synovia biopsies andscintigraphic investigations withradiolabelled immunoglobulins showedprotein extravasation, hypervascularityand neutrophil infiltration.88,89 Micro-dialysis through the skin revealed thatevoked neurogenic inflammationproduced by activation of peptidergicunmyelinated afferents is increased,90,91 and that lactateproduction is increased in the skin, which suggests thathypoxia increases the rate of anaerobic glycolysis.92 In the fluidof artificially produced skin blisters significantly higherconcentrations of interleukin 6 and tumour necrosis factor �were observed in the involved region.93,94 Furthermore, on thebasis of animal experiments it has been proposed that oxygen-derived free radicals cause increases in vascular permeability,soft tissue damage, and pain.95,96
Although there is some evidence that inflammatoryprocesses are involved in the pathogenesis of early CRPS, theexact mechanisms of initiation and maintenance of these
reactions are unclear. Animal studies have shown that thesympathetic nervous system can influence the intensity of aninflammatory process42,97–100 and clinical studies indicate thatsympatholytic procedures can ameliorate pain,inflammation, and oedema in human beings. However, thisconcept has yet to be proven in patients with CRPS.
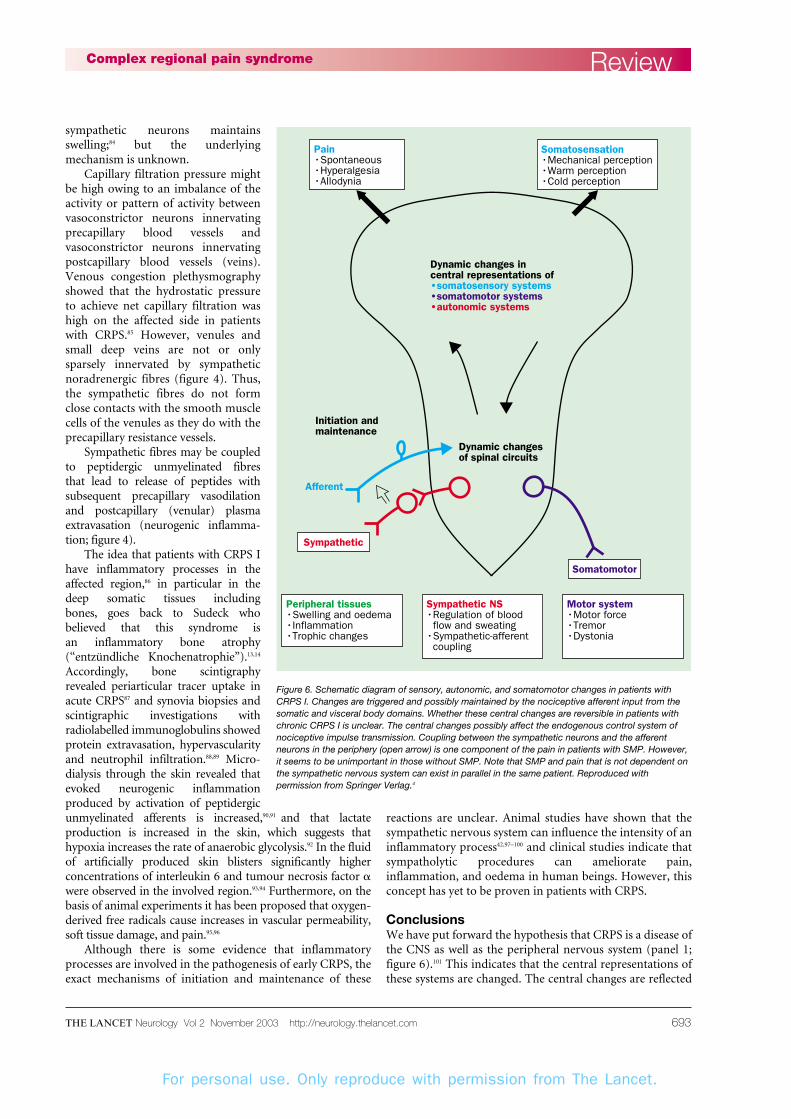
ConclusionsWe have put forward the hypothesis that CRPS is a disease ofthe CNS as well as the peripheral nervous system (panel 1;figure 6).101 This indicates that the central representations ofthese systems are changed. The central changes are reflected
ReviewComplex regional pain syndrome
Somatosensation•Mechanical perception•Warm perception•Cold perception
Peripheral tissues•Swelling and oedema edema•Inflammation•Trophic changes
Somatomotor
Sympathetic
Afferent
Initiation andmaintenance
Sympathetic NS•Regulation of blood flow and sweating•Sympathetic-afferent coupling
Motor system•Motor force•Tremor•Dystonia
Pain•Spontaneous•Hyperalgesia•Allodynia
Dynamic changes incentral representations of•somatosensory systems•somatomotor systems•autonomic systems
Dynamic changesof spinal circuits
Figure 6. Schematic diagram of sensory, autonomic, and somatomotor changes in patients withCRPS I. Changes are triggered and possibly maintained by the nociceptive afferent input from thesomatic and visceral body domains. Whether these central changes are reversible in patients withchronic CRPS I is unclear. The central changes possibly affect the endogenous control system ofnociceptive impulse transmission. Coupling between the sympathetic neurons and the afferentneurons in the periphery (open arrow) is one component of the pain in patients with SMP. However,it seems to be unimportant in those without SMP. Note that SMP and pain that is not dependent onthe sympathetic nervous system can exist in parallel in the same patient. Reproduced withpermission from Springer Verlag.4

For personal use. Only reproduce with permission from The Lancet.
THE LANCET Neurology Vol 2 November 2003 http://neurology.thelancet.com694
in changes of somatic sensations (including pain), of themotor system and of peripheral autonomically regulatedeffector systems (vasculature, sweat glands, inflammatorycells, etc) and argue that CRPS, particularly type I, is asystemic disease of these neuronal systems. The peripheralchanges cannot be seen independently of the central ones.Both systems interact with each other via the afferent andefferent signals. This view of CRPS indicates that thedisorder is not caused by just one system or just onemechanism (eg, sympathetic afferent coupling,adrenoceptor disease, peripheral inflammation, psycho-
genicity). We should also begin to understand how CRPStype I might develop after a trivial trauma, after a traumaremote from the affected region, and possibly afterimmobilisation of a limb. The multifactorial model of thedisease will explain why, in CRPS patients with SMP, a fewtemporary blocks of the sympathetic supply to the affectedregion sometimes lead to a long-lasting (even permanent)pain relief and to resolution of the other changes present inCRPS. Finally, it may help us to understand why somepatients with CRPS I develop neglect-like symptoms.
Future research and diagnostic classificationIntegration of the clinics and basic researchAs stated by Woolf and coauthors in 1998, “In creating amechanism-based classification (of pain) care must beexercised in extrapolating from animal models to clinicalmechanisms. Animal models are only approximations.Ultimately, it is advisable to align clinical and humanmodels with animal models to be certain of dissecting aparticular mechanism. Caution also needs to be exercisedwhen grouping people based on symptomatology and thentesting these people with a drug irrespective of theirunderlying disease. Once we identify mechanisms (ofpain), this should help the evolution of more uniformdescriptors for symptoms. A real challenge is to establishoperational criteria for distinct mechanisms.”102,103 Thistype of integrative research is a necessity if we are tounravel the mechanisms that operate in CRPS and if we areto find the organising pathophysiological principles thatorchestrate the different changes. It is essential that basicresearch in animal models (panel 2)101 and human beingsand clinical investigations of CRPS should be closelyaligned (figure 7). Even research in human beings is onlyan approximation to the clinical situation. Research onmechanisms in the models should concentrate onsymptoms but not on syndromes.
Review Complex regional pain syndrome
Hypotheses
Human patientClinical observations
Experimental observationsin patients
Behaviouralanimal models
Reducedanimal models
in vivo and in vitro
Figure 7. Integration of experimental human and animal models andclinical investigations in experimental research on mechanisms in CRPS.Reproduced with permission from IASP Press.101
Panel 1. The arguments for central and for peripheralchanges in CRPS
Central changes
Changes of regulation by sympathetic systemsThermoregulatory reflexes in cutaneous vasoconstriction neuronsreduced
Respiration elicited reflexes (deep in- and expiration) in cutaneousvasoconstriction reduced
Changes of activity in sudomotor neurons
Swelling reduced by sympathetic blocks
Sensory changesMechanical allodynia (quadrant, hemisensory)
Hypoaesthesia (mechanical, cold, warm; hemisensory, quadrant)
Somatomotor changesActive motor force reduced
Active range of motion reduced
Physiological tremor increased
Dystonia
Initiating eventsOut of proportion to pain disease (minor trauma)
Events remote from affected extremity (eg, in visceral domain)
Central (eg, after stroke; related to endogenous control systems?)
Pain relief by sympathetic blocks with local anaestheticsRelief of pain outlasts conduction block by an order of magnitude (ie, atemporary block is followed by a long-lasting pain relief)
A few temporary blocks are sometimes sufficient to generate permanentpain relief
Sympathetic activity maintains a positive feedback circuit (?)
Peripheral changes
Sympathetic afferent couplingAfter nerve lesion via norepinephrine and adrenoceptors (CRPS II)
Indirectly via vascular bed and other mechanisms (CRPS I; deepsomatic?)
Indirectly via inflammatory mediators and neurotrophic factors
Mediated by the adrenal medulla (epinephrine)
Inflammatory changes and oedemaNeurogenic inflammation (precapillary vasodilation, venular plasmaextravasation), involvement of peptidergic afferents (?)
Sympathetic fibres mediating effects of inflammatory mediators (eg,bradykinin) to venules leading to plasma extravasation (?)
Involvement of inflammatory cells and immune system (?)
Change of capillary filtration pressure (?)
Trophic changesLong-range consequences of inflammatory changes and oedema (?)
Direct (trophic?) effect of sympathetic and afferent fibres on tissue (?)

For personal use. Only reproduce with permission from The Lancet.
THE LANCET Neurology Vol 2 November 2003 http://neurology.thelancet.com 695
The long path approaching the CNSIn recent years, researchers concentrated on theinvestigation of peripheral mechanisms that underlie CRPS.We are now at a turning point after recognising thatimportant parts of the CRPS pathophysiology obviouslyinvolve the CNS. In the future we will fully understand theneurological components of CRPS and the effects they haveon several functional systems that are closely integrated,including the processing of cognitive and affectiveinformation.
Do genes predispose to CRPS?One of the unsolved features in human pain diseases is thatin patients with the same injury only a few patients developchronic pain. Similarly, in some nerve-lesion animalmodels, differences in pain susceptibility were caused bygenetic factors.104 To address this question in patients withCRPS, gene technology has been used to characterise thegenetic pattern of patients at risk of CRPS.105,106 In 52patients with CRPS, class I and II major histocompatibilityantigens were typed; the frequency of HLA-DQ1 wassignificantly high in patients.107 In patients with CRPS whoprogressed towards multifocal or generalised tonic dystonia,an association with HLA-DR13 was reported.108
Furthermore, a different locus, centromeric in HLA-class I,was found to be associated with spontaneous developmentof CRPS, suggesting an interaction between trauma severityand genetic factors that describe CRPS susceptibility.109
Diagnostic classificationThe definition of standardised diagnostic criteria for CRPSin 1994 was a major advance in the classification of regionalpain disorders associated with vasomotor or sudomotorabnormalities.9 On the basis of these criteria, clinicalresearch on mechanisms was done on much morehomogeneous groups of patients and studies were, for thefirst time, comparable. However, continuous improvementof the criteria based on results of systematic validationresearch is needed.110,111 The diagnostic criteria for CRPS areadequately sensitive (ie, they rarely miss a case of actualCRPS).112 However, both internal and external validationresearch suggests that CRPS is overdiagnosed.113,114 Theinclusion of motor and trophic signs and symptomsimproves specificity without losing much sensitivity.115 Theestablishment of such modified diagnostic criteria will havea huge effect on the quality of studies on pathophysiologicalmechanisms and therapy. Such a diversified researchstrategy on CRPS including diagnosis, mechanisms, andtherapy provides hope that we will ultimately be able tointervene successfully against this disease.
The variability in symptoms among patients with CRPSI/II makes it difficult to draw conclusions aboutmechanisms of the disorders based on clinical profiles andcould contribute to unclear findings in clinical trials. Strictpatient selection based on defined clinical criteria couldhelp to resolve this problem. Epidemiological studies mayalso help to elucidate the reasons for the variable incidencerates of CRPS in general, the different incidence ratesbetween women and men, and the differences between the
disease in children compared with adults. Furthermore,epidemiological studies may serve to work out prospectivestudies in order to find predictors for the development ofCRPS I/II.
Finally, whether clinical staging of patients is a validconcept is unclear. Individual patients probably do not passthrough the three stages as is still reported.3 At the time thenew taxonomy was developed, it was felt that staging was nolonger a useful concept for a diagnosis of the syndrome.
Future therapiesThe poor understanding of the underlyingpathophysiological abnormalities and the lack of objectivediagnostic criteria result in inherent difficulties of doingclinical trials of therapy. Therefore, only a few evidence-based treatment regimens for CRPS are available so far andoutcome studies find little consistent information regardingthe pharmacological agents and methods for treatment ofCRPS.116–118 Thus, treatment of CRPS is still largelyempirical. It should be immediate, pain free, and directedtoward restoration of full function of the region and includeneurologists, anaesthesiologists, orthopaedic surgeons,physiotherapists, and psychologists.
Authors’ contributionsWe both contributed equally to this review
Conflict of interestWe have no conflicts of interest
Role of the funding sourceOur work is supported by the Deutsche Forschungsgemeinschaft andby the Bundesministerium für Bildung und Forschung. No fundingsource had a role in the preparation of this review or the decision tosubmit it for publication.
ReviewComplex regional pain syndrome
Panel 2. Animal models of CRPS
Behavioural models
These models allow us to study pain-like behaviour quantitatively
following a standardised trauma with or without nerve lesion. We do not
have behavioural models that simulate pain in patients with CRPS I (for
critical discussion see 4,44,101).
Reduced animal models in vivo
These models allow us to study efferent (eg, sympathetic) or afferent
neurons, central neurons, changes of blood flow through tissues,
swelling, etc in anaesthetised animals that had undergone a
standardised trauma at variable time intervals before the measurements.
Reduced animal models in vitro
In these models isolated parts of an animal that had undergone a
standardised trauma are removed and investigated in vitro in order to
study the cellular mechanisms (eg, a dorsal-root ganglion, a skin-nerve-
preparation, a spinal-cord segment etc, or isolated afferent or
sympathetic cell bodies).
Search strategy and selection criteria
Data for this review were identified by searches ofMEDLINE and the authors’ own files.
For personal use. Only reproduce with permission from The Lancet.
THE LANCET Neurology Vol 2 November 2003 http://neurology.thelancet.com696
References1 Baron R, Jänig W. Pain syndromes with causal
participation of the sympathetic nervous system.Anaesthesist 1998; 47: 4–23.
2 Baron R, Wasner G. Complex regional painsyndromes. Curr Pain Headache Rep 2001; 5: 114–23.
3 Baron R, Fields HL, Jänig W, Kitt C, Levine JD.National Institutes of Health Workshop: reflexsympathetic dystrophy/complex regional painsyndromes: state-of-the-science. Anesth Analg 2002;95: 1812–16.
4 Jänig W, Baron R. Complex regional pain syndromeis a disease of the central nervous system.Clin Auton Res 2002; 12: 150–64.
5 Harden RN, Baron R, Jänig W. Complex regionalpain syndrome. Seattle: IASP Press, 2001.
6 Wasner G, Schattschneider J, Binder A, Baron R.Complex regional pain syndrome: diagnostic,mechanisms, CNS involvement and therapy. Spinal Cord 2003; 41: 61–75.
7 Evans JA. Reflex sympathetic dystrophy. Surg Clin North Am 1946; 26: 435–48.
8 Merskey H, Bogduk N. Classification of chronicpain: descriptions of chronic pain syndromes anddefinition of terms, 2nd edn. Seattle: IASP Press,1994.
9 Stanton-Hicks M, Jänig W, Hassenbusch S, HaddoxJD, Boas R, Wilson P. Reflex sympathetic dystrophy:changing concepts and taxonomy. Pain 1995;63: 127–33.
10 Mitchell SW. On a rare vaso-motor neurosis of theextremities, and on the maladies with which it maybe confounded. Am J Med Sci 1878; 76: 2–36.
11 Mitchell SW, Morehouse GR, Keen WW. Gunshotwounds and other injuries of nerves. New York:Lippincott JP, 1864.
12 Mitchell SW. Injuries of nerves and theirconsequences. New York: Lippincott JP, 1872.
13 Sudeck P. Über die akute (trophoneurotische)Knochenatrophie nach Entzündungen und Traumender Extremitäten. Deut Med Wschr 1902; 28: 336–42.
14 Sudeck P. Die trophische Extremitätenstörung durchperiphere (infektiöse und traumatische) Reize.Deutsch Zeitschr Chirurg 1931; 234: 596–612.
15 Leriche R. De la causalgie envisagée comme unenévrite du sympathique et de son traitement par ladénudation et l’excision des plexus nerveux péri-artériels. Presse Med 1916; 24: 178–80.
16 Leriche R. La Chirurgie de la Douleur. 3 ed. Paris:Masson, 1949.
17 Bonica JJ. Causalgia and other reflex sympatheticdystrophies. In: Bonica JJ, ed. The Management ofPain, vol 2. Philadelphia: Lea & Febiger, 1990:220–243.
18 Richards RL. Causalgia. A centennial review. Arch Neurol 1967; 16: 339–50.
19 Schwartzman RJ, McLellan TL. Reflex sympatheticdystrophy: a review. Arch Neurol 1987; 44: 555–61.
20 Stanton-Hicks M, Baron R, Boas R, et al. ComplexRegional Pain Syndromes: guidelines for therapy.Clin J Pain 1998; 14: 155–66.
21 Baron R, Schattschneider J, Binder A, Siebrecht D,Wasner G. Relation between sympatheticvasoconstrictor activity and pain and hyperalgesia incomplex regional pain syndromes: a case-controlstudy. Lancet 2002; 359: 1655–60.
22 Maleki J, LeBel AA, Bennett GJ, Schwartzman RJ.Patterns of spread in complex regional painsyndrome, type I (reflex sympathetic dystrophy).Pain 2000; 88: 259–66.
23 Price DD, Bennett GJ, Rafii A. Psychophysicalobservations on patients with neuropathic painrelieved by a sympathetic block. Pain 1989;36: 273–88.
24 Price DD, Long S, Huitt C. Sensory testing ofpathophysiological mechanisms of pain in patientswith reflex sympathetic dystrophy. Pain 1992;49: 163–73.
25 Sieweke N, Birklein F, Riedl B, Neundörfer B,Handwerker HO. Patterns of hyperalgesia incomplex regional pain syndrome. Pain 1999;80: 171–77.
26 Woolf CJ, Mannion RJ. Neuropathic pain: aetiology,symptoms, mechanisms, and management. Lancet1999; 353: 1959–64.
27 Rommel O, Malin JP, Zenz M, Jänig W. Quantitativesensory testing, neurophysiological andpsychological examination in patients with complexregional pain syndrome and hemisensory deficits.Pain 2001; 93: 279–93.
28 Rommel O, Gehling M, Dertwinkel R, et al.Hemisensory impairment in patients with complexregional pain syndrome. Pain 1999; 80: 95–101.
29 Thimineur M, Sood P, Kravitz E, Gudin J, Kitaj M.Central nervous system abnormalities in complex
regional pain syndrome (CRPS): clinical andquantitative evidence of medullary dysfunction. Clin J Pain 1998; 14: 256–67.
30 Fukumoto M, Ushida T, Zinchuk VS, Yamamoto H,Yoshida S. Contralateral thalamic perfusion inpatients with reflex sympathetic dystrophysyndrome. Lancet 1999; 354: 1790–91.
31 Juottonen K, Gockel M, Silen T, Hurri H, Hari R,Forss N. Altered central sensorimotor processing inpatients with complex regional pain syndrome. Pain2002; 98: 315–23.
32 Galer BS, Jensen M. Neglect–like symptoms incomplex regional pain syndrome: results of a self-administered survey. J Pain Symptom Manage 1999;18: 213–17.
33 Butler S. Disuse and CRPS. In: Harden RN, Baron R,Jänig W, eds. Complex regional pain syndrome.Seattle: IASP Press, 2001: 141–50.
34 Arnér S. Intravenous phentolamine test: diagnosticand prognostic use in reflex sympathetic dystrophy.Pain 1991; 46: 17–22.
35 Raja SN, Treede RD, Davis KD, Campbell JN.Systemic alpha-adrenergic blockade withphentolamine: a diagnostic test for sympatheticallymaintained pain. Anesthesiology 1991; 74: 691–98.
36 Schürmann M, Gradl G, Wizgal I, et al. Clinical andphysiologic evaluation of stellate ganglion blockadefor complex regional pain syndrome type I. Clin J Pain 2001; 17: 94–100.
37 Ali Z, Raja SN, Wesselmann U, Fuchs P, Meyer RA,Campbell JN. Intradermal injection ofnorepinephrine evokes pain in patients withsympathetically maintained pain. Pain 2000;88: 161–68.
38 Torebjörk E, Wahren L, Wallin G, Hallin R,Koltzenburg M. Noradrenaline-evoked pain inneuralgia. Pain 1995; 63: 11–20.
39 Jänig W, McLachlan EM. Characteristics offunction-specific pathways in the sympatheticnervous system. Trends Neurosci 1992; 15: 475–81.
40 Jänig W, McLachlan EM. Neurobiology of theautonomic nervous system. In: Mathias CJ,Bannister R, eds. Autonomic Failure, 4th edn.Oxford: Oxford University Press, 1999: 3–15.
41 Wasner G, Heckmann K, Maier C, Baron R.Vascular abnormalities in acute reflex sympatheticdystrophy (CRPS I): complete inhibition ofsympathetic nerve activity with recovery. Arch Neurol 1999; 56: 613–20.
42 Jänig W, Levine JD, Michaelis M. Interactions ofsympathetic and primary afferent neurons followingnerve injury and tissue trauma. Prog Brain Res 1996;113: 161–84.
43 Jänig W, Koltzenburg M. Plasticity of sympatheticreflex organization following cross-union ofinappropriate nerves in the adult cat. J Physiol 1991;436: 309–23.
44 Jänig W, Häbler HJ. Sympathetic nervous system:contribution to chronic pain. Prog Brain Res 2000;129: 451–68.
45 Jänig W, Koltzenburg M. What is the interactionbetween the sympathetic terminal and the primaryafferent fiber? In: Basbaum AI, Besson J-M, eds.Towards a New Pharmacotherapy of Pain, DahlemWorkshop Reports. Chichester: John Wiley andSons, 1991: 331–352.
46 Jänig W, Levine JD, Michaelis M. Interactions ofsympathetic and primary afferent neurons followingnerve injury and tissue trauma. Prog Brain Res 1996;113: 161–84.
47 Woolf CJ, Ma QP, Allchorne A, Poole S. Peripheralcell types contributing to the hyperalgesic action ofnerve growth factor in inflammation. J Neurosci1996; 16: 2716–23.
48 McMahon SB. NGF as a mediator of inflammatorypain. Philos Trans R Soc Lond B Biol Sci 1996;351: 431–40.
49 Khasar SG, Miao FJ-P, Jänig W, Levine JD.Vagotomy-induced enhancement of mechanicalhyperalgesia in the rat is sympathoadrenal-mediated.J Neurosci 1998; 18: 3043–49.
50 Khasar SG, Miao FJ-P, Jänig W, Levine JD.Modulation of bradykinin-induced mechanicalhyperalgesia in the rat skin by activity in theabdominal vagal afferents. Eur J Neurosci. 1998;10: 435–44.
51 Jänig W, Khasar SG, Levine JD, Miao FJ. The role ofvagal visceral afferents in the control of nociception.Prog Brain Res 2000; 122: 273–87.
52 Price DD, Long S, Wilsey B, Rafii A. Analysis of peakmagnitude and duration of analgesia produced bylocal anesthetics injected into sympathetic ganglia ofcomplex regional syndrome patients. Clin J Pain1998; 14: 216–26.
53 Low PA, Amadio PC, Wilson PR, McManis PG,Willner CL. Laboratory findings in reflex
sympathetic dystrophy: a preliminary report. Clin J Pain 1994; 10: 235–39.
54 Chelimsky TC, Low PA, Naessens JM, Wilson PR,Amadio PC, O´Brien PC. Value of autonomic testingin reflex sympathetic dystrophy. Mayo Clin Proc1995; 70: 1029–40.
55 Baron R, Maier C. Reflex sympathetic dystrophy:skin blood flow, sympathetic vasoconstrictor reflexesand pain before and after surgical sympathectomy.Pain 1996; 67: 317–26.
56 Baron R, Blumberg H, Jänig W. Clinicalcharacteristics of patients with complex regionalpain syndromes in Germany with special emphasison vasomotor function. In: Jänig W, Stanton-HicksM, eds. Progress in pain research and management,vol 6, Reflex sympathetic dystrophy: a reappraisal.Seattle: IASP Press, 1996.
57 Birklein F, Sittle R, Spitzer A, Claus D, NeundörferB, Handwerker HO. Sudomotor function insympathetic reflex dystrophy. Pain 1997; 69: 49–54.
58 Birklein F, Riedl B, Neundörfer B, Handwerker HO.Sympathetic vasoconstrictor reflex pattern inpatients with complex regional pain syndrome. Pain 1998; 75: 93–100.
59 Wasner G, Backonja MM, Baron R. Traumaticneuralgias: complex regional pain syndromes (reflexsympathetic dystrophy and causalgia): clinicalcharacteristics, pathophysiological mechanisms andtherapy. Neurol Clin 1998; 16: 851–68.
60 Wasner G, Schattschneider J, Heckmann K, Maier C,Baron R. Vascular abnormalities in reflexsympathetic dystrophy (CRPS I): mechanisms anddiagnostic value. Brain 2001; 124: 587–99.
61 Goldstein DS, Tack C, Li ST. Sympatheticinnervation and function in reflex sympatheticdystrophy. Ann Neurol 2000; 48: 49–59.
62 Fleming WW, Westfall DP. Adaptivesupersensitivity. In: Trendelenburg U, Weiner N,eds. Handbook of experimental pharmacology, vol90/I: catecholamines. New York: Springer Verlag,1988: 509–59.
63 Drummond PD, Finch PM, Smythe GA. Reflexsympathetic dystrophy: the significance of differingplasma catecholamine concentrations in affected andunaffected limbs. Brain 1991; 114: 2025–36.
64 Harden RN, Duc TA, Williams TR, Coley D, Cate JC, Gracely RH. Norepinephrine andepinephrine levels in affected versus unaffected limbsin sympathetically maintained pain. Clin J Pain 1994;10: 324–30.
65 Casale R, Elam M. Normal sympathetic nerveactivity in a reflex sympathetic dystrophy withmarked skin vasoconstriction. J Auton Nerv Syst1992; 41: 215–19.
66 Torebjörk E. Clinical and neurophysiologicalobservations relating to pathophysiologicalmechanisms of reflex sympathetic dystrophy. In:Stanton-Hicks M, Jänig W, Boas RA, eds. Reflexsympathetic dystrophy. Dordrecht: Kluwer, 1989:71–80.
67 Drummond PD, Skipworth S, Finch PM. Alpha 1-adrenoceptors in normal and hyperalgesic humanskin. Clin Sci (London) 1996; 91: 73–77.
68 Arnold JM, Teasell RW, MacLeod AP, Brown JE,Carruthers SG. Increased venous alpha-adrenoceptor responsiveness in patients with reflexsympathetic dystrophy. Ann Intern Med 1993;118: 619–21.
69 Jänig W, Häbler HJ. Organization of the autonomicnervous system: structure and function. In: VinkenPJ, Bruyn GW, eds. Handbook of clinical neurology.Amsterdam: Elsevier, 1999: 1–52.
70 Jänig W, Häbler HJ. Neurophysiological analysis oftarget-related sympathetic pathways: from animal tohuman: similarities and differences. Acta Physiol Scand 2003; 177: 255–74.
71 Blumberg H, Jänig W. Changes of reflexes invasoconstrictor neurons supplying the cat hindlimbfollowing chronic nerve lesions: a model for studyingmechanisms of reflex sympathetic dystrophy? J Auton Nerv Syst 1983; 7: 399–411.
72 Blumberg H, Jänig W. Reflex patterns inpostganglionic vasoconstrictor neurons followingchronic nerve lesions. J Auton Nerv Syst 1985;14: 157–80.
73 Jänig W, McLachlan EM. The role of modificationsin noradrenergic peripheral pathways after nervelesions in the generation of pain. In: Fields HL,Liebeskind JC, eds. Pharmacological approaches tothe treatment of pain: new concepts and criticalissues. Progress in pain research and mangement.Seattle: IASP Press, 1994: 101–128.
74 Schwartzman RJ, Kerrigan J. The movementdisorder of reflex sympathetic dystrophy. Neurology1990; 40: 57–61.
75 Deuschl G, Blumberg H, Lücking CH. Tremor in
Review Complex regional pain syndrome

For personal use. Only reproduce with permission from The Lancet.
THE LANCET Neurology Vol 2 November 2003 http://neurology.thelancet.com 697
reflex sympathetic dystrophy. Arch Neurol 1991;48: 1247–52.
76 Bhatia KP, Bhatt MH, Marsden CD. The causalgia-dystonia syndrome. Brain 1993; 116: 843–51.
77 Marsden CD, Obeso JA, Traub MM, Rothwell JC,Kranz H, La Cruz F. Muscle spasms associated withSudeck’s atrophy after injury. BMJ (Clin Res Ed)1984; 288: 173–76.
78 Galer BS, Butler S, Jensen MP. Case reports andhypothesis: a neglect-like syndrome may beresponsible for the motor disturbance in reflexsympathetic dystrophy (complex regional painsyndrome-1). J Pain Symptom Manage 1995;10: 385–91.
79 Jänig W, Koltzenburg M. Possible ways ofsympathetic afferent interactions. In: Jänig W,Schmidt RF, eds. Reflex sympathetic dystrophy:pathophysiological mechanisms and clinicalimplications. Weinheim: VCH Verlagsgesellschaft,1992: 213–45.
80 Jänig W. Organization of the lumbar sympatheticoutflow to skeletal muscle and skin of the cathindlimb and tail. Rev Physiol Biochem Pharmacol1985; 102: 119–213.
81 Schattschneider J, Wenzelburger R, Deuschl G,Baron R. Kinematic analysis of the upper extremityin CRPS. In: Harden RN, Baron R, Jänig W, eds.Complex regional pain syndrome. Seattle: IASPPress, 2001: 119–128.
82 Ribbers GM, Mulder T, Geurts AC, den Otter RA.Reflex sympathetic dystrophy of the left hand andmotor impairments of the unaffected right hand:impaired central motor processing? Arch Phys MedRehabil 2002; 83: 81–85.
83 McCabe CS, Haigh RC, Ring EF, Halligan PW, WallPD, Blake DR. A controlled pilot study of the utilityof mirror visual feedback in the treatment ofcomplex regional pain syndrome (type 1).Rheumatology 2003; 42: 97–101.
84 Blumberg H, Hoffmann U, Mohadjer M, ScheremetR. Clinical phenomenology and mechanisms ofreflex sympathetic dystrophy: emphasis on edema.In: Gebhart GF, Hammond DL, Jensen TS, eds.Proceedings of the 7th World Congress on Pain.Seattle: IASP Press, 1994: 455–481.
85 Schürmann M, Zaspel J, Gradl G, Wipfel A, Christ F.Assessment of the peripheral microcirculation usingcomputer-assisted venous congestionplethysmography in post-traumatic complexregional pain syndrome type I. J Vasc Res 2001; 38:453–61.
86 Kingery WS, Davies MF, Clark JD. A substance Preceptor (NK(1)) antagonist can reverse vascular andnociceptive abnormalities in a rat model of complexregional pain syndrome type II. Pain 2003; 104:75–84.
87 Leitha T, Korpan M, Staudenherz A,Wunderbaldinger P, Fialka V. Five phase bonescintigraphy supports the pathophysiological
concept of a subclinical inflammatory process inreflex sympathetic dystrophy. Q J Nucl Med 1996;40: 188–93.
88 Renier JC, Arlet J, Bregeon C, et al. The joint inalgodystrophy: joint fluid, synovium, cartilage. Rev Rhum Mal Osteoarthr 1983; 50: 255–60.
89 Oyen WJ, Arntz IE, Claessens RM, Van der MeerJW, Corstens FH, Goris RJ. Reflex sympatheticdystrophy of the hand: an excessive inflammatoryresponse? Pain 1993; 55: 151–57.
90 Weber M, Birklein F, Neundörfer B, Schmelz M.Facilitated neurogenic inflammation in complexregional pain syndrome. Pain 2001; 91: 251–57.
91 Birklein F, Schmelz M, Schifter S, Weber M. The important role of neuropeptides in complexregional pain syndrome. Neurology 2001;57: 2179–84.
92 Birklein F, Weber M, Neundörfer B. Increased skinlactate in complex regional pain syndrome: evidencefor tissue hypoxia? Neurology 2000; 55: 1213–5.
93 Huygen FJ, de Bruijn AG, Klein J, Zijlstra FJ.Neuroimmune alterations in the complex regionalpain syndrome. Eur J Pharmacol 2001; 429: 101–13.
94 Huygen FJ, De Bruijn AG, De Bruin MT, GroenewegJG, Klein J, Zijistra FJ. Evidence for localinflammation in complex regional pain syndrometype 1. Mediators Inflamm 2002; 11: 47–51.
95 Goris RJ. Reflex sympathetic dystrophy: model of asevere regional inflammatory response syndrome.World J Surg 1998; 22: 197–202.
96 van der Laan L, Goris RJ. Reflex sympatheticdystrophy: an exaggerated regional inflammatoryresponse? Hand Clin 1997; 13: 373–85.
97 Perl ER. Cutaneous polymodal receptors:characteristics and plasticity. Prog Brain Res 1996;113: 21–37.
98 Miao FJ-P, Green PG, Coderre TJ, Jänig W, LevineJD. Sympathetic-dependence in bradykinin-inducedsynovial plasma extravasation is dose-related.Neurosci Lett 1996; 205: 165–68.
99 Miao FJ, Jänig W, Levine JD. Role of sympatheticpostganglionic neurons in synovial plasmaextravasation induced by bradykinin. J Neurophysiol1996; 75: 715–24.
100 Levine JD, Dardick SJ, Basbaum AI, Scipio E. Reflexneurogenic inflammation. I. Contribution of theperipheral nervous system to spatially remoteinflammatory responses that follow injury. J Neurosci1985; 5: 1380–86.
101 Jänig W, Baron R. The role of the sympatheticnervous system in neuropathic pain: clinicalobservations and animal models. In: Hansson PT,Fields HL, Hill RG, Marchettini P, eds. Neuropathicpain: pathophysiology and treatment. Seattle: IASPPress, 2001: 125–149.
102 Woolf CJ, Bennett GJ, Doherty M, et al. Towards amechanism-based classification of pain? Pain 1998;77: 227–29.
103 Jensen TS, Baron R. Translation of symptoms and
signs into mechanisms in neuropathic pain. Pain2003; 102: 1–8.
104 Mogil JS, Wilson SG, Bon K, et al. Heritability ofnociception I: responses of 11 inbred mouse strainson 12 measures of nociception. Pain 1999; 80: 67–82.
105 Mailis A, Wade J. Profile of Caucasian women withpossible genetic predisposition to reflex sympatheticdystrophy: a pilot study. Clin J Pain 1994;10: 210–17.
106 Mailis A, Wade J. Genetic considerations in CRPS.In: Harden RN, Baron R, Jänig W, eds. Complexregional pain syndrome. Seattle: IASP Press, 2001:227–38.
107 Kemler MA, van de Vusse AC, van den Berg-LoonenEM, Barendse GA, van Kleef M, Weber WE. HLA-DQ1 associated with reflex sympathetic dystrophy.Neurology 1999; 53: 1350–51.
108 van Hilten JJ, van de Beek WJ, Roep BO. Multifocalor generalized tonic dystonia of complex regionalpain syndrome: a distinct clinical entity associatedwith HLA–DR13. Ann Neurol 2000; 48: 113–16.
109 van de Beek WJ, Roep BO, van der Slik AR, GiphartMJ, van Hilten BJ. Susceptibility loci for complexregional pain syndrome. Pain 2003; 103: 93–97.
110 van de Beek WJ, Schwartzman RJ, van Nes SI,Delhaas EM, van Hilten JJ. Diagnostic criteria usedin studies of reflex sympathetic dystrophy. Neurology2002; 58: 522–6.
111 van de Vusse AC, Stomp-van den Berg SG, de Vet HC, Weber WE. Interobserver reliability ofdiagnosis in patients with complex regional painsyndrome. Eur J Pain 2003; 7: 259–65.
112 Perez RS, Burm PE, Zuurmond WW, et al. Interraterreliability of diagnosing complex regional painsyndrome type I. Acta Anaesthesiol Scand 2002;46: 447–50.
113 Harden RN, Bruehl S, Galer BS, et al. Complexregional pain syndrome: are the IASP diagnosticcriteria valid and sufficiently comprehensive? Pain1999; 83: 211–19.
114 Bruehl S, Harden RN, Galer BS, et al. Externalvalidation of IASP diagnostic criteria for complexregional pain syndrome and proposed researchdiagnostic criteria. Pain 1999; 81: 147–54.
115 Bruehl S, Harden RN, Galer BS, Saltz S, Backonja M,Stanton-Hicks M. Complex regional pain syndrome:are there distinct subtypes and sequential stages ofthe syndrome? Pain 2002; 95: 119–24.
116 Kingery WS. A critical review of controlled clinicaltrials for peripheral neuropathic pain and complexregional pain syndromes. Pain 1997; 73: 123–39.
117 Perez RS, Kwakkel G, Zuurmond WW, de Lange JJ.Treatment of reflex sympathetic dystrophy (CRPStype 1): a research synthesis of 21 randomizedclinical trials. J Pain Symptom Manage 2001;21: 511–26.
118 Forouzanfar T, Koke AJ, van Kleef M, Weber WE.Treatment of complex regional pain syndrome typeI. Eur J Pain 2002; 6: 105–22.
ReviewComplex regional pain syndrome


















