
Hemophagocytose Activation macrophagique Activation lympho-histiocytaire « Hemophagocytic syndrome »
Complement activation and regulation
Seppo Meri, Haartman Institute
University of Helsinki, FinlandDubrovnik
3.10.2010
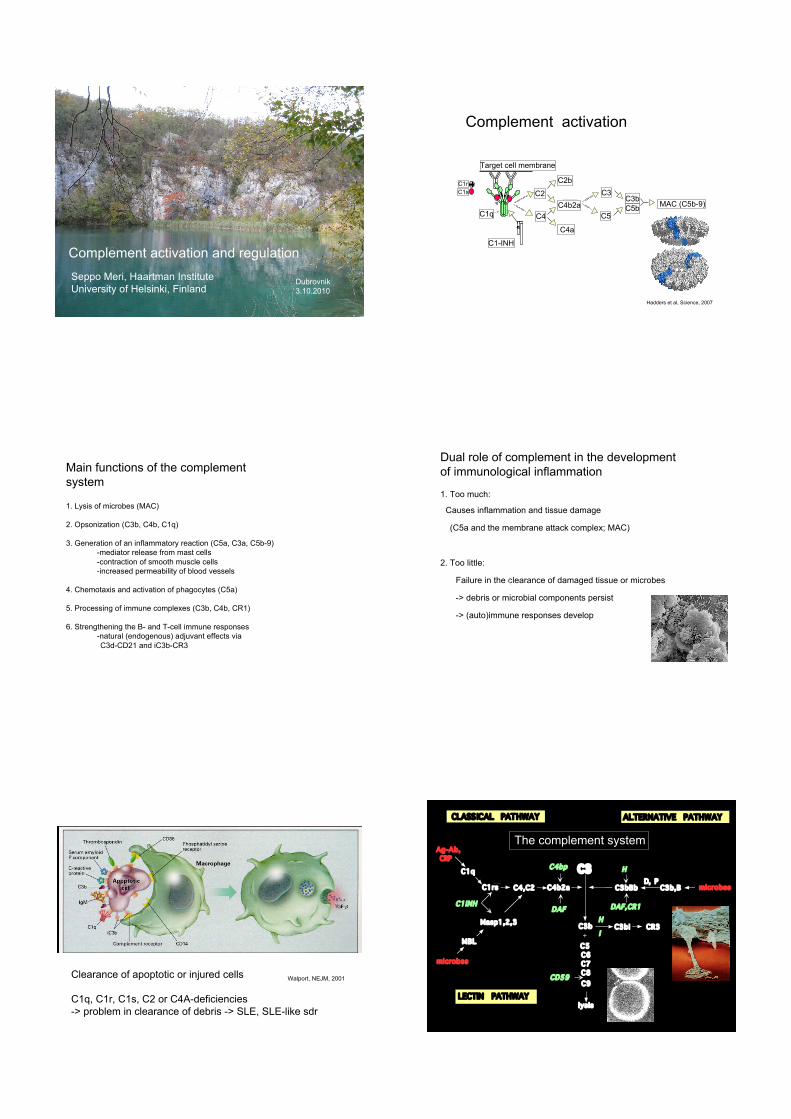
C4
C2 C3C3b
C5
C4b2aC1q
C1-INH
MAC (C5b-9)C5b
Target cell membrane
C2b
C4a
C1r
C1s
Complement activation
Hadders et al, Science, 2007
Main functions of the complement
system
1. Lysis of microbes (MAC)
2. Opsonization (C3b, C4b, C1q)
3. Generation of an inflammatory reaction (C5a, C3a, C5b-9)
-mediator release from mast cells
-contraction of smooth muscle cells
-increased permeability of blood vessels
4. Chemotaxis and activation of phagocytes (C5a)
5. Processing of immune complexes (C3b, C4b, CR1)
6. Strengthening the B- and T-cell immune responses
-natural (endogenous) adjuvant effects via
C3d-CD21 and iC3b-CR3
Dual role of complement in the development
of immunological inflammation
1. Too much:
Causes inflammation and tissue damage
(C5a and the membrane attack complex; MAC)
2. Too little:
Failure in the clearance of damaged tissue or microbes
-> debris or microbial components persist
-> (auto)immune responses develop
Walport, NEJM, 2001Clearance of apoptotic or injured cells
C1q, C1r, C1s, C2 or C4A-deficiencies
-> problem in clearance of debris -> SLE, SLE-like sdr
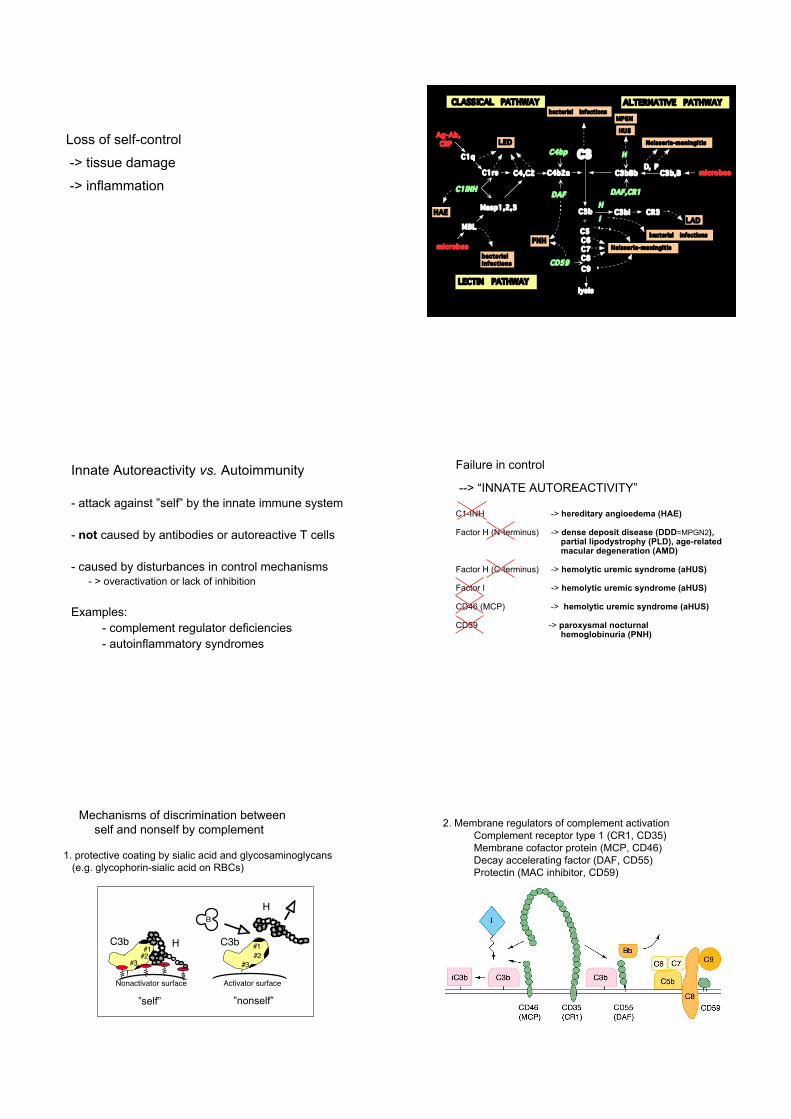
C4,C2
C3
C3bBb C3b,B
ALTERNATIVE PATHWAY
C3b
C5
C6
C7
C8
lysis
C4b2a
Ag-Ab,
CRP
CR3
C9
C3bi+
D, P
C1q
MBL
C1rs microbes
microbes
LECTIN PATHWAY
CLASSICAL PATHWAY
Masp1,2,3 H
CD59
I
C1INH
H
DAF
C4bp
DAF,CR1
The complement system
Loss of self-control
-> tissue damage
-> inflammationC4,C2
C3
C3bBb C3b,B
ALTERNATIVE PATHWAY
C3b
C5
C6
C7
C8
lysis
C4b2a
Ag-Ab,
CRP
CR3
C9
C3bi+
D, P
C1q
MBL
C1rs microbes
microbes
LECTIN PATHWAY
CLASSICAL PATHWAY
Masp1,2,3 H
CD59
I
C1INH
H
DAF
C4bp
DAF,CR1
Neisseria-meningitis
MPGN
LED
bacterial infections
PNH
HAE
bacterial
infections
LAD
Neisseria-meningitis
HUS
bacterial infections
Innate Autoreactivity vs. Autoimmunity
- attack against ”self” by the innate immune system
- not caused by antibodies or autoreactive T cells
- caused by disturbances in control mechanisms - > overactivation or lack of inhibition
Examples:
- complement regulator deficiencies
- autoinflammatory syndromes
Failure in control
--> “INNATE AUTOREACTIVITY”
C1-INH -> hereditary angioedema (HAE)
Factor H (N-terminus) -> dense deposit disease (DDD=MPGN2), partial lipodystrophy (PLD), age-related macular degeneration (AMD)
Factor H (C-terminus) -> hemolytic uremic syndrome (aHUS)
Factor I -> hemolytic uremic syndrome (aHUS)
CD46 (MCP) -> hemolytic uremic syndrome (aHUS)
CD59 -> paroxysmal nocturnal hemoglobinuria (PNH)
Mechanisms of discrimination between
self and nonself by complement
1. protective coating by sialic acid and glycosaminoglycans
(e.g. glycophorin-sialic acid on RBCs)
–––––
#1
#2#1
#2
Nonactivator surface Activator surface
#3 #3
C3b H C3b
H
B
”self” ”nonself”
2. Membrane regulators of complement activation
Complement receptor type 1 (CR1, CD35)
Membrane cofactor protein (MCP, CD46)
Decay accelerating factor (DAF, CD55)
Protectin (MAC inhibitor, CD59)

7 8 11 12 20
++ ++++
131 144FH
C3b CRP C3c C3d
DDD(MPGN2)
Complement factor H
Heparin
C3b
CRP
Binding sites:
++• soluble plasma protein
• consists of 20 short consensus
repeat (SCR, ”sushi”) domains
• inhibitor of the alternative pathway of complementGros et al, Nature Rev Immunol, 2007
Cleavage of complement C3
+
Factor H
H + I
Discrimination between activators
and nonactivators (“nonself-self”)
X = any surface, A = activator, NA = nonactivator
Dense Deposit Disease(Membranoproliferative
glomerulonephritis type 2)
1.Caused by total deficiency or
functional blocking of the N-
terminus of factor H (SCR1-5)
(or by anti-C3bBb = C3 Nef
or by anti-H antibody)
2. Glomerular damage is due to
continuous activation of the
alternative pathway
3. Leads to C3 & MAC deposition
and dense deposits on GBM
C3b
Meri et al, J Exp Med, 1992
7 8 11 12 20
++
++++
131 144FH
C3b
CRP
C3c C3d
Complement factor H
Heparin
C3b
CRP
Binding sites:
++
CRP binding region
I II
CRP = C-reactive protein
Factor H and AMD
• Science Vol. 308 15
April 2005
Age-related Macular Degeneration
• The most common cause of
blindness in the developed countries
in people over 65
• Loss of central vision
• E.g. reading, driving and recognising
faces impossible in advanced AMD
• Associated with a SNP (1277T!C)
that leads to one amino acid change:
Y402H in SCR7 of FH
• No curative treatment
normal vision
AMD
Age-related macular
degeneration
Y402H change in factor H
leads to reduced binding
of CRP
Genotypes in
46 AMD patients and
33 controls
!TT
!TC (2.7x risk)*
!CC (9.7x risk)*
*Seitsonen et al, Mol Vision, 2006
Laine et al, J Immunol, 2007
402H
402H
Binding of
FH to CRP
Laine et al, J Immunol 2007
Tyr402His
7 8 11 12 20
++ ++++
131 144FH
C3b CRP C3c C3d Hotspot for
mutations
in HUS
Complement factor H and hemolytic uremic syndrome
1. Familial HUS: a non-diarrheal form
2. Microangiopathic hemolytic anemia, thrombocytopenia and
acute renal failure
3. Thrombotic microangiopathy due to vessel wall thickening and
swelling and detachment of endothelial cells from the basement
membrane
4. Caused by point mutations in MCP, FI, (FB) or in the C-terminus of FH
(SCR19-20) -> dysfunctional or low levels of factor H
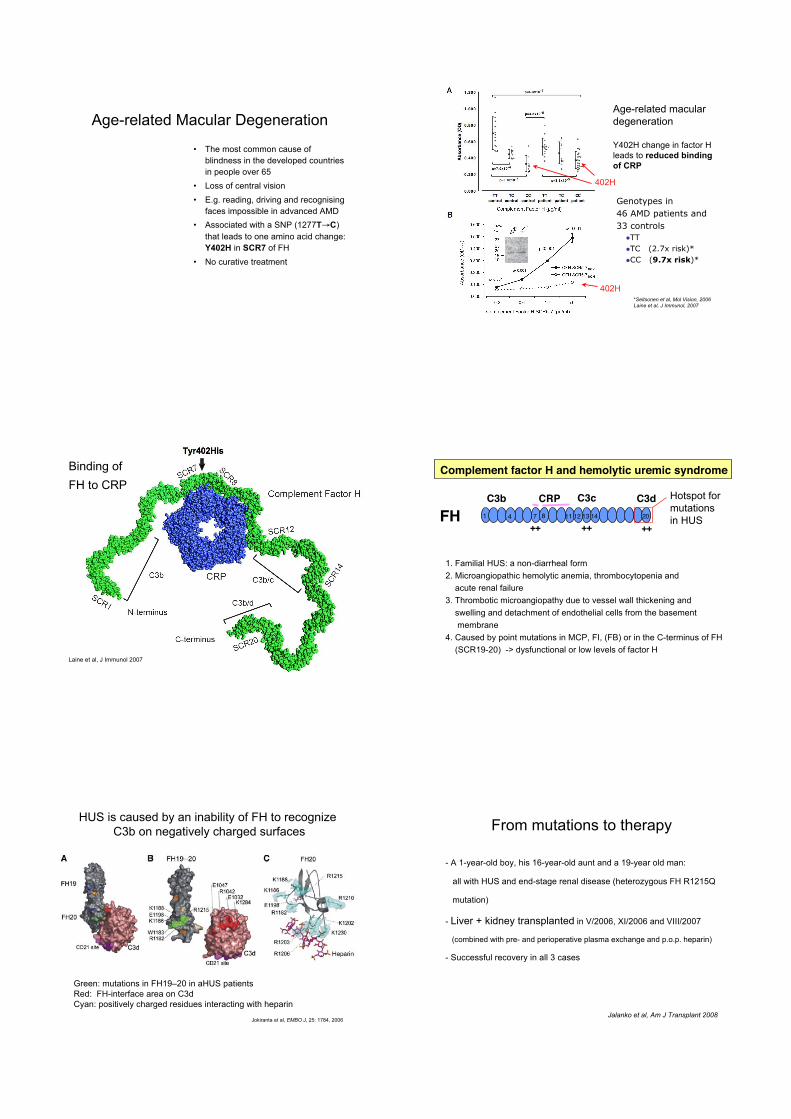
Green: mutations in FH19–20 in aHUS patients
Red: FH-interface area on C3d
Cyan: positively charged residues interacting with heparin
Jokiranta et al, EMBO J, 25: 1784, 2006
HUS is caused by an inability of FH to recognize
C3b on negatively charged surfaces From mutations to therapy
- A 1-year-old boy, his 16-year-old aunt and a 19-year old man:
all with HUS and end-stage renal disease (heterozygous FH R1215Q
mutation)
- Liver + kidney transplanted in V/2006, XI/2006 and VIII/2007
(combined with pre- and perioperative plasma exchange and p.o.p. heparin)
- Successful recovery in all 3 cases
Jalanko et al, Am J Transplant 2008
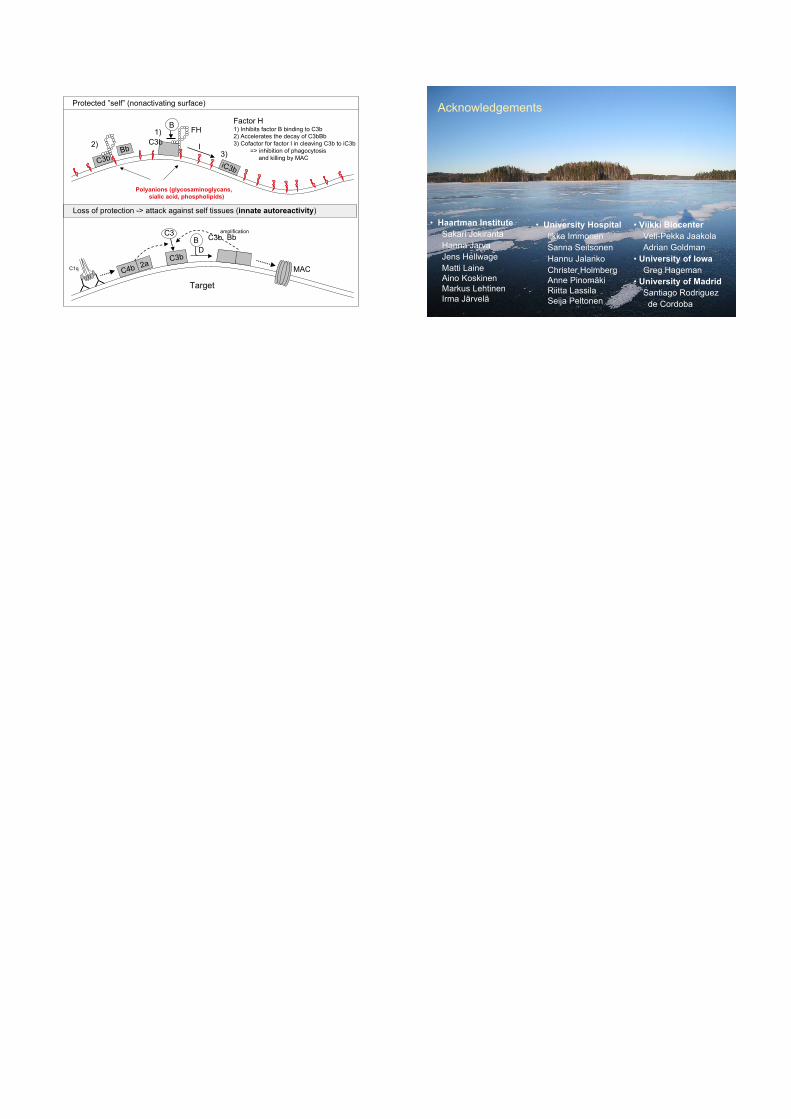
Protected ”self” (nonactivating surface)
iC3b
C3b
FHB
C3b
Polyanions (glycosaminoglycans,
sialic acid, phospholipids)
I
1)
2)
3)
Factor H1) Inhibits factor B binding to C3b
2) Accelerates the decay of C3bBb
3) Cofactor for factor I in cleaving C3b to iC3b
=> inhibition of phagocytosis
and killing by MAC
Bb
Loss of protection -> attack against self tissues (innate autoreactivity)
C3
C1q
B
Target
MAC
C3bD
C4b 2aC3b Bb
amplification
Acknowledgements
• Haartman Institute
Sakari Jokiranta
Hanna Jarva
Jens Hellwage
Matti Laine
Aino Koskinen
Markus Lehtinen
Irma Järvelä
• University Hospital
Ilkka Immonen
Sanna Seitsonen
Hannu Jalanko
Christer Holmberg
Anne Pinomäki
Riitta Lassila
Seija Peltonen
• Viikki Biocenter
Veli-Pekka Jaakola
Adrian Goldman
• University of Iowa
Greg Hageman
• University of Madrid
Santiago Rodriguez
de Cordoba


















