
Competency Based Education in General Internal...
32
DR. SHARON E CARD DIVISION OF GENERAL INTERNAL MEDICINE UNIVERSITY OF SASKATCHEWAN DR. NARMIN KASSAM DIVISION OF GENERAL INTERNAL MEDICINE UNIVERSITY OF ALBERTA Competency Based Education in General Internal Medicine
Transcript of Competency Based Education in General Internal...

D R . S H A R O N E C A R D D I V I S I O N O F G E N E R A L I N T E R N A L M E D I C I N E
U N I V E R S I T Y O F S A S K A T C H E W A N
D R . N A R M I N K A S S A M D I V I S I O N O F G E N E R A L I N T E R N A L M E D I C I N E
U N I V E R S I T Y O F A L B E R T A
Competency Based Education in General Internal Medicine

FOR POSTING
Many slides courtesy of but remain property of the Royal College.
Any dissemination should include recognition of source and authorship.

DISCLOSURES
Extensive work with the Royal College of Physicians and Surgeons of Canada (RCPSC).
Many slides courtesy of the RCPSC. Chair/Vice-Chair of General Internal Medicine
Specialty Committee, Royal College of Physicians and Surgeons of Canada.
Have served on numerous Royal College of Physicians and Surgeons of Canada Committees.
Have accepted honorariums from The Medical Council of Canada.

Help Us Spread the News
This presentation has been developed for your use:
• Share and/or incorporate these slides as needed, simply source the Royal College
• All text, images and logos contained herein are the property of Royal College of Physicians and Surgeons of Canada
Questions? Email [email protected]
4

Learning Outcomes
1. Define competency based education. 2. Define Entrustable Professional Activities. 3. Determine essential outcomes of a graduate of a
GIM Subspecialty program. 4. Outline pathways to success in achieving essential
outcomes in GIM Subspecialty programs.

Introductions

Needs Assessment
Competence by Design is: A. The new trend in interior decorating. B. A way to ensure all training will be completed faster. C. A new kind of OSCE. D. Designed to address societal health needs and patient
outcomes.

Needs Assessment
An EPA is: A. Entrustable Professional Activity B. Entry Practical Ant C. Enemy of the Professional Accountant D. Early Professional Acts

What is Competence by Design(CBD)?
Multi-year, transformational change initiative in specialty medical education;
Focused on the learning continuum from the start of residency to retirement;
Based on a competency model of education and assessment; and
Designed to address societal health need and patient outcomes.
9

CBD Identified Initiatives
CanMEDS 2015
Assessment
Lifelong Learning
Create Competency Framework & Milestones
(Generic & Speciality-Specific)
In-Training Competency-Based
Assessment
In-Practice Competency-Based
Assessment
Accreditation Credentialing
ePortfolio
Redesign Policy: Outcome-Based
Focus
Faculty Development and Faculty/Education Support
Redesign Policy: Competency-Based
Focus
CBMERe-Engineer Accreditation
Process
Re-Engineer Credentialing
Process
Deliver Cohorted Roll-Out
Change Exam Governance
Re-EngineerExam Delivery
Develop Exam Content
For Residents For Fellows
Affirmation of Continued Competence
10

Prelude: CBD and CanMEDS 2015
One of these is not like the others …
11
Prelude: CBD and CanMEDS 2015
How can we ensure our graduates are competent in all needed domains…?
12

Why CBD? Why Now? con’t
By focusing on learning rather than time, CBD will enable our MedEd system to assess for competence, but teach for excellence; ensure physician’s skills and abilities evolve throughout
practice—potentially reducing medical errors; respond to changing patient and societal needs; address gaps in the current system, like the “failure to
fail” culture of resident education; reduce burden on Faculties, promoting smoother
credentialing and accreditation; and increase accountability and promote transparency in
training.
13

TIME REMAINS AN ESSENTIAL ELEMENT…

Transformation of Postgraduate Education
“tea-steeping” Brian Hodges Academic Medicine 85(9): September 2010
Targeted to outcomes
Deliberate Practice
Direct Observation

Language -If you were training a Puffer Fish Chef?
Entrustable Professional Activities – Professional life activities that define the discipline.
Competencies – Observable Ability Milestones – Observable behaviors at various stages
on a continuum.

“EPAs are those professional activities that together constitute the mass of critical elements that operationally define a profession.”
“Each of these activities may be defined as a unit of work that should only be entrusted upon a competent enough professional.”
Olle ten Cate, and Fedde Scheele. Acad. Med. 2007; 82:542-547.
“Entrustable Professional Activities (EPAs)”
Becoming a fugu fish chef VSApplying the knife and Knowing the anatomy…

Competency Based Training
“Competency is an observable ability of a health professional, integrating multiple components such as knowledge, skills, values and attitudes. Since competencies are observable, they can be measured and assessed to assure their acquisition. Competencies can be assembled like building blocks to facilitate progressive development..” Frank et al. Med Teach 2010; 32(8): 631-7.
Current trend of itemizing the “parts” that are needed for successful completion of training.

CanMEDS 2015: What Are the Benefits?
Educators will be able to: • Identify progress of learners at different stages of training;• Provide guidance to address identified gaps in learning; • Employ better standards for assessment; and • Benefit from newly created faculty development tools
and resources.
Learners will be able to:• Follow a clear and transparent roadmap that promotes
learning and growth at each stage of training and throughout practice.
19

CanMEDS 2015: Planned Updates
• Introduce new element – milestones to mark the progression of a competence
• Emphasis on the continuum• Integrate new content and themes
(e.g. patient safety)
• Create new faculty development resources and tools
20

CanMEDS 2015: Planned Updates
21

What are the needed abilities of graduates of GIM programs?

Literature Review of GIM Training:
United States: Discrepancy between practice patterns of practicing
internists and trainingMandel1988; Baker1998;Weist2002; Blumenthal 2001.
Canada: Snell in 1989 found deficiencies in training in ambulatory
care, management of complex disorders over time, management of geriatric patients and those with psychosocial problems. Other areas of deficiency included procedures, teaching skills, continuing self-education skills as well as administration and office management.
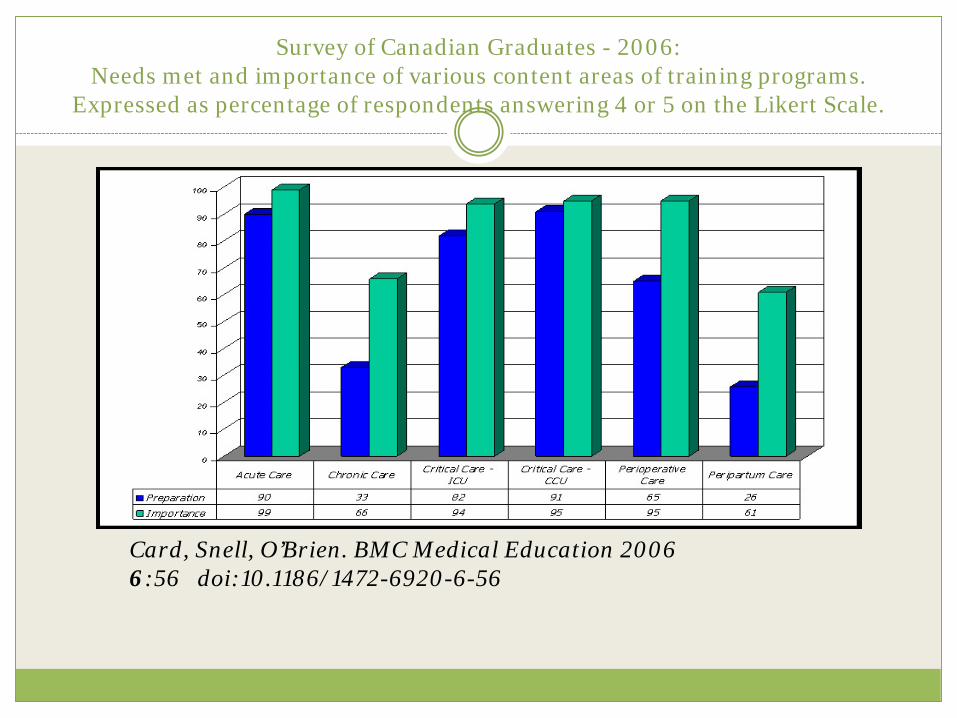
Survey of Canadian Graduates - 2006: Needs met and importance of various content areas of training programs.
Expressed as percentage of respondents answering 4 or 5 on the Likert Scale.
Card, Snell, O’Brien. BMC Medical Education 2006 6:56 doi:10.1186/1472-6920-6-56

Survey of Competencies on Draft Royal College GIM Objectives of Training - 2011
The competencies to be surveyed were developed after extensive consultation with GIM PDs, GIM Division Directors, Canadian Society of Internal Medicine (CSIM) over 8 years. The draft document of objectives forwarded to the Royal College was used as the template.Translated into French by the CSIM translator and forwarded to the French membership.Card, PausJenssen, Ottenbreit. BMC Research Notes 2011 4:480 for detailed results. Results used to further refine the GIM Objectives of Training. http://www.royalcollege.ca/portal/page/portal/rc/public

Key Features of Current GIM Training Programs At the end of GIM Training the graduatewill be able to manage/perform:
At the end of GIM Training the graduate will be able to:
1. Common & Emergency Internal Medicine Conditions
2. Internal Medicine conditions before, during and after pregnancy.
3. Multi-system disease. 4. Perioperative Care. 5. Risk Reduction 6. Procedures:
1. Ambulatory Blood Pressure monitoring
2. Holter monitoring3. Exercise Stress Testing 4. Invasive and non-invasive
ventilation
1. Develop a practice that is: • Adapted to societal needs. • Maintains generalist principles. but
may be quite different than others to meet needs of their community.
• Able to adapt over time. • Respects limits.• Incorporates effective inter and
intra-professional collaboration including excellence in transitions in care.
2. Improve population health outcomes through:
• Patient Safety Initiatives. • Preventive Care• Health Care Delivery Initiatives. • Advocacy for vulnerable
populations. • Education (patients, students,
and/or colleagues)
http://www.royalcollege.ca/portal/page/portal/rc/public

What does society need as the outcomes of GIM Training Programs?

Practice Audit Summaries
Perioperative Care IM Disorders:
Cardiovascular Diseases – CAD; Arrthymias; Valvular Heart Disease; CHF; ACLS; Syncope Respiratory Disease – ILD; COPD; OSA; VTE; Asthma; Pleural Disease
Presentations of Disease – Dyspnea; Chest Pain; Weight Loss; Fever; Pain; Delirium; Fatigue Renal – Lytes; Failure; Chronic Kidney Disease Neurological – Delirium; Seizures; Confusion; Migraine Geriatric – Falls; Polypharmacy; Pain Endocrine – Diabetes; Thyroid; Addison’s; Hypercalcemia; GI – Cirrhosis; Hepatic Failure; Hepatorenal; Pancreatitis; IBD; Ascites; Liver Disease Heme – VTE; Thrombocytopenia; Anemia; Myeloma; Leukemia; Myeloproliferative Disorders; Pancytopenia;
Splenomegaly. Infectious Disease – All Neoplasia – diagnosis and workup; cancer complications and complications of treatment; Addiction; Drug Overdose Rheum – Arthralgia; Sarcoidosis; Temporal Arthritis; RA; PMR;
Risk Reduction: Hypertension; Dyslipidemia
Obstetrical Medicine: Cardiac; Diabetes; Hypercalcemia; Thyroid; Dyspnea; Preconception counselling.
Procedures: Multiple

Potential Tools Brain Storming
Processes: Learner Accountability. Decreased Exam Emphasis – Program
of Assessment. Tools:
ePortfolios Personal Learning Projects Direct Observation:
DOPS MiniCEX
Multisource Feedback “Lay” feedback. Peer Assessment Case Based Discussion Acute Care Assessment Tool
Assessment For & Of Learning Will be Critical

Connections…
Please Network..
Sharon E. Card GIM Division University of Saskatchewan [email protected]
Phone: 1306-844-1127 Fax: 1306 844-1510 @sharon_cards

References:
Mandel JH, Rich EC, Luxenberg MG, Spilane MT, Kern DC, Parrino TA. Preparation for Practice in Internal Medicine. A Study ofTen Years of Residency Graduates. Arch Int Med 1988; 148: 853 – 86.
Baker MZ and Scofield RH. Educational needs of internal medicine residency graduates: general internist versus subspecialists. Medical Education 1988; 32: 527 – 532.
Miller DB. Procedural Skills: A Survey of General Internists in British Columbia. Annals RCPSC 1992; 25(6): 355 – 7. Soparkar GR and Card SE. Technical Skills During Residency and in Practice: A Survey of Specialists in Internal Medicine in
Saskatchewan. Annals RCPSC 1999; 32(5): 296 – 301. Snell L et al. Education of the Internist: Opinions from practicing physicians. Unpublished 1989. Shamekh F and Snell L. Are Internal Medicine Residents Prepared for Ambulatory Practice? Clin & Invest Med; 1999; 22 (4
supp): S29. Abstract # 250. Wiest FC, Ferris TG, Gokhale M, Campbell EG, Weissman JS. Preparedness of Internal Medicine and Family Practice Residents
for Treating Common Conditions. JAMA. 2002; 288: 2609 – 2614. Blumenthal D, Gokhale M, Campbell EG, Weissman JS. Preparedness for Clinical Practice: Reports of Graduating Residents at
Academic Health Centers. JAMA. 2001; 286: 1027 – 1034. Card SE, Snell L and BD O’Brien. BMC Med Education. 2006, 6:56. Determining Specific Competencies for General Internal Medicine Residents (PGY 4 and PGY 5). What are they and are programs
currently teaching them? A survey of practicing Canadian General Internists. Sharon E Card , Anne M PausJenssen and Rachel C Ottenbreit BMC Research Notes 2011, 4:480
Validation of a Canadian curriculum in obstetric medicine. A. Cumyn and P. Gibson for the CanCOM1 Investigators. Obstetric Medicine 2010; 3:145-151.
Competency-Based Postgraduate Training: Can We Bridge the Gap between Theory and Clinical Practice? Olle ten Cate and Fedde Scheele. Acad Med. 2007; 82: 542-547.
Are Canadian General Internal Medicine training program graduates prepared for their future careers? Sharon E Card, Linda Snell and Brian D. O’Brien. BMC Medical Education 2006; 6:56.
Toward a definition of competency-based education in medicine: a systematic review of published definitions. Frank JR et al. Med Teach 2010: 32(8): 631-7.
A Tea-Steeping or i-Doc Model for Medical Education. Brian D Hodges. Acad Med 85(9): September Supplement 2010.
Royal College website http://www.royalcollege.ca/portal/page/portal/rc/public


















