COMPARISON OF NERVE BANKING TECHNIQUES IN DELAYED … · 2017. 8. 2. · 690 Peterson et al,...
6
Ann Otol Rhinol Laryngol 108:1999 COMPARISON OF NERVE BANKING TECHNIQUES IN DELAYED LARYNGEAL REINNERVATION ROBERT J. ANDREWS, MD Los ANGELES, CALIFORNIA MING YE, MD Los ANGELES, CALIFORNIA K. LINNEA PETERSON, MD SEATTLE, WASHINGTON JOEL A. SERCARZ, MD Los ANGELES, CALIFORNIA KEITH E. BLACKWELL, MD Los ANGELES, CALIFORNIA KEVIN KEVORKIAN, MD Los ANGELES, CALIFORNIA GERALD S. BERKE, MD Los ANGELES, CALIFORNIA Successful laryngeal transplantation will require adequate reinnervation of the larynx to allow phonation, coordinated swallow- ing, and respiration. A delay between laryngectomy and transplantation would be necessary in oncology patients because of the need for immunosuppression. In these patients, reinnervation of the donor organ would require "banking" and recovery of dormant recipient recurrent laryngeal nerves (RLNs). This pilot study was undertaken to compare the effectiveness of RLN storage using 1 of 2 techniques: 1) inserting the nerve into a muscle pocket or 2) anastomosing the proximal RLN stump to the ansa cervicalis. Six months following nerve transection and "banking," the proximal anterior branch of the RLN was reanastomosed to the distal ante- rior segment and the posterior branch was anastomosed directly to the posterior cricoarytenoid muscle. Tensionometry, image analy- sis, and electromyographic data were collected 1 year later. Results show reinnervation of adductors and abductors with both tech- niques. Banking of the RLN branches during total laryngectomy is effective and should permit delayed physiological reinnervation following laryngeal transplantation. KEY WORDS — delayed reinnervation, laryngeal reinnervation, laryngeal transplantation. INTRODUCTION Laryngeal transplantation remains an elusive goal of laryngologiste. Several criteria must be met in or- der for laryngeal transplantation to be successful. The donor organ must work as a dynamic functional unit that allows phonation, coordinated swallowing with- out aspiration, and an adequate airway diameter. These functions must be equal to or better than those of patients with a total laryngectomy and excellent tracheoesophageal fistula speech. Immunosuppression must be adequate to allow or- gan survival without significant compromise of the patient's overall health or oncological result. Unless more targeted immunosuppression is developed, pa- tients with malignancies will require a delay between laryngectomy and transplantation in the range of 1 to 2 years in order to reduce the likelihood of recur- rence. This delay adds complexity to an already chal- lenging task, requiring return of appropriate func- tion of a recipient nerve that has been dormant for an extended period of time. The nerve must have adequate axon sprouting into the donor larynx to re- innervate the musculature. Once the larynx has been transplanted, 6 to 12 months must pass before the functional outcome is known. In the interim, the pa- tient requires tracheostomy and must depend on alter- native methods of communication, such as use of an electrolarynx. Techniques and outcomes of laryngeal reinnerva- tion have varied. Methods include direct anastomo- sis, 1 ' 2 nerve grafting 3 with nerves such as the vagus and phrenic, laryngeal nerve-muscle pedicle, 4 and nerve-muscle pedicle reinnervation with a branch of the ansa. 5 Outcome has been contradictory at times, with some investigators reporting poor outcome with little evidence of reinnervation 6 and others report- ing moderate to good results. 5 · 7 · 8 More recent tech- niques have involved selective reinnervation of the abductor and adductor branches of the recurrent la- ryngeal nerve (RLN). 2 - 8 These results have been prom- ising, achieving reinnervation and function while minimizing the problem of synkinesis 9 and paradox- ical vocal cord motion. However, each of these stud- ies was done with immediate repair or grafting. From the Division of Head and Neck Surgery, University of California, Los Angeles School of Medicine, Los Angeles, California. This work was supported by Veterans Administration Merit Review Grant 0001. This study was performed in accordance with the PHS Policy on Humane Care and Use of Laboratory Animals, the NIH Guide for the Care and Use of Laboratory Animals, and the Animal Welfare Act (7 U.S.C. et seq.); the animal use protocol was approved by the Institutional Animal Care and Use Committee (IACUC) of the University of California, Los Angeles. Presented at the meeting of the Pacific Coast Oto-Ophthalmological Society, San Diego, California, June 21-24, 1997. Winner of the 1997 Resident Research Award of the Pacific Coast Oto-Ophthalmological Society. CORRESPONDENCE — K. Linnea Peterson, MD, Virginia Mason Medical Center, Dept of Otolaryngology, X10-ON, 1100 Ninth Ave, Seattle, WA98111. 689
Transcript of COMPARISON OF NERVE BANKING TECHNIQUES IN DELAYED … · 2017. 8. 2. · 690 Peterson et al,...
-
Ann Otol Rhinol Laryngol 108:1999
COMPARISON OF NERVE BANKING TECHNIQUES IN DELAYED LARYNGEAL REINNERVATION
ROBERT J. ANDREWS, MD Los ANGELES, CALIFORNIA
MING YE, MD
Los ANGELES, CALIFORNIA
K. LINNEA PETERSON, MD SEATTLE, WASHINGTON
J O E L A. S E R C A R Z , M D
Los ANGELES, CALIFORNIA
K E I T H E. B L A C K W E L L , M D
Los ANGELES, CALIFORNIA
K E V I N K E V O R K I A N , M D
Los ANGELES, CALIFORNIA
GERALD S. BERKE, MD Los ANGELES, CALIFORNIA
Successful laryngeal transplantation will require adequate reinnervation of the larynx to allow phonation, coordinated swallow-ing, and respiration. A delay between laryngectomy and transplantation would be necessary in oncology patients because of the need for immunosuppression. In these patients, reinnervation of the donor organ would require "banking" and recovery of dormant recipient recurrent laryngeal nerves (RLNs). This pilot study was undertaken to compare the effectiveness of RLN storage using 1 of 2 techniques: 1) inserting the nerve into a muscle pocket or 2) anastomosing the proximal RLN stump to the ansa cervicalis. Six months following nerve transection and "banking," the proximal anterior branch of the RLN was reanastomosed to the distal ante-rior segment and the posterior branch was anastomosed directly to the posterior cricoarytenoid muscle. Tensionometry, image analy-sis, and electromyographic data were collected 1 year later. Results show reinnervation of adductors and abductors with both tech-niques. Banking of the RLN branches during total laryngectomy is effective and should permit delayed physiological reinnervation following laryngeal transplantation.
KEY WORDS — delayed reinnervation, laryngeal reinnervation, laryngeal transplantation.
INTRODUCTION Laryngeal transplantation remains an elusive goal
of laryngologiste. Several criteria must be met in or-der for laryngeal transplantation to be successful. The donor organ must work as a dynamic functional unit that allows phonation, coordinated swallowing with-out aspiration, and an adequate airway diameter. These functions must be equal to or better than those of patients with a total laryngectomy and excellent tracheoesophageal fistula speech.
Immunosuppression must be adequate to allow or-gan survival without significant compromise of the patient's overall health or oncological result. Unless more targeted immunosuppression is developed, pa-tients with malignancies will require a delay between laryngectomy and transplantation in the range of 1 to 2 years in order to reduce the likelihood of recur-rence. This delay adds complexity to an already chal-lenging task, requiring return of appropriate func-tion of a recipient nerve that has been dormant for an extended period of time. The nerve must have adequate axon sprouting into the donor larynx to re-
innervate the musculature. Once the larynx has been transplanted, 6 to 12 months must pass before the functional outcome is known. In the interim, the pa-tient requires tracheostomy and must depend on alter-native methods of communication, such as use of an electrolarynx.
Techniques and outcomes of laryngeal reinnerva-tion have varied. Methods include direct anastomo-sis,1'2 nerve grafting3 with nerves such as the vagus and phrenic, laryngeal nerve-muscle pedicle,4 and nerve-muscle pedicle reinnervation with a branch of the ansa.5 Outcome has been contradictory at times, with some investigators reporting poor outcome with little evidence of reinnervation6 and others report-ing moderate to good results.5·7·8 More recent tech-niques have involved selective reinnervation of the abductor and adductor branches of the recurrent la-ryngeal nerve (RLN).2-8These results have been prom-ising, achieving reinnervation and function while minimizing the problem of synkinesis9 and paradox-ical vocal cord motion. However, each of these stud-ies was done with immediate repair or grafting.
From the Division of Head and Neck Surgery, University of California, Los Angeles School of Medicine, Los Angeles, California. This work was supported by Veterans Administration Merit Review Grant 0001. This study was performed in accordance with the PHS Policy on Humane Care and Use of Laboratory Animals, the NIH Guide for the Care and Use of Laboratory Animals, and the Animal Welfare Act (7 U.S.C. et seq.); the animal use protocol was approved by the Institutional Animal Care and Use Committee (IACUC) of the University of California, Los Angeles. Presented at the meeting of the Pacific Coast Oto-Ophthalmological Society, San Diego, California, June 21-24, 1997. Winner of the 1997 Resident Research Award of the Pacific Coast Oto-Ophthalmological Society. CORRESPONDENCE — K. Linnea Peterson, MD, Virginia Mason Medical Center, Dept of Otolaryngology, X10-ON, 1100 Ninth Ave, Seattle, WA98111.
689
-
690 Peterson et al, Delayed Laryngeal Reinnervation
Anterior branch
Anterior branch
\ l
Anterior branch
Anterior branch
RLN
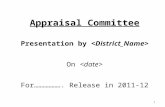
Fig 1. Schematic of surgical procedure for ansa storage. A) Stage 1 procedure with anastomosis of proximal anterior and posterior branches to ansa cervicalis branches. B) Stage 2 procedure with anastomosis of proximal anterior branch to distal segment of anterior branch, and placement of pos-terior segment into pocket of posterior cricoary-tenoid (PCA) muscle. RLN — recurrent laryngeal nerve.
B
The current study was undertaken to address the outcome of "banking" nerves for later transplanta-tion, to minimize degeneration of the nerve. Two dif-ferent methods were used and results were compared in this preliminary study. Neural storage, or anasto-mosis to a branch of the ansa, was compared to the use of a nerve-muscle pedicle or a nerve-muscle "pocket."
MATERIALS AND METHODS Experimental Model. Two male mongrel dogs (25
and 35 kg) were studied. The first dog underwent division of the anterior and posterior branches of the RLN with anastomosis of the proximal segments to the ansa cervicalis. The second dog underwent divi-sion of these branches with use of a nerve-muscle pedicle to the stemothyroid muscle for the posterior branch, with the anterior branch being tucked directly into a muscle pocket of this same muscle.
Methods. Each dog was anesthetized with intrave-nous pentobarbital sodium and placed supine on an operating table. Direct laryngoscopy was performed to confirm normal laryngeal anatomy. The animal was intubated with a 7.0 endotracheal tube under di-rect visualization, and kept under general anesthesia with inhalation of halothane in the range of 1 % to 1.5%, with oxygen at 4 L/min.
A midline incision was made from the upper bor-der of the thyroid cartilage to just below the cricoid cartilage. Trie superior laryngeal nerve was identi-fied and preserved. The inferior border of the crico-pharyngeus was cut to allow access to the distal por-tion of the RLN at the point of bifurcation into ante-rior and posterior branches, and the branches were then isolated on the left side. In the first experimen-
tal dog, branches of the ansa cervicalis were identi-fied and cut. The proximal segments of the anterior and posterior branches of the RLN were then anasto-mosed to distal segments of the ansa (Fig 1). The second experimental animal had a muscle pedicle cut from the posterior cricoarytenoid (PCA) muscle for the posterior branch of the RLN. This muscle pedicle was sutured to the stemothyroid muscle. The anterior branch was cut, and the proximal neural end was placed into a pocket in the strap muscle and se-cured (Fig 2). The wounds were then closed, and the animals were recovered.
The dogs were kept for 6 months and then returned to the operating room for a second procedure, at which time the anterior and posterior branches of the RLN were reanastomosed or placed into target muscles. By the same protocol, the dogs were placed under general anesthesia. Via the same approach, the anterior and posterior branches of the RLN were iso-lated. The proximal and distal ends of the anterior branches were identified and reanastomosed; in the first dog, this required transection of the RLN-ansa segment. The new anastomosis may have contained a portion of the ansa graft. The posterior branch was cut, again possibly with some ansa graft, and the end was inserted into a pocket of the PCA muscle. In the second dog, the proximal portion of the anterior branch was cut just prior to its insertion into the strap muscle. The distal end of the anterior branch was located, and the nerve ends were reanastomosed. The posterior branch was cut just as it entered the strap muscle, and the proximal end was tucked into the PCA muscle. The dogs were again recovered, with suture removal at about 2 weeks.
One year later, the dogs were returned for a third
-
Peterson et al, Delayed Laryngeal Reinnervation 691
Anterior branch
Fig 2. Schematic of surgical pro-cedure for muscle storage. A) Stage 1 procedure with banking of anterior branch into pocket of sternothyroid muscle and muscle pedicle of posterior branch into strap muscle. B) Stage 2 proce-dure with anastomosis of proxi-mal and distal ends of anterior segment, and placement of pos-terior segment into pocket in PC A muscle.
Sternothyroid
Anterior branch
surgery, at which time tensionometry, video, and electromyography (EMG) data were collected. The same protocol for general anesthesia was followed. A midline incision was made from the superior end of the thyroid cartilage to just above the sternal notch. A distal tracheostomy was placed, and the oral endo-tracheal tube was removed. A mouth gag was used to allow direct visualization of the larynx. A button was placed through the epiglottis to suspend the epi-glottis out of the field of view. Videolaryngoscopy and tensionometry were performed with obstructive respiratory dyspnea. Electromyography was per-formed under conditions of obstructive respiratory dyspnea and pharyngeal stimulation, recording sig-nals from the PCA and thyroarytenoid (TA) muscles, respectively. The first dog, with muscle banking, de-veloped bilateral tension pneumothoraces during the experiment and was unable to be resuscitated. Ten-sionometry data are not available for this animal.
The RLNs were dissected out bilaterally, and rub-ber electrodes (monopolar, flexible, conductive neo-prene with silicone, coated by insulating silicone KE45 W) were applied. Videolaryngoscopy and ten-sionometry data were collected with nerve stimula-tion. Finally, the animals were humanely euthanized according to the Animal Care and Use protocol. The anterior and posterior branches, as well as the main trunk, of the left RLN were harvested from both ani-mals. The larynx was also removed. All tissue was placed in 10% formalin for fixation.
Equipment. For videolaryngoscopy, a 0° Storz en-doscope was placed through the mouth and above the vocal cords. A video camera was used to record images on a Sony U-matic Vidéocassette Recorder, model VO-9850 (Sony, Japan). Analysis was per-
PCA
B
formed with ImagePro for Windows 3.1 software (Media Cybernetics, NJ) on a Zeos 486 PC, with a FlashPoint ISA (Version 2.0, Integral Technologies, Indianapolis, Ind) color frame grabber. Measure-ments were made of vocal cord excursion under the given conditions, to compare the relative excursion of each side against the midline. Measurements were made of glottal area in the relaxed state and with maximal abduction. Measurements with nerve stimu-lation were compared from separate trials.
Abductory force measurements were made by a "tensionometer," as described by Nasri et al,10 by placing a straight rod with a plate with a surface area of 3.06 mm2 just lateral to the midportion of the ary-tenoid. The tensionometer was adapted with a digi-tal force gauge (DF-0.5R, Shimpo, Japan). Adductory measurements were made with the same rod, by plac-ing the plate medial to the true vocal cord, just anteri-or to the anterior border of the arytenoid. Compara-tive measurements were made for abductory and ad-ductory force under each set of conditions. Five se-quential measurements of abduction or adduction were made for each trial. Zero and peak readings were recorded, and the zero settings were subtracted out.
A constant current nerve stimulator was used (WR Medical Electronics Co, St Paul, Minn, model S2LH) for RLN stimulation. The frequency and duration of stimuli were 80 Hz and 1.5 milliseconds' duration, respectively. The stimulus levels for abduction mea-surements were set by finding the threshold level for maximal abduction. The adductory measurements were made at the threshold for complete glottal clo-sure.
Electromyography was performed with the Nicolet
-
692 Peterson et al, Delayed Laryngeal Reinnervation
TABLE 1. TENSIONOMETRY DATA FOR ANSA STORAGE ANIMAL
Right Left
PCA (abduction) Tube occlusion RLN stimulation
TA (adduction) RLN stimulation
1.95 ±0.71 2.72 ± 0.08
2.42 ± 0.24 1.98 ±0.40
4.50 ± 0.25 4.38 ± 0.50 Data are in grams (mean ± SD). PCA — posterior cricoarytenoid, RLN — recurrent laryngeal nerve, TA — thyroarytenoid.
Viking IV system (Nicolet, Madison, Wis). Concen-tric needle electrodes (26 gauge, 3.7 cm long, record-ing area 0.068 mm2; Nicolet) were used, with the needles placed into the respective muscles via a trans-oral approach.
All animal protocols were approved by the UCLA Animal Care and Use Committee and were per-formed in compliance with the local, state, and feder-al regulations for the humane use of animals in re-search.
Statistical Analysis. Statistical analysis was per-formed by a 1-way, repeated-measures analysis of variance comparing sides under each set of condi-tions. Tensionometry data were assessed to compare abductory and adductory force on sides under condi-tions of nerve stimulation and obstructive respirato-ry dyspnea. The data were analyzed with SYSTAT software. Glottal images obtained from nerve stimu-lation were analyzed to compare vocal cord excur-sions on each side. These data are reported in terms of mean and standard deviation.
RESULTS Tensionometry. Tensionometry data are available
only for the dog that underwent ansa storage (Table 1 and Fig 3). The results show no significant differ-ence between the left side and the right for abductory
4 -
3 "
2 "
■ Ansa- Nerve stimulation, right Q Ansa- Nerve stimulation, left
-
TABLE 2. IMAGE ANALYSIS COMPARING EXCURSIONS OF RIGHT VERSUS LEFT CORDS
AND GLOTTAL AREA IN ANSA STORAGE ANIMAL VERSUS MUSCLE STORAGE ANIMAL
Right
Tube occlusion Ansa 57.13 ±1.99 Muscle 61.80 ±2.32
Stimulation of RLN Muscle 33.79 ± 6.66
After SLN transection Muscle Data are percent (mean ± SD)
Left
42.87 ± 1.99 38.20 ±2.32
37.22 ±4.13
SLN — superior laryngeal nerve. *Relaxed state to maximal abduction.
Change in Area*
36.97 ± 4.42 30.89 ±3.88
15.89 ±4.21
force under conditions of tube occlusion. With stimu-lation of the posterior branch of the RLN, abductory force was greater on the right than the left, with a statistically significant difference: p < .05, F(l,4) = 25.35. With stimulation of the main trunk of the RLN, there was nearly equal force of adduction and no sta-tistically significant difference.
Image Analysis. Video data demonstrated vocal cord excursion from midline of right versus left vo-cal cords, as well as change in glottal area from the relaxed state to full abduction under varying condi-tions (Table 2 and Fig 4). These results show the excursion on the right to be approximately 57% of the glottal width, versus 43% for the left under condi-tions of tube occlusion for the animal with ansa stor-age (SD 1.99%). This 43% for the left represents 75% of the excursion demonstrated on the right. The animal with muscle storage had 62% for the right versus 38% for the left, under the same conditions (SD 2.32% for both sides). This is 62% of the ex-pected excursion, or the excursion found on the right. The change in glottal area from the relaxed state to full abduction with tube occlusion shows a 36.97% change (SD 4.42%) in total area with ansa storage,
6
5
41
3
D
Ansa-Tube occlusion, right Ansa-Tube occlusion, left
Ansa-Nerve stimulation, right
Ansa-Nerve stimulation, left
B Fig 3. Ansa storage. A) Force of adduction with nerve stimulation, right versus left. B) Force of abduction, tube occlusion versus nerve stimulation, right versus left.
-
Peterson et al, Delayed Laryngeal Reinnervation 693
100
80
60
40
20
■ Ansa- Tube occlusion, right
0 Ansa- Tube occlusion, left
Θ Muscle- Tube occlusion, right
G Muscle- Tube occlusion, left
100
-, 90 CO (D
S 80 -^ 70 Φ H1 60 co -5 50 0) σ> 40 CO
ΐ 30 ϋ a 20 D.
10
-
-
■ Ansa- Tube occlusion
0 Muscle- Tube occlusion
B Fig 4. Image analysis. A) Relative excursion with tube occlusion, ansa versus muscle storage, right versus left. B) Percentage change in area with tube occlusion, ansa versus muscle storage.
versus only a 30.89% change (SD 3.88%) with mus-cle storage. The results for RLN stimulation show a 33.79% change (SD 6.66%) in area with stimulation on the right versus a 37.22% change (SD 4.13%) with stimulation on the left in the dog with muscle banking. No RLN stimulation data are available for the ansa storage dog.
Electromyography. The EMG data for the 2 ani-mals showed evidence of selective reinnervation of the TA and PCA muscles (Figs 5 and 6). There was physiologically appropriate firing of motor units, the PCA firing with respiration and the TA firing with pharyngeal stimulation and adduction. The dog with ansa storage showed a single motor unit for both the TA and PCA muscles. The dog with muscle storage demonstrated similar signals, although with smaller motor units.
DISCUSSION The success of laryngeal transplantation for can-
cer patients requires the coordination of immunosup-pression and functional reinnervation. The latter ap-pears to be the most limiting factor, while improve-ments in immunosuppression have allowed excel-lent results in solid organ transplantation. Techniques in reinnervation have evolved, especially over the past 20 years, with methods to avoid synkinesis. In our laboratory, selective reanastomosis of the adduc-tor and abductor branches has been successful in achieving reinnervation with functional, physiologi-cal motion.2'10
Fig 5. Electromyography with ansa storage. A) PCA muscle with tube occlusion in single mo-tor unit followed by burst of activity with ab-duction. B) Thyroarytenoid (TA) muscle with glottal closure in single motor unit and activ-ity with adduction.
The desire to avoid immunosuppression of can-cer patients requires a delay in transplantation until the risk of cancer recurrence is low. In order for these patients to be eligible for future transplantation, they would need to have their RLNs preserved by "bank-ing" them to prevent nerve degeneration.
The results of this study demonstrate return of physiological motion following denervation of the anterior and posterior branches of the RLN with a 6-month delay between transection and reanastomosis. One year was allowed for neural regeneration prior to data collection. Two different techniques of bank-ing were used: ansa cervicalis storage with neural anastomosis of the proximal segments of the anteri-or and posterior branches of the RLN to branches of the ansa; and muscle storage with the anterior branch tucked into a pocket in the sternothyroid muscle, and a muscle pedicle of the posterior branch attached to this same strap muscle.
Tensionometry data show good return of force with ansa storage, with nearly equal adductory force. Abductory force also had good recovery, with no sta-tistically significant difference between the operated and control sides with obstructive respiratory dysp-nea. With nerve stimulation, there was a significant difference, with the left being weaker than the right. Tensionometry measures could not be performed in the muscle banking animal.
The image data also support the recovery of both laryngeal abduction and adduction. Both animals had
200 uV 5 ns 100 ns 50 uV 5 ns
^W
100 ns
X»4^*44^π'^MM",^
A B
-
694 Peterson et al, Delayed Laryngeal Reinnervation
100 uV 5 «15
—