COMPARATIVE STUDY OF CHANGES IN PHARYNGEAL...
90
COMPARATIVE STUDY OF CHANGES IN PHARYNGEAL AIRWAY DIMENSION AND HYOID BONE POSITION FOLLOWING NONSURGICAL ORTHODONTIC TREATMENT IN CLASS I AND CLASS II SUBJECTS Dissertation Submitted to THE TAMIL NADU DR. M.G.R. MEDICAL UNIVERSITY In Partial fulfilment for the degree of MASTER OF DENTAL SURGERY BRANCH - V ORTHODONTICS AND DENTOFACIAL ORTHOPAEDICS APRIL – 2013
Transcript of COMPARATIVE STUDY OF CHANGES IN PHARYNGEAL...

COMPARATIVE STUDY OF CHANGES IN PHARYNGEAL AIRWAY
DIMENSION AND HYOID BONE POSITION FOLLOWING
NONSURGICAL ORTHODONTIC TREATMENT IN
CLASS I AND CLASS II SUBJECTS
Dissertation Submitted to
THE TAMIL NADU DR. M.G.R. MEDICAL UNIVERSITY
In Partial fulfilment for the degree of
MASTER OF DENTAL SURGERY
BRANCH - V
ORTHODONTICS AND DENTOFACIAL ORTHOPAEDICS
APRIL – 2013

CERTIFICATE
This is to certify that the dissertation entitled
“COMPARATIVE STUDY OF CHANGES IN PHARYNGEAL AIRWAY
DIMENSION AND HYOID BONE POSITION FOLLOWING NONSURGICAL
ORTHODONTIC TREATMENT IN CLASS I AND CLASS II SUBJECTS” done
by Dr. N.M.VIJAYKUMAR Post graduate student (M.D.S), Orthodontics
(branch V), Tamil Nadu Govt. Dental College and Hospital, Chennai, submitted to
the Tamil Nadu Dr. M.G.R. Medical University in partial fulfilment for the M.D.S.
degree examination (April 2013) is a bonafide research work carried out by him
under my supervision and guidance.
Guided By
Dr. M.C.SAINATH M.D.S.,
Professor and Head of the Department,
Dept. of Orthodontics,
Tamil Nadu Govt Dental College & Hospital,
Chennai - 600 003
Dr. K.S.G.A. NASSER, M.D.S.,
Principal,
Tamil Nadu Govt Dental College, & Hospital,
Chennai - 600 003.

DECLARATION
I, Dr. N.M.VIJAYKUMAR , do hereby declare that the dissertation titled
“COMPARATIVE STUDY OF CHANGES IN PHARYNGEAL AIRWAY
DIMENSION AND HYOID BONE POSITION FOLLOWING NONSURGICAL
ORTHODONTIC TREATMENT IN CLASS I AND CLASS II SUBJECTS” was
done in the Department of Orthodontics, Tamil Nadu Government Dental College
& Hospital, Chennai 600 003. I have utilized the facilities provided in the
Government Dental College for the study in partial fulfilment of the requirements
for the degree of Master of Dental Surgery in the speciality of Orthodontics and
Dentofacial Orthopaedics (Branch V) during the course period 2010-2013 under the
conceptualization and guidance of my dissertation guide, Professor Dr. M. C.
Sainath, MDS.
I declare that no part of the dissertation will be utilized for gaining financial
assistance for research or other promotions without obtaining prior permission from
the Tamil Nadu Government Dental College & Hospital.
I also declare that no part of this work will be published either in the print or
electronic media except with those who have been actively involved in this
dissertation work and I firmly affirm that the right to preserve or publish this work
rests solely with the prior permission of the Principal, Tamil Nadu Government
Dental College & Hospital, Chennai 600 003, but with the vested right that I shall
be cited as the author(s).
Signature of the PG student Signature of the HOD
Signature of the Head of the Institution

ACKNOWLEDGMENT
My sincere thanks to Dr. K.S.G.A. NASSER, M.D.S., Principal, Tamil
Nadu Government Dental College and Hospital, Chennai-3, for his kind support
and encouragement.
I express my deep sense of gratitude and great honour to my respected
guide, Professor Dr. M.C.SAINATH M.D.S., Head of the Department,
Department of Orthodontics and Dentofacial orthopaedics, Tamilnadu Govt. Dental
College and Hospital, Chennai-3, for his patience guidance, support and
encouragement throughout the study.
I owe my thanks and great honour to Dr. G. VIMALA M.D.S, Professor,
Department of Orthodontics and Dentofacial Orthopaedics, Tamilnadu Govt.
Dental College and Hospital, Chennai3, for helping me with her valuable and
timely suggestions and encouragement.
I owe my thanks and great honour to Dr.S.PREMKUMAR M.D.S,
Professor, Department of Orthodontics and Dentofacial Orthopaedics, Tamilnadu
Govt. Dental College and Hospital, Chennai3, for helping me with his valuable and
timely suggestions and encouragement.
I am grateful to Dr.B.BALASHANMUGAM, M.D.S., Assistant
Professor, Department of Orthodontics, Tamil Nadu Government Dental College
and Hospital, Chennai –3 for his support and encouragement.

I am grateful to Dr. USHA RAO, M.D.S., Assistant Professor, Department
of Orthodontics, Tamilnadu Government Dental College and Hospital, Chennai-3
for her support and encouragement.
I am grateful to Dr. K. USHA, M.D.S., Assistant Professor, Department of
Orthodontics, Tamil Nadu Government Dental College and Hospital, Chennai –3
for her support and encouragement.
I thank Dr. R. RAVANAN M.Sc., M.Phil., Ph.D., Professor of Statistics,
Presidency College, for helping me with the Statistics in the study.
I take this opportunity to express my gratitude to my friends and colleagues
for their valuable help and suggestions throughout this study.
I offer my heartiest gratitude to my family members for their selfless
blessings.
I seek the blessings of the Almighty God without whose benevolence; the
study would not have been possible.

TRIPARTITE AGREEMENT
This agreement herein after the “Agreement” is entered into on this
day............... day of December 2012 between the Tamil Nadu Government Dental College
and Hospital represented by its Principal having address at Tamilnadu Government
Dental college and Hospital, Chennai-03, (hereafter referred to as , ’the college’)
And
Dr. M. C. Sainath aged 55 years working as professor at the college, having residence
address at Block ‘U’, Door no 11,4th main road, Annanagar, Chennai 600040, Tamilnadu
(herein after referred to as the ‘Principal investigator’)
And
Dr. N.M.VIJAYKUMAR aged 28 years currently studying as postgraduate student in
department of Orthodontics in Tamilnadu Government Dental College and Hospital
(herein after referred to as the ‘PG/Research student and co- investigator’).
Whereas the ‘PG/Research student as part of his curriculum undertakes to
research on “Comparative study of changes in pharyngeal airway dimension and hyoid
bone position following nonsurgical orthodontic treatment in class I and class II
subjects.” for which purpose the PG/Principal investigator shall act as principal
investigator and the college shall provide the requisite infrastructure based on availability
and also provide facility to the PG/Research student as to the extent possible as a Co-
investigator.
Whereas the parties, by this agreement have mutually agreed to the various issues
including in particular the copyright and confidentiality issues that arise in this regard.
Now this agreement witnesseth as follows:

1. The parties agree that all the Research material and ownership therein shall become the
vested right of the college, including in particular all the copyright in the literature
including the study, research and all other related papers.
2. To the extent that the college has legal right to do go, shall grant to licence or assign the
copyright do vested with it for medical and/or commercial usage of interested
persons/entities subject to a reasonable terms/conditions including royalty as deemed by
the college.
3. The royalty so received by the college shall be equally by all the parties.
4. The PG/Research student and PG/Principal Investigator shall under no circumstances
deal with the copyright, Confidential information and know – how generated during the
course of research/study in any manner whatsoever, while shall sole vest with the manner
whatsoever and for any purpose without the express written consent of the college.
5. All expenses pertaining to the research shall be decided upon by the principal
investigator/Co-investigator or borne sole by the PG/research student.(co-investigator)
6. The college shall provide all infrastructure and access facilities within and in other
institutes to the extent possible. This includes patient interactions, introductory letters,
recommendation letters and such other acts required in this regard.
7. The principal investigator shall suitably guide the student Research right from selection
of the Research Topic and Area till its completion. However the selection and conduct of
research, topic and area research by the student researcher under guidance from the
principal investigator shall be subject to the prior approval, recommendations and
comments of the Ethical Committee of the college constituted for this purpose.

8. It is agreed that as regards other aspects not covered under this agreement, but which
pertain to the research undertaken by the student Researcher, under guidance from the
Principal Investigator, the decision of the college shall be binding and final.
9. If any dispute arises as to the matters related or connected to this agreement herein, it
shall be referred to arbitration in accordance with the provisions of the Arbitration and
Conciliation Act, 1996.
In witness whereof the parties hereinabove mentioned have on this the day month and year
herein above mentioned set their hands to this agreement in the presence of the following
two witnesses.
College represented by its Principal PG Student
Witnessess Student Guide
1.
2.

CONTENTS
Sl.No. Title Page No.
1. INTRODUCTION 01
2. AIM AND OBJECTIVES 05
3. REVIEW OF LITERATURE 06
4. MATERIALS AND METHODS 28
5. STATISTICAL ANALYSIS 39
6. RESULTS 40
7. DISCUSSION 55
8. SUMMARY AND CONCLUSION 64
9. BIBLIOGRAPHY 66

List of tables
S.no Table Page no.
1. Cephalometric Landmarks 30
2. Airway Parameters 32
3. Hyoid Bone Position Parameters 32
4. Dentofacial parameters 32
5. Distribution of study subjects - based on gender 40
6. Distribution of study subjects based on age. 41
7. Comparison of Airway related parameters among study subjects
within Class I malocclusion group
42
8. Comparison of Hyoid position related parameters among study
subjects within Class I malocclusion group
42
9. Comparison of Dento-facial related parameters among study
subjects within Class I malocclusion group.
43
10. Comparison of Airway related parameters among study subjects
within Class II malocclusion group.
44
11. Comparison of Hyoid position related parameters among study
subjects within Class II malocclusion group.
44
12. Comparison of Dento-facial related parameters among study
subjects within Class II malocclusion group.
45
13. Comparison of airway parameters between Class I and Class II
malocclusion groups.
46
14. Comparison of Airway Parameters between Class I And Class II
Malocclusion Groups Independent Samples Test
47
15. Comparison of hyoid position related parameters between Class
I and Class II malocclusion groups.
49
16. Comparison of hyoid position related parameters between
subjects with Class I and Class II occlusion - Independent
Samples Test
49

17. Comparison of airway related parameters between subjects with
Normal, Class I and Class II occlusion at baseline
51
18. Comparison of airway related parameters between subjects with
Normal, Class I and Class II occlusion -post treatment.
51
19. Comparison of hyoid position related parameters between
subjects with Normal, Class I and Class II occlusion at baseline.
52
20. Comparison of hyoid position related parameters between
subjects with Normal, Class I and Class II occlusion-post
treatment.
52
21. Changes In Airway dimension And Hyoid bone position -
Based On Gender
53

List of colour plates
1. Cephalostat
2. Canon D520 MF scanner
3. Standardization with Transparent Grid
4. Standardization with Adobe photoshop CS5
5. Ax Ceph Cephalometric Analysis Software
6. Analysis of digitized lateral cephalograms – Control subject
7. Analysis of digitized lateral cephalograms – Class I subject
Pretreatment and post treatment.
8. Analysis of digitized lateral cephalograms – Class II subject
Pretreatment and post treatment.

Abstract
Background: Pharyngeal airway dimensions, narrowing of pharyngeal passage and hyoid bone
positions are of interest in orthodontics .It is evident that there exists a mutual correlation
between position of the hyoid bone, volume of pharyngeal airway and dentofacial structures.
Therefore it is relevant to evaluate the changes in nasopharyngeal airway and hyoid bone
position in subjects with moderate dentofacial deformities, who had orthodontic treatment. This
retrospective, analytical cephalometric study had been undertaken to investigate correlation in
skeletal Class I and skeletal Class II subjects who had undergone non-surgical orthodontic
treatment.
Aim: The aim of this study was to evaluate and compare the changes in pharyngeal airway
dimension and hyoid bone position following non-surgical orthodontic treatment in Class I and
Class II dentofacial deformities.
Materials and methods: 40 sets (pre & post treatment ) of lateral cephalograms of subjects (20
skeletal Class I & 20 skeletal Class II malocclusion) were analysed. The control group consisting
of 20 lateral cephalograms of subjects with normal occlusion and good visibility of hyoid bone
were used .All cephalograms were taken in natural head position, with PLANMECA PM 2002
CC PROLINE machine. All the radiographs were scanned with CANON D520 MF scanner and
digitized. A Cephalometric analysis software AX CEPH version 2.3.0.74 was used to analyse the
radiographs.
Results: Pretreatment hypopharynx area was significantly constricted in both Class I and Class
II groups with highly significant reduction (p value < 0.001) in Class II groups in comparison
with normoocclusion group. In Class I malocclusion group there was a significant decrease in
overall upper airway dimensions, with more reduction in glossopharynx and hypopharynx areas
following orthodontic treatment with only velopharynx and glossopharynx areas approximating
to the values of the normoocclusion group. In Class II malocclusion the glossopharynx and
hypopharynx areas were widened significantly, still the hypopharynx area was not widened to
the level of normoocclusion group. After treatment the hyoid was retracted postero inferiorly in
Class I group and in Class II group the hyoid bone was shifted anterosuperiorly. Still the hyoid
position was not approximated to that of normoocclusion group. There was no statistically
significant (p value > 0.05) sexual dimorphism in both pharyngeal airway dimensions and hyoid
bone positions in all three groups.
Conclusion: There is a definite difference in pharyngeal airway dimension and hyoid bone
position in different malocclusions. It was evident that Non-surgical orthodontic treatment had a
significant influence on the pharyngeal airway dimensions and hyoid bone positions in Class I
and Class II malocclusion corrections.
Key Words: Pharyngeal Airway, Hyoid Bone, Lateral Cephalograms, Class I & Class II
Malocclusion.

Introduction
1
Introduction
Pharyngeal airway dimensions and resistance are of interest in
orthodontics. Ever since, several studies have indicated a close association
between airway dimensions and dentofacial structures20, 24
. Numerous
evidences from cephalometric studies support a link between airway
dimensions, hyoid bone positions and maintenance of dentofacial harmony.
The pharynx is a 12–14 cm long musculomembranous tube shaped like
an inverted cone 29
. It extends from the cranial base to the lower border of the
cricoid cartilage (the level of the sixth cervical vertebra), where it becomes
continuous with the oesophagus73
.
The pharynx communicates with the nasal, oral and laryngeal cavities
via the nasopharynx, oropharynx and laryngopharynx respectively45
. The
nasopharynx and the oropharynx have significant locations and functions as
they form a part of the unit in which respiration and deglutition are carried out.
The nasopharynx forming the upper part of respiratory system is connected
anteriorly with nasal cavity and posteriorly it extends as oropharynx. The
oropharynx extends from the soft palate to the base of epiglottis (from second
to fourth cervical vertebra). The laryngopharynx joins the oropharynx at the
level of pharyngoepiglottic fold and the hyoid, and then it continues upto the
level of the sixth cervical vertebra.
The pharynx is composed of three coats: mucous,
fibrous, and muscular. The muscles of the pharynx are three circular

Introduction
2
constrictors and three longitudinal elevators. The constrictors may be thought
of as three overlapping cones which arise from structures at the sides of the
head and neck and pass posteriorly to insert into a midline fibrous band, the
pharyngeal raphe (overlapping has been compared with that of three flower
pots placed one inside another)73
. Its lining mucosa is continuous with that
lining the pharyngotympanic tubes, nasal cavity, mouth and larynx 29
.
Nasal obstruction due to anatomical variations and pathologies can
cause chronic mouth breathing and a number of postural changes, such as open
mandibular posture, downward and forward positioning of the tongue, and
extension of the head. If these postural changes continue during the active
growth stage without any restrictions, over a period of time many dentofacial
disorders at different levels of severity can be seen, such as long face syndrome
or adenoid facies51
. Other than these factors there is also the natural anatomical
predisposition of narrower airway passages. Skeletal features such as retrusion
of the maxilla and mandible and vertical maxillary excess in hyperdivergent
patients may lead to narrower anteroposterior dimensions of the airway75
.
Obstructive sleep apnoea is a serious medical problem and may be
precipitated by any narrowing of the upper airway caused by external or
internal factors. Investigators have reported a steeper mandibular plane angle,
shorter mandibular body length and a low hyoid bone position in patients
suffering from obstructive sleep apnoea.
Hence pharyngeal study is of importance to both otolaryngologists and
orthodontists alike.

Introduction
3
According to the Balter's philosophy, Class II malocclusions are a
consequence of a backward position of the tongue, due to which the normal
respiratory function is impeded and thus resulting in a faulty deglutition and
mouth breathing; while Class III malocclusions are due to a more forward
position of tongue28
.
The size of nasopharyngeal area is significantly greater in Class I than in
Class II malocclusions20
. Hence a significant interaction is expected to occur
between the pharyngeal structures and dentofacial pattern.
The hyoid bone is a horseshoe-shaped bone situated in the anterior
midline of the neck between the chin and the thyroid cartilage. At rest, it lies at
the level of the base of the mandible in the front and the third cervical
vertebra behind29, 45
. Unlike other bones of neck hyoid does not have any bony
articulations. It provides attachments for ligaments, muscles, fascia of cranium
and mandible. The two major group of muscles attached to hyoid bone are
suprahyoid and infrahyoid muscles. Both suprahyoid and infrahyoid muscles
have wide range of actions.
Digastric muscle is one of the suprahyoid muscles increase the antero
posterior dimensions of oropharynx during deglutition. The stylohyoid and
posterior belly of digastric act together to prevent the regurgitation of food49
.
The hyoid bone plays an important and active part in accomplishing the
delicate balance between anterior and posterior muscle tension relative to the

Introduction
4
occipital condyles, which in turn helps to balance the head as man assumed an
upright posture.
It is evident that there exists a mutual correlation between position of the
hyoid bone, volume of pharyngeal airway and dentofacial structures. In all
types of dentofacial deformities there is a difference in position of dentofacial
structures including teeth. Therefore it is relevant to evaluate the changes in
nasopharyngeal airway and hyoid bone position in subjects with moderate
dentofacial deformities, who had orthodontic treatment. The methods for
evaluating pharyngeal dimension in orthodontic practices are limited.
This retrospective, analytical cephalometric study had been undertaken
to investigate such correlation in skeletal Class I and skeletal Class II subjects
who had undergone non-surgical orthodontic treatment with extraction of four
premolar teeth and comparing it with normoocclusion subjects.

Aim and Objectives
5
AIM AND OBJECTIVES
AIM:
The aim of this study was to evaluate and compare the changes in
pharyngeal airway dimension and hyoid bone position following non-
surgical orthodontic treatment in Class I and Class II dentofacial deformities.
OBJECTIVES:
To determine whether the pharyngeal airway dimensions and hyoid
bone position were affected by non-surgical orthodontic treatment in
skeletal Class I & skeletal Class II subjects.
To evaluate the pharyngeal airway dimensions and hyoid bone position
in normal subjects of South Indian origin.
To compare the changes of pharyngeal airway dimensions and hyoid
bone positions between these groups.
To determine any sexual dimorphism in the changes of pharyngeal
airway dimensions and hyoid bone positions following non-surgical
orthodontic treatment in both Class I and Class II groups.

Review Of Literature
6
Review of literature
The Pharyngeal airway is composed of 20 or more muscles that are
attached proximally to skeletal structures and those size and form are affected
by the developing craniofacial skeleton. The oral and pharyngeal regions are
said to have a primary function in maintaining a patent airway. This is
accomplished by a dynamic musculoskeletal balance. The pharyngeal airway is
one of the determinants of anteroposterior relationship of jaws, particularly the
mandible; by means of determining the tongue position. Accordingly, the
dimensions of pharynx are determined by the position and relation of the
maxilla and the mandible. Moss56
while explaining the functional matrices goes
one step further by including the pharynx into the oro-naso-pharyngeal
functioning spaces, whose volumetric growth is primary morphogenetic event
in facial skull growth. The literature related to the development of pharyngeal
airway and hyoid bone position and their association with the various
malocclusions has been reviewed here.
Balters28
(1952) had a unique view as far as the aetiology of the development
of malocclusion was concerned. According to his hypothesis, Class II
malocclusions were a consequence of a backward position of the tongue which
impedes the respiratory function, concomitantly leading to narrower
pharyngeal airway and mouth breathing. By the same analysis, he reasoned that
Class III conditions are due to a more forward position of tongue and
consequently larger pharyngeal airway dimensions.

Review Of Literature
7
Allan G. Brodie2 (1952) discussed the role of musculature in diagnosis,
treatment and retention. According to him, the hyoid and the tongue are
intimately associated structures and both are positioned in space by a 3 point
muscular suspension.
Carmine Durzo et al14
(1962) studied the growth behaviour of the hyoid bone
in relation to other craniofacial structures in a longitudinal cephalometric study.
They concluded that the hyoid bone has a stable vertical position in normal
individuals, at a level opposite the lower portion of third and upper portion of
fourth cervical vertebra. During growth its relative position remains constant
when it descends as the cervical vertebrae increase their length and the cranial
base and mandible descend and move away from each other. In the mandibular
deformity cases the hyoid movements followed closely those of mandibular
growth movements and were restricted both anteroposteriorly and vertically.
The hyoid movements were also modified as per the demands of maintaining a
patent airway.
Reul Bench74
(1963) carried out an elaborate cephalometric study on the
growth of the cervical vertebra as related to tongue; face and denture
behaviour. He concluded that, in older ages, the behaviour of the hyoid bone is
more consistent to the growth of the cervical vertebrae than chin growth. At 3
years of age the hyoid lies at a level between 3rd and 4th cervical vertebrae and

Review Of Literature
8
descends to the level of the 4th vertebrae at adulthood. Furthermore the clinical
manifestations of open bite are characterized by unusual position and behaviour
of the hyoid bone. He noted that in dolichocephalic persons there was a more
vertical descent of the hyoid bone than in brachycephalic persons. However the
latter was characterized by a more anterior growth shift of the hyoid bone. It
was postulated that the descent and retraction of the tongue seemed to offer one
explanation of the late crowding that develops in the anterior region of the
lower dental arch following orthodontic treatment or in normal untreated cases.
Robert Sloan et al71
(1967) using cineflurography compared the hyoid
movement during deglutition in Class I and Class II patients. They concluded
that in Class I malocclusion patients, the hyoid bone was found to be positioned
more posteroinferiorly and showed the greatest range of vertical movement
during deglutition. It also showed the most limited functional pattern in this
group. In Class II patients, the hyoid was positioned more upwards and
forwards or anterosuperiorly to the mandible and showed the greatest range
during deglutition. The authors confirmed two patterns of hyoid bone
movement during deglutition-Circular and Oblique or Elliptical.
Moss56
(1969) in his functional matrix theory of facial growth, states that the
changes in cell size, shape and spatial position, and indeed the very
maintenance of all the skeletal units; are always secondary to the primary

Review Of Literature
9
changes in their functional matrices. He called pharynx as, a part of one of the
primary functional spaces – the oro-naso-pharyngeal functioning space
(orofacial capsular matrix); and it is the volumetric expansion of these
pharyngeal, oral and nasal spaces that causes the translation of all the skeletal
units embedded within the orofacial capsule.
Ian Milne and John Cleal37
(1970) evaluated the functional adaptation of
orofacial structures in a cineflurographic study. They concluded that the hyoid,
the tongue and the mandible worked as an integrated unit. The positional
changes of the hyoid bone are characteristics of the integration of numerous
structures involved in deglutition. The tongue tip and pharyngeal structures are
capable of acting in part, autonomously and the adaptive movements of the
hyoid are responsible for the maintenance of an adequate airway.
Gary Cuozzo and Douglas Bowman27
(1975) shed light on the changes in the
hyoid bone during deglutition following forced distal positioning of the tongue
by a tongue crib. The conclusions suggested that in persons with the hyoid
resting close to the mandible, the hyoid bone moved in a posteroinferior
direction following crib placement and in persons where hyoid rest position
was distant from the mandible, the hyoid bone did not show any positional
change following crib placement. They attributed these differences to the

Review Of Literature
10
limitation of posterior displacement of the hyoid bone in need for maintaining a
patent airway.
Garland Hershey.H et al26
(1976) in their study of Changes in nasal airway
resistance associated with rapid maxillary expansion with six boys and eleven
girls (between 11 and 14 years of age) who had mouth breathing, concluded
that rapid maxillary expansion was not only an efficient method for increasing
the width of narrow maxillary arches but also reduces nasal resistance from
levels associated with mouth breathing to levels compatible with normal nasal
respiration.
David Gobielle and Douglas Bowman21
(1976) illustrated the hyoid bone and
muscle changes in 10 children, 11 to 15 years of age, after distal positioning of
the tongue. They concluded the following,
a. The hyoid bone assumed a posteroinferior position in individuals with the
rest position of the hyoid bone near the mandible and in individuals with hyoid
rest position distant from the mandible, there was no change in hyoid position
after distal tongue repositioning.
b. There was no change in hyoid path during deglutition before and after distal
tongue positioning.

Review Of Literature
11
Proffit68
(1978) explained that if there was difficulty in breathing due to airway
obstruction, the physiologic adaptation that facilitate mouth breathing include a
forward posture of head and a lowered position of the mandible with a low and
forward tongue posture.
Lee Graber48
(1978) correlated pre and post treatment hyoid positions after
chin cup therapy in 30 individuals of average 6 years of age using lateral
cephalograms. He found that the hyoid bone followed the posteroinferior
direction of mandibular rotation during the course of treatment. He concluded
his result to be attributed to the tongue repositioning and the proximity of the
oropharyngeal and laryngeal spaces to the hyoid bone.
Bibby and Preston10
(1981), described the hyoid triangle analysis. After an
extensive study of the literature, he concluded that the vast variation found in
the previous studies may be because of the fact that the hyoid bone was
correlated to cranial structures. The hyoid, by virtue of being totally suspended
by soft tissues and located away from the cranial structures, any small variation
in the position of the reference planes due to head position changes would
result in a much greater apparent variation of the hyoid bone.
In their analysis, they related the hyoid bone to the vertebrae and the mandible.
Since the mandibular symphysis is at a level more comparable to the axis of
rotation of the head than the cranium, the effect of head movement was

Review Of Literature
12
minimized and the hyoid position was determined more accurately. He had
given standard values for the hyoid triangle and also concluded that there is no
sexual dimorphism in the position of the hyoid.
Ioannis P.Adamidis et al38
(1983) evaluated the position of the tongue,
mandible and hyoid bone in children aged 9 years having lymphadenoid
hypertrophy, mouth breathing and Class I malocclusion. They concluded that
the tongue was placed more downwards and forwards in the lymphadenoid
hypertrophy group. The mandible showed a clockwise rotation and a
significant downward inclination, increased lower anterior facial height and
increased gonial angle in lymphadenoid hypertrophy group. The hyoid bone
was found to follow the mandibular inclination and was found to rotate and
attain a more inferior direction in the lymphadenoid hypertrophy group.
Bibby11
(1984) used his hyoid triangle analysis to evaluate the hyoid bone
position in mouth breathers and tongue thrusters and compared to a control
sample. The results did not show any significant differences in hyoid bone
position in the three groups compared and he concluded that the hyoid has a
stable position independent or any posture alterations due to tongue thrusting or
mouth breathing.

Review Of Literature
13
McNamara41
(1984) suggested that lower pharyngeal width can be measured
from the intersection of posterior border of tongue and inferior border of the
mandible to the closest point on the posterior pharyngeal wall. He felt that the
width of the lower pharynx greater than 15 mm suggested anterior positioning
of the tongue.
Athanasiou et al8 (1991) studied the changes in pharyngeal depth and hyoid
bone at the level of 2nd
and 4th
cervical vertebrae and their relationship in
mandibular prognathism in lateral cephalograms of patients who received
combined orthodontic-surgical treatment. The hypothesis that posterior
mandibular repositioning may reduce the airway at the levels of 2nd
and
4thcervical vertebrae cannot be supported by the findings of this study. It also
indicated that reflex alteration in pharyngeal musculature and biomechanical
conditions of supra and infrahyoid muscles occur postoperatively.
Taylor et al59
(1996) gave brilliant literature regarding the soft tissue growth of
oropharynx. With the help of lateral cephalograms, they demonstrated that hyoid
bone descends and moves slightly anterior upto age 18. The soft palate increased
1 mm in length and 0.5 mm in thickness every 3years after age 9. Thus, in
general, two periods of accelerated change (6-9 yrs. and 12-15 yrs.) and two
periods of quiescence (9-12 yrs. and 15-18 yrs.) were identified for pharyngeal
soft tissue.

Review Of Literature
14
Ioannis Kollias et al39
(1999) conducted a longitudinal study to investigate by
cephalometric means the alterations in craniofacial morphology and hyoid bone
positions in males and females in three different age groups with a ten year
interval. They concluded that the hyoid bone assumed a more inferior position
in adult life in relation to various skeletal structures in both men and women. In
males, the descent was more pronounced than that in females. The horizontal
position was however found to be stable.
Joanna M. battagel et al43
(2000) analyzed the upright lateral cephalometric
radiographs of 115 dentate Caucasian males. 45 subjects exhibiting proven
Obstructive Sleep Apnoea Syndrome, 45 simple snorers and remaining 24
subjects with no history of respiratory disease or snoring, acted as controls. Only
the cranial base angle and mandibular body showed significant intergroup
differences. Both snorers and OSAS patients exhibited narrow airway, reduced
oropharyngeal areas, shorter and thicker soft palate and large tongue than their
control counterparts.
Boon H.Seto et al12
(2001) tested the hypothesis that maxillary morphology
differs between OSAS patients and non-snoring, non-apnoea control subjects.
Patients had a smaller maxillary to mandibular and maxillary to facial width
ratios. These results suggest that OSA patients have narrower, more tapered and
shorter maxillary arches than the controls.

Review Of Literature
15
Armando Gale et al5 (2001) studied the hyoid bone position after surgical
mandibular advancement and concluded that with a surgical advancement of
the mandible the hyoid bone follows the advancement and moves closer to the
body of the mandible. However there are variations in the positions of the
hyoid bone and head position that are difficult to predict.
Anette M. C. Fransson et al3 (2002) in their study of influence of mandibular
protruding device on airway passages and dentofacial characteristics in
obstructive sleep apnoea and snoring evaluated the influence of a mandibular
protruding device (MPD) after 2 years of nocturnal usage on the upper airway
and its surrounding structures. They concluded that the nocturnal use of an MPD
for 2 years improved the airway passage because of an increase in the pharyngeal
area by a mean of 9% in OSA patients and snorers. A mandibular posterior
rotation and a proclination of the mandibular incisors were observed but
considered modest.
Takahashi.S and Ono.T et al79
(2002) conducted a study on breathing modes,
body positions, and suprahyoid muscle activity. Electromyographic activities of
genioglossus and geniohyoid muscles were recorded during both nasal and oral
breathing, with the subjects were in the both upright and supine positions. The
EMG activities of the genioglossus and geniohyoid muscles were compared
during mouth opening, swallowing, mandibular advancement, and tongue

Review Of Literature
16
protrusion. They concluded that EMG activities from the genioglossus and
geniohyoid muscles were differentiated well. Also, it appears that variations in
the breathing mode and body position significantly affect the genioglossus
activity and not that of the geniohyoid activity.
Lena Zettergren-Wijk et al50
(2002) evaluated longitudinal effect on facial
growth after tonsillectomy in children with obstructive sleep apnoea. They
studied 14 children with mean age of 5.7 years. Polysomnographic and lateral
cephalometric evaluation Preoperative, 1-year postoperative, and 3-year
postoperative revealed normalization of the facial growth after relief of the
obstruction (tonsillectomy) occurred mostly during the first postoperative year.
Siddik Malkoc, et al76
(2005) studied the Reproducibility of airway dimensions
and tongue and hyoid positions on lateral cephalograms. Three lateral
cephalograms each of 30 patients were obtained in natural head positions at 30-
minute intermissions. 12 measurements, including pharyngeal airway dimensions
and tongue and hyoid positions, were taken and analysed. They concluded that
airway dimension and tongue- and hyoid bone position measurements are highly
reproducible on natural-head-position cephalograms.

Review Of Literature
17
Mirja Kirjavainena & Turkka Kirjavainen61
(2007) studied the upper airway
dimensions in Class II malocclusion and effect of cervical headgear treatment on
it using lateral cephalograms. They concluded that Class II division 1
malocclusion is associated with narrower upper airway even without retrognathia.
Headgear treatment is associated with an increase in retropalatal airway space.
Craig Fairburn et al18
(2007) analysed the morphologic 3 dimensional changes
in the airway in OSA patients using CT scanning following maxillomandibular
advancement surgery. It resulted in a significant increase in both anteroposterior
and lateral airway dimensions.
Gunduz Arslan et al31
(2007) evaluated craniofacial and upper airway structures
in lateral cephalograms of patients with hypohydrotic ectodermal dysplasia,
whose characteristic features are Class III malocclusion with retrusion of maxilla,
and deficiency in vertical, transverse and sagittal growth of the jaw. Ectodermal
dysplasia patients have smaller pharyngeal and upper airway dimensions, and
hyoid bone is positioned more posteriorly compared with Class III control
individuals.
Maria Julia et al54
(2007) conducted a cephalometric assessment of the hyoid
bone position in Oral Breathing Children and concluded that the hyoid bone

Review Of Literature
18
keeps a stable position, probably in order to secure correct ratios in the airways,
and it does not depend on the respiratory pattern.
Yuko Shigeta et al86
(2008) examined the influence of age and gender on the
oropharynx configuration using the computed tomography measurements. They
concluded that the airway lengthens with aging specifically in males and
speculated that it becomes more collapsible. No significant relationship was
identified in females.
Dan Grauer et al19
(2009) assessed the differences in airway shape and volume
among subjects with various facial patterns, using CBCT. Both airway volume
and shape vary with different anteroposterior jaw relations; airway shape but not
volume differs with various vertical jaw relationships.
Tomonori Iwasaki et al80
(2009) evaluated the characteristic shape of
oropharyngeal airway in children with Class III malocclusion by cone beam
computed tomography (CBCT). The Class III malocclusion is associated with a
large and flat oropharyngeal airway compared with Class I malocclusion.
Emine Kaygısız et al23
(2009) appraised the effects of maxillary protraction and
fixed appliance therapy on the pharyngeal airway. 25 patients (11 girls, 14 boys;

Review Of Literature
19
mean age, 11.32 years) treated with a reverse pull headgear appliance were
assessed in their study. They concluded that the nasopharyngeal airway
dimensions improved after the treatment with maxillary protraction, and
favourable effects in pharyngeal airway remained over the post-treatment period
of 4 years.
Soonshin Hwang et al78
(2010) in their lateral cephalometric study assessed the
changes in hyoid, tongue, pharyngeal airway and head posture in patients who had
mandibular setback surgery by intraoral vertical ramus osteotomy. The hyoid and
tongue moved posteriorly after the setback but had a tendency to relapse back to
its original position. However, the final pharyngeal airway width remained
narrower even after long term observation period.
Zhe Zhong et al87
(2010) did a cephalometric 1comparison study of upper airway
among different sagittal and vertical facial morphologies in non-snoring children.
In normodivergent group, a tendency for reduced upper airway in inferior part
was found in Class III, I and Class II subgroups in that order; while in normal
sagittal pattern, the superior part of airway decreased with the increasing
mandibular plane angle. Thus, they concluded that sagittal and vertical skeletal
patterns may be contributory factors for variation in inferior and superior part of
upper airway, respectively.

Review Of Literature
20
Yoon-Ji Kim et al83
(2010) studied the three dimensional pharyngeal airway
volumes in healthy preadolescent children with different anteroposterior skeletal
patterns using CBCT. They compared the airway volume in children with a
retrognathic mandible and those with normal craniofacial growth, to study the
possible relationship among the studied cephalometric variables and airway
morphology. The mean total airway volume in retrognathic patients was
significantly smaller than that of normal skeletal relationship. However, the
difference in the volume of four sub regions of airway was not statistically
significant between the two groups.
Ashok Kumar Jena et al7 (2010) in their study of sagittal mandibular
development effects on the dimensions of the awake pharyngeal airway passage
concluded that sagittal mandibular development had significant effects on the
dimensions of the awake pharyngeal airway passage. The length of the soft
palate was smaller among subjects with mandibular prognathism than among
subjects with normal and retrognathic mandibles. The thickness of the soft
palate was greater among mandibular prognathic subjects than among subjects
with normal and retrognathic mandibles. Sagittal mandibular development had
a significant influence on the inclination of the soft palate. The dimensions of
the nasopharynx and hypopharynx were independent of sagittal mandibular
development. The depth of the oropharynx was greater among subjects with
mandibular prognathism than among subjects with normal and retrognathic
mandibles

Review Of Literature
21
Pirilä-Parkkinen.K et al66
(2010) in their study about Cephalometric evaluation
of children with nocturnal sleep-disordered breathing concluded that upper
airway resistance syndrome (UARS) and obstructive sleep apnoea (OSA) were
associated with decreased pharyngeal diameters at the levels of the adenoids
(PNS–ad1) and tip of the uvula (u1–u2), an increased diameter at the level of the
base of the tongue (rl1–rl2), a thicker soft palate, and anteriorly positioned maxilla
in relation to the cranial base. Lateral cephalograms may thus reveal important
predictors for sleep-disordered breathing (SDB) in children.
Kyung-Min Oh et al47
(2011) in their study of Three-dimensional analysis of
pharyngeal airway form in children with anteroposterior facial patterns
concluded that Children with Class II malocclusion have more backward
orientation and smaller volume of the pharyngeal airway than do children with
Class I and III malocclusion. Inclination of the oropharyngeal airway might be
a key factor in determining the form of the entire pharyngeal airway and is
related to head posture. In the skeletal Class II group, the average inclination of
Oropharyngeal airway was significantly larger and the Oropharyngeal airway in
the sagittal plane was shown as a more backward orientation to the FH plane.
Tomonori Iwasaki et al81
(2011) evaluated the upper airway obstruction in
dolichofacial and brachyfacial children with Class II malocclusion. The size of
the airway did not differ much between the two facial types. They developed a

Review Of Literature
22
fluid-mechanical stimulation system to detect the differences in airway
obstruction that were not apparent from other morphologic studies.
Gundega Jakobsone et al30
(2011) evaluated the effect of maxillary
advancement and impaction on the upper airway after bimaxillary surgery to
correct Class III malocclusion. They concluded that clinically significant
advancement (>2 mm) of the maxilla significantly increased the airway dimension
at the nasopharyngeal level and to some extent compensated for the effect of
mandibular setback at the hypopharyngeal level.
Derya Germec-Cakan et al22
(2011) compared the changes in Uvulo-
glossopharyngeal dimensions in non-extraction, extraction with minimum
anchorage and extraction with maximum anchorage. They concluded that superior
and middle airway size increased in subjects treated with extraction and minimum
anchorage. In patients treated non-extraction by air-rotor stripping, no significant
change was observed in airway dimensions. Middle and inferior airway size
narrowed in subjects treated with extraction and maximum anchorage.
Pirila-Parkkinen et al67
(2011) evaluated the validity of upper airway assessment
by comparing the capability of two-dimensional lateral cephalograms in
recognizing pharyngeal obstruction with that of the three-dimensional magnetic

Review Of Literature
23
resonance imaging and clinical observation of tonsillar size. The findings
confirmed that lateral cephalograms are a valid method for measuring dimensions
of nasopharyngeal and retropalatal region; and for evaluating oropharyngeal size,
clinical assessment of tonsillar size is a relatively reliable method.
Hakan El and Palomo32
(2011) evaluated the nasal passage and oropharyngeal
airway volumes of patients with different dentofacial skeletal patterns. The study
sample consisted of 140 patients which were divided into 3 groups according to
the ANB angle as Class I (1°≤ ANB ≤ 3
°), Class II (ANB > 3
°) and Class III (ANB
< 1°). The area of most constricted region at the base of the tongue had a high
potential of explaining the oropharyngeal airway volume; which was smaller for
Class II subjects when compared to Class I and Class III subjects. Mandibular
position with respect to cranial base had an effect on oropharyngeal airway
volume; but the only significant difference in nasopharyngeal volume was
between Class I and Class II groups, with a smaller volume observed in Class II
group.
Faruk Izzet Ucar and Tancan Uysal24
(2011) measured the oropharyngeal
airway dimensions in subjects with Class I malocclusion and different growth
patterns. 31 low angle, 40 high angle and 33 normal growth pattern cases with
Class I malocclusion were examined using lateral cephalometric radiographs.
Statistically significant differences were found in nasopharyngeal airway space,

Review Of Literature
24
palatal tongue space, and upper posterior airway space and tongue gap. No
significant orofacial airway differences were determined between low angle and
normal growth subjects. High angle subjects had larger tongue gap than those
with normal and low angle. Nasopharyngeal airway space and upper pharyngeal
airway space were larger and palatal tongue space was narrower in low angle than
high angle subjects.
Yoshihiko Takemoto et al84
(2011) evaluated the Pharyngeal airway in children
with prognathism and normal occlusion. 25 girls with prognathism and 15 girls
with normal occlusion were assessed in their study. They concluded that girls with
prognathic mandible had a significantly wider lower pharyngeal airway compared
with those with normal occlusion.
Austin Phoenix et al9 (2011) studied the changes in hyoid bone position
following rapid maxillary expansion in adolescents and noted that before
treatment, the hyoid to mandibular plane distance is greater in patients with
narrow maxillae requiring RME. They concluded that the hyoid to mandibular
plane distance significantly decreased post rapid maxillary expansion while the
tongue length remained unaffected. They suggested that RME treatment tends
to normalize hyoid bone position.

Review Of Literature
25
Ashok Kumar and Ritu Duggal6 (2011) studied the hyoid bone position in
subjects with different vertical jaw dysplasia and concluded that the
anteroposterior position of the hyoid bone was more forward in subjects with
short face syndrome. The vertical position of the hyoid bone was comparable
among subjects with different vertical jaw dysplasias. The axial inclination of
the hyoid bone closely followed the axial inclination of the mandible.
Qingzhu Wang, Peizeng Jia, Nina K. Anderson, Lin Wang and Jiuxiang
Lin70
(2012) in their study compared the Changes of pharyngeal airway size and
hyoid bone position following orthodontic treatment of Class I bimaxillary
protrusion concluded that following retraction of incisors, the velopharyngeal,
glossopharyngeal, and hypopharyngeal airway became narrower. The changes of
the pharyngeal airway size were no different between the hyperdivergent and non-
hyperdivergent groups. The hyoid bone tends to move in a posterior and inferior
direction. A significant relationship has been demonstrated between the reduction
of the velopharynx, glossopharynx, and the retraction distance of lower incisors in
their study.
Fitin Aloufi et al25
(2012) in their retrospective study about the changes in the
upper and lower pharyngeal airway spaces associated with rapid maxillary
expansion concluded that rapid maxillary expansion during orthodontic
treatment have a positive effect on the upper nasopharyngeal airway, with no

Review Of Literature
26
significant change on the lower pharyngeal airway. They also confirmed that
there was no significant difference with respect to mode of breathing.
Nanda Kishore Sahoo et al63
(2012) evaluated the upper airway dimensional
changes and hyoid position following mandibular advancement in patients with
skeletal Class II malocclusion. They quantified upper airway dimensional changes
and hyoid bone positional variation for a given degree of mandibular
advancement. They established a ratio of mandibular advancement to increase in
airway dimensions. The mean ratio of mandibular advancement to increase
Posterior Airway Space, Superior Airway Space, and Minimum Airway Space
was 1:0.35, 1:0.34, and 1:0.24, respectively. Hyoid bone moved superiorly and in
an anterior direction by 2.1 ± 2.8 mm.
Yu Chen et al85
(2012) evaluated the effect of large incisor retraction on upper
airway morphology in adult bimaxillary protrusion patients using three-
dimensional multi slice computed tomography. 30 adult patients with bimaxillary
protrusion treated with four first premolars extractions and miniscrews anchorage
were evaluated. They concluded that the hyoid was retracted in the horizontal and
vertical directions. No significant difference was observed in the cross-sectional
area of the nasopharynx, while significant differences were found in the mean
cross-sectional areas of the glossopharynx, palatopharynx and hypopharynx these

Review Of Literature
27
mean cross-sectional areas were decreased. The largest change in the cross-
sectional area is always noted in the hypopharynx.
Sila Mermut Gokce et al77
(2012) studied the relationship between Class III
malocclusion and hyoid bone displacement during swallowing by using
cinemagnetic resonance imaging and concluded that the forward and upward
displacements of the hyoid bone during bolus swallowing were significantly
related to craniofacial morphology. Although the pattern of hyoid bone movement
during swallowing was similar in patients with skeletal Class III malocclusion and
control subjects with normal occlusion, differences were noted in the degree of the
movement. Specifically, as the magnitude of the skeletal Class III deformity
increased, the amount of forward and upward displacement of the Hyoid bone
increased.
Halise Aydemir et al33
(2012) in their study of Pharyngeal airway space, hyoid
bone position and head posture after orthognathic surgery in Class III patients
concluded that different surgical procedures have different effects on pharyngeal
airway space. Mandibular setback surgeries cause the most narrowing effect on
the pharyngeal airway. Bimaxillary surgeries mostly decrease the narrowing effect
of the mandibular setback surgeries and must be preferred when planning these
cases. Maxillary advancement procedures have a widening effect on the
pharyngeal airway. No significant change occurs in craniocervical posture and
hyoid bone position after Class III orthognathic surgeries.

Materials and Methods
28
Materials and methods
In this study, the treatment records of 40 patients who underwent fixed
orthodontic treatment between the years 2006 to 2009 at Department Of
Orthodontics and Dentofacial Orthopaedics, Tamilnadu Government Dental
College and Hospital Chennai were analysed. Of 40 sets of standardized lateral
cephalometric radiographs 20 were Class I malocclusion and 20 were Class II
malocclusion. The control group consisting of 20 lateral cephalograms of subjects
with normal occlusion and good visibility of hyoid bone were used. The age range
was between 18 and 25 years. Inclusion and exclusion criteria were analysed from
the clinical records of the subjects.
Selection criteria:
The lateral cephalograms evaluated for this study were taken in natural head
position, with PLANMECA PM 2002 CC PROLINE machine 70kvp, 30mA, for
1.8seconds from fixed distance of 60 inches from the cephalostat available in the
Department Of Oral Medicine and Radiology, Tamilnadu Government Dental
College and Hospital Chennai. All cephalograms were taken in same cephalostat
with Frankfort horizontal plane of the subjects parallel to the floor. All
cephalograms were standardized using a transparent grid of 1mm accuracy and
Adobe Photoshop CS5. All the radiographs were scanned with CANON D520 MF
scanner and digitized. A Cephalometric analysis software AX CEPH version
2.3.0.74 was used to analyse the radiographs.

Materials and Methods
29
Inclusion criteria for Class I group:
Skeletal Class I (ANB 2º- 4º), Class I molar and canine relationship.
Both maxillary and mandibular arches with moderate to severe crowding 69
(4-10
mm - moderate to severe crowding according to Little’s irregularity index)
Orthodontic treatment with extraction of four first premolars.
Average BMI and Growth pattern.
No obvious hyperplasia of tonsils or adenoids on cephalograms.
Pretreatment and posttreatment radiographs with good soft and hard tissue outlines
with good visibility of the hyoid bone and teeth in full occlusion, lips resting in
natural position.
Inclusion criteria for Class II group:
Mild to moderate skeletal Class II (ANB 5º-7º), Class II molar and canine
relationship.
Both maxillary and mandibular arches with moderate to severe crowding 69
(4-10
mm – moderate to severe crowding according to Little’s irregularity index)
Orthodontic treatment with extraction of two first premolars in upper arch & two
second premolars in lower arch.
Average BMI and Growth pattern.
No obvious hyperplasia of tonsils or adenoids and tongue on cephalograms.

Materials and Methods
30
Pretreatment and posttreatment cephalograms with good soft and hard tissue with
good visibility of the hyoid bone outlines and teeth in full occlusion, lips resting in
natural position.
Exclusion criteria:
Craniofacial anomalies.
History of craniofacial trauma & pathology.
History of previous craniofacial surgery / orthodontic treatment.
History of abnormal oral habits.
History of nasal obstruction and allergic conditions.
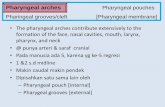
Cephalometric evaluation:
The pharynx is divided into of four different sections, nasopharynx, velopharynx,
glossopharynx, and hypopharynx. 7 parameters for these 4 sections of pharynx and
4 parameters for hyoid bone positions were selected and analysed 70
.
Cephalometric Landmarks and Measurements Analysed :
Table 1 : Cephalometric landmarks
Hor Most inferior point of spheno-occipital synchondrosis
R
Point of intersection of line from Hor to PNS and posterior
pharyngeal wall
Ba Lowermost point on anterior margin of foramen magnum
Ad1 Point of intersection of posterior pharyngeal wall and line Ptm-Ba

Materials and Methods
31
SPPW
Point of intersection of line from soft palate center perpendicular to
posterior pharyngeal wall and posterior pharyngeal wall
SPP
Point of intersection of line from soft palate center perpendicular to
posterior pharyngeal wall and posterior margin of soft palate
U The tip of the uvula
MPW
Foot point of perpendicular line from point U to posterior
pharyngeal wall
TPPW
Point of intersection of posterior pharyngeal wall and
extension of line B-Go
V The most posteroinferior point on the base of the tongue
TB
Point of intersection of base of the tongue & extension of
line B-Go
LPW
Foot point of perpendicular line from point V to posterior
pharyngeal wall
E Base of epiglottis.
C3 The most anteroinferior point of the third vertebra
H The most superior and anterior point of hyoid bone
RGN The most protrusive point of retrognathion
H1 Foot point of perpendicular line from RGN to C3

Materials and Methods
32
Table 2 :Airway Parameters (in mm)
VAL
Vertical airway length, distance
between PNS and V
PNS-R Distance between PNS and R.
PNS-Ad1 Distance between PNS and Ad1.
SPP-SPPW Distance between SPP and SPPW.
U-MPW Distance between U and MPW.
TB-TPPW Distance between TB and TPPW.
U-MPW Distance between U and MPW.
TB-TPPW Distance between TB and TPPW.
V-LPW Distance between V and LPW.
Table 3: Hyoid Position Parameters (in mm)
HRgn , mm Distance between H and RGN
HH1, mm Distance between H and H1
C3H, mm Distance between C3 and H
SH, mm Distance between S and H
Table 4 :Dentofacial Parameters
ANB, degrees Angle between point A and B at nasion
FH-MP, degrees Angle between the mandibular plane and the FH plane
U1-FH, degrees Angle between the FH plane & long axis of upper incisors
L1-MP, degrees Angle between the mandibular plane and long axis of lower

Materials and Methods
33
incisors
UL-E line, mm
Horizontal distance from the most protrusive point of upper
lip to E line
LL-E line, mm
Horizontal distance from the most protrusive point of lower
lip to E line
U1FHp, mm
Horizontal distance from the tip of the upper incisor crown to
constructed FH plane vertical
L1FHp, mm
Horizontal distance from the tip of the lower incisor crown to
constructed FH plane vertical
U6FHp, mm
Horizontal distance from the distal point of the upper first
molar crown to constructed FH plane vertical
L6FHp, mm
Horizontal distance from the distal point of the lower first
molar crown to constructed FH plane vertical
The process of digitization, landmark identification and analysis for all
cephalograms were carried out by same investigator. The intra-examiner reliability
was evaluated by re-recording the measurements at three weeks interval.

Materials and Methods
34
Cephalostat
CANON D520 MF scanner

Materials and Methods
35
Standardization with Transparent Grid
Standardization with Adobe Photoshop CS5

Materials and Methods
36
Ax Ceph Cephalometric Analysis Software
Analysis of digitized lateral cephalograms – Control subject

Materials and Methods
37
Analysis of digitized lateral cephalograms of Class I subject - pretreatment
Analysis of digitized lateral cephalograms of Class I subject - posttreatment

Materials and Methods
38
Analysis of digitized lateral cephalograms of Class II subject - pretreatment
Analysis of digitized lateral cephalograms of Class II subject - posttreatment

Statistical Analysis
39
Statistical Analysis
The data collected during the study was recorded in Microsoft Excel
Spreadsheet. The data was subjected to data analysis using Statistical Package for
Social Sciences (SPSS) software version 17. Within group differences in data
pertaining to airway dimension parameters, hyoid bone position parameters and
Dentofacial parameters among Class I and Class II malocclusion group before and
after treatment was compared using paired t test. Between group differences in the
above parameters among subjects with ideal group, Class I group and Class II
group was compared using one way ANOVA.
The intra-examiner reliability in recording the measurements was assessed
using Cronbach’s alpha method.
For all the analysis, p value of < 0.05 was considered to be statistically
significant.

Results
40
RESULTS
Table 5: Distribution of study subjects based on their gender
Gender Normoocclusion
(n) Class I group (n) Class II group (n)
Male 10 9 12
Female 10 11 8
Chi square value – 0.93 df – 2 p value - 0.62 (NS)
10
9
12
10
11
8
0
2
4
6
8
10
12
14
Normoocllusion (n) Class I (n) Class II (n)
male
female
Nu
mb
er o
f su
bje
cts

Results
41
Table 6: Distribution of study subjects based on their age
Type of occlusion Mean age S.D F value p value
Normoocclusion 21.2 1.92
2.74 0.07 (NS) Class I group 21.4 1.81
Class II group 21.05 1.76
The intra-examiner reliability was evaluated by re-recording the
measurements at three weeks interval. The kappa value for reliability was found
to be 0.84 denoting a high level of consistency in recording the measurements at
two different time period.
20.8
20.9
21
21.1
21.2
21.3
21.4
Normoocclusion CLASS I CLASS II
Age

Results
42
Table 7: Comparison of Airway related parameters among study subjects within
Class I malocclusion group
Variable Mean Std.
Devn
Mean
difference t value df
p
value
PNS –R
(mm)
Pre-treatment 22.36 1.66 -0.20 -3.27 19 0.004
Post-treatment 22.55 1.65
PNS -Ad1
(mm)
Pre-treatment 31.45 1.21 0.26 3.69 19 0.002
Post-treatment 31.20 1.33
SPP-
SPPW
(mm)
Pre-treatment 17.95 1.00 0.36 4.07 19 0.001
Post-treatment 17.58 1.10
U-MPW
(mm)
Pre-treatment 11.39 0.97 0.60 3.33 19 0.004
Post-treatment 10.79 1.21
TB-
TPPW
(mm)
Pre-treatment 10.85 0.95 0.73 5.91 19 0.001
Post-treatment 10.12 0.95
V-LPW
(mm)
Pre-treatment 14.08 1.37 1.14 14.44 19 0.001
Post-treatment 12.93 1.41
VAL
(mm)
Pre-treatment 60.72 1.39 -0.95 -6.42 19 0.001
Post-treatment 61.67 1.35
Table 8: Comparison of Hyoid position related parameters among study subjects
within Class I malocclusion group
Variable Mean Std.
Devn
Mean
difference t value df p value
HRGN
(mm)
Pre-treatment 34.30 1.27 -1.04 -6.46 19 0.001
Post-treatment 35.34 1.31
HH1
(mm)
Pre-treatment 3.58 0.81 -0.38 -2.28 19 0.035
Post-treatment 3.95 0.69
C3H
(mm)
Pre-treatment 38.18 1.25 0.89 7.68 19 0.001
Post-treatment 37.29 1.16
SH
(mm)
Pre-treatment 91.74 3.13 -1.30 -9.40 19 0.001
Post-treatment 93.04 2.89

Results
43
Table 9: Comparison of Dento-facial related parameters among study subjects
within Class I malocclusion group
Variable Mean Std.
Deviation
Mean
difference t value df
p
value
ANB
(degree)
Pre-treatment 3.11 0.71 -0.11 -1.67 19 0.112
Post-treatment 3.22 0.64
FH-MP
(degree)
Pre-treatment 25.27 2.11 -0.37 -4.72 19 0.001
Post-treatment 25.63 2.15
U1-FH
(degree)
Pre-treatment 128.64 4.41 14.92 38.16 19 0.001
Post-treatment 113.73 3.64
L1-MP
(degree)
Pre-treatment 100.50 4.30 6.51 21.77 19 0.001
Post-treatment 94.00 3.46
UL-Eline
(mm)
Pre-treatment 3.23 1.18 2.13 11.37 19 0.001
Post-treatment 1.10 0.47
LL-Eline
(mm)
Pre-treatment 5.28 0.84 3.24 22.19 19 0.001
Post-treatment 2.04 0.53
U1-FHP
(mm)
Pre-treatment 79.19 2.62 6.26 25.76 19 0.001
Post-treatment 72.93 2.69
L1-FHP
(mm)
Pre-treatment 75.27 2.28 4.70 24.47 19 0.001
Post-treatment 70.57 2.31
U6-FHP
(mm)
Pre-treatment 40.11 1.40 -0.60 -7.78 19 0.001
Post-treatment 40.71 1.53
L6-FHP
(mm)
Pre-treatment 40.55 1.40 -0.62 -8.57 19 0.001
Post-treatment 41.17 1.62

Results
44
Table 10: Comparison of Airway related parameters among study subjects within
Class II malocclusion group
Table 11: Comparison of Hyoid position parameters among study subjects within
Class II malocclusion group
Variable Mean Std.
Devn
Mean
difference t value df p value
HRGN
(mm)
Pre-treatment 36.41 2.59 .38 14.90 19 0.001
Post-treatment 36.03 2.58
HH1
(mm)
Pre-treatment 2.73 .81 .49 8.67 19 0.001
Post-treatment 2.24 .79
C3H
(mm)
Pre-treatment 34.79 2.37 -.94 -10.98 19 0.001
Post-treatment 35.73 2.37
SH
(mm)
Pre-treatment 93.85 3.64 1.19 6.72 19 0.001
Post-treatment 92.66 3.73
Variable Mean Std.
Devn
Mean
difference t value df p value
PNS –R
(mm)
Pre-treatment 25.45 1.34 .46 3.63 19 .002
Post-treatment 24.99 1.38
PNS -Ad1
(mm)
Pre-treatment 34.55 1.36 .78 3.47 19 .003
Post-treatment 33.78 1.83
SPP-SPPW
(mm)
Pre-treatment 16.48 1.24 -.09 -.73 19 .476
Post-treatment 16.57 1.16
U-MPW
(mm)
Pre-treatment 13.85 1.04 -1.05 -12.46 19 0.001
Post-treatment 14.91 1.07
TB-TPPW
(mm)
Pre-treatment 11.06 1.23 -1.29 -14.23 19 0.001
Post-treatment 12.35 1.06
V-LPW
(mm)
Pre-treatment 11.03 1.32 -2.31 -21.59 19 0.001
Post-treatment 13.34 1.32
VAL
(mm)
Pre-treatment 55.95 2.20 -1.31 -8.29 19 0.001
Post-treatment 57.26 2.49

Results
45
Table 12: Comparison of Dento facial related parameters among study subjects
within Class II malocclusion group
variable Mean Std.
Devn
Mean
difference t value df p value
ANB
(degree)
Pre-treatment 5.98 .79
.67 11.05 19 0.001
Post-treatment 5.31 .67
FH-MP
(degree)
Pre-treatment 26.03 1.59
-.75 -8.20 19 0.001
Post-treatment 26.78 1.60
U1-FH
(degree)
Pre-treatment 125.93 3.78
11.72 22.21 19 0.001
Post-treatment 114.21 3.32
L1-MP
(degree)
Pre-treatment 101.78 4.78
7.45 13.29 19 0.001
Post-treatment 94.33 3.53
UL-Eline
(mm)
Pre-treatment 4.41 1.06
2.66 12.83 19 0.001
Post-treatment 1.75 .29
LL-Eline
(mm)
Pre-treatment 5.36 .81
3.34 27.10 19 0.001
Post-treatment 2.02 .32
U1-FHP
(mm)
Pre-treatment 87.72 2.28
5.25 29.13 19 0.001
Post-treatment 82.47 1.86
L1-FHP
(mm)
Pre-treatment 83.64 2.09
3.09 21.21 19 0.001
Post-treatment 80.56 2.21
U6-FHP
(mm)
Pre-treatment 40.38 1.14
-.64 -5.61 19 0.001
Post-treatment 41.02 1.36
L6-FHP
(mm)
Pre-treatment 38.76 1.18
-3.23 -14.13 19 0.001
Post-treatment 41.99 1.21

Results
46
TABLE 13: Comparison of airway parameters between Class I and Class II
malocclusion groups
Class N Mean Std. Devn
Std. Error
Mean
PNS-R
PRE
Class 1 20 22.3560 1.66376 .37203
Class 2 20 25.4455 1.33739 .29905
PNS-R
POST
Class 1 20 22.554 1.6472 .3683
Class 2 20 24.987 1.3848 .3096
PNS-AD1
PRE
Class 1 20 31.4545 1.21288 .27121
Class 2 20 34.5525 1.36179 .30451
PNS-AD1
POST
Class 1 20 31.198 1.3254 .2964
Class 2 20 33.775 1.8265 .4084
SPP-SPPW
PRE
Class 1 20 17.9450 1.00384 .22447
Class 2 20 16.4785 1.23577 .27633
SPP-SPPW
POST
Class 1 20 17.5810 1.09900 .24574
Class 2 20 16.5680 1.15832 .25901
U-MPW
PRE
Class 1 20 11.3905 .96696 .21622
Class 2 20 13.8520 1.04164 .23292
U-MPW
POST
Class 1 20 10.7900 1.21063 .27071
Class 2 20 14.9055 1.06762 .23873
TB – TPPW
PRE
Class 1 20 10.8480 .95446 .21342
Class 2 20 11.0585 1.22819 .27463
TB – TPPW
POST
Class 1 20 10.1220 .95095 .21264
Class 2 20 12.3500 1.05607 .23614
V-LPW
PRE
Class 1 20 14.0780 1.37332 .30708
Class 2 20 11.0280 1.31877 .29489
V-LPW
POST
Class 1 20 12.9340 1.41081 .31547
Class 2 20 13.3425 1.31865 .29486
VAL
PRE
Class 1 20 60.716 1.3861 .3100
Class 2 20 55.946 2.1985 .4916
VAL
POST
Class 1 20 61.666 1.3455 .3009
Class 2 20 57.257 2.4904 .5559

Results
47
Table 14: Comparison of Airway Parameters between Class I And Class II
Malocclusion Groups - Independent Samples Test
Levene's
test
for
Equality
of
Variances
t-test for Equality of Means
F Sig. t df
Sig.
(2-
tailed)
Mean
Difference
Std. Error
Difference
PNS-R
PRE
Equal
variances
assumed
.927 .342 -6.473 38 <.001 -3.0895 .47732
Equal
variances not
assumed
-6.473 36.322 <.001 -3.0895 .47732
PNS-R
POST
Equal
variances
assumed
.757 .390 -5.055 38 <.001 -2.432 .4812
Equal
variances not
assumed
-5.055 36.910 <.001 -2.432 .4812
PNS-
AD1
PRE
Equal
variances
assumed
.875 .355 -7.597 38 <.001 -3.0980 .40777
Equal
variances not
assumed
-7.597 37.502 <.001 -3.0980 .40777
PNS-
AD1
POST
Equal
variances
assumed
3.607 .065 -5.107 38 <.001 -2.577 .5046
Equal
variances not
assumed
-5.107 34.666 <.001 -2.577 .5046
SPP-
SPPW
PRE
Equal
variances
assumed
.776 .384 4.119 38 <.001 1.4665 .35601
Equal
variances not
assumed
4.119 36.469 <.001 1.4665 .35601
SPP-
SPPW
POST
Equal
variances
assumed
.007 .936 2.837 38 .007 1.0130 .35704
Equal
variances not
assumed
2.837 37.895 .007 1.0130 .35704
U-
MPW
PRE
Equal
variances
assumed
.223 .640 -7.745 38 <.001 -2.4615 .31781
Equal
variances not
assumed
-7.745 37.792 <.001 -2.4615 .31781

Results
48
U-
MPW
POST
Equal
variances
assumed
.001 .982 -
11.402 38 <.001 -4.1155 .36093
Equal
variances not
assumed
-
11.402 37.415 <.001 -4.1155 .36093
TB –
TPPW
PRE
Equal
variances
assumed
1.350 .253 -.605 38 .549 -.2105 .34781
Equal
variances not
assumed
-.605 35.816 .549 -.2105 .34781
TB –
TPPW
POST
Equal
variances
assumed
1.214 .277 -7.011 38 <.001 -2.2280 .31777
Equal
variances not
assumed
-7.011 37.590 <.001 -2.2280 .31777
V-
LPW
PRE
Equal
variances
assumed
.053 .820 7.164 38 <.001 3.0500 .42574
Equal
variances not
assumed
7.164 37.938 <.001 3.0500 .42574
V-
LPW
POST
Equal
variances
assumed
.271 .605 -.946 38 .350 -.4085 .43181
Equal
variances not
assumed
-.946 37.828 .350 -.4085 .43181
VAL
PRE
Equal
variances
assumed
5.365 .026 8.206 38 <.001 4.769 .5812
Equal
variances not
assumed
8.206 32.045 <.001 4.769 .5812
VAL
POST
Equal
variances
assumed
5.890 .020 6.966 38 <.001 4.409 .6329
Equal
variances not
assumed
6.966 29.222 <.001 4.409 .6329

Results
49
Table 15: Comparison of hyoid position related parameters between Class I and
Class II malocclusion groups.
Class N Mean Std. Deviation Std. Error
Mean
H-RGN
PRE
Class 1 20 34.2990 1.26646 .28319
Class 2 20 36.4110 2.59176 .57954
H-RGN
POST
Class 1 20 35.3360 1.31194 .29336
Class 2 20 36.0305 2.58043 .57700
HH1
PRE
Class 1 20 3.5775 .80951 .18101
Class 2 20 2.7280 .80983 .18108
HH1
POST
Class 1 20 3.9525 .69208 .15475
Class 2 20 2.2400 .79382 .17750
C3H
PRE
Class 1 20 38.1810 1.25319 .28022
Class 2 20 34.7930 2.36943 .52982
C3H
POST
Class 1 20 37.288 1.1603 .2594
Class 2 20 35.733 2.3734 .5307
SH
PRE
Class 1 20 91.7360 3.13418 .70082
Class 2 20 93.8490 3.64104 .81416
SH
POST
Class 1 20 93.037 2.8947 .6473
Class 2 20 92.664 3.7273 .8335
Table 16: Comparison of hyoid position related parameters between subjects with
Class I and Class II occlusion - Independent Samples Test
Levene's Test
for Equality
of Variances
t-test for Equality of Means
F Sig. t df Sig.(2-
tailed)
Mean
Difference
Std. Error
Difference
H-
RGN
PRE
Equal
variances
assumed
14.986 .000 -
3.274 38 .002 -2.1120 .64502
Equal
variances not
assumed
-
3.274 27.584 .003 -2.1120 .64502
H-
RGN
POST
Equal
variances
assumed
14.247 .001 -
1.073 38 .290 -.6945 .64729
Equal
variances not
-
1.073 28.207 .292 -.6945 .64729

Results
50
assumed
HH1
PRE
Equal
variances
assumed
.014 .908 3.318 38 .002 .8495 .25604
Equal
variances not
assumed
3.318 38.000 .002 .8495 .25604
HH1
POST
Equal
variances
assumed
.357 .553 7.272 38 <.001 1.7125 .23549
Equal
variances not
assumed
7.272 37.307 <.001 1.7125 .23549
C3H
PRE
Equal
variances
assumed
8.663 .006 5.653 38 <.001 3.3880 .59936
Equal
variances not
assumed
5.653 28.859 <.001 3.3880 .59936
C3H
POST
Equal
variances
assumed
8.561 .006 2.631 38 .012 1.555 .5907
Equal
variances not
assumed
2.631 27.591 .014 1.555 .5907
SH
PRE
Equal
variances
assumed
.121 .730 -
1.967 38 .057 -2.1130 1.07425
Equal
variances not
assumed
-
1.967 37.177 .057 -2.1130 1.07425
SH
POST
Equal
variances
assumed
1.002 .323 .353 38 .726 .373 1.0553
Equal
variances not
assumed
.353 35.806 .726 .373 1.0553

Results
51
Table 17: Comparison of airway related parameters between subjects
with Normal, Class I and Class II occlusion at baseline (mm)
Variable Normal
subjects
Class I
subjects
Class II
subjects F value* p value
PNS –R
(mm) 22.6 22.36 25.45 15.17 < 0.001
PNS -Ad1
(mm) 28.61 31.45 34.55 37.11 < 0.001
SPP-SPPW
(mm) 15.95 17.95 16.48 3.72 0.03
U-MPW
(mm) 10.78 11.39 13.85 34.10 < 0.001
TB-TPPW
(mm) 10.34 10.85 11.06 0.85 0.43
V-LPW
(mm) 15.11 14.08 11.03 25.5 < 0.001
VAL
(mm) 59.54 60.72 55.95 12.91 < 0.001
*One way ANOVA
Table 18: Comparison of airway related parameters between subjects
with Normal, Class I and Class II occlusion post treatment (mm)
Variable Normal subjects
Class I
subjects
Class II
subjects
F value* p value
PNS –R
(mm) 22.6 22.55 24.99 9.92 < 0.001
PNS -Ad1
(mm) 28.61 31.2 33.78 24.94 < 0.001
SPP-SPPW
(mm) 15.95 17.58 16.57 2.34 0.104
U-MPW
(mm) 10.78 10.79 14.91 65.02 < 0.001
TB-TPPW
(mm) 10.34 10.12 12.35 9.78 < 0.001
V-LPW
(mm) 15.11 12.93 13.34 7.52 0.001
VAL
(mm) 59.54 61.67 57.26 9.75 < 0.001
*One way ANOVA

Results
52
Table 19: Comparison of hyoid position related parameters between
subjects with Normal, Class I and Class II occlusion baseline (mm)
Variable Normal
subjects
Class I
subjects
Class II
subjects F value* p value
HRGN
(mm) 36.95 34.30 36.41 3.05 0.05
HH1 (mm) 3.16 3.58 2.73 0.75 0.47
C3H (mm) 39.00 38.18 34.79 8.22 < 0.001
SH (mm) 97.23 91.74 93.85 5.85 0.004
*One way ANOVA
Table20: Comparison of hyoid position related parameters between
subjects with Normal, Class I and Class II occlusion post treatment
(mm)
Variable Normal
subjects
Class I
subjects
Class II
subjects
F
value*
p
value
Mean HRGN
(mm) 36.95 35.34 36.03 1.01 0.36
Mean HH1 (mm) 3.16 3.95 2.24 3.12 0.05
Mean C3H (mm) 39.00 37.29 35.73 4.44 0.01
Mean SH (mm) 97.23 93.04 92.66 4.96 0.01
*One way ANOVA

Results
53
Table 21– Changes In Airway dimension And Hyoid bone position – Based On
Gender
Levene's
Test for
Equality of
Variances
t-test for Equality of Means
F Sig. t df
Sig.
(2-
tailed)
Mean
Difference
Std. Error
Differenc
e
Pns-R
pre
Equal variances
assumed 3.561 .075 -.164 18 .871 -.1261 .76772
Equal variances
not assumed -.174 15.970 .864 -.1261 .72524
Pns-R
post
Equal variances
assumed 3.899 .064 -.040 18 .969 -.030 .7606
Equal variances
not assumed -.042 15.818 .967 -.030 .7175
Pns-Ad1
Pre
Equal variances
assumed 1.348 .261 .220 18 .828 .1231 .55934
Equal variances
not assumed .215 15.078 .833 .1231 .57335
Pns Ad1
Post
Equal variances
assumed 2.126 .162 .016 18 .988 .010 .6120
Equal variances
not assumed .015 13.513 .988 .010 .6371
SPP-
SPPW
Pre
Equal variances
assumed .423 .524 .365 18 .719 .1687 .46185
Equal variances
not assumed .358 15.609 .725 .1687 .47086
SPP-
SPPW
Post
Equal variances
assumed .577 .457 -.039 18 .969 -.0200 .50748
Equal variances
not assumed -.039 15.847 .970 -.0200 .51609
U-MPW
Pre
Equal variances
assumed .449 .511 -.457 18 .653 -.2029 .44395
Equal variances
not assumed -.456 17.002 .654 -.2029 .44537
U-MPW
Post
Equal variances
assumed 3.864 .065 -1.296 18 .211 -.6929 .53466
Equal variances
not assumed -1.215 11.139 .250 -.6929 .57037
TB-
TPPW
Pre
Equal variances
assumed .962 .340 .293 18 .773 .1289 .43971
Equal variances
not assumed .301 17.942 .767 .1289 .42767
TB-
TPPW
Post
Equal variances
assumed .482 .497 .167 18 .869 .0731 .43879

Results
54
Equal variances
not assumed .161 14.297 .874 .0731 .45327
V-LPW
Pre
Equal variances
assumed .114 .739 .683 18 .503 .4279 .62611
Equal variances
not assumed .681 16.995 .505 .4279 .62815
V-LPW
Post
Equal variances
assumed .700 .414 .680 18 .505 .4372 .64329
Equal variances
not assumed .685 17.675 .502 .4372 .63811
VAL
pre
Equal variances
assumed .040 .843 .190 18 .852 .121 .6395
Equal variances
not assumed .192 17.889 .850 .121 .6306
VAL
Post
Equal variances
assumed 1.491 .238 .752 18 .462 .460 .6118
Equal variances
not assumed .729 14.553 .477 .460 .6304
H-RGN
Pre
Equal variances
assumed 1.250 .278 -.350 18 .730 -.2042 .58284
Equal variances
not assumed -.334 12.860 .743 -.2042 .61064
H-RGN
post
Equal variances
assumed .404 .533 .380 18 .708 .2295 .60341
Equal variances
not assumed .374 15.862 .713 .2295 .61356
HH1
pre
Equal variances
assumed .536 .474 -.756 18 .459 -.2783 .36802
Equal variances
not assumed -.761 17.579 .457 -.2783 .36579
HH1
Post
Equal variances
assumed 1.801 .196 -1.875 18 .077 -.5480 .29233
Equal variances
not assumed -1.947 17.563 .068 -.5480 .28150
C3H
pre
Equal variances
assumed .041 .843 -.248 18 .807 -.1432 .57772
Equal variances
not assumed -.248 17.147 .807 -.1432 .57837
C3H
Post
Equal variances
assumed .028 .869 -.797 18 .436 -.420 .5266
Equal variances
not assumed -.802 17.602 .433 -.420 .5232
SH
pr
Equal variances
assumed 1.725 .206 -.588 18 .564 -.8432 1.43360
Equal variances
not assumed -.571 14.667 .576 -.8432 1.47551
SH
post
Equal variances
assumed 2.796 .112 -.532 18 .601 -.706 1.3264
Equal variances
not assumed -.507 12.719 .621 -.706 1.3916

Discussion
55
Discussion
Pharyngeal airway dimensions, narrowing of pharyngeal passage and
hyoid bone positions are of interest in orthodontics. Several studies have
indicated that there are significant relationships between pharyngeal
dimensions and craniofacial abnormalities.
Nasopharyngeal airway area increases rapidly until 13 years of age and
after this the growth slows down. An inactive period of growth in pharyngeal
structures has been reported beyond 15 years of age.16,82,42,51,59
. Chang min et
al 15
reported the developmental changes on pharynx and hyoid position. By 3
years of age the hyoid lies at a level between 3rd and 4th cervical vertebrae and
descends to the level of the 4th vertebrae at adulthood. Later during growth the
relative position of the hyoid remains constant.14,74
. Literature findings indicate
that growth may have little effect if any on the sagittal depth of the pharyngeal
airway.
This study was performed to evaluate the changes in the pharyngeal
airway dimensions and the hyoid bone position following nonsurgical
orthodontic treatment in class I and class II subjects with moderate to severe
crowding and compared with normoocclusion using lateral cephalometric
radiograph. In the present study subjects of 18 – 25 years of age were
evaluated.
As this analytical study was retrospective in nature, direct assessment of
the respiratory pattern for individual patient was not possible. The medical

Discussion
56
history and dental history recorded in the clinical orthodontic records were
analysed for the criteria for selection of the subjects. Prior history about
tonsillectomy and respiratory infections were considered. Any one of these
factors could have been related to respiratory obstructions 44, 62
. Patients with a
positive history of airway obstructions and other craniofacial abnormalities
were excluded from the study. All the subjects in this study had normal BMI
and were treated with extractions followed by straight wire appliance 0.022”
Roth prescription.
Husamettin Oktay 36
and Hiroyuki Ishikawa et al 35
reported that ANB
angle was considered to be the reliable indicator of the anteroposterior skeletal
discrepancy. Although clinical significance and reliability of the ANB angle to
determine the anteroposterior jaw relationship was argued in the literature, it is
still a widely used method to describe anteroposterior dentofacial discrepancies
and thus was the measurement of choice for this study to group the subjects. In
our study, subjects with ANB angle between 2-4º were included in Class I
group and subjects with ANB angle 5-7º were included in Class II group.
Normal respiration is dependent on sufficient anatomical dimensions of
the airway. Many studies have contributed to the knowledge that variations in
the skeletal pattern could lead to upper airway obstruction.55
The pharyngeal airway is an irregular lumen. Narrowing in one or more
segments of the airway may induce breathing as well as sleeping problems like
obstructive apnoea. Cross sectional area is a better indicator than volume with

Discussion
57
which to evaluate change in the size of the pharyngeal airway. The size of the
pharyngeal airway on lateral cephalograms can be measured as the depth and
height in the sagittal plane. So there is an inherent limitation of the study as
pharyngeal airway is a three-dimensional structure and it can only be evaluated
two dimensionally on lateral cephalometric films. However, Miles et al.
reported a high reliability of cephalometric landmarks and measurements 60
.
Aboudara et al 13
showed that the resistance to airflow is related to
airway size as well as form. So if the airway has a large volume but is bent,
then the airway resistance could greatly affect respiration. An airflow test,
nasoendoscope examination, nasal resistance measures, lateral cephalograms ,
Magnetic Resonance Imaging, Computed tomography, Cone Beam CT are
used for diagnosing nasal obstruction. Lateral cephalograms particularly have
been a very helpful tool because of their simplicity, low cost, and
reproducibility13, 67
. In our study, lateral cephalograms were used to analyse the
pharyngeal airway dimension and hyoid bone positions.
The process of converting the analogue information into digital form is
called digitization. Quantitative, systematic, and objective measurements based
on hard and soft tissue landmarks determined on cephalometric films are used
in orthodontics as a valuable tool in orthodontics. Korkmaz Sayinsu et al 46
and
Cleomar Donizeth Rodrigues et al 17
confirmed that there was no statistically as
well as clinically significant difference in the tracings between digitized
cephalograms, direct digital and conventional methods. In the present study

Discussion
58
lateral cephalograms were digitized using Canon D520 Mf scanner and
analysed using Ax Ceph version 2.3.0.74 software.
Mergen D.C and Jacobs R.M20
in their study measured the size of
nasopharynx (upper pharyngeal airway); and compared it between those with
normal Class I occlusion and Class II malocclusion. They concluded that the
midsagittal nasopharyngeal area was significantly greater in subjects with
normal class I occlusion than in those with Class II malocclusion. Oscar Martin
et al65
tried to describe the nasopharyngeal patterns in patients with ideal
occlusions and found that nasal fossa, cranial base, and adenoid tissue were
larger in men than in women. However, Marcos Roberto de Freitas et al53
did
not find any correlation between the upper pharyngeal airway in Class I and
Class II malocclusion types; but concluded that those with vertical growth
pattern have narrower upper airway dimensions.
In this pharyngeal dimension study, Class I and Class II malocclusion
(skeletal and dental) subjects with crowding grades from 4 to 10 mm69
analysed
from the models (Little’s irregularity index – moderate to severe) were
included and compared with normoocclusion subjects.
All subjects in this group were treated with extraction of four first
premolars. In class II group all subjects were treated with extraction of two
maxillary first premolars and two mandibular second premolars .The extraction
space was utilized for correction of crowding and mild proclination.

Discussion
59
A significant correlation was observed among the extent of central
incisor retraction, the amount of hyoid retraction in the horizontal direction,
and the change in the cross-sectional area of the hypopharynx85
. The main
reason for the narrowing of the hypopharynx may be the retraction of the
hyoid, which was caused by the retraction of the central incisor. Previous
studies have shown a possible relationship between hypopharynx and skeletal
structures, soft tissues, and musculature.55, 78
.
In the present study, changes in the nasopharynx, velopharynx,
glossopharynx and hypopharynx dimensions and hyoid bone positions were
measured according to the methods followed by Zhe zhong et al 87
and Alan
Lowe et al1. These changes were compared with the normoocclusion control
group.
The mean differences in the dimensions of nasopharynx, velopharynx,
glossopharynx and hypopharynx of Class I group and Class II Group following
orthodontic treatment were compared (Table 7 and Table 10).
In our study, there was a significant overall reduction in the pharyngeal
airway after orthodontic treatment in Class I group. Compared to the
palatopharynx and oropharynx, the cross sectional areas of glossopharynx and
hypopharynx were significantly reduced (p value 0.001) more after the
treatment. Nasopharynx and oropharynx were reduced by 0.26mm and 0.6mm
respectively whereas glossopharynx and hypopharynx were reduced by
0.73mm and 1.14mm respectively. These findings were coinciding with the

Discussion
60
results of the study by Qingzhu Wang 70,
, Derya Germec-Cakan et al22,
and Yu
Chen85
. This amount of decrease cannot be explained by growth changes and
might be due to narrowing of the tongue space after incisor retraction.
But our results differed from the result of a study by Valiathan et al 52
in
which they demonstrated that oropharyngeal volumes did not show significant
change after orthodontic treatment with extraction of four premolars in
adolescents. This negative finding may be attributed to mandibular growth as
their study group had subjects in the age range of 11 – 13 years and the high
variability of oropharyngeal volume.
However, in our study, it was not the same in case of Class II group. The
nasopharyngeal airway dimensions were reduced after treatment significantly
(p value 0.002) but the velopharynx, glossopharynx and hypopharynx areas
were significantly increased by 1.05mm , 1.29mm and 2.31mm respectively (p
value 0.001) following treatment. A possible explanation for this increase in
airway might be an increase in posterior tongue space after forward movement
of mandible due to the use of orthodontic mechanotherapy for Class II
corrections. The average mesial molar movement was 3.23 mm (TABLE 12) in
this group.
The importance of hyoid bone lies in its distinctive relationships. It has
no bony articulations but provides attachment for muscles, ligaments,
mandible, fascia of the pharynx and cranium 29, 73
. A close association of the
hyoid bone to the cartilages of the larynx also suggests the importance of hyoid
in the performance of both respiration and deglutition. The anteroposterior

Discussion
61
position of the hyoid bone follows the anteroposterior position of the chin.
When the mandible was rotated in counter clockwise direction, the suprahyoid
muscles pulled the hyoid bone to move into a more anterior position, and when
the mandible was rotated in a clockwise direction, the hyoid bone moved
posteriorly.
Yu Chen et al75
and Qingzhu Wang et al85
demonstrated a significant
change in position of hyoid bone following orthodontic treatment in Class I
bimaxillary protrusion cases. The hyoid bone was retracted postero inferiorly
after treatment. Masayoshi Kawakami et al55
confirmed that the vertical and
horizontal spaces around the tongue were maintained postoperatively with the
backward and downward movement of the hyoid, which compensates for the
reduction in oral volume after mandibular setback surgeries. The hyoid position
depends on the relative balance of muscle attachment from the base of the
cranium bilaterally and the region of the mandibular symphysis14
.
The mean differences in the hyoid bone positions of Class I group and
Class II Group following orthodontic treatment were shown in table 8 and table
11.
In our study, there was a significant change in the hyoid position in
relation to the point RGN (Retrognathion), Third cervical vertebra (C3) and
Sella point in both Class I and Class II groups. The hyoid bone was found to be
retracted postero inferiorly in Class I group. The amount of retraction was 1.04
mm and 1.30 mm in horizontal and vertical direction (Table 8). Findings of our

Discussion
62
study were coinciding with that of the study by Qingzhu Wang 70
. The inferior
movement of the hyoid bone seen in the present study was consistent with the
findings of other studies, showing that this movement is an adaptation
preventing an encroachment of the tongue into the pharyngeal airway 85
. Our
findings confirmed that the horizontal spaces around the tongue (TB-TPPW)
were decreased with the downward movement of the hyoid bone caused by the
retraction of incisors. But in class II group of our study the hyoid bone was
found to be shifted antero superiorly.
Comparison of the airway dimensions and hyoid positions of Class I and
Class II to the normoocclusion subjects reveals the following:
Pretreatment nasopharynx and velopharynx areas of class I and class II
subjects were wider than the normoocclusion subjects. But the hypopharynx
area was constricted in both Class I and Class II groups with highly significant
reduction in Class II groups which is attributable to the retrognathic mandible
and posteriorly positioned tongue. Vertical length of the airway was also
reduced in Class II group in comparison with that of Class I group and
normoocclusion group.
After treatment the overall pharyngeal space was significantly reduced
in Class I group, with only velopharynx and glossopharynx areas
approximating to the values of the normoocclusion group. Whereas in Class II
group, there was a significant widening of the velopharynx, glossopharynx and
hypopharynx areas attributable to the forward positioning of the mandible after

Discussion
63
the treatment which may be due to the orthodontic mechanotherapy to correct
class II condition which includes the use of inter arch elastics or protraction of
molars or fixed functional appliance during treatment. Whereas the
hypopharynx area was not widened to the normal levels.
At baseline the Hyoid bone was positioned antero superiorly in Class I
subjects and postero superiorly in class II subjects when compared to the
normoocclusion groups. After treatment the hyoid was retracted postero
inferiorly in Class I group attributable to the constriction in lower airway.
Whereas in class II group the hyoid bone was shifted anterosuperiorly after
treatment which can be attributed to the forward movement of mandible due to
the orthodontic mechanotherapy to correct class II condition which includes the
use of inter arch elastics or protraction of molars or fixed functional appliance
during treatment. The changes were statistically significant in both the
conditions with p values less than 0.05.
There was no statistically significant (p value > 0.05) sexual
dimorphism in the changes of pharyngeal airway dimensions and hyoid
positions of the study groups.

Summary and Conclusion
64
Summary and Conclusion
Pharyngeal airway dimension plays an important role in dentofacial
development. The malocclusion type and sagittal jaw relationship had been
proved to affect the pharyngeal airway dimensions in healthy subjects with
average growth pattern. This study had been undertaken to correlate subjects
with normal respiratory function with Class I and Class II malocclusions.
There was a significant difference in the changes in the airway dimensions
and hyoid bone position between Class I and Class II groups following
non-surgical orthodontic treatment.
Pretreatment nasopharynx, glossopharynx and velopharynx areas of Class I
and Class II malocclusion subjects were marginally wider than the
normoocclusion subjects. But the hypopharynx area was significantly
constricted in both Class I and Class II groups with highly significant
reduction (p value < 0.001) in Class II groups.
In Class I malocclusion group there was a significant decrease in overall
upper airway dimensions, with more reduction in glossopharynx and
hypopharynx areas following non-surgical orthodontic treatment with only
velopharynx and glossopharynx areas approximating to the values of the
normoocclusion group.
Unlike in Class I malocclusion group, Class II malocclusion group
revealed diverse changes in airway dimensions after orthodontic treatment.
Nasopharynx was constricted minimally and the glossopharynx and

Summary and Conclusion
65
hypopharynx areas were widened significantly. Whereas the hypopharynx
area was not widened to the level of normoocclusion group.
Pretreatment Hyoid bone position was antero superior in Class I subjects
and postero superior in Class II subjects when compared to the
normoocclusion groups. After treatment the hyoid was retracted postero
inferiorly in Class I group. Whereas in Class II group the hyoid bone was
shifted anterosuperiorly after treatment. Still the hyoid position was not
approximated to that of normoocclusion group.
There was no statistically significant (p value > 0.05) sexual dimorphism
in both pharyngeal airway dimensions and hyoid bone positions in all three
groups.
Future prospects:
Further studies may be aimed at long-term effects of nonsurgical
orthodontic treatment on pharyngeal airway and hyoid positions.
It was evident that non-surgical orthodontic therapy has an effect on
pharyngeal airway dimensions. Future studies may be carried out to
evaluate the changes in airway dimensions following surgical
orthodontic therapy.
Future studies may be done to evaluate the airway flow capacity in
different malocclusions using 3D imaging systems.

Bibliography
66
Bibliography
1. Alan A. Lowe, Takashi Ono, D Kathleen A. Ferguson, Eung-Kwon Pae, C. Frank
Ryan and John A. Fleetham- Cephalometric comparisons of craniofacial and upper
airway structure by skeletal subtype and gender in patients with obstructive sleep apnea -
Am J Orthod Dentofac Orthop 1996;110:653-64.
2. Allan G. Brodie - Consideration of musculature in diagnosis, treatment, and retention -
Presented at the forty-eighth Annual Meeting Of The American Association Of
Orthodontists, St. Louis, Mo., April 23. 1952
3. Anette M. C. Fransson, Åke Tegelberg, Bjo rn A. H. Svenson, Bertil Lennartsson,
and Go ran Isacsson, - Influence of mandibular protruding device on airway passages
and dentofacial characteristics in obstructive sleep apnea and snoring Am J Orthod
Dentofacial Orthop 2002;122:371-9
4. Antje Tallgren And Beni Solow - Long-Term Changes In Hyoid Bone Position And
Craniocervical Posture In Complete-Denture Wearers- Acta Odontol Scand
1984;42:257-267
5. Armando Gale, Pauli V.J.Kilpelainen, Maija T.Laine Alava - Hyoid Bone Position
After Surgical Mandibular Advancement - European Journal Of Orthodontics 23(2001)
695-701
6. Ashok Kumar Jena; Ritu Duggal - Hyoid Bone Position In Subjects With Different
Vertical Jaw Dysplasias - Angle Orthod. 2011;81:81–85, 183-214
7. Ashok Kumar Jenaa; Satinder Pal Singhb; Ashok Kumar Utrejac - Sagittal
mandibular development effects on the dimensions of the awake pharyngeal airway
passage - Angle Orthod. 2010;80:1061–1067.

Bibliography
67
8. Athanasios E. Athanasiou, , Nick Toutountzakis,, Dimitrios Mavreas, Martin
Ritzau, , and Ann Wenzel, - Alterations of hyoid bone position and pharyngeal depth
and their relationship after surgical correction of mandibular prognathism -Am J Orthod
Dentofac Orthop 1991 ;100:259-65.
9. Austin Phoenix; Manish Valiathan; Suchitra Nelson; Kingman P. Strohl; Mark
Hans - Changes In Hyoid Bone Position Following Rapid Maxillary Expansion In
Adolescents - Angle Orthod. 2011;81:632–638
10. Bibby. R. E. and C. B. Preston- The Hyoid Triangle - Volume 80, Number 1, Am J
Orthod July 1981
11. Bibby R. E. - The Hyoid Bone Position In Mouth Breathers And Tongue-Thrusters -
Am. J. Orthod., May 1984, Volume 85, Number 5
12. Boon H.Seto, Helen Gotsoloulos, Milton R.Sims, Peter A.Cistulli – maxillary
morphology in obstructive sleep apnoea syndrome - European Journal of orthodontics
23 (2001) 703-714
13. Cameron Aboudara, Ib Nielsen, John C. Huang, Koutaro Maki, Arthur J. Miller,
and David Hatcher - Comparison of airway space with conventional lateral headfilms
and 3-dimensional reconstruction from cone-beam computed Tomography - Am J
Orthod Dentofacial Orthop 2009;135:468-79
14. Carmine A.Durzo, Allan G.Brodie – Growth Behavior Of The Hyoid Bone – July
1962, Vol 32, No 3 Angle Orthodontist
15. Chang-Min Sheng; Li-Hsiang Lin; Yu Su; Hung-Huey Tsai - Developmental
Changes in Pharyngeal Airway Depth and Hyoid Bone Position from Childhood to
Young Adulthood - Angle Orthod. 2009;79:484–490.

Bibliography
68
16. Chester S. Handelman, George Osborne – Growth of the nasopharynx and adenoid
development from one to eighteen years – vol 46, No. 3, July 1976
17. Cleomar Donizeth Rodrigues, Márcia Maria Fonseca da Silveira, Orivaldo Tavano,
Ronaldo Henrique Shibuya, Giovanni Modesto, Carlos Estrela - Evaluation of
indirect methods of digitization of cephalometric radiographs in comparison with the
direct digital method Dental Press J Orthod 2010 July-Aug;15(4):124-32
18. Craig Fairburn.S , DMD, MD, Peter D. Waite, MPH, DDS, MD, George Vilos,
DDS, MS, Susan M. Harding, MD, Wanda Bernreuter, MD, Joel Cure, MD, and
Sai Cherala, MD - Three-Dimensional Changes in Upper Airways of Patients With
Obstructive Sleep Apnea Following Maxillomandibular Advancement - J Oral
Maxillofac Surg 65:6-12, 2007
19. Dan Grauer, Lucia S. H. Cevidanes, Martin A. Styner, James L. Ackerman, and
William R. Proffit - Pharyngeal airway volume and shape from cone-beam computed
tomography: Relationship to facial morphology - Am J Orthod Dentofacial Orthop
2009;136:805-14
20. Darrell C. Mergen, Richard M.Jacobs – the size of nasopharynx associated with
normal occlusion and class II malocclusion - Vol 40, No 4 oct 1970
21. David M. Gobeille, D.D.S., And Douglas C. Bowman, D.D.S. - Hyoid And Muscle
Changes Following Distal Repositioning Of The Tongue - Volume 70, Number 3 Am J
Orthod September 1976
22. Derya Germec-Cakan, Tulin Taner and Seden Akan - Uvulo-glossopharyngeal
dimensions in non-extraction, extraction with minimum anchorage, and extraction with
maximum anchorage - European Journal of Orthodontics 33 (2011) 515–520

Bibliography
69
23. Emine Kaygısız; Burcu Balos¸ Tuncer; Sema Yu¨ ksel; Cumhur Tuncer; Cem
Yıldız - Effects of Maxillary Protraction and Fixed Appliance Therapy on the
Pharyngeal Airway Angle Orthod. 2009; 79:660–667.)
24. Faruk Izzet Ucar ; Tancan Uysal - Orofacial airway dimensions in subjects with Class
I malocclusion and different growth patterns - Angle Orthod. 2011;81:460–468
25. Fitin Aloufi, Charles B. Preston, and Khalid H. Zawawi - Changes in the Upper and
Lower Pharyngeal Airway Spaces Associated with RapidMaxillary Expansion
International Scholarly Research Network,ISRN Dentistry Volume 2012, Article ID
290964 ;10.5402/2012/290964
26. Garland Hershey .H , Bruce stewart Donald warren – Changes in nasal airway
resistance associated with rapid maxillary expansion- Am J Orthod. 1976
Mar;69(3):274-84.
27. Gary Cuozzo and Douglas C. Bowman - Hyoid Positioning During Deglutition
Following Forced Positioning Of The Tongue - Volume 68, Number 5, Am. J. Orthod.,
November 1975.
28. Graber TM, Neumann B. Removable orthodontic appliances. Philadelphia: WB
Saunders, 1984: 357-375
29. Gray’s anatomy ; the anatomical basis of clinical practice.40th
edition by Susan
Standring 2008
30. Gundega Jakobsone, Arild Stenvik, and Lisen Espeland - The effect of maxillary
advancement and impaction on the upper airway after bimaxillary surgery to correct
Class III malocclusion Am J Orthod Dentofacial Orthop 2011;139:e369-e376

Bibliography
70
31. Gunduz Arslan, J Devecioglu Kama, T Ozer and IYavuz - Craniofacial and upper
airway cephalometrics in hypohidrotic ectodermal dysplasia Dentomaxillofacial
Radiology (2007) 36, 478–483
32. Hakan El and Juan Martin Palomo - Airway volume for different dentofacial skeletal
patterns - Am J Orthod Dentofacial Orthop 2011;139:e511-e521
33. Halise Aydemir; Ufuk Memikog˘ lub; Hakan Karasuc - Pharyngeal airway space,
hyoid bone position and head posture after orthognathic surgery in Class III patients
Angle Orthod. 2012;82:993–1000
34. Hans Holmberg and Sten Linder-Aronson - Cephalometric radiographs as a means of
evaluating the capacity of the nasal and nasopharyngeal airway- American Journal of
orthodontics Volume 76, Number 5 November, 1979
35. Hiroyuki Ishikawa, Shinji Nakamura, Hiroshi Iwasaki and Shinichi Kitazawa -
Seven parameters describing anteroposterior jaw relationships Postpubertal prediction
accuracy and interchangeability- Am J Orthod and Dentofacial Orthop 2000;117:714-20
36. Hosamettin Oktay - A comparison of ANB, WITS, AF-BF, and APDI measurements -
Volume 99 Number 2 - Am. J. Orthod. Dentofac. Orthop. February 1991
37. Ian milne , Jhon cleal – Cinefluorographic study of functional adaptation of the
oropharyngeal structures -Angle Orthod. 1970 Oct;40(4):267-83.
38. Ioannis.P.Adamidis and Meropi n. Spyropoulos – The effects of lymphadenoid
hypertrophy on the position of the tongue, the mandible and the hyoid bone. Eur J
Orthod. 1983 Nov;5(4):287-94.

Bibliography
71
39. Ioannis Kollias, Olaf Krogstad - Adult Craniocervical And Pharyngeal Changes –
A Longitudinal Cephalometric Study Between 22 And 42 Years Of Age. Part II :
Morphological Uvulo-Glossopharyngeal Changes - Eur J Orthod 21 (1999) 345-355
40. James A.McNamara Jr. Influence of respiratory pattern on craniofacial growth. Angle
Orthod, 1981; 51: 269-300.
41. James A. McNamara, Jr., - A method of cephalometric evaluation -American Journal
of orthodontics - Volume 86, Number 6 December, 1984
42. Jeans .W. D, J. Fernando, A. R. Maw and B. C. Leighton - A longitudinal study of
the growth of the nasopharynx and its contents in normal children - British Journal of
Radiology, 54,117-121, 1981
43. Joanna M.Battagel, Amandeep Johal, Bhik Kotecha – A cephalometric comparison
of subkects with snoring and obstructive sleep apnoea - European journal of
orthodontics 22 (2000) 353-365
44. Katherine W. L. Vig - Nasal obstruction and facial growth: The strength of evidence
for clinical assumptions - Am J Orthod Dentofacial Orthop 1998;113:603-11
45. Kenneth P. Moses, Pedro B. Nava, John C. Banks - Atlas of Clinical Gross Anatomy:
second edition Philadelphia 2012
46. Korkmaz Sayinsu , Fulya Isik , Göksu Trakyali and Tülin Arun - An evaluation of
the errors in cephalometric measurements on scanned cephalometric images and
conventional tracings European Journal of Orthodontics 29 (2007) 105–108
47. Kyung-Min Oh; Ji-Suk Hong; Yoon-Ji Kim; Lucia S.H. Cevidanes; Yang-Ho Park
- Three-dimensional analysis of pharyngeal airway form in children with anteroposterior
facial patterns - Angle Orthod. 2011;81:1075–1082.

Bibliography
72
48. Lee W.Graber - Hyoid Changes Following Orthopedic Treatment Of Mandibular
Prognathism - January 1978, Vol 48, No 1
49. Lee W. Graber, Robert L. Vanarsdall Jr., Katherine W. L. Vig orthodontics current
priciples and techniques – fifth edition Philadelphia mosby – 2012
50. Lena Zettergren-Wijk, Sten Linder-Aronson,Britt Nordlander, ,Karin Ågren,Eva
Svanborg, - Longitudinal Effect on Facial Growth After Tonsillectomy in Children with
Obstructive Sleep Apnea - World J Orthod 2002;3:67–72.
51. Luc P. M. Tourne - Growth of the pharynx and its physiologic implications - Am. J.
Orthod. Dentofac. Orthop. - Volume 99 Number 2 February 1991
52. Manish Valiathan; Hakan El; Mark G. Hans; Martin J. Palomo - Effects of
extraction versus non-extraction treatment on oropharyngeal airway volume - Angle
Orthod. 2010;80:1068–1074
53. Marcos Roberto de Freitas, Nadyr Maria Penteado Virmond Alcazar, Guilherme
Janson, Karina Maria Salvatore de Freitas, and José Fernando Castanha
Henriques - Upper and lower pharyngeal airways in subjects with Class I and Class II
malocclusions and different growth patterns - Am J Orthod Dentofacial Orthop
2006;130:742-5
54. Maria Julia Pereira Coelho Ferraz1, Darcy Flávio - Cephalometric Assessment Of
The Hyoid Bone Position In Oral Breathing Children - Rev Bras Otorrinolaringol
2007;73(1):47-52.
55. Masayoshi KAWAKAMI_, Kazuhiko YAMAMOTO, Masaki FUJIMOTO,
Kazuhiko OHGI, Masahide INOUE, Tadaaki KIRITA - Changes in tongue and

Bibliography
73
hyoid positions, and posterior airway space following mandibular setback surgery
Journal of Cranio-Maxillofacial Surgery (2005) 33, 107–110
56. Melvin Moss, D.D.S., Ph.D., and Letty Salentijn, D.D.S. - The primary role of
functional matrices in facial growth - Am. J. Orthodontics - June 1969 Volume 55
Number 6
57. Michael Major. P, Carlos Flores-Mir,b and Paul W. Majorc - Assessment of lateral
cephalometric diagnosis of adenoid hypertrophy and posterior upper airway obstruction:
A systematic review - Am J Orthod Dentofacial Orthop 2006;130:700-8
58. Michael Stepovich .L, - A Cephalometric Positional Study Of The Hyoid Bone -
Volume 51, Number 12 Am J Orthod December 1965
59. Michael Taylor, Kingman P.Strohl, B.Holly Broadbent - Soft tissue growth of the
oropharynx - Angle Orthod 1996; 66(5) : 393-400
60. Miles P.G, O'Reilly M, Close J. -
The reliability of upper airway landmark identification-Aus Orthod J.1995Oct;14(1):3-6.
61. Mirja Kirjavainen; Turkka Kirjavainen - Upper Airway Dimensions in Class II
Malocclusion Effects of Headgear Treatment - Angle Orthodontist, Vol 77, No 6, 2007
62. Nancy Ung, Jane Koenig, Peter A. Shapiro, Gail Shapiro, Georgina Trask - A
Quantitative Assessment Of Respiratory Patterns And Their Effects On Dentofacial
Development – American J of Orthod and Dentofac Orthop - 1990;98:523-32.
63. Nanda Kishore Sahoo , Balakrishnan Jayan, Sukbir Singh Chopra, - Evaluation of
Upper Airway Dimensional Changes and Hyoid Position Following Mandibular
Advancement in Patients With Skeletal Class II Malocclusion The Journal of
Craniofacial Surgery & Volume 23, Number 6, November 2012 e623-7

Bibliography
74
64. Nonglak Pracharktam, Suchitra Nelson, Mark G. Hans, B. Holly Broadbent, Susan
Redline, Carl Rosenberg and Kingman P. Strohl - Cephalometric assessment in
obstructive sleep apnea - Am J Orthod Dentofac Orthop 1996;109:410-9.
65. Oscar Martin, Leonor Muelas, and M. José Viñasa - Nasopharyngeal cephalometric
study of ideal occlusions - Am J Orthod Dentofacial Orthop 2006;130:436.e1-436.e9
66. Pirilä-Parkkinen .K, Heikki Löppönen, Peter Nieminen Uolevi Tolonen and Pertti
Pirttiniemi - cephalometric evaluation of children with nocturnal sleep-
disordered breathing. Eur J Orthod. 2010 Dec;32(6):662-71
67. Pirila-Parkkinen .K; Heikki Lo¨ppo¨nen; Peter Nieminen; Uolevi Tolonen; Eija
Pa¨a¨kko¨; Pertti Pirttiniemi - Validity of upper airway assessment in children - A
clinical, cephalometric, and MRI study - Angle Orthod. 2011;81:433–439.
68. Proffit W.R- Equilibrium theory revisited : factors influencing position of the teeth -
Angle Orthodontist, Vol 48, no 3 july 1978
69. Profit W.R contemporary orthodontics 4th
edition St.Louis, Mosby 2007.
70. Qingzhu Wang; Peizeng Jia; Nina K. Anderson; Lin Wang; Jiuxiang Lin - Changes
of pharyngeal airway size and hyoid bone position following orthodontic treatment of
Class I bimaxillary protrusion Angle Orthod. 2012;82:115–121
71. Robert F. Sloan, Ruel W.Bench, James F. Mulick – The Application Of
Cephalometrics To Cineflurography : Comparative Analysis Of Hyoid Movement
Patterns During Deglutition In Class I And Class II Orthodontic Patients – Vol 37, No 1
January 1967
72. Robert M Ricketts - Respiratory obstruction syndrome - American journal of
orthodontics July 1968 volume 54, no 7

Bibliography
75
73. Ronan O'Rahilly, Fabiola Müller,Stanley Carpenter, Rand Swenson - Basic Human
Anatomy – A Regional Study Of Human Structure - 2008
74. Ruel Bench - Growth Of The Cervical Vertebrae As Related To Tongue, Face And
Denture Behavior - Am. J. Orthodontics, March 1963
75. Sarwat Memon, Mubassar Fida and Attiya Shaikh - Comparison of Different
Craniofacial Patterns with Pharyngeal Widths - Journal of the College of Physicians and
Surgeons Pakistan 2012, Vol. 22 (5): 302-306
76. Siddik Malkoc, Serdar Usumez,Metin Nur, and Claire E. Donaghy - Reproducibility
of airway dimensions and tongue and hyoid positions on lateral cephalograms Am J
Orthod Dentofacial Orthop 2005;128:513-6
77. Sila Mermut Gokce, Hasan Suat Gokce, Serkan Gorgulu, Seniz Karacay, Eralp
Akca, Huseyin Olmez - Relationship Between Class III Malocclusion And Hyoid Bone
Displacement During Swallowing: A Cine-Magnetic Resonance Imaging Study - Korean
J Orthod 2012;42(4):190-200
78. Soonshin Hwang; Chooryung Judi Chung; Yoon-Jeong Choi; Jong-Ki Huh;
Kyung-Ho Kim - Changes of Hyoid, Tongue and Pharyngeal Airway after Mandibular
Setback Surgery by Intraoral Vertical Ramus Osteotomy – Angle Orthod. 2010;80:302–
308.
79. Takahashi.S , Ono.T , Y. Ishiwata and T. Kuroda - Breathing modes, body positions,
and suprahyoid muscle activity J Orthod. 2002 Dec;29(4):307-13;
80. Tomonori Iwasaki, Haruaki Hayasaki, Yoshihiko Takemoto, Ryuzo Kanomi, and
Youichi Yamasaki - Oropharyngeal airway in children with Class III malocclusion

Bibliography
76
evaluated by cone-beam computed tomography - Am J Orthod Dentofacial Orthop
2009;136:318.e1-318.e9
81. Tomonori Iwasaki, Issei Saitoh, Yoshihiko Takemoto, Emi Inada, Ryuzo Kanomi,
Haruaki Hayasaki,and Youichi Yamasaki - Evaluation of upper airway obstruction in
Class II children with fluid-mechanical simulation Am J Orthod Dentofacial Orthop
2011;139:e135-e145
82. Verin . E., Tardif C., X. Buffet , J.P. Marie , Y. Lacoume , J. Andrieu-
Guitrancourt , P. Pasquis - Comparison between anatomy and resistance of upper
airway in normal subjects, snorers and OSAS patients - Respiration Physiology 129
(2002) 335–343
83. Yoon-Ji Kim, Ji-Suk Hong, Yong-In Hwang, and Yang-Ho Park - Three-
dimensional analysis of pharyngeal airway in preadolescent children with different
anteroposterior skeletal patterns - Am J Orthod Dentofacial Orthop 2010;137:306.e1-
306.e11
84. Yoshihiko Takemotoa; Issei Saitohb; Tomonori Iwasakic; Emi Inadac; Chiaki
Yamadaa; Yoko Iwased;Miyuki Shinkaia; Ryuzo Kanomie; Haruaki Hayasakif;
Youichi Yamasakig - Pharyngeal airway in children with prognathism and normal
occlusion - Angle Orthod. 2011;81:75–80
85. Yu Chen; Liu Hong; Chun-ling Wang; Shi-jie Zhang; Cong Cao; Fulan Wei; Tao
Lv; Fan Zhang; Dong-xu Liu - Effect of large incisor retraction on upper airway
morphology in adult bimaxillary protrusion patients - Three-dimensional multislice
computed tomography registration evaluation - Angle Orthod. 2012;82:964–970

Bibliography
77
86. Yuko Shigeta, DDS, PhD, Takumi Ogawa, DDS, PhD, Jaqueline Venturin, DDS,
Manuel Nguyen,DDS, Glenn T Clark, DDS, MS, and Reyes Enciso, PhD - Gender-
and age-based differences in computerized tomographic measurements of the
oropharynx - Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2008;106:563-70
87. Zhe Zhong; Zhihui Tang; Xuemei Gao; Xiang-Long Zeng - A Comparison Study of
Upper Airway among Different Skeletal Craniofacial Patterns in Nonsnoring Chinese
Children - Angle Orthod. 2010;80:267– 274.