
Comparative analyses of Drug- Adverse Event Associations ... · Adverse Event Associations in...
35
Comparative analyses of Drug- Adverse Event Associations in Various European Databases Raymond G. Schlienger, PhD, MPH. Global Clinical Epidemiology, Novartis Pharma AG, Basel, Switzerland Mark de Groot, PhD. Division of Pharmacoepidemiology & Clinical Pharmacology, Utrecht Institute for Pharmaceutical Sciences, Utrecht University, The Netherlands First results from PROTECT WP2-WG1 ISPE Mid-Year Meeting, Munich, 12-Apr-2013
Transcript of Comparative analyses of Drug- Adverse Event Associations ... · Adverse Event Associations in...

Comparative analyses of Drug-
Adverse Event Associations
in Various European Databases
Raymond G. Schlienger, PhD, MPH. Global Clinical Epidemiology, Novartis Pharma AG, Basel, Switzerland
Mark de Groot, PhD. Division of Pharmacoepidemiology & Clinical
Pharmacology, Utrecht Institute for Pharmaceutical Sciences, Utrecht University, The Netherlands
First results from PROTECT WP2-WG1
ISPE Mid-Year Meeting, Munich, 12-Apr-2013

Disclosures
• RGS: full-time employee of Novartis Pharma AG,
Basel Switzerland. The views expressed in this
presentation are those of the author in his role of
industry co-lead for IMI Protect WP2/WG1
• MdG: employee of Utrecht University, The
Netherlands, and partly funded by TI Pharma
Mondriaan grant T6.101
2

Acknowledgements
• The research leading to these results was conducted as part
of the PROTECT consortium (Pharmacoepidemiological
Research on Outcomes of Therapeutics by a European
ConsorTium, www.imi-protect.eu) which is a public-private
partnership coordinated by the European Medicines Agency
• PROTECT work in this presentation is work by WP2/WG1
colleagues
• The views expressed are those of the authors only

Contents
• Background Working Group 1 (WP2/WG1)
– Framework of WP2/WG1 within Protect
• Objectives of WP2/WG1
• Methods
• Results
– Descriptive studies
• Current status and next steps
• Conclusions
4

5
WG1 Databases
WG2 Confounding
WG3 Drug utilization
Number of participants
n=46 33 public, 13 private
n=14 10 public, 4 private
n=9 5 public, 4 private
Public partners EMA, LMU-München, Witten
University4, AEMPS, CEIFE, CPRD, DKMA and UU
UU FIFC, LMU and Witten
University4
Private partners
Amgen, AstraZeneca, Genzyme, GlaxoSmithKline, La-Ser, Merck,
Novartis, Roche and Pfizer
Amgen, Novartis, Roche and Pfizer
Amgen, Novartis and Roche
WG Coordinators
Raymond Schlienger1 (Novartis) Mark de Groot2 (UU)
Nicolle Gatto (Pfizer) Rolf Groenwold (UU)
Joan Fortuny3 (Novartis)
Luisa Ibanez (FIFC)
WP2 coleaders Olaf Klungel (UU) - Robert Reynolds (Pfizer)
WP2 coleaders alternates
Tjeerd van Staa (CPRD) - Jamie Robinson (Roche)
WP2 Project Manager
Ines Teixidor (UU)
1 from October 2010 replacing John Weil (GSK), 2 from 1 February 2011 replacing Frank de Vries (UU), 3 from 15 March 2012 replacing Hans Petri (Roche), 4 New partner, accession approved by SC in January 2013
WP2: Participants and their roles
WP2: Framework for pharmacoepidemiological studies
6
To:
• develop
• test
• disseminate
of pharmacoepidemiological studies applicable to:
• different safety issues
• using different data sources
methodological standards for the:
• design
• conduct
• analysis
Objectives:

Objective WP2 – WG1
• Explain differences in drug-adverse event (AE)
associations due to choices in methodology and
databases
– Reduce variation due to methodological choice of individual
researchers
– Explain variation due to characteristics of country/database
– More consistency in drug-AE studies to improve B/R assessment of
medicines
7

Methods
• Conduct of drug-AE studies in different EU
healthcare databases, using different study designs
– Selection of 6 key drug-AE pairs
AEs that caused regulatory decisions
Public health impact (seriousness of the event, prevalence
of drug exposure, etiologic fraction)
Feasibility
Range of relevant methodological issues
– Development of study protocols for all drug-AE pairs
– Compare results of studies
– Identify sources of discrepancies
8

Methods: Drug - AE pair selection
• Selection of 6 key AEs and drug classes
– Initial list of 55 AEs and >55 drugs
– Finalisation based on literature review and consensus
meeting
9
Drug – AE pair
Antidepressants - Hip fracture
Benzodiazepines - Hip fracture
Antibiotics - Acute liver injury
Beta2 Agonists - Myocardial infarction
Antiepileptics - Suicide
Calcium Channel Blockers - Cancer

Methods: Characteristics of individual
databases
10
Dat
abas
e
Co
un
try
Cu
mu
lati
ve
po
pu
lati
on
(200
8)
Act
ive
po
pu
lati
on
(200
8)
Dat
a
sou
rce
Co
din
g
dia
gn
ose
s
Co
din
g
dru
gs
Rec
ord
ing
of
dru
g u
se
BIFAP ES 3.2 Mio 1.6 Mio GP ICPC ATC Prescribing
CPRD UK 11.0 Mio 3.6 Mio GP READ BNF Prescribing
THIN UK 7.8 Mio 3.1 Mio GP READ BNF Prescribing
Mondriaan NPCRD AHC
NL 0.7 Mio
0.26 Mio
0.34 Mio 0.17 Mio
GP
GP/Pharmacy
ICPC ICPC
ATC ATC
Prescribing
Prescribing + dispensing
The Danish national registries
DK 5.2 Mio 5.2 Mio GP + specialist doctors
ICD-9 ATC Prescribing + dispensing
Bavarian Claims Database
DE 10.5 Mio 9.5 Mio Claims health insurance
ICD-10 ATC Claims
Methods: Designs
• Descriptive studies for drug-AE pairs in all DBs
– Prevalence of exposure of interest
– Prevalence/incidence of outcome of interest
• Association studies: Different study designs in selected
DBs
– Cohort studies
– Nested case-control studies
– Case crossover studies
– Self-controlled case series
11

Methods: Overview of planned studies
Drug - AE pair
Descriptive Cohort Nested case control
Case crossover
Self-Controlled case series
AB - ALI All Databases
CPRD BIFAP
CPRD BIFAP
CPRD BIFAP
CPRD BIFAP
AED - Suicide All Databases
CPRD DKMA
n/a n/a n/a
AD - Hip All Databases
THIN Mondriaan BIFAP
THIN Mondriaan BIFAP
THIN Mondriaan
THIN Mondriaan
BZD - Hip All Databases
CPRD BIFAP Mondriaan
CPRD BIFAP Mondriaan
CPRD BIFAP
CPRD BIFAP
B2A - AMI All Databases
CPRD Mondriaan
n/a n/a n/a
CCB - Cancer All Databases
CPRD DKMA
n/a n/a n/a
12
Methods: Standardization of methods
• Common protocol for each drug-AE pair
• Common standards, templates, procedures
– Detailed data specifications (statistical analysis plan)
including definitions, codes for diseases, drugs etc.
– Age-/sex-standardization to European reference
population
• Blinding of results of individual DB analyses
• Submission of protocols to ENCePP study registry
13

Methods: Standardisation to European
reference population
• age stratification
14
Europe
0-9
10-19
20-29
30-39
40-49
50-59
60-69
70-79
80+
Mondriaan-AHC
0-9
10-19
20-29
30-39
40-49
50-59
60-69
70-79
80-89
90+
BIFAP
0-9
10-19
20-29
30-39
40-49
50-59
60-69
70-79
80-89
90+
THIN
0-9
10-19
20-29
30-39
40-49
50-59
60-69
70-79
80-89
90+
Danish Registries
0-9
10-19
20-29
30-39
40-49
50-59
60-69
70-79
80-89
90+
CPRD
0-9
10-19
20-29
30-39
40-49
50-59
60-69
70-79
80-89
90+
Mondriaan-NPCRD
0-9
10-19
20-29
30-39
40-49
50-59
60-69
70-79
80-89
90+
KVB
0-19
20-29
30-39
40-49
50-59
60-69
70-79
80-89
90+

Results: Benzodiazepine exposure
prevalence 2001-2009
15
Crude Standardised

Results: Benzodiazepine exposure
prevalence by age & sex (2008)
16
Females Males

Results: Benzodiazepine exposure
prevalence – methodological issues
• Marked differences of BZD exposure prevalence
across countries/DBs
– Unlikely to be primarily explained by DB characteristics
(e.g. different drug coding systems)
Prescribing vs dispensing information
– Rather explained by different prescribing habits, e.g.
driven by country guidelines/policies, marketing,
reimbursement, ...
• Age-/sex-standardization had relevant impact
specifically on Mondriaan data
17

Results: Hip fracture incidence by sex
18
Adjusted Incidence of Hip Fractures in Males over 50 years old
0
5
10
15
20
25
30
35
40
2003 2004 2005 2006 2007 2008 2009
Years
Incid
*10,0
00p
y
DKMA
BAVARIAN
AHC
BIFAP
CPRD
THIN
NPCRD
Adjusted Incidence of Hip Fractures in Females over 50 years old
0
10
20
30
40
50
60
70
80
2003 2004 2005 2006 2007 2008 2009
YearsIn
cid
*10,0
00p
y
DKMA
BAVARIAN
AHC
BIFAP
CPRD
THIN
NPCRD

Results: Hip fracture incidence -
methodological issues
• Hip fracture: defined as a fracture of the proximal
femur in the cervix or in the trochanteric region
• Operational definition for this study: “any femur
fracture”
– Some coding systems (International Classification of
Primary Care ([ICPC-2]) don’t have a specific code for
hip fracture, but only a broader code for “femur”
fracture
19
Results: Hip fracture incidence -
methodological issues (2)
• Definition and coding of hip fracture/femur fracture
– ICPC-2: BIFAP and Mondriaan - 1 code
– ICD-10: Danish Registries and Bavarian Claims DB - 9
codes
– READ: THIN and CPRD - 64 codes
20
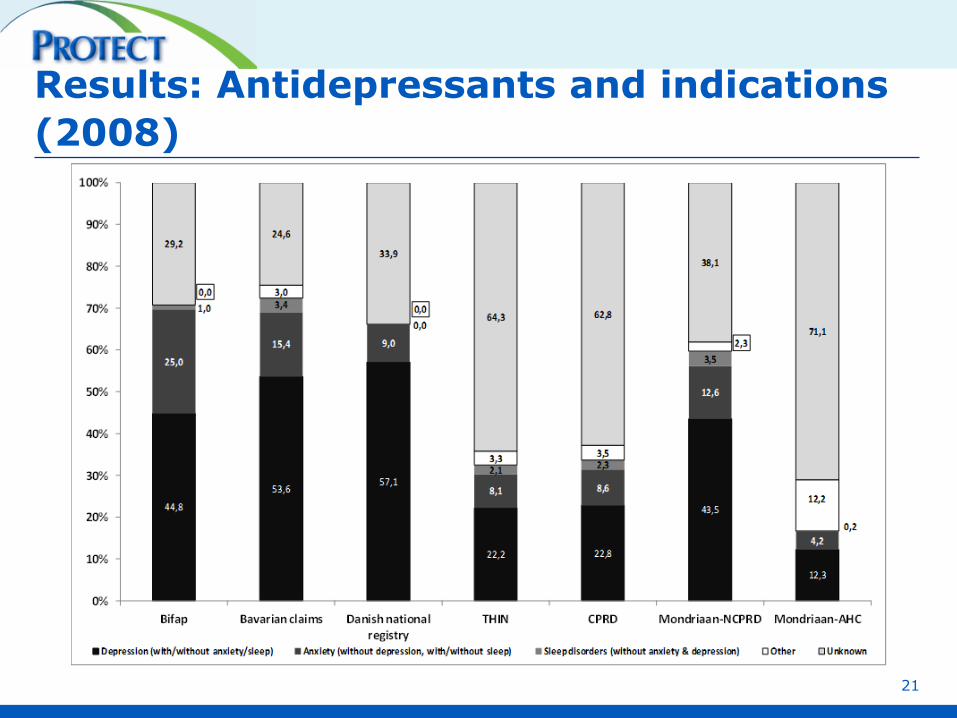
Results: Antidepressants and indications
(2008)
21

Results: Antidepressants and indications -
methodological issues
• Major differences across DBs regarding underlying
‘indications’ for ADs
• Most DBs do not capture specific information on
indication
• Time window defined ± 90 days around AD
prescribing date to identify disorder which may
correlate to AD prescribing
22
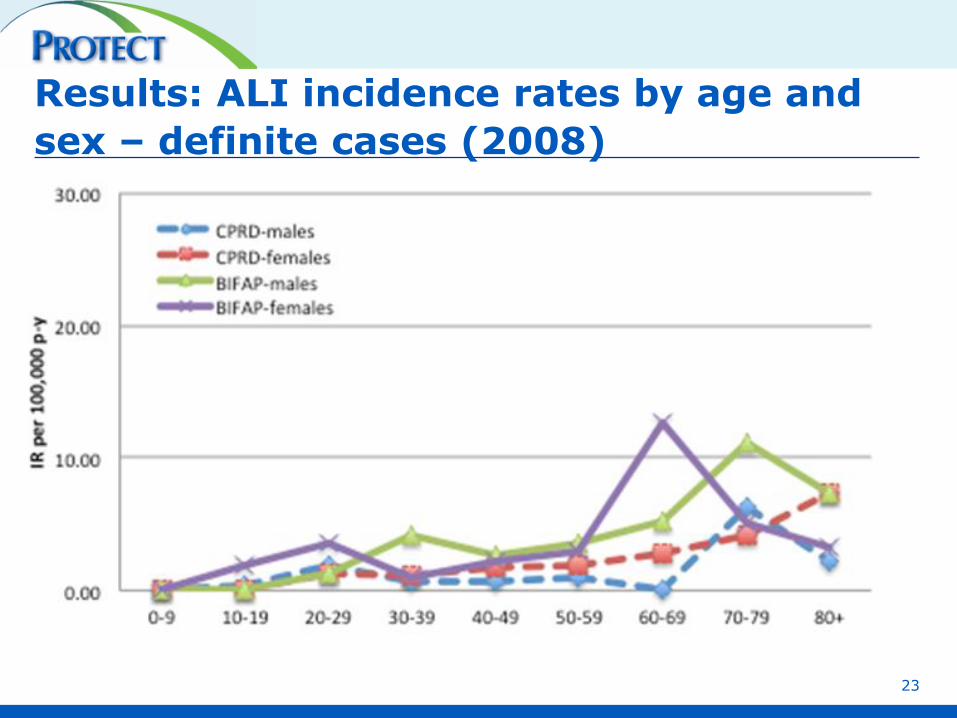
Results: ALI incidence rates by age and
sex – definite cases (2008)
23

Results: Standardised ALI incidence rates
– definite cases (2008)
24

Results: Incidence of acute liver injury -
methodological issues
• Major challenge to define idiopathic ALI in DB which
use different coding systems
– Codes specific of liver disease or symptoms (e.g.
hepatitis , acute hepatic failure, icterus, ...)
– Non-specific codes (e.g. liver function tests abnormal,
increased transaminases)
• Manual review of ‘free-text’ (in BIFAP and CPRD)
• Classification in ‘definite’, ‘probable’, ‘non-cases’
based on available DB information
25

Results: Incidence of acute liver injury -
methodological issues (2)
26

Results: Incidence of acute liver injury -
methodological issues (3)
27

Results: Antiepileptic drug prevalence
28
Period Prevalence (standardised)
2001
2002
2003
2004
2005
2006
2007
2008
2009
0
100
200
300
400
per 1
0,0
00
KVB
CPRD
THIN
Mondriaan - AHC
Mondriaan - NPCRD
Danish registries
BIFAP

Results: AED exposure prevalence -
methodological issues
• Definition of AED - literature provides different
definitions of drugs belonging to that drug class
• Broad range of neurological and psychiatric
indications for AEDs in addition to epilepsy
29

Results - Cohort studies
• Due to blinding of results policy we cannot show any
results at this point
30

WG1: Progress of studies
31
Drug - AE pair
Descriptive Cohort Nested case control
Case crossover
Self-controlled case series
AB - ALI Completed Completed March 2013 May 2013 March 2013
AED - Suicide Completed March 2013 n/a n/a
n/a
AD - Hip Completed Completed Aug 2013
Dec 2013 n/a
BZD - Hip Completed Completed Sept 2013
Sept 2013 Sept 2013
B2A - AMI Completed March 2013 n/a
n/a
n/a
CCB - Cancer Completed April 2013 n/a
n/a
n/a
Conclusions
• WP2/WG1 provides unique framework for studying and
explaining potential differences in drug-AE
associations due to choices in methodology and DBs
• Descriptive studies on exposure and outcomes to
better characterize the individual DBs have been
finalized
• Association studies:
– Cohort studies on all outcomes across all DBs being
finalized
– Other designs within same DB ongoing or starting soon
32

Conclusions (2)
• Challenge to dissect identified differences (both of
exposure and outcome data)
– Due to different prescribing habits
– Due to true underlying differences in individual
populations
Life-style factors, genetics
Different co-morbidities, risk factor distribution
Latitude
Other
33

Conclusions (3)
– Due to differences in DB characteristics/structure
Information on certain life-style factors (alcohol, smoking),
BMI
Prescribing vs dispensing
Primary care EMR db vs health claims DB vs population
registries
Underlying coding systems
Other
– Due to different interpretation of protocol/data
specifications
– Differences because of different statistical software
– Impact of different study designs
34

Questions
35
















![Intravenous fluid resuscitation is associated with septic ... · identified associations between fluid administration [6, 7], fluid balance [8–12], and adverse outcomes. The mechanisms](https://static.fdocuments.us/doc/165x107/5ed551d812a6d6201a657f53/intravenous-fluid-resuscitation-is-associated-with-septic-identified-associations.jpg)
