Community Based Approaches: A review of intervention models and evidence of their effectiveness for...
13
Community Based Approaches: A review of intervention models and evidence of their effectiveness for preventing maternal-to-child transmission of HIV Joanna Busza 17 July 2011
-
Upload
arlene-banks -
Category
Documents
-
view
215 -
download
1
Transcript of Community Based Approaches: A review of intervention models and evidence of their effectiveness for...

Community Based Approaches:
A review of intervention models and evidence of their
effectiveness for preventing maternal-to-child transmission
of HIV
Joanna Busza17 July 2011

Thematic Synthesis of the Evidence on:
Increased uptake of HIV care and treatment services among pregnant women and vertically-infected children;
Improved retention of individuals in prevention for vertical transmission, care and treatment programs;
Enhanced adherence of pregnant and lactating women, their partners and children to ARV prophylaxis and/or ART and/or other care regimens;
Strengthened psychosocial well being of pregnant and lactating women and children enrolled in care and treatment programs

Methods Identification of existing systematic
reviews
Review of data on barriers to PMTCT
Development of conceptual framework
Literature Searches
Assessment of research quality based on study designs
Analysis of available data on community based intervention approaches

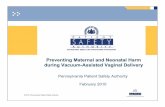
HIV Treatment Cascade
Awareness Testing Diagnosis Treatment initiation
Adherence & Follow-
Up
Clinical & Psychosoci
al outcomes
Perceived or experienced stigma
Perception of Risk
Accurate local
understanding
Opportunities to test
Partner communicati
on & approval
Transport, time & costs
Motivation vs. fear of results
Family support & Disclosure
Male involvement
Delivery in a clinic
Decision making power
Fear of abandonment &
violence
Self-efficacy
Perception of service
qualityDepression
Social capital and networks
Ill health

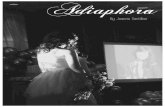
Socio-cultural Environment
Community Context
Peer & Family Influences
Individual
Legal and Policy
Structures
Self efficacy Motivation
Decision makingRisk Perception
DepressionDisease progression
Health Beliefs
GenderNorms
Religion
Social Welfare &Safety Nets
ARV Supply
Distance to Services
StigmaQuality of
Care
PartnerInvolvement
Communication& Disclosure
Support
SocialNetworks
Access to Resources
HealthPractices
Health Systems& Infrastructure
SOCIAL ECOLOGICAL FRAMEWORK

Partners, Peers & Family: Community based & home testing
• Increases opportunity• Introduces perception of risk• Engages family as a unit
Increasing male involvement• Targets communication, disclosure & decision-
making• Introduces perception of risk• Couple counselling, ANC participation and
breastfeeding advice Evidence strongly supports community testing,
although implications less clear for identifying pregnant women
“Male involvement” increases PMTCT retention but poorly defined and not always seen as positive by women

Community Context (1): Formalised Links
• Improves facility “friendliness” and support• Relies on peer volunteers or hired liaison staff• SMS message reminders
Home Based Care• Targets access to resources and food
insecurity• Logistical & adherence support• Efforts to challenge stigma and reduce
isolation Links improve relations, but no evidence that they
address wide range of barriers faced Rigorous research demonstrates that HBC improves
adherence & follow-up, although sustainability an issue

Community Context (2): Community Health Workers
• Work to change health beliefs and practices• Many different models have been evaluated• Applied to a wide range of health outcomes
Traditional Birth Attendants• Birth planning, attendance & referral• Nevirapine provision• No outcome evaluations for PMTCT
Long legacy of success with CHW but process factors important given heterogeneity of implementation
Feasibility studies & process evaluations suggest TBA could be useful in settings with low facility deliveries

Socio-cultural environment (1): Community Mobilisation
• Complex interventions – multiple components• Engage traditional leaders• Participatory, based on theories of
empowerment and social action• Drama events, outreach, peer approaches,
media Support Groups
• HIV+ support – target psychosocial outcomes• Evidence drawn from maternal & neonatal
health• Influence norms, supportive environment &
behaviour Cash Transfers
• Incentive for behaviour change• Provide a basic social safety net; address
inequity

Socio-cultural environment (2):
Very difficult to evaluate community mobilisation, especially to differentiate relative effectiveness of components
Support groups have been rigorously evaluated and show promise for PMTCT given similar determinants of health-seeking and programme retention
Cash transfers successful in Latin America in increasing service use; transfer to poorer settings with weaker health systems unclear

Remaining Gaps: Greater emphasis on process evaluation to
identify how activities lead to intended outcomes
Ways to create demand for services Understanding complementary and
reinforcing relationships between intervention activities to create optimal “package” for a given context
Adapting strategies from Asia and Latin America for African settings
Measuring psychosocial outcomes through standardised and comparable measures

Ways Forward: Moving beyond research on “proof of
concept” for community based approaches to learning from practice
Contextualisation – applying the social ecological framework to identify barriers and design activities for each programme settings
New approaches to scaling up and replication – transfer of process instead of content
Long term commitment – resources and efforts need to sustain community motivation; interim measures will change faster than outcomes

Thank you!
Questions and comments?