Communication for the New Graduate Registered Nurse
38
State of Nebraska Transition Grant Copyright 2011 Communication for the New Graduate Registered Nurse Education Module
Transcript of Communication for the New Graduate Registered Nurse

State of Nebraska Transition Grant
Copyright 2011
Communication for the
New Graduate Registered
Nurse
Education Module

2
Title: Communication
Introduction:
Purposeful communication between healthcare team members is an integral part of your
personal and professional world as a nurse. You have learned in school about nurse-patient
therapeutic communication and how effective communication can bring about positive health
outcomes and improved quality of care for the patient. The communication between the nurse
and fellow members of the healthcare team can affect your stress level, your attitude about your
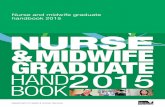
work and how you will become socialized to your new work environment. Notice from the
figure below that total communication is not only verbal but includes also nonverbal and most
important how you decide to affectively interact with the healthcare team where you work. As a
new nurse you will find that communication is the basis for everything you do from interacting
with your patient, to talking to the physician, dietician, physical therapist, etc. Communication
also involved how you report to other healthcare team members, how you chart so that the next
nurse knows what is going on with the patient, how you fill out forms and how you tactfully ask
well thought out questions.
There are many factors that can influence communication between healthcare workers.
The person‘s culture, whether they feel you are honest and can be trusted, your knowledge level,
and the amount of respect, patience and commitment that you show to others can ‗make or
break‘ you. Characteristics such as cynicism and sensitivity to constructive criticism can be
interpreted in a negative way.
Learning Outcomes:
Upon completion of this education module, the newly licensed registered nurse will:
1. Discuss how nonverbal and affective communication can support or cancel the meaning of
verbal communication.
2. Compare and contrast communication strategies that can help or hinder a nurse‘s
socialization process as a member of a healthcare organization.
Total Communication
Nonverbal
Expression/eye contact
Posture/appearance
Movement/gestures
Verbal
Spoken/written word
Vocal pitch
Rate tone
Affective
Feeling tone
Respect for space
Mood/emotion
Attitude

3
3. Recognize and describe situations where a newly hired nurse‘s effective communication
skills can enhance opportunities for personal growth and professional success.
4. Evaluate the effectiveness in interactions with co-workers, supervisors, physicians and
other members of the interdisciplinary health care team.
5. Describe how effective communication and the use of specific communication tools
ensures quality care and promotes patient safety.
6. Utilize clear and concise communication when directing nursing staff in patient care.
7. Develop communication techniques for approaching experienced co-workers.
8. Identify information that should be given in a concise manner when reporting on patient
conditions in situations such as shift report, pre-and post-procedure hand-off, team
huddles, patient care conferences, nursing rounds, physician rounds, and other
interdisciplinary conferences using SBAR.
9. Utilize effective communication that promotes decision making in unit meetings, team
conferences, and patient care conferences.
10. Develop awareness of how to communicate with individuals of different generations and
cultures.
11. Offer constructive feedback that incorporates empowering communication techniques to
a patient or family member.
12. Examine strategies to respond assertively when feedback is perceived to be negative
or inaccurate.
Interactive Exercises
1. Write a paragraph discussing a recent incident, preferably personal, in which a
communicator failed to communicate what was intended. Analyze why this happened and
how it could have been avoided.
2. Introduce yourself to co-workers and other members of the healthcare team. Ask them
why they chose their profession and what they like best about it.
3. Prepare questions to ask in orientation to a new facility or new position.
4. Review the policy/guidelines on how to access the use of a medical interpreter.
5. Take the Diversity Self-Assessment in the Preceptor Education Program (PEP): Types of Conflict M6.04.1, Personal/Value Differences. Discuss this with your preceptor.
6. Call a physician with your preceptor by your side using an SBAR tool.
http://www.saferhealthcare.com/sbarsamples.pdf
Guidelines for Report Assessment of My Report
Identify self, unit, patient, room number

4
State problem briefly, what it is, when it happened or started, how severe
Give pertinent background information
related to the situation to include:
Admitting diagnosis, date of admission
Current meds, allergies, IV fluids, labs
Most recent vital signs
Lab results: date, time, previous results
Other clinical information
Code Status
Your assessment of the situation
Your recommendation, what you want from
the provider
Guidelines for Report Assessment of My Report
Patient full name
Room number
Major diagnosis
New or changes in physician orders
Critical assessments included
PRN medication received
Lab results or diagnostic tests done
Activity level of patient
% eaten
Voiding and BM
Results of treatments
Concerns of the patient
If verbal did you tell staff that you would answer any questions they have at the end of report?
If taped or by phone, could it be heard?
Was the report complete?
Were you concise?

5
7. Participate in a team huddle or nursing rounds. Reflect on the participants in this group
activity, identifying their generational characteristics and variables, their style of
communication, and how you felt when interacting with them. Discuss this with your
preceptor.
8. Complete the following reports and use the table below to assess your reports, then
discuss each one with your preceptor:
a. End-of-shift report
b. Telephone report when transferring a patient
c. Medication reconciliation
d. Receipt of a transfer, post-op, post-procedure or newly admitted patient
9. Ask your preceptor if they would like feedback from you and if so when and how?
Ideally, the opportunity to provide feedback to your preceptor will come up during
orientation when you‘re talking about the feedback process for you.
What is your motive for giving feedback to your preceptor?
Is it to make your learning experience better?
What is appropriate feedback to give your preceptor?
10. Review the table on characteristics of different generations in the workforce and identify
challenges you might have with communication. (Refer to table in supplemental
resources.)
11. Ask for feedback from your preceptor on a task or skill you have performed. Keep in mind
the following:
Show how you applied knowledge and skills you know.
Receive feedback non-defensively, show appreciation, and explain your view using
diplomacy.
Display a positive learning attitude and openness to learning new ideas.
Take initiative to seek out information and learning on your own.
12. Reflect for a moment on your experience with receiving feedback. Think about both
positive and negative experiences.
How would you rate your openness to receiving feedback today?
How would you like feedback to be presented to you?
Informally as you‘re working with patients?
In private after a session with a patient?
After you‘ve had a chance to self-reflect and present your own evaluation of your
performance?
Together with suggestions to improve your performance?
Together with ideas and information that lets you decide how to improve your
performance?
What did you do well?
What could you have improved?

6
Keep these notes handy to refer to when you and your preceptor discuss the feedback
process.
13. Respond to the following telephone case scenario.
Mary Jones is a 65 year old who has been suffering with flu-like symptoms for several
days. She calls her primary care provider to talk to the nurse. This conversation follows:
Nurse: ―Mid-City Clinic, this is Amy, can you hold for a minute.‖ After a 2-3 minute wait,
Amy comes back on the line.
Patient: ―Is this the nurse?‖
Nurse: ―Yeah, this is her. What can I help you with?‖ Patient: ―This is Mary Jones. I have been feeling terrible. I think I have the flu. But I
shouldn‘t have the flu; I got my flu shot last fall. What do you think?‖
Nurse: ―You may have the flu but we are so busy with flu patients, the doctor doesn‘t have
any openings until tomorrow.‖
After a brief pause, patient responds hesitantly.
Patient: ―I can‘t come tomorrow, I just feel bad. I have to see the doctor today.‖
Nurse: ―There are no openings today; you will have to go the emergency care clinic, okay,
good-bye.‖
What is wrong with this communication interaction? What information was not
requested? What attitude was conveyed by the nurse in her responses?
14. While observing a LPN/VN, medication aide, nursing assistant or unlicensed assistive
personnel give constructive feedback on a task that they did. Give a positive and a
negative feedback. Utilize the table below to assess your results.
15. Read the following case scenarios and discuss with your preceptor.
Feedback Suggestions Assessment of Your Feedback
Was it timely?
Constructive to learn from mistakes?
Objective (just the facts) and accurate?
Specific and relevant to the situation?
Did you include:
What was done right?
What needs improving?
What to do next time?
Avoid words ―all‖, ―never‖ ―always‖?
Avoid assumptions about intentions?
Avoid interpretations related to actions?
Was it firsthand information or a comment from a
colleague?
Did you make sure the person knew you were giving
feedback?
Did you let the person go first?

7
Scenario # 1
You work in a surgical area. The LPN/VN is very talkative with her patients but her
conversation is often not related to care. She talks about her children and her personal
life. She is supposed to ambulate her patients each morning. She develops rapport with
them easily and you give her this positive feedback, then you encourage her to ambulate
her patients as directed. She thanks you and quips ―I know what I‘m doing‖. Two days
later the chattiness continues and her patients still haven‘t been walked by 11:00.
What points would you want to include in providing feedback to this LPN?
In deciding how to address the issue, keep in mind that you‘ve already addressed it once
with the LPN. How might that impact on what you‘re going to say this time?
Scenario # 2
John, a LPN is very quiet and fearful that he might make an error in his first few days of
giving medications. He is hesitant and tells you that he gets very flustered when he feels
rushed or when someone is watching him. He appears motivated but when asked to
demonstrate the checking of his medication, he says ―Can I watch you once more?‖
Use the following questions to guide your response:
What are some of the possible causes of John‘s anxiety?
Ask John to express some of the concerns with giving medication? (3 checks, number of
patients, time allowed, number of medications per patient, etc)
Does John understand that it may take longer when you first start passing medications?
Scenario # 3
A UAP performed a risky intervention trying to get up a patient by himself without a gait
belt that required two assist. You inform him that you wish to be present for the next 2
assisted transfers until you felt confident that he can work independently. He has made
comments to another team member on the unit about the quality of your skills. He said
you were very critical.
How would you address your UAP‘s behavior and his evaluation of your skill?
Questions to guide you response:
1. First, how angry are you? If your anger may overpower your efforts to be
constructive, you may want to wait until you‘ve cooled down to talk to the UAP.
2. You‘ve got two issues to deal with here − the UAP‘s unprofessional behavior and his
frustration with the limited level of independence you‘re giving him. Consider which
one should be dealt with first. For example, will you be better able to problem-solve
the issue of independence if you first get the bad behavior issue out of the way?
Did you share your perspective?
Did you mutually develop a plan?
Did you follow up with observation?

8
3. In both instances, consider how you can address them in a way that allows the
UAP to reflect and come up with his own solutions.
16. How would you handle the following situation? Complete an incident report on this
situation. Have your preceptor review it with you. Complete an incident report on a real
situation if possible.
Annie Smith was found by the nursing assistant in the bathroom of her room (209). Her
left leg was bent underneath her body at the knee. She was crying out in pain, ―Help me!
Help me! I slipped in my urine when getting up from the stool. My leg is hurting really
bad. Get me up! Get me up!‖
17. How would you communicate the following situation to the RN charge nurse?
A LPN/VN is drawing up an injection from an ampule using a filter needle. A nursing
assistant is helping the nurse roll the patient over for the injection. The nursing assistant
reports to you that after he commented on how big the needle was, the nurse pulled the
needle out of the patient‘s skin quickly, went to the medication room and returned with a
―thinner needle‖ on the syringe and finished injecting the medication into the patient.
18. Verbal orders are taken from physicians only in emergency situations. What would
be your reply to the physician on rounds when he gives you a verbal order to slow
down the IV rate to 125gtts/min and add potassium 40 mEq to the next IV bag?
19. You are working with an experienced RN. She does not mix the regular and NPH
insulin correctly and does not double check her insulin with another nurse? How
would you confront her with your observation of this incorrect procedure? Review the
TeamSTEPPS Strategies such as Two-Challenge rule, CUS, Call-out and Check Back.
http://teamstepps.ahrq.gov/aboutnationalIP.htm
21. Role play with your preceptor or another nurse the scenarios in the document
Communication Components. (Refer to the supplemental resources.)
22. Participate in a committee meeting. Offer to take the minutes. Observe therapeutic
communication techniques and techniques that block effective communication. Be
attentive to the affective and nonverbal communications that you observe. Discuss this
with your preceptor.
24. Review the document Communication with Age Groups and observe other nurses
interacting with patients of the particular age group you are working with. (Refer to
document in the supplemental resources.) Talk with your preceptor about what you
observed. From a generational perspective, discuss your communication style.
25. Perform an admission assessment in a hospital setting or a MDS data collection tool in a
long term care setting. Have your preceptor review the form and offer feedback on
content included. These forms are communication tools utilized by nurses.

9
References
Bossers, A., Bezzina, M., Hobson, S., Kinsella, A., MacPhail, A., Schurr, S., Moosa, T.,
Rolleman, L., Ferguson, K., DeLuca, S., Macnab, J., Jenkins, K. Preceptor
Education Program for Health Professionals and Students. Accessed September 29,
2010, from http://www.preceptor.ca/index.html Module 3: Giving and Receiving
Informal Feedback
Cardillo, D. (2005). Do nurses eat their young? Retrieved September 29, 2010 from
http://www.nurseweek.com/news/Features/05-01/DearDonna_01-10-05.asp
Delaney. C. (2003). Walking a fine line: Graduate nurse‘s transition experiences during
orientation. Journal of Nursing Education. 42(10), 437-443
Haig, K., Sutton, S., Whittington, J. (2006). SBAR: A shared mental model for improving
communication between clinicians. Joint Commission Journal on Quality and Patient
Safety, 32 (3) pp. 167-175.
Hallberg, I., Norberg, A. (2008). Strain among nurses and their emotional reactions during
1 year of systematic clinical supervision combined with the implementation of
individualized care in dementia nursing. Journal of Advanced Nursing, 18 (12) pp.
1860-
1875.
Hartman-Ellis, B. Miller K. (1994). Supportive communication among nurses: effects on
commitment, burnout and retention. Health Communication, 6 (2) pp. 77-96.
Hill, S., Howlett, H. (2009). Success in practical/vocational nursing: From student to leader. (6th
ed.) St. Louis: Saunders. Chapter 11 Straightforward Communication.
Improving Interpersonal Communication Between Healthcare Providers and Clients:
Reference Manual. Quality Assurance Project 1999. Center for Human Services,
Bethesda, MA http://www.qaproject.org/training/ipc/ref.pdf
Phillips-Jones, L. (2003). The mentee‘s guide: How to have a successful relationship
with a mentor. (revised edition). Grass Valley, CA: Coalition of Counseling Centers.
Tamparo, C., Lindh, W. (2008). Therapeutic Communications for Health Care. (3rd
ed). New
York: Thompson Delmar Learning.
Zemke, R., Rains, C., Filipczak, B. (2000). Generations at work. Managing the clash of
veterans,
boomers, xers, and nexters. New York: AMA Publications

10
Supplemental Resources
Table -- Generational Characteristics
Comparison of Characteristics for Each Generational Age
Variable Matures Baby Boomers Generation X Millennials
Years
1922 to 1946
1946 to 1964
1965 to 1980 1981 to 1991
Population
at Birth 75 million 80 million 46 million 81 million
Names
Silent Generation
Traditionalists
Best Generation
Veterans/Ikes
GI Generation
Me Generation
Sandwich Generation
Slackers
Busters
Cuspers
Busters
Generation Y
Nexters
Echo Boom
Baby Busters
Millennial Kid
Netsters Generation
Slogans
Waste not, want not
Rock around clock
We are the world
Candle in the wind

11
History
Great Depression
The Holocaust
Hindenburg Crash
World War II
Apollo XI Moonwalk
Watergate
Civil rights
Vietnam
3 Mile Island disaster
HIV/AIDS
Challenger Shuttle
Anti-war
demonstrations
Oklahoma City
bombing
Hurricane Andrew
Columbine High
School
Desert Storm
Morals
and
Values
Loyalty/patriotism
Hard work
Duty
Sacrifice
Dedication
Must vote
We deserve it
Personal Fulfillment
Optimism
Crusading causes
Idealism
If want to vote
Uncertainty
Personal focus
Live for today
Eliminate the task
Skepticism
Vote but private
―What‘s next?‖
On my terms
Just show up
Do what‘s asked
Positive outlook
Voter issues
Money
Fiscal Conservatism
No handouts
Pay as you go
What is credit?
Men had the money
Spend, spend, spend
Buy now, pay later
Credit card debt
Joint accounts
Who pays for what?
Save, save, save
Savings account
Bargain for best deal
Credit card for deal
Individual accounts
Earn, save, spend
Saving account
Save for
needs/wants
Credit card paid off
Joint accounts
Marriage
Marry young
Until death Do you
part
Grow old together
Decent house
Birth control
40% divorced
Sexual freedom
Expensive house
Live first then…
Put off marriage
Fear of commitment
Do I need a house?
Find the right
partner
Want marriage to
last
Gay marriages
Live with parents

12
Family
Wife/mother Home
Extended family
Chores then fun
Meals at table
4-6 children
Started young
Suburb living
Rebellious youth
Never home to eat
1-2 children
Parents work
Single parenting
Latchkey kids
Eat-on-the-go
1-2 children
Value/respect
parents
No regular
mealtimes
Tech nerds
Eat when hungry
2-4 children
Health
Home remedies
Polypharmacy
Forced exercise
Pickled/canning
Stress illnesses
Stress medication
Exercise for looks
TV dinners
High noncompliance
rate
Only needed meds
Exercise for a goal
Fast food
Research own health
Herbals or none
Exercise part of life
Health food/fast
foods
Technology
Radio
Typewriters
Telephone
Typewriters
Television
Some computers
Computer literate
Laptops
E-mail/FAX
World wide web
Palm Pilots
E-mail/text message

13
Work Style
Corporate loyalty
Seniority
―Pay your dues‖
Authoritarian
Top down decisions
Disciplined
Dutiful listeners
Appreciative
Pride in work
One job whole life
Job security
Want to win
Work fast
Teaming Recognition
Consensus
Participatory style
Question authority
Autonomy
Relationships
Discussion
Workaholics
Idealistic
Job opportunity
Want to manage
I win, you lose
Work efficiently
Individualist
Trust peers
Gratification
Goal oriented
Coaching style
Work/life balance
Flexible schedules
Immediate benefits
Entrepreneurs
Innovative
Portable careers
I win, you win
Work effectively
Multitaskers
Job security
Respect for authority
Authoritative
Immediate rewards
Instant change agent
Flexible schedules
Work with
distractions
Future rhinkers
Appreciate diversity
Go with the flow
I win, you win
Work on task
Education
Training
Learning
Styles
8th Grade to HS
experiences
Rote memory
One-room school
Lecture
Expert presentation
Structured
Policy-oriented
On job training
Verbal explanation
Private feedback
Linear thinkers
College/birthright
Group discussion
Discovery learning
Middle schools
Enhancement
Personal contact
Past experiences
Lots of examples
No games
Reasoning
Hands on
Linear thinkers
College degrees
Variety of media
Learn thru games
Preschools
Choices to learn
Work best with peers
Needs to be ―fun‖
Wandering minds
No long discussions
Investigate/question
Immediate feedback
Critical thinkers
Technical degrees
Variety of media
Self-paced learning
Web schools
Computer
interaction
Focus on tasks
Use graphics &
color
―Fun stuff‖
Short reading
material
Lifelong learning
Hands n
Mosaic thinkers
References:
Hicks, R., Hicks, K. (1999). Boomers, xers, and other strangers. Illinois: Tyndale

14
Lancaster, L., Sillman, D. (2002, February 1). When generations collide: Who they are. Why
they clash. How to solve the generational puzzle at work. Retrieved April 1, 2004, from
http://www.socialsciencesweb.com/When_Generations_Collide_House
Zemke, R., Rains, C., Filipczak, B. (2000). Generations at work. Managing the clash of
veterans, boomers, xers, and nexters. New York: AMA Publications
Table -- Communication with Age Groups
Techniques for Communicating with the Young and Older Adults
Children - Consider the parents a good source of reliable information about the child; although
some parents may exaggerate certain points. Offer small children toys or materials to do so the
parents can give their full attention to your information gathering.
Developmental
Level Thought Processes, Communication Patterns Recommended Communication
Techniques
Newborn
(birth to 1 m)
Mouthing, rooting, and sucking. Attends to
stimulation with eye movements, starring,
facial and body movements (reaching).
Demands relief from discomfort by crying. If
over stimulated looks away, arches back,
rapidly moves arms and legs, cries
Use high-pitched voice; make eye
contact about 8 inches from the
face. To calm crying newborn,
hold while making soothing
sounds, patting newborn, moving
in rocking fashion observe for
bonding between infant & parent
Infant
(1 m to 1 y)
Signals by smiling, cooing, blowing,
laughing. Delay in gratification of needs is
threatening. Most influenced by the sound of
the voice. Parents can tell after while what
each type of cry means. Few words (mama,
dada) by late in first year. Imitates facial and
body gestures at 1-2 months, initiates
nonverbal behaviors(reaching to be held,
pushing objects away, shaking head) around
6 months. Fear of strangers begins at 6
months
Make contact slowly, respect
personal space, mimic parents‘
tone and behavior. Interact with or
through parents to prove one is a
―safe‖ person, keep parent in view
during interaction. Respond to
needs promptly. No loud or harsh
sounds or sudden movements.

15
Toddler (1 to 3 y)
Vocabulary increases, but not consistently verbal. The body acts out what the words
cannot tell. Children are egocentric, believe
that others know what they want, so may
refuse to verbalize when prompted. Can
effectively use gestures—pointing, pushing,
pulling adult, shaking head
Separation Anxiety – sense of abandonment;
loud protest, kicking, crying until they go to
sleep
3 stages-Protest, Despair, Denial
Focus on child. Set concrete limits and abide by them
consistently. Provide an
opportunity for child to explore
new environment (equipment used
for health assessment). Use
concrete explanations, short
sentences, and incorporate child‘s
words when possible. Know that
they may regress with personal
needs such as potty training,
brushing teeth etc. Laughing at
them or trying to reason is
counterproductive. Tantrums
common, removing them from the
area to a more quiet area does
help. Don‘t wait until the child
falls asleep for the parent to leave-
it will disrupt their sense of trust.
Playing games such as peek-a-boo,
hide and seek, toys, pictures of the
family or favorite stories help a
lot, maintain family routines while
in hospital.

16
Preschool (3 to 5 y)
Talks for the fun of it, engages others in conversation. Vocabulary limited, each word
has only one meaning. Can answer direct
questions about self, feelings. Still
egocentric, ascribes human feelings, needs,
and motives to objects, believes most events
are controlled by adults. Views events in
cause—effect terms with cause near in time
to effect. Feel they can cause events by own
thoughts
Uses direct concrete questions, explanations. Avoid analogies
(shot is a ―little stick in the arm‖
may evoke image of a stick from a
tree poked into the arm; better to
say ―needle stick‖). Watch the
words you use such as ―you just
kill me‖ or you‘ll get a bang out of
this‖, Prepare for new experiences
(medical treatment) by
encouraging manipulation of
objects involved in viewing, then
participating as procedure is
carried out on a doll. Using play
to reenact the event after it is over
will also reduce feelings of
powerlessness. After
hospitalization the preschooler
may be irritable and demanding,
they want to stay home with mom
or dad and not go to babysitter.
School age
(5 to 12 y)
Thinking is still concrete. Can reason
logically, to understand cause and effect.
Grasps that body has internal parts that
perform functions. Can make choices
between alternatives, even if all are
undesirable. Can grasp that something can
hurt and still be good for them. Able to
mentally rehearse to prepare for a difficult
event. Is open and candid if trust is
established—can precisely express concerns
and needs for help. Seek explanations—
why? why? why?
Show interest in child‘s point of
view. Listen actively. Provide
information and support to prepare
for new experiences. Use actual
objects or pictures (internal
organs, operating room
equipment) for explanations of
illness or procedures. Give
choices whenever possible.
Involve the child directly in
activities or procedures—give
opportunity to perform task or
assume key role.

17
Adolescent (12-18 y)
Ability to think abstractly begins about age 11 and develops throughout this period.
Fluctuations between adult and childlike
thinking and behavior are common. Group
identity is important; is evidenced by
appearance, selection of activities, modes of
verbal expression. Control issues-like to be
involved in decisions.
Convey acceptance, respect. Listen actively. Use
conversational tome when
questioning to avoid impression
that the ―right‖ answer is
expected. If possible, spend time
when no demands are made.
Focus questions on essential
information versus global inquires,
especially with younger
adolescents. If dealing with
intimate or private concerns,
assure confidentiality. Don‘t
impose judgments or values on
them. Sit, don‘t hover over them.
Don‘t stare, be at eye level.
Allow friends to visit with rules
for behavior during visits.

18
Techniques for Communicating with the Elderly
Elder- Include family and friends in the conversation but don‘t let them take over the
conversation; speak to the elder not to the family in front of the elder.
Communication Patterns Recommended Communication Techniques
Sensory deficits; hearing, seeing. Attention
deficits; memory and distractibility. Difficulty
with articulation due to change in oral cavity,
voice tone, dentures, and dry mucous
membranes. May be aphasic. Fatigue is more
common. Like to reminisce. Find support in
family and friends.
Listen carefully and speak to the unaffected ear.
Make sure hearing aid is in place if worn.
Speak in a slow low pitched tone. Turn off
background noise (TV, Radio). Make sure
glasses are on and clean. Use large print
materials with contrasting colors. Use visual
cues such as pictures, objects. Bold colors; No
pastel colors. Proper lighting in the room (over
the shoulder light is better than overhead). Be at
eye level in front of elder. Interview early in the
day. Watch for cues that might indicate fatigue
such as eye drooping, leaning or vague
answers. Don‘t use long sentences. Use focus
and open ended questions. Allow time for
answers. Be aware of items in the room for
reminiscence to develop sense of well being. If
aphasic, fill in words for the elder. Repeat
sentences and words with changing the phrase.
References:
Potter, P., Perry, A. (2007). Basic nursing: essentials for practice. (6th
ed.) St. Louis:
Mosby/Elsevier.
Roach, S. (2001). Introductory gerontological nursing. Philadelphia:
Lippincott/Williams/Wilkins.
Tamparo, C., Lindh, W. (2008). Therapeutic communications for health care. (3rd
ed.)
New York: Thompson/Delmar Learning.

19
COMPONENTS OF COMMUNICATION
To examine the process of communication it is necessary to interrupt the process – thus
artificially giving it a beginning and an ending. By punctuating communication in this manner,
what is really a complex and ongoing process appears to be much simpler than it really is. For
the purpose of study, an interaction may be isolated from the total communication as the
following illustrates:
A. Nurse Do you mean that you were awake the entire night?
B. Patient: No, it just seemed that way. The last time I looked at the clock it was about 2
A.M. I probably dozed off after that, but I just couldn‗t stop thinking.
A. Nurse: What were you thinking about?
In this interaction, A sends a message to B: ―Do you mean that you were awake the entire
night?‖ B receives the message and returns a message to A ―No…it just seemed that way.‖ A
receives this message and sends another, ―What were you thinking about?‖ This provides a
simple way to analyze the interaction. However, analysis increases in complexity when A is
viewed not only as sending a message to B (―Do you mean that you were awake the entire
night?) but, also simultaneously receiving non-verbal messages from B. B may be looking
downcast, fidgeting with the bed covers or staring out the window for example. While receiving
a verbal message from A, B is also sending nonverbal messages and receiving A‘s nonverbal
message. So simply to identify A as the sender and B as the receiver, when both are
simultaneously sending and receiving messages, is artificial, but useful for learning purposes. In
reality, the process is much more dynamic and complex than the study model indicates. For the
purpose of study, it is appropriate to identify five functional components of the communication
process in an interaction.
VOICE
Nonverbal communication also occurs through the voice. The rate of speech, loudness and tone
of voice, and diction all convey messages about the speaker and the speaker‘s intent.
Mrs. Miller: Did the doctor tell you the results of my liver biopsy yet?
Nurse Roberts: Will (pause) no (longer pause), but I‘m sure he will be in later to talk to you.
Let's get on with your treatment (at faster speed).
The use of pauses and a change in the rate of speech may give a variety of negative nonverbal
messages including the messages that the speaker is being less than truthful with the listener.
Voice tone conveys meaning, even when language is not clear. Pets and young children, for
example, often respond to a commanding voice tone, even though they do not understand all of
the speaker‘s words.
The use of pauses and a change in the rate of speech may give a variety of negative nonverbal
messages including the messages that the speaker is being less than truthful with the listener.
Voice tone conveys meaning, even when language is not clear. Pets and young children, for

20
example, often respond to a commanding voice tone, even though they do not understand all of
the speaker‘s words.
TEACHING
Nurses are frequently involved in formal or informal teaching of patients about their health care.
The following examples illustrate collaborative communication in a teaching situation.
I‘m Jeff Smith, one of the nurses from the nursery. I invited all of you new mothers
together so you could share your concerns about caring for your infants. We‘ll all have a
chance to exchange ideas with each other. You may also want to ask me questions and
I‘ll also demonstrate various ways of bathing and dressing babies for those of you who
would find that helpful.
Mrs. Nguyen, let‘s practice together the breathing techniques you learned in your Lamaze
class. That will help us to work together more effectively later when your labor is
stronger.
Mr. Swanson, why don‘t we take a few minutes to review those leg exercises in the
exercise plan that you and the physical therapist developed. That will help us decide
whether you need any assistance from me to do them correctly.
FACILITATING EXPRESSION OF FEELINGS
Facilitating expression of feelings is a powerful skill in the nurse-patient relationship.
Expressing feelings (1) is an effective means of defusing one‘s emotions and preparing for
problem solving and (2) provides opportunities for personal growth. Such openness, however, is
perceived as a risk by some individuals. Patients may believe that exposing personal feelings
will cause nurses to perceive them as weak or unworthy. Fearing rejection, they may withhold
expressing their concerns. Nurses who are able to effectively communicate empathy, respect and
caring will create a climate of trust in which open expression of feelings is more likely to occur.
The following example illustrates this.
Nurse Reed: I noticed you seem to be apprehensive today. Is something on your mind
you‘d like to talk about?
Ms. Jacob: Dr. Smith said I could go home today and….well I‘m not sure that‘s such
a good idea.
Nurse Reed: The thought of being discharged is making you uneasy….Could you tell me a bit
more about that?
Ms. Jacob: It‘s difficult to talk about…but since the mastectomy, I don‘t feel like myself.
Maybe I lost more than a breast in surgery.
Nurse Reed: The idea of returning to your home roles---being a wife and mother---seems a
little overwhelming?
Ms. Jacob: I…..a little I guess. Somehow I‘m feeling rather inadequate.

21
Helping patients get in touch with and to express their feelings increases self-awareness. It is a
beginning point for dealing with feelings.
ALLEVIATING ANXIETY AND FEAR
Anxiety is frequently associated with alterations in health status. Nurses are often called on to
clarify information patients have received about their health or illness and to assist patients with
common anxiety-producing situations such as preparing for surgery or exploration of a patient‘s
fears about anesthesia.
Mr. Gagne: The thing that scares me most about surgery is the spinal
anesthesia. I‘m afraid it‘ll leave me paralyzed.
Nurse Mendoza: Paralysis is a frightening thought. Let‘s talk about spinal anesthesia.
Maybe our discussion will put your mind at ease.
An opportunity to identify and discuss fears and anxiety is often sufficient to alleviate or even
eliminate them.
PROMOTING PROBLEM SOLVING
The working phase of the nurse-patient relationship involves the patient‘s identifying the
problem making a commitment to action to solve the problem, and acting on the commitment.
Collaborative communication during these phases of the relationship often provides the impetus
for patients to make a decision and act on it. Nurses facilitate patient exploration of personal
values, particularly values that may conflict with one another. This may require that nurses press
patients for more concreteness or specify---which may be threatening to patients. To prevent
this, it is important that a sufficient level of trust be developed before using more confrontational
communication.
Ms. Catalfa: I‘m really confused. Dr. Li says my stomach problem may be helped by
medicine, but that often surgery is necessary. I can‘t decide whether to try the
medicine for a while—or just get it over with and have the operation now.
Nurse Kohn: I get the feeling you are uneasy about the surgery but unwilling to go through too
much more of the kinds of symptoms you‘ve been experiencing.
Ms. Catalfa: Yes, the pain and the nausea, and now the bleeding has been really awful—I
mean, it was really scary to see blood when I vomited last week. But the idea of
surgery—I‘d be laid up for a while…I‘d have pain..
Nurse Kohn: You have to choose between two alternatives, neither of which looks desirable.
It‘s not an easy situation, but that seems to be the reality right now.
Ms. Catalfa: You‘re right. There‘s no getting around it. I might as well stop feeling sorry for
myself and get some more information. Can you tell me anything about that drug
Dr. Li mentioned? I can‘t even remember the name of it.
In helping patients to recognize attitude or behaviors that are not conducive to problem solving,
nurses facilitate patients making alternative choices.

22
Listening
Listening is an active process as contrasted with hearing, which is a passive process. Listening is
also an art that involves not only use of the auditory senses but the use of a third ear, so to speak,
that allows the listener to be aware of verbal and nonverbal behavior, the concurrent
metacommunication, the context, and the effects of internal feedback. This is no easy task, and
no one is able to do this all of the time; however, awareness that listening is a crucial ingredient
to successful communication is the first step to being an effective listener. Certainly everyone
has been involved in interactions in which one participant seemed distracted or disinterested.
The effect on the other participant can be devastating. However, when a listener really focuses
on the speaker and responds appropriately to the message, the effect of being truly heard can be
quite uplifting.
Attending Behaviors
Attending behaviors are those physical acts and verbal cues that a listener uses to communicate
interest in a speaker. As emphasized earlier, nonverbal and metacommunication significantly
affect communication. A listener using attending behaviors is consciously selecting nonverbal
behaviors and verbal behaviors such as ―um,‖ ―uh-ha,‖ and ―go on‖ with the intent of
encouraging the speaker to continue. Being given the benefit of another‘s time, energy, and
attention enhances a speaker‘s self-respect and encourages self-exploration.
The following table shows a given nonverbal modality can also communicate inattentiveness,
which compotes rejection and is injurious to trust and communication in a collaborative
relationship.

23
HOW NONVERBAL MODALITIES COMMUNICATE ATTENTIVENESS
OR INATTENTIVENESS
Nonverbal Modality Inattentiveness Attentiveness
These behaviors are likely to
close off or slow down the
conversation
These behaviors encourage
communication because they show
acceptance and respect for the other
person
Space Distant/very close Approximately arms length
Movement Away Toward
Posture Slouching, rigid-seated leaning
away
Relaxed but attentive, seated leaning
slightly toward other person
Eye contact Absent: defiant, jittery Regular
Time Continues with present action
before responding, in a hurry
Respond to first opportunity, share time
with helper
Feet and Legs (in
sitting)
Used to keep distance between
the persons
Unobtrusive
Furniture Used as a barrier Used to drive persons together
Facial expression Does not match feelings, scowl,
blank look
Matches own or other‘s feelings, smile
Gestures Compete for attention with
words
Highlight own words, unobtrusive,
smooth
Mannerisms Devious, distracting None or unobtrusive
Voice, volume Very loud or very soft Clearly audible
Voice, rate Impatient or staccato, very slow
or hesitant
Average or a bit lower
Energy level Apathetic, sleepy, jumpy, pushy Alert, stays alert throughout a long
conversation
The following examples illustrate levels of empathic response made by a nurse to a patient‘s
statement.

24
EXAMPLE 1:
Patient: The harder I try to get along with my son, the more I feel he just wants
to be left alone.
Nurse:
Level 1: He‘s making it plain how he feels. Why not just accept that? (Hurtful
response)
Level 2: That‘s a shame. (Communicates a partial awareness of surface feelings
only)
Level 3: It must be hard for you to reach out and have him reject you. (Surface
feelings reflected)
Level 4: It is upsetting not to get the response you want. (Underlying feelings
identified)
EXAMPLE 2
Patient: I‘m really worried about that CT scan. Is it painful?
Nurse:
Level l: It‘s as easy as one, two, and three. (Doesn‘t deal with feelings at all.)
Level 2: Yes, it can be scary. (Partially acknowledges surface feelings.)
Level 3: It is kind of scary having a test that you know nothing about.
(Accurately acknowledges surface feelings.)
Level 4: Having tests, you don‘t know anything about can be upsetting. I wonder if it‘s
even more worrisome thinking about the possible outcome. (Acknowledge
underlying feelings.)
Respect
Respect communicates belief in a patient and is assessed as follows:
Level 1 imposes nurse‘s values or opinions, thus devaluing patients as individuals.
Level 2 indicates that a nurse‘s withholding him- or herself from involvement by
declining to enter into a relationship by ignoring patient‘s statements or by responding in
a casual or mechanical manner.
Level 3 indicates that a nurse perceives patients as persons of worth, capable of thinking
and acting responsibly.
Level 4 indicates that a nurse is willing to expend personal energy for a patient to further
the helping relationship.
The following example illustrates levels of respect in communication between nurses and
patients.

25
EXAMPLE 1
Patient: The staff really treats me like I‘m a child. Everyone tells me what to do no one
ever asks me my opinion. After all, it is my body.
Nurse:
Level 1: Well, you are sick. Don‘t you think you should let us take care of you? (Imposes
nurse‘s opinion on patient.)
Level 2: I don‘t think that I can help you with this. This is a personal matter between you
and the staff. (Declines entering into relationship.)
Level 3: It makes you angry not to be included in your health care decisions. Let‘s talk
about what we might be able to do. (Communicates openness to developing
relationships with patient.)
Level 4: It bothers you a lot not to be recognized for your capabilities to handle your life.
I‘ll certainly do what I can to help and I‘ll discuss this with the rest of the staff so
that everyone is aware of the need to involve you in the planning.
(Communicates acceptance of patient as a person of worth and willingness of
nurse to make extra effort to help.)
EXAMPLE 2:
Patient: When that nurse came in this morning she just about took my head off. She never
even said good morning – just ―turn over so I can give you your shot.‖
Level 1: You should have given her a piece of your mind. (Imposes nurse‘s opinion on
patient.)
Level 2: The nurse actually did that to you. (Casual remark, declines involvement.)
Level 3: It really upsets you to be treated like that. I‘m here if you want to discuss it.
(Open to a helping relationship with patient.)
Level 4: It hurts to be treated like an object. Would you like to talk about how to deal with
situations like this? Also I‘m willing to talk to the nurse, if that would make you
feel better. (Shows involvement and commitment on part of nurse.)
Note the similarity between the level 3 empathy responses and the level 3 respect responses.
When a listener is nonjudgmental in responding, the response combines both respect and
empathy.
Warmth
Through warmth, nurses convey genuine caring. Warmth is communicated primarily through the
use of non-verbal behaviors. Also, words such as, ―You‘re really in pain; let me do what I can to
help.‖ Convey caring. The levels of warmth are defined as follows.
Level 1: Displays visible disapproval or disinterest.

26
Level 2: Characterized by neutral or absent gestures and responses that sound
mechanical.
Level 3: Clearly shows attention and interest.
Level 4: Indicates that a nurse is intensely involved and attentive to the
interaction. Patients feel accepted and valued.
The following example illustrates these levels of warmth in a nurse‘s response to a patient‘s
statement.
Patient: I just want to get out of here. (Urgent voice tone, tense facial muscles.)
Level 1: Oh, so do I! (Goes on with tasks.)
Level 2: Looks at patient but does not change affect. Says without expression --
―That‘s too bad.‖ (Mechanical expression.)
Level 3: Sits down next to the patient, shrugs concern on face, and offers to talk about
situation. (Clear nonverbal response.)
Level 4: Uses most effective attending behaviors. Demonstrates positive affect. Appears
alert. Voice tones are appropriate to the seriousness of the interaction. Vocal
quality seems relaxed, serious, and concerned. Maintains eye contact. May make
physical contact such as a touch of the arm or shoulder. (Intense nonverbal
communication)
Sometimes a nurse can be very empathic and respectful, but still not be perceived as a warm
individual. In this situation, the nurse may find it takes longer to build a solid base for a helping
relationship. On the other hand, a nurse may display high levels of warmth and low levels of
empathy and respect. This occurs when a nurse doesn‘t really care about a patient or seeks to
manipulate a patient. Insincerity can usually be detected by patients.
Genuineness
A genuine person is one who has it ―all together‖, a congruent person. Levels of the genuineness
include:
Level 1: A nurse is defensive, punitive or deceitful to the patient.
Level 2: A nurse gives incongruent verbal and nonverbal messages.
Level 3: A nurse‘s responses are congruent; however the nurse refrains from displaying
feelings.
Level 4: A nurse‘s responses are not only congruent but also spontaneous. Whether the
patient is positive or negative, the nurse is real, and responds in a manner that is
constructive and opens new areas for exploration.
The following examples illustrate the levels of genuineness.

27
EXAMPLE 1
Patient: My baby is being kept in the nursery. I‘m really worried about him. I‘m also
worried that the separation will interfere with breastfeeding.
Nurse:
Level 1: Well, that‘s not my territory – you‘ll have to deal with the nursery staff
about that problem. (Defensive response)
Level 2: As a nurse on this unit, I can assure you that we will do all we can to help you.
(No nonverbal display of interest or wonder). (Incongruent verbal and nonverbal
behavior).
Level 3: I can see you‘re upset about this, but to be honest with you, I‘m a new nurse here
and I‘m not sure how I can help you. (Congruent verbal and nonverbal response.)
Level 4: I can see this is a problem for you. I‘m a little shaky about dealing with it
because of my newness on this unit. But I will go to the nursery and see if I can
get some answers for you. (Shows concern and willingness to help nonverbally.)
EXAMPLE 2
Patient: Does it ever bother you to give injections and to see all the blood and gore?
(Patient asks as nurse changes a dressing).
Level 1: Why should those things bother me? (Nurse is flip with patient)
Level 2: In my line of work, you learn to get used to everything. (Face shows disgust.)
(Incongruent verbal and nonverbal behavior)
Level 3: Yes sometimes it bothers me a lot. (Congruent verbal and nonverbal behavior).
Level 4: Yes, sometimes I really feel bothered by what I see. I realize that some
unpleasant things are temporary in the process of getting well. It‘s very satisfying
to be part of that. (Congruent verbal and nonverbal behavior and expression of
feelings.)
Self-disclosure
In order for patients to get the most out of a relationship, they eventually have to get to know
nurses so that they can relate to them more fully. This knowledge comes through a nurse‘s
appropriate use of self-disclosure. Self-disclosure involves sharing which is an important aspect
of mutuality. Levels of self-disclosure are:
Level 1: A nurse withholds all personal information.
Level 2: A nurse may answer some direct personal questions, but does not
volunteer information.

28
Level 3: A nurse reveals personal ideas, attitudes, and experiences in a general
fashion.
Level 4: A nurse freely and spontaneously shares personal information that is
relevant to a patient‘s interests and concerns.
The following examples illustrate the use of self-disclosure by a nurse reporting to a patient‘s
situation.
EXAMPLE 1
Patient: I can‘t seem to get the knack of giving myself an insulin injection. Did you ever
have trouble when you were learning?
Level 1: Oh you‘ll get it soon. (Shares no personal information)
Level 2: Yes, it was hard, but my situation as a nurse is different from yours. (Answers
direct question; does not volunteer information.)
Level 3: Oh yes, I remember it was very difficult for me to give injections. (Reveals
personal reaction in a general way.)
Level 4: Gosh yes, I can remember before my first ―real‖ injections. I practiced what I
would say, how I would give the injection and I injected dozens of willing
oranges. (Freely shares specific personal information.)
EXAMPLE 2
Patient: I‘ve been in the hospital so long, I‘m afraid that this will become a permanent
condition. Have you ever been hospitalized?
Level 1: It‘s more important that we talk about you. (Refuses to answer personal
question).
Level 2: Once, when I had my son. (Answers question but volunteers no information.)
Level 3: I was hospitalized once and I found it uncomfortable. (Answers personal
question in a general way.)
Level 4: I remember when I had my son, I felt homesick and uneasy. It gave me a greater
appreciation for how difficult it is to be in the hospital. (Freely shares specific
personal information in response to questions.)
Immediacy
In the helping relationship, immediacy refers to communication exchanged between nurse and
patient about their relationship at a particular moment in time. Because the communication can
involve both positive and negative information, immediacy can temporarily increase the anxiety
level of both nurse and patient.

29
Nurses should continually evaluate the strengths and deficiencies of a nurse-patient relationship
and cues that indicate obstacles in the relationship. Nurses need to deal with these obstacles in
order to help patients deal with important problems.
The levels of immediacy range from a nurse‘s ignoring all cues from patients about the
relationship, to a nurse‘s concise discussion of what is occurring in the nurse-patient relationship.
A level 1 response ignores all cues from a patient that there is a problem in the
relationship.
A level 2 response may give superficial acknowledgement about the interpersonal issue
but does not discuss it.
A level 3 response is characterized by the nurse‘s acknowledgement of the interpersonal
difficulty followed by a general rather than a personal discussion.
A level 4 response makes a precise interpretation abort the nurse-patient relationship and
discusses the issue in a direct personal and explicit manner.
The following example illustrates levels of immediacy a nurse uses in responding in a patient
situation.
EXAMPLE 1
Mrs. Crowley, an oncology patient has just been readmitted for the fourth time in year. All of
the nursing staff know her well and really like her. Nurse Blake has been her primary nurse.
Mrs. Crowley seems very upset when Nurse Blake enters the room. Nurse Blake says, ―You
seem upset. Can I help in any way? Mrs. Crowley says, ―What do you care? You get paid to
be nice. It‘s part of your job.‖
Nurse Blake:
Level 1: I‘m not always nice, believe me. (Ignores patient‘s question.)
Level 2: Boy! You sure do seem upset about something. It‘s time to take you to x-ray.
(Give token acknowledgement to expression to expression of immediacy, but
avoids discussing it.)
Level 3: You seem upset about something. I wonder what is bothering you. (Reflects the
patient‘s feelings about the relationship in a general way.)
Level 4: I‘m sorry to see that you doubt my regard for you. I wonder if you are afraid that
no one will be there to help you after you have surgery tomorrow. (Current and
specific interpretation of the behavior.)
EXAMPLE 2
Mr. Collins has been seeing Mrs. Kidwell, a psychiatric liaison nurse in the clinic for 6 months.
Mr. Collins has been recently unemployed and is experiencing a moderate degree of depression.
Mrs. Kidwell had to cancel their last appointment. This week, Mr. Collins refuses to look at her
and answers her in monosyllables and shrugs of his shoulders.

30
Mrs. Kidwell:
Level 1: If you don‘t care to talk today. Mr. Collins, that‘s fine with me. I‘m quite busy.
(Ignores the issue between nurse and patient.)
Level 2: You seem bothered today, but I‘d like to know what happened with the job
interviews you went on last week. (Gives token recognition to expressions of
immediacy and then changes the subject.)
Level 3: You seem upset today. Can I help? (Reflects feelings of immediacy and then
shows openness to sharing responsibility for improving the relationship.)
Level 4: You seem angry. I wonder if when I canceled our appointment last week, you
thought I was deserting you. (Explicit and specific interpretation of immediacy.)
The foregoing discussion has emphasized the use of verbal communication in each phase of the
helping relationship. Communication in each of the dimensions discussed above is enhanced
with the use of appropriate nonverbal behavior. The table below provides examples of ineffective
and effective nonverbal behaviors that are frequently associated with high or low levels of each
dimension.

31
EXAMPLES OF INEFFECTIVE AND EFFECTIVE NONVERBAL BEHAVIORS
Ineffective Behaviors Effective Behaviors
Helper nonverbal behaviors likely to
communicate low levels of the
dimension.
Helper nonverbal behaviors likely to
communicate high levels of the
dimension.
Empathy Frown resulting from lack of
understanding
Positive head nods, facial expression
congruent with content of
conversation
Respect Mumbling, patronizing tones of voice;
engages in doodling or self-
stimulating behavior to the point of
appearing more involved in that than
with the patient.
Spends time with patient, fully
attentive.
Warmth Apathy delay in responding to
approach of patient, insincere
effusiveness, fidgeting, signs of
wanting to leave (e.g. remains
standing some distance from patient
Smile: Physical contact proximity
Genuineness Low or evasive eye contact, lack of
congruency between verbal and
nonverbal behavior, less frequent
movement excessive smiling.
Congruency between verbal and
nonverbal behavior.
Self-disclosure Bragging gestures: points to self; self
important manner.
Gestures that keep reference to self,
low-key e.g. a shrug accompanying
the words when talking about a
personal incident.
Immediacy Turns away or moves back when the
conversation focuses on the present
relationship.
Concern: Eye contact
Failure to Listen:
There are three common barriers to effective listening. The first block is lack of attentiveness.
When nurses make eye contact with patients and display appropriate nonverbal and verbal

32
behaviors. In response to patients, the nurses are being attentive listeners. By contrast, nurses
who repeated glances at the clock or allow other concerns to flood their thoughts are not
attending to the speaker and their nonverbals will communicate their lack of involvement to
patients loudly and clearly.
The second barrier to effective listening is responding to content instead of meaning. If a patient
tells a nurse that he is tired because he lies awake at night and worries about his diagnosis and
the nurse responds that she will get him sleeping medication, then the nurse has missed the
whole point of the patient‘s communication.
Effective listening is also blocked when nurses responses are subjective- that is when nurses
respond to patients from personal feeling state.
Subjective Response
Patient: My son hasn‘t been to see me at all during this hospitalization.
Nurse: Well, that is certainly a selfish way to treat you. Doesn‘t he know that you
need him?
Empowering Response:
Patient: My son hasn‘t been to see me at all during this hospitalization.
Nurse: Sounds like that hurts.
Failure to Follow Up
Following up is to explore thoroughly a positive action in therapeutic communication.
Following up is a way of achieving mutual understanding. Effective follow-ups clarify or
pinpoint patient‘s statements, giving a nurse a richer understanding of patient perspective. When
patients statements are general or vague, failure to follow up can result in communication
remaining on a superficial level, which trivializes patient concerns. Inviting elaboration, on the
other hand, is a gift of oneself that enables patients to reveal more significant feelings if they
desire.
Failure to Seek Clarification
There are many occasions in human communication when words or messages are ambiguous –
that is they may convey several meanings. Sometimes the context or the topic of conversation is
sufficient to suggest intent, but assuming a speaker‘s meaning is usually unwise. It is quite
possible that the listener‘s interpretation and the intent of the speaker will differ. The differences
in interpretation can be the basis for further miscommunication, which may have a harmful effect
on the interaction-even on the relationship itself. Tin a nurse-patient relationship, failure to seek
clarification or verify a patient‘s meaning can lead to inappropriate nursing care. For example, a
new mother may say to a nurse, ―It really hurts me to breast feed. I think I should wean my
baby.‖ If the nurse does not seek clarification about what the patient means by ―it really hurts
me,‖ the nurse may come to the wrong conclusion about the kind of support to provide. The
―hurt‖ may be related to the development of mastitis, an infection that should be treated; it may

33
be an emotional, not a physical pain; or the hurt may be the result of the baby sucking
incorrectly. Each of these meanings would require a different nursing response.
Following Standard Forms Too Closely:
Using standard forms to obtain health information provides valuable information in a brief
period of time. However, relying entirely on such forms cuts off exploration of patient feelings
and perceptions about their situation and relegates patients to the role of objects. If pressed for
time, nurses can note areas of further concern for future follow-up and can promise to return later
to discuss them.
Being Judgmental
Being judgmental essentially communicates to patients that they should think and feel as the
nurse does. Statements such as ―That‘s good‖, ―that‘s bad,‖ ―you shouldn‘t do…. or ―you should
do….‖ Are judgmental and place nurse‘s values, beliefs, and perceptions above those of patients.
Giving Easier Reassurance:
Comments such as ―Everything will be fine‖, attempt to wipe away the pain of a patient‘s
situation. Such remarks deny or block patient‘s expressions of feelings. They are meaningless
and insulting. False reassurance‘s often used when nurses are uncomfortable with the topic on
emotions, a patient is sharing. Patients feel genuine reassurance when they feel accepted and
secure as a result of other elective communication with a nurse.
When nurses feel the need to protect others, they may block a patient‘s discussion of feelings or
opinions. For instance if a patient says, ―That nurse Sara Blackwell is so rough; I hate it when
she comes on the 3-11 shift‖, and her nurse responds by defending Sara Blackwell, that nurse is
rejecting the patient‘s opinion. Defending statements convey the message to patients that you do
not have the right to complain and your feelings are not important.
ADDITIONAL EMPOWERING COMMUNICATION TECHNIQUES
Technique Description Therapeutic Values
Silence Periods of no verbal
communication among participants.
Nonverbally communicates
nurse‘s acceptance of patient.
Establish guidelines State roles, purpose, and limitations
for a particular interaction.
Helps patient to know what is
expected.
Give broad openings Ask patients to determine the
direction the interaction should
take.
Enables patient to decide what to
discuss and to encourage
continuation of the interaction.

34
Reduce distance Diminish physical space between nurse and patient.
Nonverbally communicates that nurse wants to be involved with
patient.
Acknowledgement Recognize patient for contribution
to an interaction.
Emphasizes the importance of
patient‘s role within the
relationship
Restate Repeat what the nurse believes to
be the main thoughts or feelings
expressed.
Asks for validation of nurse
interpretation of the feeling or
message.
Reflect Direct back patient‘s ideas,
feelings, questions, or content
Attempts to show patient the
importance of patient‘s own
feelings and interpretations.
Seek clarification Ask for additional input to
understand the message received.
Demonstrates nurse‘s desire to
understand patient‘s
communication.
Follow up To explore thoroughly, asks
questions to stimulate elaboration.
Enables expression of deeper
feelings, enhances mutuality.
Seek consensual
validation
Attempt to reach a mutual
denotative and connotative
meaning of specific words.
Demonstrates nurse‘s desire to
understand patient‘s verbal
communication and emotions.
Focus Questions to help patients develop
or expand an idea.
Directs conversation toward topics
or feelings of importance.
Summarize State main areas discussed during
interaction.
Helps a patient to separate
relevant from irrelevant.
Plan Mutual decision-making regarding
the goals, direction and so on of
future interactions
Reiterates patient‘s roles within
relationship.
Types of Interviews
Interviews can be either informal or formal. Both informal and formal interviews seek
information about (1) patients‘ past health history, (2) current concerns, (3) level of
understanding about health and current problems, and (4) care and assistance desired.

35
Informal Interview
The informal interview may be conducted in a variety of settings—for example the waiting room
of a clinic, the school nurse‘s office or a patient‘s home. The informal interview is usually direct
and seeks to obtain expeditiously the most important data. The following example illustrates a
nurse‘s informal interview.
SEEKING INFORMATION ABOUT CURRENT CONCERNS AND PAST HEALTH
HISTORY.
Nurse: What brings you to the hospital today?
Patient: My arthritis is really acting up. I can barely cope with the pain.
Nurse: Is this a long-standing problem? Tell me more about it.
Patient: I‘ve had it for several years. I‘ve been taking a drug called Clinoril, but I ran out
about a week ago.
ASKING ABOUT UNDERSTANDING CURRENT PROBLEM
Nurse: Without the drug, is your arthritis much worse?
Patient: I don‘t know if it‘s worse, but I don‘t cope without it.
ASKING ABOUT ASSISTANCE THAT PATIENT NEEDS:
Nurse: What would you like us to do for you today?
Patient: Well I would like to get another prescription for Clinoril. But I heard that
relaxation techniques are effective with arthritis pain. I would like to talk
about this with you or the doctor.
In this example, the nurse is using both open-ended and direct questions to obtain the necessary
information. Both types of questions are useful. However, they each seek a different type of
information. Open-ended questions do not restrict responses to a specific topic or theme.
However they can be used to seek elaboration from patients on a particular topic. They
encourage patient involvement and self-exploration because they elicit responses that are more
than one or two words in length. In answering this, type of question, patients provide their
thoughts, perceptions and feelings regarding the issue under discussion. For instance, in the
example, when the nurse asks the open-ended question, ―What brings you the hospital today?‖,
the patient answers about the present hospital visit.
On the other hand, direct questions usually seek yes, no, or other short responses from patients.
In the example, ―Is this a long standing problem?‖, is a direct question, followed by an open-
ended statement, ―Tell me more about it.‖
It is important that nurses match the appropriate type of question to the type of information that
is sought. In some situations, it is essential to obtain factual information quickly so that patients‘
problems can be expeditiously handled. At other times, it is more important to understand the

36
patients‘ perception of their problems. Usually however, a mix of open-ended and direct
questions is most effective.
Formal Interview
The formal interview is usually longer and more structured than the informal interview.
Frequently nurses use a printed form, checklist or outline that may consist of topic headings or
questions. This approach seeks to guarantee complete and comprehensive data collection.
Following are suggestions for effective interviewing:
Establish a verbal contract with patients. This includes giving patients the interviewer‘s
name, title, role or position; explaining the purpose for the interview (which is usually to
form the basis for planning or evaluating care); informing patients of the approximate
length of the interview; indicating whether notes will be taken and discussing
confidentiality.
Sit at patient‘s level.
Make the setting a private and as free from distractions as possible.
Attend to patients‘ immediate physical needs before expecting them to focus on the
interview.
Vary the approach and format to meet patients‘ needs. For instance, a patient who is
deaf, unable to talk, or easily fatigued will necessitate a modification in a nurse‘s
approach.
Balance the use of direct and open-ended questions depending on the type of information
sought.
Collect only data that are not available elsewhere. It is a waste of both patients‘ and
nurses‘ time to seek information that is readily available on the chart.
Collect only information that is relevant to patient care.
Respect the patient‘s rights to refuse to provide all requested data.
As the interview draws to a close, inform patients that the process is almost complete. A
statement such as ―I only have two more questions‖ helps patients to focus on the
interview and gives them an opportunity to raise any final questions before the interview
is over.
Summarize the data acquired during the interview. This provides a mechanism to
validate data with patients and to assure that nurses‘ perceptions are correct.
SUMMARY:
Communication encompasses the process of interacting with others. Its main purpose is
transferring meaning, which has implications for nurses in teaching, facilitating others,
expressions of feelings, relieving anxiety, promoting, problem solving, and asserting self. The
collaborative approach is inherent in each of the aspects. Communication can be collaborative as
when patients‘ thoughts and feelings are valued and sought after. Or it can be controlling, as
when nurses limit or block patients‘ input. To provide effective care, nurses must understand the
importance of collaborative, empowering communication, and the techniques that facilitate as
well as hinder this process.

37
Communication occurs through verbal and nonverbal modes. The nonverbal mode – which
involves using body, voice, and environment--comprises the majority of communication.
Nonverbal communication is more challenging to nurses to interpret correctly and to respond to
appropriately. Metacommunication, which refers to the meaning behind the verbal and
nonverbal modes, is another important element in understanding the communication process.
Empowering communication, which is essential to mutuality, responds to patients‘ verbal and
nonverbal messages and communicates acceptance. Specific techniques of empowering,
communication include the use of listening, attending behaviors, and the techniques of warmth,
empathy, respect, genuineness, self-disclosure, and immediacy.
Several listener behaviors can serve as barriers to empowering communication. The most
important block is failure to listen to what patients are really saying. The other blocks include
failure to follow up, failure to examine, patients meaning, following standard forms too closely,
being judgmental, giving false reassurance, defending, giving advice, making stereotype
responses, and changing the topic.
The interview is presented as an example of a structured conversation, with a specific purpose- to
gather information. Interviews can be informal or formal; different techniques are appropriate to
each type. Interviewing is a necessary nursing activity that serves to collect data for research,
admission to a health care unit, and planning collaborative patient care. Effective
communication skills on the part of nurses are integral to the interview process.

38
References
Effective communication tips: http://www.effectivecommunicationtips.org/
Holsey, J. Molle-Matthews, E. (2006). A practical guide for therapeutic communication for
health professionals. St. Louis: Elsevier/Saunders.
Potter, P.,Perry, A. (2007). Basic nursing: essentials for practice. (6th
ed.) St. Louis:
Mosby/Elsevier.
Tamparo, C., Lindh, W. (2008). Therapeutic communications for health care. (3rd
ed.) New
York: Thompson/Delmar Learning.