
Communicable Diseases Rubella, Rubeola, Roseola, Fifth’s Disease, Chicken Pox, Scarlet Fever,...
16
Communicable Diseases Communicable Diseases Rubella, Rubeola, Roseola, Fifth’s Disease, Chicken Pox, Scarlet Fever, Mononucleosis
Transcript of Communicable Diseases Rubella, Rubeola, Roseola, Fifth’s Disease, Chicken Pox, Scarlet Fever,...

Communicable Communicable DiseasesDiseases
Rubella, Rubeola, Roseola, Fifth’s Disease, Chicken Pox, Scarlet Fever, Mononucleosis

Review terminology r/t communicable diseases:◦Incubation period◦Prodromal symptoms◦Period of communicability◦Types of Isolation: contact, respiratory
PreventionPrevention
Immunizations can prevent many of these diseases—primary prevention strategy
Careful handwashing to prevent transmission in essential for healthcare practitioners and for families
Infection Control: pp. 1019-1020 & Box 27-3Early identification of symptoms so that
treatment can be initiated is also paramount to a good outcome.

If a child is admitted to the hospital with an UNDIAGNOSED EXANTHEMA, strict isolation is instituted until a diagnosis is confirmed.
These are a few communicable diseases that require isolation: ◦ diphtheria ◦ chickenpox ◦ Measles, mumps, rubella◦ tuberculosis ◦ adenovirus ◦ Haemophilus influenzae type B ◦ influenza ◦ meningitis◦ Mycoplasma pneumonia, pseudomonas aeroginosa pneumonia ◦ pertussis ◦ RSV ◦ streptococcal pharyngitis, scarlet fever◦ Clostridium difficile, e.coli, shigella◦ pneumonia / pneumonic plague /
(AAP, Committee on Infectious Diseases, 2003) Reportable Communicable Dz list for Cook County

Prevent complicationsPrevent complications
Any immunocompromised children—those receiving steroid or immunosuppressive therapy, are always at risk for viremia, especially from viruses like herpes zoster.
Children with sickle cell anemia may develop aplastic anemia from erythema infectiosum (EI)[Fifth’s Dz]. The human parvovirus (HPV) infects and lyses RBC precursors.
Diphtheria and Scarlet Fever are bacterial and prevention of complications requires compliance with antibiotic therapy.

Prevent complicationsPrevent complications
High-risk children exposed to chickenpox should receive VZIG (varicella zoster immune globulin).
Acyclovir (Zovirax) may be used to treat varicella infections in high risk children with the disease.
Vitamin A supplementation in high doses has recently been shown to decrease morbidity and mortality rates in measles. Careful instruction to parents on safe storage of Vitamin A is essential.

Provide comfortProvide comfort
Alleviate itching that is one of the most common discomforts of rashes◦Cool/tepid baths without soap, may use oatmeal◦Calamine/Caladryl lotions must be applied sparingly
to prevent toxic levels being absorbed. They contain diphenhydramine.
◦Wear lightweight, loose clothing, keep cool◦Keep nails short, wear mittens on young children◦Suggest po. Diphenhydramine (Benadryl)
Offer antipyretics (acetominophen or ibuprofen) for fever and general malaise
Lozenges, saline rinses for sore throatsSuggest quiet activities

Support family and childSupport family and child
Provide accurate information re: period of communicability and period of recovery.
Provide support and encouragement.
Review importance of compliance with therapy.
No Salicylate products with all viral diseases because of link to Reye Syndrome

Review Table 16-1 Communicable Diseases of Childhood pp. 608-614 (Hockenberry et al, 9th ed.)
Know association of high fever and febrile seizures with Roseola and importance of careful antipyretic management.
Know common sx of Rubeola (measles) including koplik’s spots, photophobia.
Know period of communicability of Varicella/chickenpox and appropriate counsel to parents re: when child can return to school
Know etiology of Scarlet Fever, common sx, management, and when to return to school
Know risks to fetus if Rubella is contracted in the mother’s first trimester of pregnancy
Know appearance of rash for Fifth Disease (HPV)
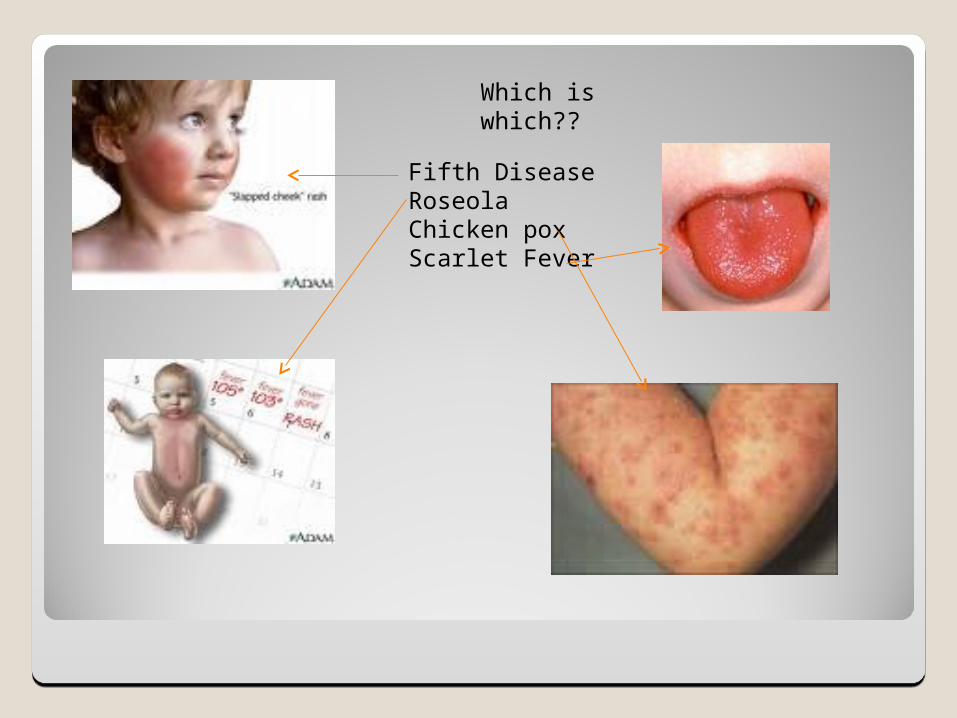
Which is which??
Fifth DiseaseRoseolaChicken poxScarlet Fever

MononucleosisMononucleosis
Etiology: Epstein Barr VirusNatural Hx:
◦Typically self-limiting & uncomplicated◦Incubation period: 30-60 days◦Preclinical stage: 3-5 days◦Acute illness: 7-20 days◦Convalescence: 2-6 weeks◦Viral excretion may occur many months after
infection◦Often asymptomatic and difficult to diagnose

Mononucleosis (cont’d)Mononucleosis (cont’d)
Transmission: through saliva (usually intimate contact, thus the nickname, ‘Kissing Disease’)
Pathophysiology◦ EBV infects B-lymphocytes lymphoproliferation◦ Lab results: atypical lymphocytes called Downey cells
WBC’s especially lymphs and liver enzymes EBV antibody titer + Monospot test

Mononucleosis (Cont’d)Mononucleosis (Cont’d)
Signs and Symptoms◦General malaise◦Sore throat, gelatinous film over palate and
uvula, red macules on palate◦Tonsillar enlargement, white exudate on
tonsils, red pharynx◦Fever◦Macular rash (trunk)◦Abdominal pain◦Cervical lymphadenopathy◦Splenomegaly◦Hepatomegaly

Mononucleosis (cont’d)Mononucleosis (cont’d)
Population most affected:12-26 yr oldsNursing concerns
◦Potential for secondary infection◦Potential for injury◦School absenteeism◦Possible complications:
Aseptic meningitis Encephalitis Guillian Barré Syndrome Splenic rupture

Primary prevention◦ General health promotion measures
Secondary prevention◦ Prompt medical attention for sore throats to r/o strep
throat◦ Screening to r/o secondary bacterial infection
Tertiary prevention◦Palliative:
Fever (rest, calories, fluids, Acetominophen Saline gargles Soft foods
◦No contact sports◦Referral for home-bound teacher, if pt has to
stay home for lack of energy and malaise◦Can go to school if feels up to it

Wash your hands and stop the Wash your hands and stop the spread of these communicable spread of these communicable
diseases!diseases!
That should do it!


















