Common Deficiences in Bioequivalence Studies and Biowaiver ...
28
Common Deficiences in Bioequivalence Studies and Biowaiver Requests submitted to the JFDA DIMA S. SHAHIN, M.SC. MEMBER OF THE BIOEQUIVALENCE STUDIES TECHNICAL COMMITTEE REGISTRATION DEPARTMENT, DRUG DIRECTORATE- JORDAN FOOD AND DRUG ADMINISTRATION (JFDA) 2 ND MENA REGULATORY CONFERENCE ON BIOEQUIVALENCE, BIOWAIVERS, BIOANALYSIS, DISSOLUTION AND BIOSIMILARS
Transcript of Common Deficiences in Bioequivalence Studies and Biowaiver ...
Common Deficiences in Bioequivalence Studies and Biowaiver Requests submitted to the JFDA
DIMA S. SHAHIN, M.SC. M E M B E R O F T H E B I O E Q U I V A L E N C E S T U D I E S T E C H N I C A L C O M M I T T E E
R E G I S T R A T I O N D E P A R T M E N T ,
D R U G D I R E C T O R A T E - J O R D A N F O O D A N D D R U G A D M I N I S T R A T I O N ( J F D A )
2 N D M E N A R E G U L A T O R Y C O N F E R E N C E O N B I O E Q U I V A L E N C E , B I O W A I V E R S , B I O A N A L Y S I S , D I S S O L U T I O N A N D B I O S I M I L A R S

Topics for Discussion
• Why to request BE studies for generic drugs?
• Statistics for BE studies \ BW requests submitted in 2013
• Common deficiencies in BE\BW submissions • Case studies
• Recommendations for better BE and Bio-waivers submissions

A generic product must meet the standards established by Jordan Food and Drug Administration
(JFDA) to be approved for marketing in Jordan.
JFDA approves a generic product for marketing if it is proved to be therapeutically equivalent to the
reference product.
Therapeutic Equivalence = Pharmaceutical Equivalence / Alternative + Bioequivalence
Same safety and efficacy profiles after administration of same dose
A therapeutically equivalent generic product is interchangeable with the RLD.
Why to request BE studies for generic drugs?

Why to request BE studies for generic drugs? Establishing Equivalence… Comparative pharmacokinetic studies
– In vivo comparative bioavailability studies
– Comparison of performance of FPPs based rate and extent of absorption of API from each formulation
• Area under the concentration-time curve (AUC)
• Maximal concentration (Cmax)
• Time to maximal concentration (Tmax)
Comparative pharmacodynamic studies
Comparative clinical trials
Comparative in vitro methods
– Biopharmaceutics Classification System (BCS)-based biowaivers
– Additional strengths biowaivers
Statistics for BE studies \ BW requests submitted in 2013
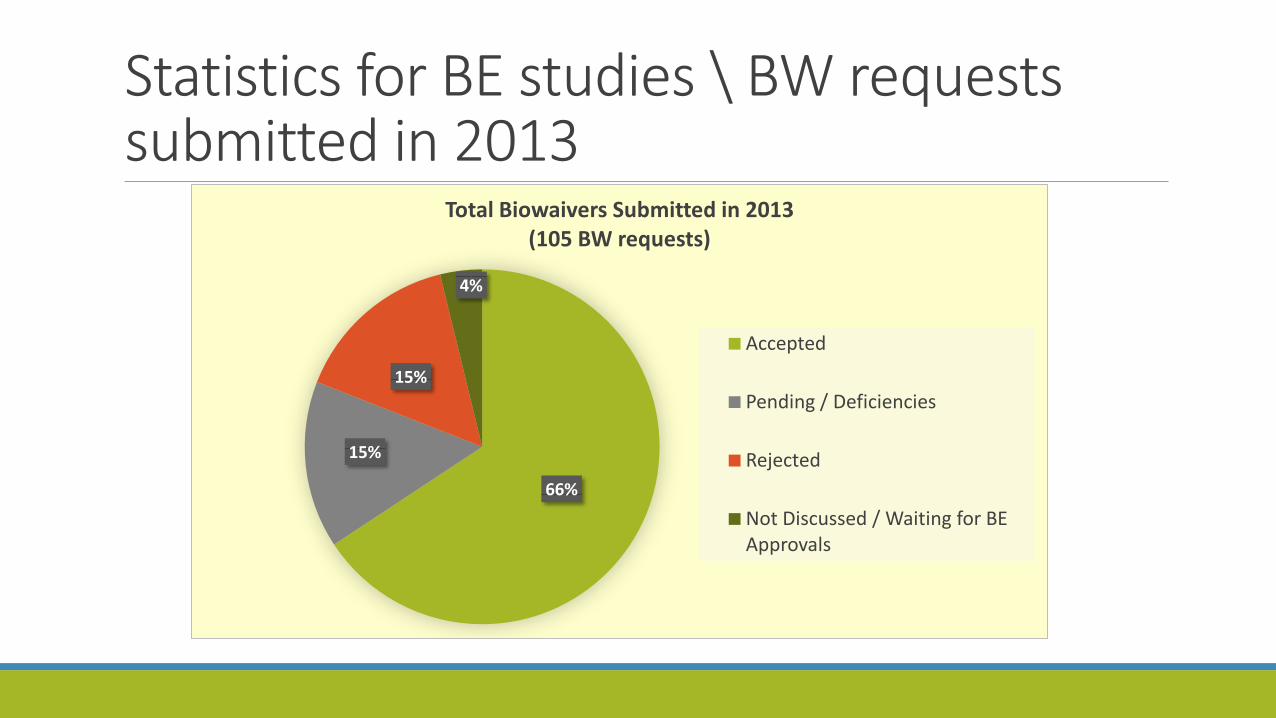
A total of 61 (36.75%) Bioequivalence Studies and 105 (63.25%) Bio-waiver requests were submitted in 2013
Results of the review process within the past 2 years (till the end of August 2015)
All (61) submitted BE Studies have been evaluated
Only 4 of the submitted (105) BW requests have not been Discussed / Waiting for BE Approvals

Statistics for BE studies \ BW requests submitted in 2013
87%
6%
7%
Total BE Studies Submitted in 2013 (61 BE Studies)
Accepted
Pending / Deficiencies
Rejected

Statistics for BE studies \ BW requests submitted in 2013
13.11%
85.25%
1.64% 0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
80.00%
90.00%
1 2 3
Accepted BE Studies relative to no. of BE Committee sessions
1st 2nd 3 or more 13.11% 57.14% 80.95% Accepted 85.25% 36.73% 19.05% Pending / Deficiencies
1.64% 6.12% 0.00% Rejected
Statistics for BE studies \ BW requests submitted in 2013
66%
15%
15%
4%
Total Biowaivers Submitted in 2013 (105 BW requests)
Accepted
Pending / Deficiencies
Rejected
Not Discussed / Waiting for BE Approvals

Statistics for BE studies \ BW requests submitted in 2013
9.90%
60.00%
38.89%
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
1 2 3
Accepted BW Requests relative to no. of BE Committee sessions
1st 2nd 3 or more 9.90% 60.00% 38.89% Accepted
82.18% 36.00% 47.22% Pending / Deficiencies
7.92% 4.00% 13.89% Rejected
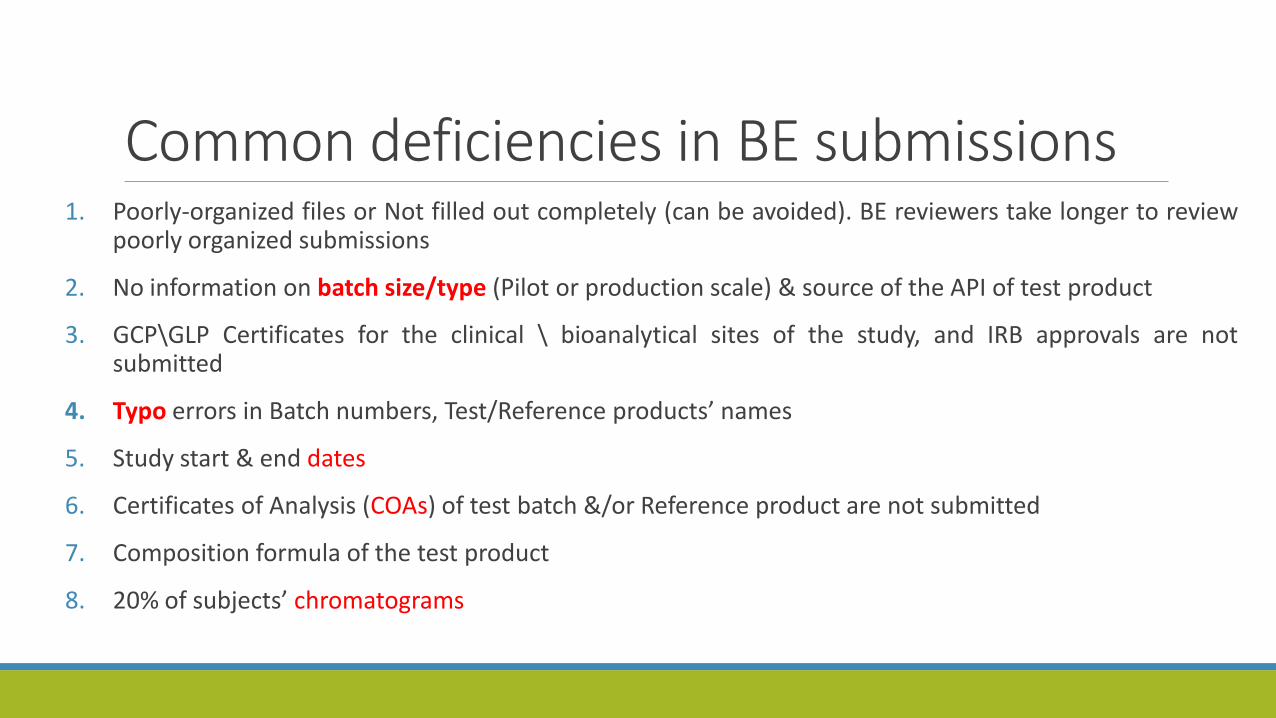
Common deficiencies in BE submissions 1. Poorly-organized files or Not filled out completely (can be avoided). BE reviewers take longer to review
poorly organized submissions
2. No information on batch size/type (Pilot or production scale) & source of the API of test product
3. GCP\GLP Certificates for the clinical \ bioanalytical sites of the study, and IRB approvals are not submitted
4. Typo errors in Batch numbers, Test/Reference products’ names
5. Study start & end dates
6. Certificates of Analysis (COAs) of test batch &/or Reference product are not submitted
7. Composition formula of the test product
8. 20% of subjects’ chromatograms
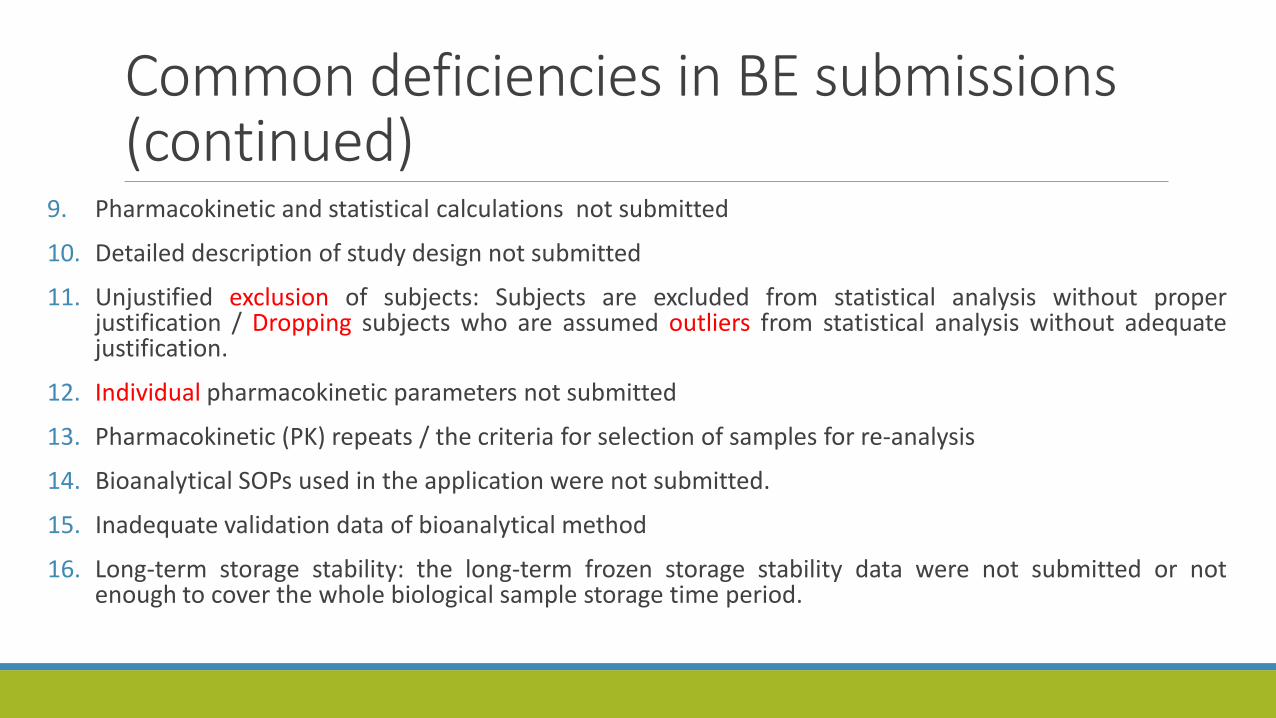
Common deficiencies in BE submissions (continued)
9. Pharmacokinetic and statistical calculations not submitted
10. Detailed description of study design not submitted
11. Unjustified exclusion of subjects: Subjects are excluded from statistical analysis without proper justification / Dropping subjects who are assumed outliers from statistical analysis without adequate justification.
12. Individual pharmacokinetic parameters not submitted
13. Pharmacokinetic (PK) repeats / the criteria for selection of samples for re-analysis
14. Bioanalytical SOPs used in the application were not submitted.
15. Inadequate validation data of bioanalytical method
16. Long-term storage stability: the long-term frozen storage stability data were not submitted or not enough to cover the whole biological sample storage time period.
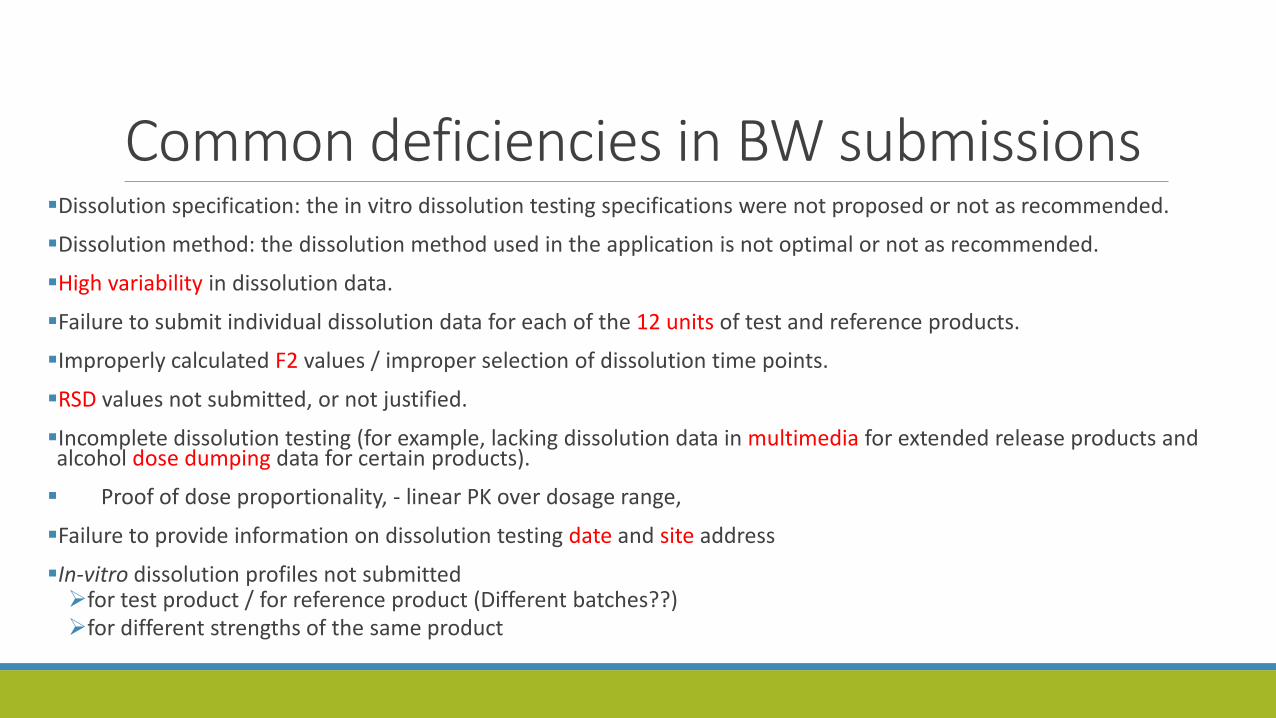
Common deficiencies in BW submissions Dissolution specification: the in vitro dissolution testing specifications were not proposed or not as recommended.
Dissolution method: the dissolution method used in the application is not optimal or not as recommended.
High variability in dissolution data.
Failure to submit individual dissolution data for each of the 12 units of test and reference products.
Improperly calculated F2 values / improper selection of dissolution time points.
RSD values not submitted, or not justified.
Incomplete dissolution testing (for example, lacking dissolution data in multimedia for extended release products and alcohol dose dumping data for certain products).
Proof of dose proportionality, - linear PK over dosage range,
Failure to provide information on dissolution testing date and site address
In-vitro dissolution profiles not submitted for test product / for reference product (Different batches??) for different strengths of the same product

Case Studies

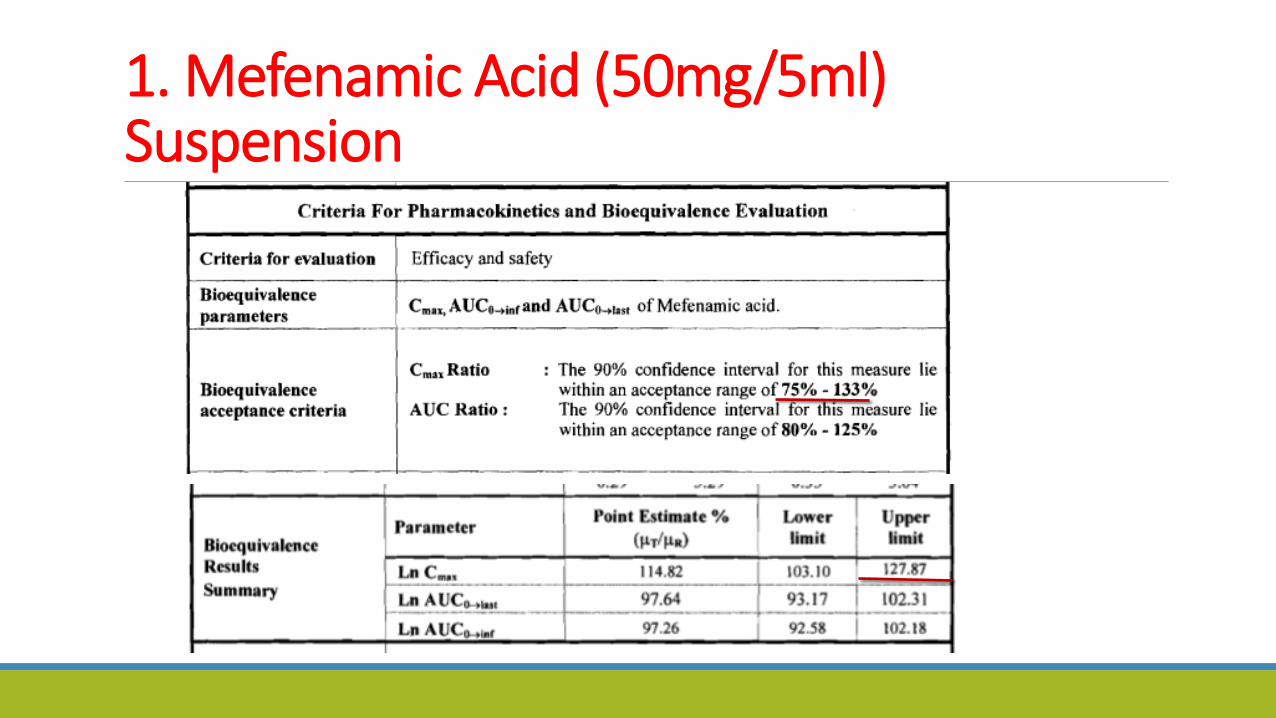
1. Mefenamic Acid (50mg/5ml) Suspension
1. Mefenamic Acid (50mg/5ml) Suspension

1. Mefenamic Acid (50mg/5ml) Suspension
Fasting or Fed???
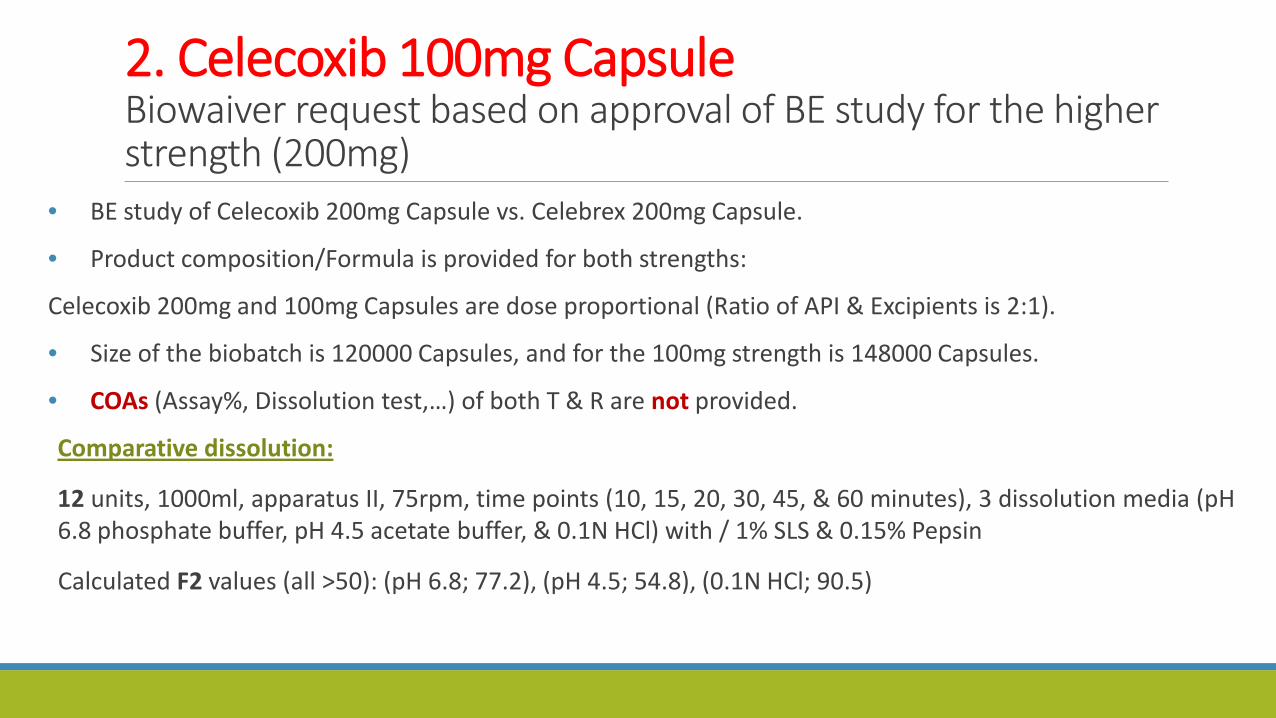
2. Celecoxib 100mg Capsule Biowaiver request based on approval of BE study for the higher strength (200mg)
• BE study of Celecoxib 200mg Capsule vs. Celebrex 200mg Capsule.
• Product composition/Formula is provided for both strengths:
Celecoxib 200mg and 100mg Capsules are dose proportional (Ratio of API & Excipients is 2:1).
• Size of the biobatch is 120000 Capsules, and for the 100mg strength is 148000 Capsules.
• COAs (Assay%, Dissolution test,…) of both T & R are not provided.
Comparative dissolution:
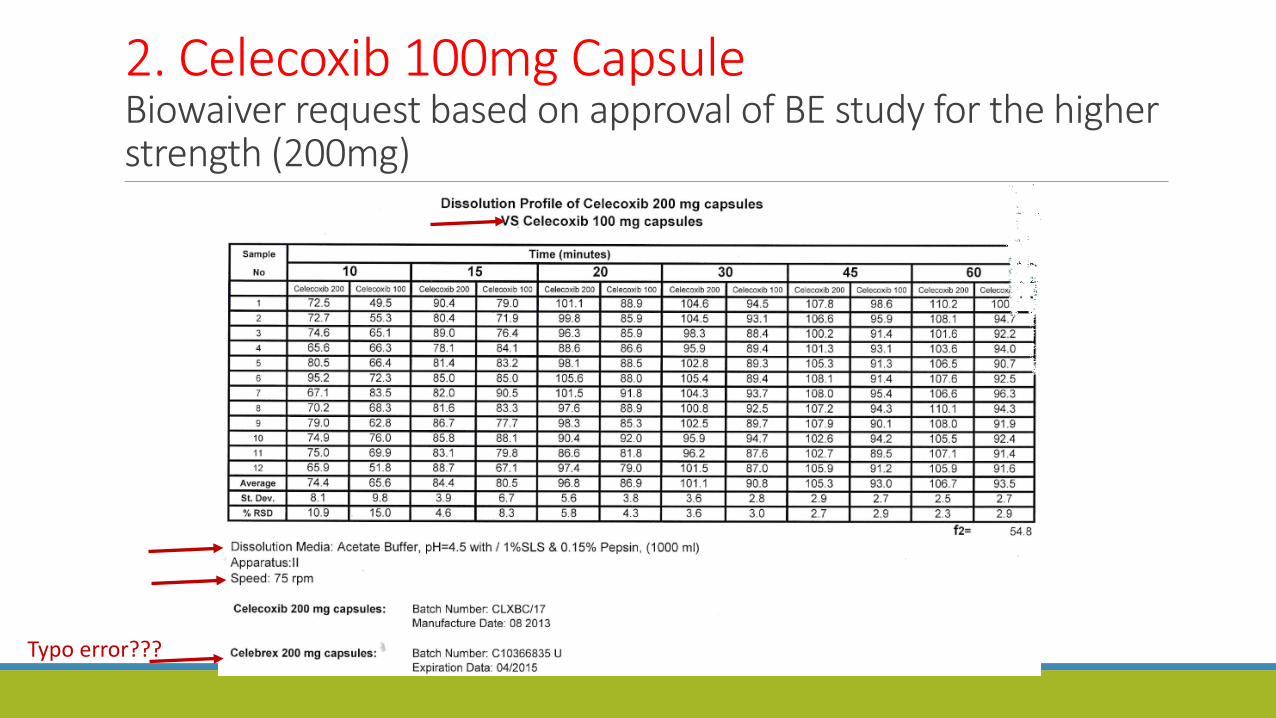
12 units, 1000ml, apparatus II, 75rpm, time points (10, 15, 20, 30, 45, & 60 minutes), 3 dissolution media (pH 6.8 phosphate buffer, pH 4.5 acetate buffer, & 0.1N HCl) with / 1% SLS & 0.15% Pepsin
Calculated F2 values (all >50): (pH 6.8; 77.2), (pH 4.5; 54.8), (0.1N HCl; 90.5)

2. Celecoxib 100mg Capsule Biowaiver request based on approval of BE study for the higher strength (200mg)

2. Celecoxib 100mg Capsule Biowaiver request based on approval of BE study for the higher strength (200mg)
2. Celecoxib 100mg Capsule Biowaiver request based on approval of BE study for the higher strength (200mg)
Typo error???

2. Celecoxib 100mg Capsule Biowaiver request based on approval of BE study for the higher strength (200mg)

In the analytical method validation report,…
concentration of the filtered samples?
(LLOQ, HLOQ)??
2. Celecoxib 100mg Capsule Biowaiver request based on approval of BE study for the higher strength (200mg)

3. Erlotinib 100mg Film Coated Tablet Biowaiver request based on approval of BE study for the higher strength (150mg)

Erlotinib 100mg Film Coated Tablet Biowaiver request based on approval of BE study for the higher strength (150mg)
RSD values??? COAs of T & R???
Erlotinib 100mg vs. Erotinib 150mg (Biobatch)???
Size of the T product batch is 30000 FCT
Addition of 1% SLS to the 3 dissolution media???
(same deficiencies apply to the dissolution profile
In other media)

Risperidone 4mg Tablet BE study under fasting conditions
1. No IRB signature.
2. Study was conducted on 4mg concentration and for safety reasons it must be conducted on the 1mg strength.
3. GLP dated 2006 / year of study 2003 .**The bioanalytical part of bioequivalence trials should be performed in accordance with the principles of Good Laboratory Practice (GLP)
4. GMP for manufacturer dated 2008 / biobatch manufactured in 2003.

Glimepiride 1 mg Film Coated Tablet BE study under fasting conditions
1. Assay difference between T (99%) and R (106%) > 5% .** assayed content of the batch used as test product should not differ more than 5% from that of the batch used as reference product . .EMEA CPMP/QWP/EWP/1401/98 Rev. 1
2. Long term stability for samples in matrix did not cover period of storage and analysis.

Recommendations for Better BE Submissions
Complete data filling at time of submission
According to the CTD format
Check the New JFDA Guidelines in 30/9/2010, and their latest updates
Check the recommended dissolution methods listed in Dissolution Database for comparison to different method applicant may propose (http://www.accessdata.fda.gov/scripts/cder/dissolution/index.cfm)
Check the periodically updated BE Recommendations Databases
(In form of draft or final guidance) (http://www.fda.gov/cder/guidance/bioequivalence/default.htm)

Thank you for your kind attention