Colorectal Surgery & Preoperative Risk in the Elderly · Tekkis et al ACPGBI CRC study 2002. lymph...
34
Colorectal Surgery & Preoperative Risk in the Elderly 1st Geneva International Scientific Day on Senior Visceral Surgery RA Audisio, MD, FRCS University of Liverpool UK
Transcript of Colorectal Surgery & Preoperative Risk in the Elderly · Tekkis et al ACPGBI CRC study 2002. lymph...

Colorectal Surgery & Preoperative Risk in the
Elderly
1st Geneva International Scientific Day on Senior Visceral Surgery
RA Audisio, MD, FRCSUniversity of Liverpool UK

Gerontography
http://www.worldmapper.org/index.html

People >80 (2000, projections for 2030 and 2050)US Census Bureau & National Institute on Aging report1

Age-specific colon ca. - Japan

Ann Oncol. 1997 Apr;8(4):317-26Elective surgery for gastrointestinal tumours in the elderlyAudisio RA, et al.
Authors age n. pts op. † % 5yr surv %_______________________________________________________________________Jensen, Hermanek, Waldron, Umpley,Irvin, Brown, > 70 2,834 12 (1-29) 48 (26-52)Katshan, Mulcahy
Payne, Bader,Raab, Kingston > 75 990 10 (7-14) 46 (31-50)
Arnad, Sunouchi > 80 150 20 41

older patients can be operated
good long-term cancer outcomes
slightly increased short-term outcomes
selection bias

Evidence of under-management:
NJ Turner BMJ 1999

under-staging
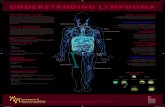
Tekkis et al ACPGBI CRC study 2002

lymph node positivity with age

lymph node harvest with age
Tekkis et al ACPGBI CRC study 2003

assessing frailty

Definition of frailty is crucial in:
Designing Clinical Studies/Trials
Consenting patient
Individualising treatment
Predicting outcome
Comparing series

life expectancy
n./severity of comorbidities
CGA – MGA – screening tools
“rule of thumb”
ASA - POSSUM
Patients’ selection

the Rule of ThumbSurgical assessment was highly
accurate…
lack of consistency
…but not reproducible

Life expectancy tables
consistency in advise to treatmentmean 68.6% (range 30.9% - 91.6%)

Life expectancy tables

Prevalence of comorbidity across the age spectrum
Piccirillo JF. Crit Rev Onc Hem 2008

Comorbidity is prognostically most important in situations where the prognostic impact of the tumour is small.
Comorbidity
Read WL. JCO 2004
Conversely, where the tumour is advanced or aggressive and the prognosis is poor, comorbidity information is less important.


Age & co-morbiditiesare NOT
independent risk factors for operative mortality

• Comorbidities & Functional Status are independent
• Correlation between PS & ADL/IADL is moderate
• Patients with comorbidities do not have a higher risk of developing complications
Comorbidities
Extermann M. JCO 1998Repetto L. JCO 2002Lemmens V. WJSO 2006

POSSUM & P-POSSUM
observed † POSSUM † P-POSSUM † overall 7.5% 8.2% 7.1%elective 3.2% 4.6% 3.8%emergency 23.4% 16.7% 19.5%
<50yrs 0.5% 3.3% 2.6%50-59yrs 2.7% 6.1% 3.6%60-69yrs 5.3% 7.5% 6.2%70-79yrs 8.6% 11.8% 9.7%>80yrs 22.0% 12.4% 12.3%
PP Tekkis et al.BJS 2003;90:340

POSSUM & P-POSSUMPP Tekkis et al.
BJS 2003;90:340

complications (any & major) by severity of surgery stratified
by age group
010203040506070
70-74 75-79 80+ 70-74 75-79 80+ 70-74 75-79 80+
Severity of surgery
Major Any
Mod/ intermediate Major Complex major
Type of complication
Age group:
% with complications

multivariate analysis(Cox Regression)
Component of PACE RR* 95%CI
30 days Morbidity
BFI mod/severe fatigue (>3) 1.46 1.18-2.13
IADL dependent (<8) 1.36 1.04-2.05
Hospital stay
ADL dependent (>0) 2.00 1.37-2.92

PACE: probability of complications andn. deranged components
0
10
20
30
40
50
60
70
% w
ith
at lea
st 1
mor
bidi
ty
0 1 2 3

Functional Health StatusPerformance Status (PS)Mini mental State (MMS)
Brief Fatigue Inventory (BFI)Activities of Daily Living (ADL)
Geriatric Depression Scale (GDS)Instrumental activities of daily living (IADL)
Quick toolsVES-13
GFI“up & go”
Prospective series of consenting (MMS >18) elderly (>70 yrs) surgical cancer patients
PREOP
End Points30-day mortality & morbidity
n. of specialists involved

Frailty & Surgical Practice:Unbiased selection
Comparison of surgical outcomesConsenting & treatment planning
Tackling comorbiditiesIndividualised care
Improved survival (?)

personal tips
Per-operativelyMinimise blood lossesCareful anaesthetics
Post-operativelyNo NGTPrompt mobilizationEarly post-operative oral feeding
Pre-operativelyAvoid acute settingPrevention chest infections with positive
pressure chest physiotherapyOptimize nutritional statusNo bowel preparationSupra-pubic catheter (♂)

Surgery:
“If you can do it,it does not mean itneeds to be done”

TME – Total Mesorectal Excision

TME in the elderlyCancer Registry Data: 1,508pt >75yrs
Rutten HJT. Lancet Onc 2008

excessive operative death
Rutten HJT. Lancet Onc 2008
“… the effectiveness of TME surgery in the overall population cannot be simply derived from findings of studies involving a younger age group.”

Assessing Frailty in Surgical Practice
Understanding patient’s needs
Consenting & treatment planning
Tackling comorbidities
Individualising care
Improving survival & QoL